
Abstract
Most people with a psychotic illness will never be violent; however, it is widely known that violence is more prevalent in this group compared to the general community, particularly during first-episode psychosis (FEP). Despite this, there is limited research into what contributes to this increased risk during FEP. The present systematic review aimed to identify whether certain risk factors are differentially associated with severity and timing of violence perpetration during FEP. The following databases were used to identify studies, up to March 8, 2024: MEDLINE, Embase, PsycINFO, CINAHL, and ProQuest. A total of 15 studies were included. Male gender, non-white ethnicity, history of violence, higher general psychopathology, and recent substance use were significantly associated with any violence, regardless of the time at which violence was committed. Serious violence was not associated with any risk factors. Higher general psychopathology was associated with any violence committed before presentation to services, while male gender was associated with violence perpetrated at service entry. Only male gender and unemployment were associated with violence committed after treatment. Based on our results, risk factors appear to vary according to the severity and timing of violence. These risk factors also overlap with those found associated with violence risk in the general community, and those correlated with the risk of psychosis. Past studies are limited in the range of risk factors studied and further work is needed to understand correlates of violence in people who have experienced FEP to inform treatment options.
Introduction
People with serious mental illnesses, such as non-affective (schizophrenia) and affective (bipolar disorder) psychotic disorders, are often portrayed in the media as being violent, which can perpetuate negative attitudes and misconceptions about these disorders by the general public (Ahonen et al, 2019; Mentxaka et al., 2023). Nevertheless, although most people with psychotic disorders will never act violently, the risk of violence perpetration in this group is known to be higher than in the general population (Fazel et al., 2009a; Whiting et al., 2022), and previous studies have shown that the rate of violence is increased in people with schizophrenia-spectrum, personality and substance use disorders, compared to other psychiatric disorders (Ahonen et al., 2019; Whiting et al., 2021).
Increased rates of violence have also been shown during early stages of the disorder, particularly during the first-episode psychosis (FEP; Fazel et al., 2009b; Látalová, 2014; Nielssen & Large, 2010; Nielssen et al., 2012; Weiser, 2018), which typically refers to the initial period following the onset of psychotic symptoms. Systematic reviews have reported rates of violence between 13.4% (Youn et al., 2024) and 35.4% (Large & Nielssen, 2011) during this stage; rates that are higher than those reported in more established disorders (Large & Nielssen, 2011; Nielssen et al., 2012) (around 9.9% (Fazel et al., 2009a) to 19.1% (Swanson et al., 2006)). While it is widely agreed that people with FEP are at greater risk of perpetrating violence, evidence for the precise reasons for increased violence and the associated risk factors remains limited (Witt et al., 2013). Consequently, this has likely contributed to ongoing stigma for people with psychosis as being violent and dangerous, without fully understanding what may be contributing to this increased prevalence.
Several reviews have explored risk factors of violence during more established stages of psychosis (e.g., Douglas et al., 2009; Witt et al., 2013), but only a small number of reviews have focused on the earlier stages of illness. The last systematic review to examine a broad range of risk factors for violence during FEP was published over 10 years ago, and this study found that involuntary treatment, forensic history, and demographic factors such as younger age and male sex were associated with violence (Large & Nielssen, 2011). Although this study provided a comprehensive overview of the prevalence and risk factors of violence, the findings are outdated and it is possible that the nature and correlates of violence may have changed, particularly with the recent reduction in the overall rate of violence (Youn et al., 2024). Another older review (Winsper et al., 2013) explored the pooled prevalence of violence while considering methodological factors (e.g., assessment tools, study location) and timing of violence (e.g., before or after treatment initiation); however, it did not explore a broad range of clinical, demographic, or treatment variables. Similarly, two systematic reviews have been conducted in more recent years, but rather than considering a broad range of both dynamic (modifiable) and static (fixed or nonmodifiable) risk factors, they only narrowly focused on specific clinical factors, including trauma (Del Pozzo et al., 2021) and duration of untreated psychosis (DUP; Látalová, 2014).
Additionally, there is some evidence that prevalence and risk factors vary according to the timing and severity of violence; however, only one study (Large & Nielssen, 2011) has thoroughly reviewed the existing literature according to these attributes. This review found that rates and correlates of violence differed according to severity (less serious, more serious, and severe violence) and when the violence was perpetrated (before or after treatment initiation). For example, serious violence was associated with forensic history, DUP, and overall total symptom score; however, the overall total symptom score did not emerge as a risk factor when the severity of violence was not considered. One potential barrier to examining violence according to these factors is the wide variability in the estimated rates and risk factors among individual studies (Douglas et al., 2009). This is largely attributed to studies failing to consider these factors and using inconsistent methods when defining and categorizing violence, which can lead to high between-study heterogeneity (Douglas et al., 2009; Youn et al., 2024).
In addition to the need for an updated review, by examining a comprehensive range of risk factors associated with violence, we can identify potential modifiable targets for early intervention and improve our understanding of who may be at increased risk for violence, to reduce the risk of future violence (Marion-Veyron et al., 2015). A better understanding of the complex relationship between violence and FEP may also subsequently help address the stigma of violence for people with psychotic disorders. Therefore, the broad aim of the current study was to provide an updated review investigating which factors have been associated with increased risk for violence perpetration in people experiencing FEP. A further aim was to understand whether correlates of risk vary according to both severity of violence (less serious, serious, and any violence) and the timing at which violence (before first presentation, at initial presentation to services, and after treatment initiation) was perpetrated.
Method
Search Strategy
The search plan has been outlined previously (Youn et al., 2024). In the current study, however, the publication year was not limited to a specific time period, to allow a thorough and comprehensive review of all existing literature. Although the search plan was similar to a previous study that examined rates of violence, the differences in inclusion/exclusion criteria ensured that only the relevant studies examining risk factors were selected during the full-text screening stage. Grey literature (e.g., unpublished theses) were also included to reduce publication bias (Remington et al., 2013). Five search plans were used to locate studies from MEDLINE, Embase, PsycINFO, CINAHL, and ProQuest. All searches were conducted on March 8, 2024. The reference lists of relevant papers were manually searched for additional studies that may have been missed.
Inclusion Criteria
Participants
Studies were included if participant diagnosis was reported as early psychosis or FEP of any non-affective (schizophrenia, schizophreniform disorder, brief psychotic disorder, and delusional disorder) or affective (bipolar disorder, schizoaffective disorder, and major depressive disorder with psychotic features) psychotic disorder, or psychotic disorder not otherwise specified. The terms “early psychosis” and “first-episode psychosis” are often used interchangeably across studies; however, the term “first-episode psychosis” has been more commonly used in similar previous reviews (Large & Nielssen, 2011; Nielssen et al., 2012). FEP is usually defined broadly as the early stage of psychotic disorder or treatment, and not necessarily the first “episode” of psychosis (Breitborde et al., 2009). To address this issue, a previous study (Breitborde et al., 2009) has recommended using the term “recent-onset psychosis” instead of FEP based on the duration of the psychotic disorder. However, this can be challenging, as most of the existing studies do not report this information. Hence, instead of determining diagnoses based on illness duration, we adopted a similar approach to pre-existing reviews (Large & Nielssen, 2011; Nielssen et al., 2012) and included studies with people who were experiencing early psychosis or FEP, unless they: (1) did not specify stage of disorder and whether participants were experiencing early psychosis or FEP; (2) did not use a well-validated diagnostic framework (e.g., Diagnostic and Statistical Manual of Mental Disorders [DSM], International Classification of Diseases [ICD]); (3) did not specify method of diagnosis; (4) only included forensic samples (e.g., prison populations); and/or (5) did not include a non-violent control group. There was no limit on participant age, as FEP can occur at any age (Simon et al., 2017), although it is most common between 15 and 30 years (Jones, 2013).
Violence
Studies were included if they investigated factors associated with violence perpetration. There was no time limit on when the violence was committed (e.g., before first presentation to services, at first entry to services, after treatment initiation), or the length of follow-up period. Studies were excluded if they: (1) assessed verbal aggression or violence toward the self or objects only, and not in addition to physical violence toward other people; and (2) did not specify whether violence included violence toward other people.
Within the psychosis literature, violence is typically defined as behavior involving physical force toward another person (Large & Nielssen, 2011). Similarly, for the purpose of the current study we focused only on physical violence perpetrated toward other people, and did not include violence toward the self, objects, or verbal aggression. Violence was further grouped according to severity, based on definitions from Large and Nielssen (2011): (1) any violence (any form of physical violence perpetrated toward other people). The term “any violence” was used when studies did not report the severity of violence; (2) less serious violence (physical violence against other people not causing injury and without weapon use); (3) serious violence (physical violence causing any degree of injury with or without weapon use or any sexual assault); and (4) severe violence (physical violence toward others resulting in serious injury requiring treatment in hospital or permanent physical harm). Violence was also categorized according to the timing at which the violence was perpetrated: (1) before presentation (at least 3 months or unspecified period before presentation to services); (2) at first presentation (“baseline” or less than 3 months before or after first presentation to services); and (3) after presentation to services (at least 3 months since treatment initiation).
Factors Associated with Violence
All included studies reported associations between violence and a range of demographic, sociodemographic, clinical and treatment characteristics, or sufficient information to calculate the relevant statistics. These characteristics were defined broadly to ensure that all relevant information was captured. Studies that only examined physiological characteristics such as genetic and/or neurological factors (e.g., via brain imaging) were not included, to ensure that the scope of the review was appropriate, and that findings are translatable to early intervention services, which usually have a strong focus on psychosocial and psychopharmacological interventions (Correll et al., 2018).
Procedure
Study Selection
Three researchers (SY, SM, NC) independently screened study’s titles and abstracts. Studies were selected if: (1) participants had a diagnosis of early psychosis or FEP of any psychotic disorder; and (2) violence or aggression was assessed. Full-text articles were then screened by SY and SM according to the inclusion criteria. Studies with overlapping samples were identified and excluded if the study was: (1) not the original study (i.e., later publication year) and/or (2) included less information about factors associated and/or not associated with violence, compared to the original study.
Data Extraction
The following variables were extracted independently by SY and SM: author; year of publication; title; country; study setting; recruitment period; sample size; sample demographics (age, gender); diagnostic method; participant diagnoses; definition and measurement of violence, including source of data (e.g., official police reports); severity (e.g., severe violence), timing (e.g., before first presentation to services); and information related to factors that were both associated and/or not associated with violence (e.g., effect size, 95% confidence intervals [CI], p-values). These data were extracted by SY for all studies, and a random sample of five studies was selected for extraction by SM to ensure inter-rater reliability.
Extracted variables were categorized as one of the following: demographic, sociodemographic, neurocognitive, treatment-related, violence and forensic, psychosis-related, psychopathology, and substance use. When possible, variables were further categorized on the recency of the event. For example, “recent substance use” (e.g., alcohol, cannabis) was defined as any substance use in the past 6 months, and “history of substance use” referred to substance use more than 6 months ago. As previously recommended (Witt et al., 2013), variables were only extracted for statistical analyses if they were examined in three or more studies. For studies that reported separate associations for violence toward others, self, and/or objects, only information related to violence toward others was included. If studies examined violence toward others, but only reported data for unspecified violence, the latter was included.
Quality Appraisal of Studies
The methodological quality of studies was assessed by SY and SM using adapted versions of the Joanna Briggs Institute Critical Appraisal Checklist for: (1) Studies Reporting Prevalence Data; (2) Analytical Cross-Sectional Studies; and (3) Cohort Studies (see Supplemental Table 1). The adapted version was a five-item scale pertaining to quality of methodologies used in a study. A response of “yes,” “no,” “unsure,” or “not applicable” was given for each item. “Yes” and “not applicable” responses were scored “1,” while “no” and “unsure” responses were scored “0.”
Statistical Analysis
Statistical analyses were conducted using R Version 4.1.1 (R Core Team, 2020). Descriptive statistics were used to describe the studies.
Odds ratios (OR) were extracted from studies or calculated separately based on the available information. ORs were then converted to log transformed ORs before conducting the statistical analyses (Chinn, 2000). When studies did not report ORs but included frequency data or chi-squared (χ2) results, ORs were manually calculated using this information. If studies reported results from t-tests, these values were converted to Cohen’s d, then to ORs, and finally to log transformed ORs. When studies reported mean and standard deviation (SD) values and no frequency data or effect size, the mean and SD were used to calculate Cohen’s d, which was then transformed to OR, and finally to log transformed OR. Non-independent samples were excluded from each analysis, when studies reported more than 1 OR for 1 variable. To do this, analyses were separated by severity and timing of violence. When studies reported separate ORs for two different time points (e.g., 1 week before and 1 week after presentation), which fell into one time point category defined in the study (e.g., both fall under “at first presentation”), the ORs that were calculated across all time points were extracted, and not separate ORs. ORs were considered weak (OR = 1.5–2.5), moderate (OR = 2.5–4), strong (OR = 4–10), or very strong (OR > 10; Rosenthal, 1996).
Subgroup analyses were also conducted based on violence severity (e.g., less serious, serious, and severe violence) and timing of violence (e.g., before presentation, at first presentation, and after presentation). High levels of between-study heterogeneity were expected due to discrepancies in results such as demographic factors and the definition, measurement, and timing of violence across studies. Hence, a random-effects model was chosen a priori to calculate pooled proportions. Heterogeneity of studies was assessed using Cochran’s Q and I2 statistic. I2 values greater than 75% indicated very high heterogeneity (Thompson & Higgins, 2002). When I2 was greater than 75%, meta-regression analyses were conducted to examine whether there was a mediating relationship between ORs and a between-study characteristics. Age and gender were selected as a potential between-study study characteristic, as it is been widely agreed upon that younger age and male gender are associated with increased violence risk (Coid et al., 2013; Dan-Glauser et al., 2023; Dean et al., 2007; Large & Nielssen, 2011) in FEP groups. Publication year was also selected as a potential between-study characteristic, as later publication year (i.e., more recent publication year) has been found to be significantly associated with lower rates of violence (Youn et al., 2024). Publication bias was assessed using Egger’s test analysis for continuous variables, and Peters’ regression technique was used to examined publication bias for long-transformed ORs, unless between-study heterogeneity was high (I2 > 75%; van Aert et al., 2016) or there were less than 10 studies included in the analysis (Sterne et al., 2011). Outliers were identified using the find.outliers(m.gen) function; however, these studies were only reported if they appeared to be significantly contributing to the between-study heterogeneity.
Results
Search Results
A total of 4,534 studies were identified via database search, and an additional 5 studies were found through hand searching reference lists of included studies. After removing 1,785 duplicates and excluding 2,754 studies during title and abstract screening, 165 studies were selected for full text review. After the exclusion of 150 papers, 15 studies were included (Figure 1). There were a total of 3,788 participants across studies. The percentage of males in studies ranged from 51.4% (Chang et al., 2015) to 100% (Hachtel et al., 2020), and the mean age ranged between 18.5 (Harris et al., 2010) and 33.3 years (Keane et al., 2019). FEP diagnoses were generally broad and included all non-affective (e.g., schizophrenia and brief psychotic disorder) or affective (e.g., bipolar disorder and major depressive disorder with psychotic features) psychotic disorders. Diagnoses were typically made based on the DSM-IV and ICD-10 criteria. Table 1 summarizes the study details, demographic information, overall quality score, and information related to violence.
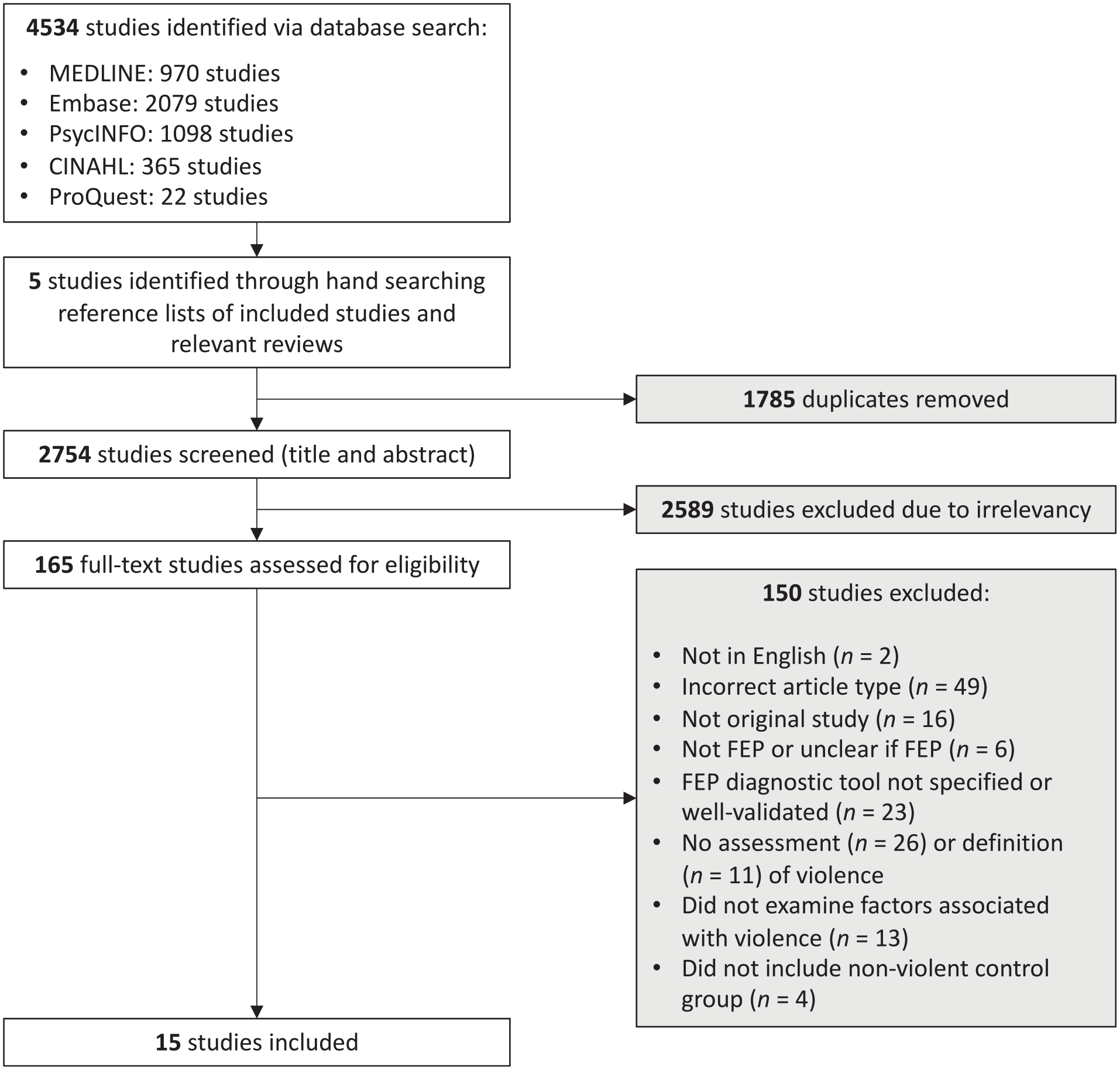
PRISMA flowchart.
Study Details, Demographics, Information Related to Violence, and Quality Score of 15 Included Studies.
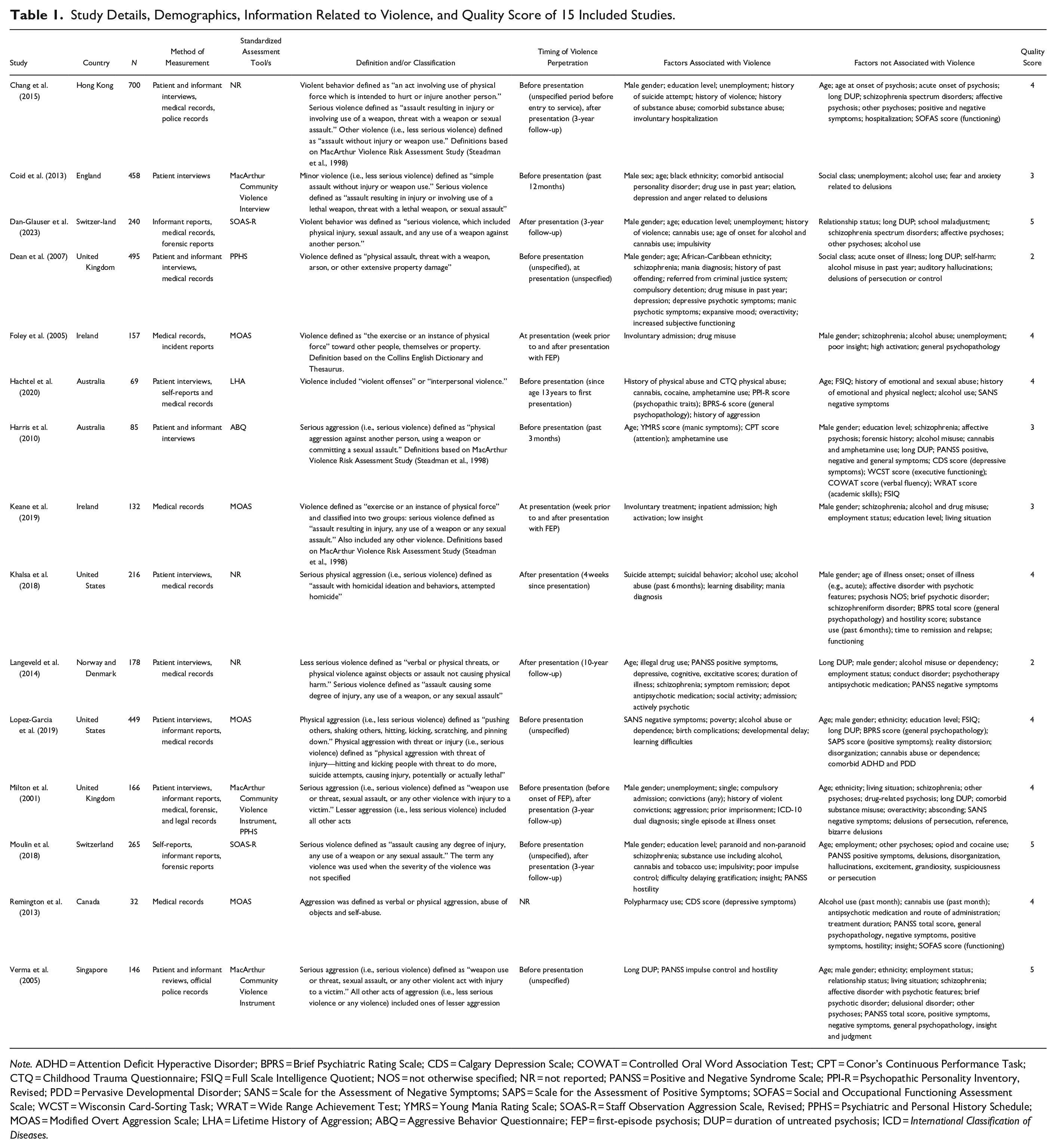
Note. ADHD = Attention Deficit Hyperactive Disorder; BPRS = Brief Psychiatric Rating Scale; CDS = Calgary Depression Scale; COWAT = Controlled Oral Word Association Test; CPT = Conor’s Continuous Performance Task; CTQ = Childhood Trauma Questionnaire; FSIQ = Full Scale Intelligence Quotient; NOS = not otherwise specified; NR = not reported; PANSS = Positive and Negative Syndrome Scale; PPI-R = Psychopathic Personality Inventory, Revised; PDD = Pervasive Developmental Disorder; SANS = Scale for the Assessment of Negative Symptoms; SAPS = Scale for the Assessment of Positive Symptoms; SOFAS = Social and Occupational Functioning Assessment Scale; WCST = Wisconsin Card-Sorting Task; WRAT = Wide Range Achievement Test; YMRS = Young Mania Rating Scale; SOAS-R = Staff Observation Aggression Scale, Revised; PPHS = Psychiatric and Personal History Schedule; MOAS = Modified Overt Aggression Scale; LHA = Lifetime History of Aggression; ABQ = Aggressive Behavior Questionnaire; FEP = first-episode psychosis; DUP = duration of untreated psychosis; ICD = International Classification of Diseases.
Quality Appraisal
The total quality score ranged between 2 (Dean et al., 2007; Langeveld et al., 2014) and 5 (Dan-Glauser et al., 2023; Moulin et al., 2022; Verma et al., 2005) out of a maximum score of 5 (average score = 3.7). Most studies provided sufficient detail about the sample, study setting, and factors associated with violence. Most studies also used appropriate statistical analyses and provided a rationale for the selected statistical methods. Several studies did not report detailed information regarding inclusion and exclusion criteria (Chang et al., 2015; Coid et al., 2013; Dean et al., 2007; Foley et al., 2005; Harris et al., 2010; Keane et al., 2019; Langeveld et al., 2014; Milton et al., 2001), and only six studies used standardized definitions (e.g., “assault causing any degree of injury, any use of weapon or any sexual assault”) and well-validated tools to measure violence (Chang et al., 2015; Dan-Glauser et al., 2023; Foley et al., 2005; Milton et al., 2001; Moulin et al., 2022; Verma et al., 2005).
Meta-Analysis of Factors Associated with Violence According to Severity
Any Violence
A total of 28 variables were extracted (Table 2). Male gender and non-white ethnicity were weakly associated with an increased risk of any violence. There was a strong relationship between having a history of violence and violence perpetration, at any time point. The following factors were not associated with any violence across all time points: age, living alone, being single, being unemployed, or education level.
Association Between Risk Factors and Any Violence, at Any Time Point.
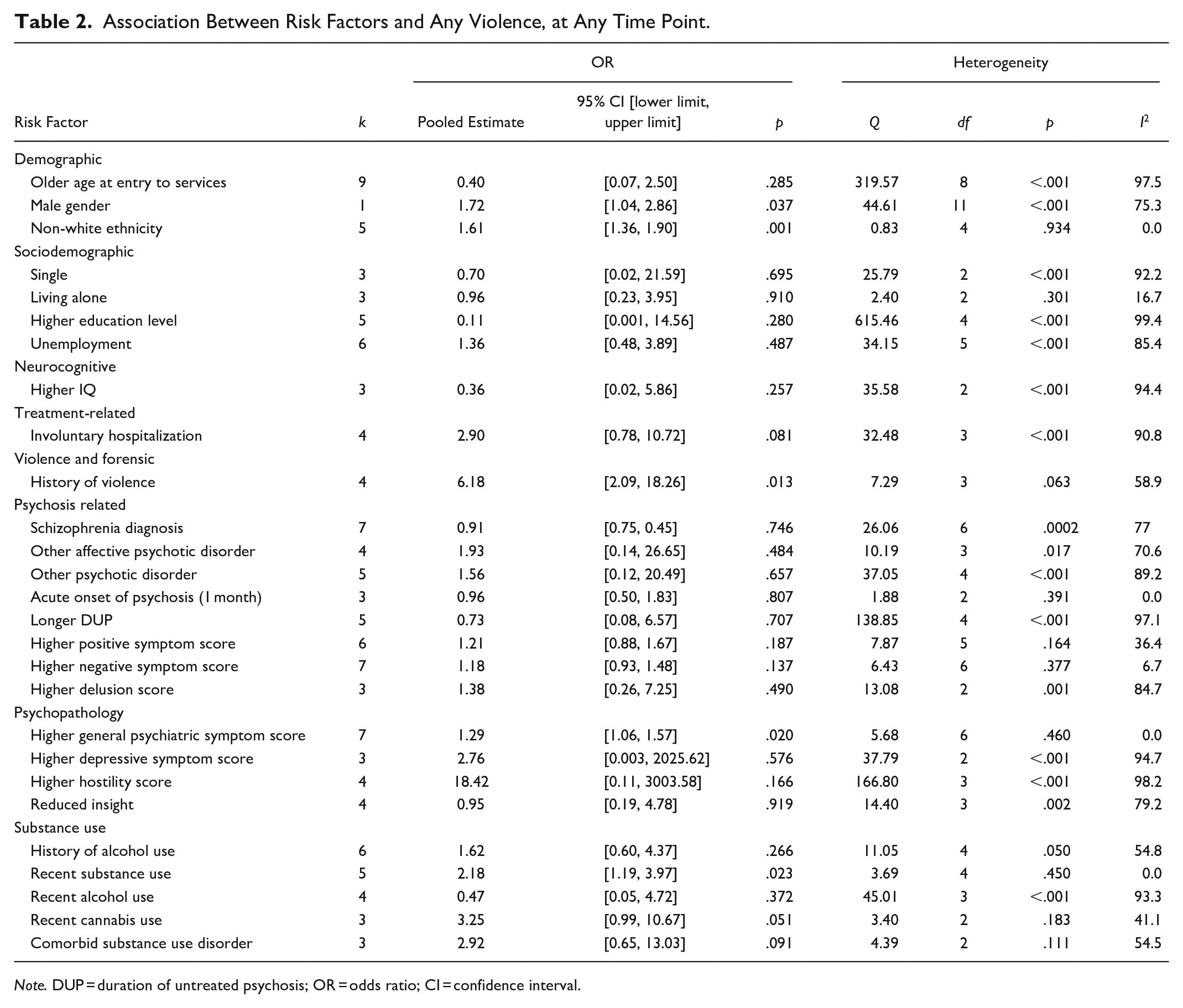
Note. DUP = duration of untreated psychosis; OR = odds ratio; CI = confidence interval.
No particular psychotic disorder was associated with violence. The following factors were also not associated with violence: reduced insight, delusions, positive symptoms, and negative symptoms. While violence was not associated with longer DUP, age mediated the relationship between DUP and violence (k = 3, β = .04, 95% CI [0.03, 0.26]).
General psychiatric symptoms were significantly, but weakly associated with violence. Depressive symptoms and involuntary hospitalization at entry to services were not associated with violence risk. For impulsivity, one study (Verma et al., 2005) was removed from analysis, as it led to a very large confidence interval (95% CI [0.001, 12511381.11]), due to the variability in how impulsivity was measured. After the removal of this study, as there were only two studies remaining (i.e., did not meet the minimum requirement of three studies), impulsivity was removed from further analyses.
Violence was weakly associated with recent substance use. There was no association between violence and the following: comorbid substance use disorder, history of alcohol use, recent alcohol use, or recent cannabis use. Although there was no significant association between violence and recent alcohol use, according to meta-regression analyses, age had a significant influence on the association between violence and recent alcohol use (k = 4, β = −.41, 95% CI [−0.57, −0.25]).
There was no association between Full Scale Intelligence Quotient (FSIQ) and violence, based on three studies (Hachtel et al., 2020; Harris et al., 2010; Lopez-Garcia et al., 2019).
Serious Violence
The relationship between serious violence and 11 variables (see Supplemental Table 3) were examined; however, there were no significant associations. There were insufficient data to calculate separate pooled ORs for less serious and severe violence.
Meta-Analysis of Factors Associated with Violence According to Timing
Before Presentation to Services
Only general psychopathology was weakly associated with violence perpetrated before presentation to services. The following variables were not associated with violence committed before treatment initiation: age, gender, FSIQ, schizophrenia disorder, other affective psychotic disorder, longer DUP, positive symptoms, and negative symptoms (see Supplemental Table 4).
At First Presentation to Services
Only male gender was weakly associated with violence committed at first presentation to services. Unemployment, schizophrenia disorder, history of alcohol use, and recent substance use were not associated with violence during this time point (see Supplemental Table 5).
Following Treatment Initiation
Male gender and unemployment at entry were moderately associated with an increased risk of violence perpetration after treatment initiation (see Supplemental Table 6).
Discussion
It is a common public myth that individuals with psychotic disorders are inherently violent. Our work has been important for providing an updated description of rates (see Youn et al., 2024), characteristics, and correlates of violence in individuals with FEP. The current review and meta-analysis is the first of its kind in a decade examining a broad range of risk factors associated with overall violence, as well as differences according to severity and timing of violence perpetration.
Regarding correlates of violence, our analysis that included any violence regardless of severity and across all time points revealed that male gender, non-white ethnicity, history of violence, recent substance use, and more severe general psychiatric symptoms were significantly associated with violent behavior. These findings are largely consistent with previous studies (Chang et al., 2015; Large & Nielssen, 2011; Látalová, 2014). However, some previously reported risk factors were not significant in the current study. For example, the earlier review by Large and Neilssen (2011) reported both involuntary treatment and lower education to be associated with any violence, a finding not replicated here. This discrepancy may be because our study focused on involuntary hospital inpatient admissions only, whereas the study by Large and Nielssen (2011) examined involuntary treatment more generally, likely including outpatient community-based interventions, thus confounding comparisons across studies.
Consistent with previous reports (Chang et al., 2015; Large & Nielssen, 2011), a history of violence emerged as the strongest risk factor. Individuals who committed violence during their FEP were over six times more likely to have a history of violence compared to those who did not engage in violent behavior. Recent substance use emerged as the next strongest risk factor, suggesting the importance of considering the recency of substance use, and its variability in risk according to timing. Although we could not investigate this further due to limitations of the data, previous studies have consistently identified substance use as a strong risk factor for violence (Foley et al., 2005; Langeveld et al., 2014; Nielssen et al., 2012), with much of the violence thought to be due to comorbid substance use (Foley et al., 2005). Substance use is a known risk factor for violence regardless of both treatment status (Elbogen & Johnson, 2009; Fazel et al., 2009b; Foley et al., 2005; Milton et al., 2001) and stage of illness, up to 10 years following initial presentation to services (Langeveld et al., 2014). Given that the rate of comorbid substance use disorders can be as high as 74% in people with FEP (Conus et al., 2007), these findings highlight the importance of targeting substance use in early intervention to reduce violence risk. Consistent with previous studies (Foley et al., 2005; Hachtel et al., 2020; Large & Nielssen, 2011; Verma et al., 2005), there was a relationship between violence and severity of general psychopathology, but not negative or positive symptoms. In the later stages of psychosis, general psychopathology has not been identified as a correlate of violence. However, specific symptom domains, such as positive symptoms (e.g., persecutory delusions), have been recognized for their association with violent behavior (Lamsma & Harte, 2015; Witt et al., 2013). This finding suggests that it may be important to focus on phase-specific risk factors unique to FEP.
The second major finding of this study was that correlates varied as a function of timing of violence. When comparing any severity of violence across different time points, general psychopathology severity was the only factor associated with violence perpetrated before presenting to services, while male gender was the only risk factor for violence committed at first presentation to services. After treatment initiation, male gender and unemployment were both significantly associated with violence. People who perpetrated violence after presenting to services were nearly three times more likely to have been unemployed, compared to those who were not violent after treatment initiation. This aligns with findings from previous studies, which have found a relationship between violence and unemployment in both people with (Černý et al., 2018; Chang et al., 2015; Milton et al., 2001; Rolin et al., 2019) and without psychosis (Jawadi et al., 2021; Mauri et al., 2019). The protective nature of employment has been less commonly reported within the violence and FEP literature; however, the current findings reinforce the importance of incorporating vocational interventions as part of recovery for people with psychosis, as this may not only reduce violence risk, but also other outcomes that are associated with violence, such as treatment delay (Marion-Veyron et al., 2015), more severe positive symptoms, and disruptions in the continuity of care (Ramsay Wan et al., 2014; Victoria, 2021).
Third, risk factors varied according to the severity of violence. Due to insufficient data, separate pooled ORs could not be calculated for less serious and severe violence. Interestingly, we found no significant associations between any potential risk factors examined here and serious violence. This was in contrast to an earlier review (Large & Nielssen, 2011), which found an association between serious violence and forensic history, longer DUP and higher global symptom scores. This is likely because the previous review (Large & Nielssen, 2011) examined forensic history broadly (including both history of violence and criminal convictions), whereas in the present study, forensic and violence history were separated into two variables. This was due to several studies having non-independent samples, and also, as we believe that past criminal convictions and violence history are in fact separate constructs. Our negative findings for DUP and violence are not supported by other meta-analytic studies (Large & Nielssen, 2008, 2011); however, they do reflect those of an earlier systematic review (Látalová, 2014). These discrepancies may be due to differences in how DUP is defined across studies (Látalová, 2014); although DUP typically refers to the time between the onset of psychosis and the start of treatment, determining DUP is not straightforward, as the onset of psychotic symptoms and treatment initiation are defined in various ways (Beiser et al., 1993; Polari et al., 2011), leading to difficulties when interpreting particularly positive findings. For example, one study (Verma et al., 2005) found an association between violence and DUP in people with FEP; however, it concluded that it was difficult to clearly identify the exact age of illness onset and when the violence occurred. Hence, there is a possibility that some incidents of violence occurred before illness onset, confounding the relationship between violence and DUP (Látalová, 2014).
Fourth, there was high between-study heterogeneity for several pooled ORs. Confidence intervals were also notably large, with the width of confidence intervals being up to 6876.39. These findings are likely reflective of the large variability in study methodology, including the definition and measurement of violence, as well as risk factors. Among the included studies, the definition of violence was inconsistent, based on a range of different data sources (e.g., patient report via interview and official police records). Only a small number of studies used standardized definitions (e.g., “assault causing any injury, any use of weapon or any sexual assault”) and well-validated diagnostic criteria (e.g., DSM-5). These inconsistencies have been found repeatedly across reviews (Douglas et al., 2009; Youn et al., 2024) and make it challenging to determine whether the associations between violence and potential risk factors are influenced by methodological factors, except in cases where additional analyses are conducted. For example, the use of standardized measures (e.g., Modified Overt Aggression Scale, Psychiatric and Personal History Schedule) can lead to increased reporting of violence compared to unstructured measures (35% vs. 26%). In comparison, self-reports are known to be associated with higher reported rates of violence (34%) compared to case notes (31%) or criminal records (27%; Winsper et al., 2013). Future research would benefit from the use of standardized methods for measuring/assessing both violence and risk factors, and also account for methodological factors (e.g., measurement tools) that may be contributing to this between-study heterogeneity.
Clinical Implications and Future Directions
Most risk factors identified in this study are also associated with violence in the general community and non-FEP clinical populations (Witt et al., 2013), with the exception of higher general psychopathology. For example, male gender (Iozzino et al, 2015), history of violence, unemployment (Jawadi et al., 2021; Mauri et al., 2019), and substance use (Brook et al., 2003; Fazel et al., 2018; Iozzino et al., 2015) have also been identified as common risk factors of violence in non-clinical community samples, or those with mental illnesses other than schizophrenia. Therefore, these risk factors alone cannot explain why the prevalence of violence is higher in people with FEP, and further research is needed to identify what differentiates FEP groups from non-FEP groups. It may also be important to consider other risk factors of violence that have been found in broader, non-FEP populations, but have not been explored in our review, such as antisocial personality disorder (de Barros & de Pádua Serafim, 2008; Fazel et al., 2018; Yu et al., 2012), psychopathy (Aharoni & Kiehl, 2013; Coid & Yang, 2011; Neumann & Hare, 2008; Reidy et al., 2011), and history of sexual, physical and/or emotional abuse (Babchishin et al., 2015; Fazel et al., 2018; Jespersen et al., 2009; Smith-Marek et al., 2015). Although it was surprising that these variables did not emerge as risk factors in our study, this is likely because they have not yet been commonly explored in the violence and FEP literature. Future studies are encouraged to investigate these risk factors to determine whether these variables are also associated with violence in FEP populations or are unique to general community and other clinical cohorts.
Some of the risk factors identified in this study are also associated with psychosis generally. For instance, substance misuse has been commonly identified as a risk factor for violence among FEP groups (Foley et al., 2005; Langeveld et al., 2014; Nielssen et al., 2012); however, it is also significantly associated with the increased risk of developing psychosis (Janoutová et al., 2016), and poorer outcomes such as failure to achieve symptom remission (Lambert et al., 2005). One review (Lamsma & Harte, 2015) identified 41 potential causal pathways to violence in people with psychosis, highlighting the complex and interconnected nature of these relationships; however, this is yet to be explored in FEP populations specifically, and compared across stages of illness. An investigation of these relationships may help determine whether psychosis-specific factors and/or other more generic risk factors are contributing to the increased risk of violence during FEP.
A social determinants framework can also be useful for understanding risk of violence and psychosis (Anglin, 2023; Fusar-Poli et al., 2023; Jester et al., 2023). Substance use, non-white ethnicity, and unemployment are also common factors within marginalized groups experiencing social inequalities such as racial discrimination and poverty. This suggests that the increased risk for violence in psychosis cannot be purely attributed to the illness itself, and must be explored in relation to other systemic factors, which are likely contributing to the increased prevalence of violence (Fusar-Poli et al., 2023; Stuart, 2003). A government audit in the United Kingdom found that people from non-white ethnic backgrounds were more likely to access mental health services via forensic services, compared to those from white ethnic backgrounds (Cabinet Office London, 2017). On this basis, it may not be the risk factor (i.e., non-white ethnicity) itself that leads to a higher rate of contact with criminal justice services, but also the social inequalities around race.
One way of addressing the increased risk of violence is adopting a multidisciplinary approach to treatment. Such an approach would integrate mental health, criminal justice, vocational services, and drug and alcohol programs, acknowledging the interconnected relationship between male gender, substance use, unemployment (Patel et al., 2016; Sara et al., 2013), and violence. It is strongly recommended that employment is prioritized, as unemployment can be a significant risk factor for substance use (Henkel, 2011) and economic insecurity, which can, in turn, lead to higher rates of violence as a means to meet financial needs (Fagan & Freeman, 1999; Morgan & Boxall, 2022; Pah et al., 2017). Unemployment can also allow more time to engage in violent behavior (Schleimer et al., 2022) and reduce opportunities to create meaningful relationships with others, a known protective factor for violence risk (Sampson & Laub, 1990).
Finally, another effective method for addressing the high prevalence of violence is the early identification of people at increased risk of perpetrating violence. Implementing brief screeners or standardized risk assessment tools, such as the Historical Clinical and Risk Management (HCR-20; Webster et al., 1997) and Oxford Mental Illness and Violence tool (OxMIV; Whiting et al., 2023) across various settings (e.g., criminal justice, mental health services, and hospitals), can help determine the overall level of violence risk before it occurs, potentially at initial contact with services. These assessment tools consider a wide range of risk factors identified in this review, and other studies. By identifying individuals at greater risk, early intervention strategies can be employed to reduce the likelihood of future violence.
Strengths and Limitations
A major strength of the study was that we examined a broad range of risk factors and further separated these variables based on the recency and type of risk factors. We also separated violence according to severity and timing, which allowed us to conduct more detailed analyses. In terms of limitations, first, we did not examine inter-relationships between risk factors. The relationship between variables is known to be complex, with some studies identifying 41 possible causal pathways to violence (Lamsma & Harte, 2015). However, this was beyond the scope of the review, and we were limited by the small number of studies, which also impacted our ability to conduct sub-analyses on all variables. Second, although we included age, gender, and publication year as potential sources of between-study heterogeneity, in the broader psychosis literature, it has been suggested that it is important to also consider factors such as diagnosis and methodological differences, such as study setting, and the measurement of violence (Douglas et al., 2009). Third, due to the strict inclusion/exclusion criteria around diagnosis, some relevant studies may have been excluded. However, we believe a stricter approach was necessary to allow for consistency across studies, and to ensure that diagnoses are made using well-validated, standardized tools, particularly given diagnoses can be unstable in early stages of illness (Fusar-Poli et al., 2016; Wood et al., 2021).
Critical Findings
Risk factors varied according to the timing and severity of violence.
Risk factors included male gender, non-white ethnicity, history of violence, recent substance use, general psychopathology, and unemployment.
The identified risk factors are also known to be associated with psychosis generally, as well as violence in the general population.
Implications
Future studies should explore the inter-relationships between risk factors and variables associated with violence in non-FEP and general populations.
Risk factors should be interpreted in relation to broader, systemic factors such as social determinants.
A multidisciplinary approach to treatment including mental health, criminal justice, vocational services, and drug and alcohol programs, is recommended.
Supplemental Material
sj-docx-1-tva-10.1177_15248380241309297 – Supplemental material for Systematic Review and Meta-Analysis: Risk Factors of Violence During First-Episode Psychosis
Supplemental material, sj-docx-1-tva-10.1177_15248380241309297 for Systematic Review and Meta-Analysis: Risk Factors of Violence During First-Episode Psychosis by Sarah Youn, Amity E. Watson, Belinda L. Guadagno, Sean Murrihy, Linda K. Byrne, Nicholas Cheng and Sue M. Cotton in Trauma, Violence, & Abuse
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Deakin University Postgraduate Research Scholarship (DUPRS).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.