
Abstract
Child maltreatment (CM) poses significant risks to victims, resulting in enduring physical, psychological, and developmental consequences. Adult survivors of CM seem especially vulnerable to perinatal complications. However, existing research on perinatal outcomes presents mixed results and relies heavily on self-reported data, which may not align with official medical data. Hence, a systematic review using official health data may provide clarity on this association; it may orient future research and the provision of perinatal services. This scoping review aimed to synthesize and evaluate the quality of the literature that utilizes official health data to explore associations between CM and perinatal complications. Following Arksey and O’Malley’s model, searches across four databases (PsycINFO, MEDLINE, Scopus, and ProQuest Dissertations/Thesis) produced 8,870 articles. After screening, 23 articles met the inclusion criteria (e.g., recorded perinatal complications using official health data, and peer-reviewed studies or dissertation). Evidence indicates CM survivors have less prenatal care visits, more fetal loss and preterm births, lower gestational age, and increases in emergency cesarean sections. Adults had more cervical insufficiency, lower episiotomies and sphincter ruptures, and overall pregnancy and postpartum complications while adolescents had lower Apgar scores. No associations were observed on other outcomes (e.g., vaginal bleeding, group B streptococcus, and fetal distress). Mixed findings emerged for other perinatal and maternal health concerns such as birth weight and blood pressure. CM survivors may face an increased risk of experiencing perinatal complications. Findings point to the relevance of leveraging health data for CM research and adopting trauma-informed practices in perinatal services.
Roughly 16.5 out of every 1,000 North American children are victims of child maltreatment before the age of 18 (CM; physical, emotional, and sexual abuse, physical and emotional neglect by a caregiver, and exposure to domestic violence; Fallon et al., 2022; U.S. Department of Health & Human Services Administration for Children and Families, 2021). Survivors of CM seem at increased risk of experiencing perinatal complications, defined as medical conditions that may affect the mother or the fetus’s health during pregnancy, childbirth, and postpartum (Centers for Disease Control and Prevention, 2023). Examples are preterm births, gestational diabetes, miscarriages, sepsis, low-birth-weight, and infant feeding issues (Kerkar et al., 2021; Kern, Khoury, et al., 2022; Lev-Wiesel & Daphna-Tekoa, 2007; Möhler et al., 2008; Nesari et al., 2018; Souch et al., 2022). Previous reviews on CM and perinatal complications have provided conflicting findings, often focusing primarily on low-birth-weight and preterm births (Kern, Khoury, et al., 2022, Nesari et al., 2018, Souch et al., 2022; Madkour et al., 2014). These inconclusive results may be due to limited studies assessing CM intricacies (i.e., specific forms of CM, poly-victimization, severity, and frequency), which have been documented to be related to specific perinatal complications. For instance, survivors of child sexual abuse experience increased pregnancy-related hospitalizations and premature births (Leeners et al., 2010; Selk et al., 2016) and all forms of CM, except physical abuse and emotional neglect, have been shown to increase the odds of overall perinatal complications, even after adjusting for factors like psychiatric disorders (Shamblaw et al., 2021). Inconclusive findings from past reviews might also stem from an over-reliance on self-reports. For instance, recalling preeclampsia, eclampsia, late-onset preeclampsia, gestational hypertension, and vaginal bleeding during pregnancy (Bryant et al., 1989; Coolman et al., 2010; Liu et al., 2013; Seoane et al., 1998; Sou et al., 2006) and details about delivery methods and infant information have been shown to misalign with medical records, especially when assessed years after pregnancy (Boeke et al., 2012; Liu et al., 2013).
Using official health data to explore relationships between all forms of CM and perinatal complications is vital due to the limitations of self-reporting and may provide clarity regarding inconsistent findings from past research. Thus, this systematic scoping review aims to: (a) synthesize existing evidence on the associations between CM and perinatal complications as measured using official health data, and (b) systematically assess the methodological quality of this body of research. This will deepen our understanding of these associations while pinpointing existing gaps to fill in future research and providing an up-to-date snapshot for medical professionals wishing to better address the needs of CM survivors seeking perinatal care. Ultimately, this may result in reducing pregnancy complications for CM survivors.
Methods
The five-stage framework, established by Arksey and O’Malley (2005), was followed to ensure rigor and reduce bias and error. The stages included: (a) identification of the research problem, (b) identification of relevant studies, (c) selection of studies, (d) charting the data, and (e) collating, summarizing, and reporting the results. Additionally, a systematic evaluation of the methodological quality of included studies was performed.
Identification of Relevant Studies
The search strategy was created in collaboration with a librarian and was executed on April 13th, 2023, in databases PsycINFO (Ovid; 1806-Present), MEDLINE (Ovid; 1946-Present), Scopus, and ProQuest Dissertations and Thesis Global. Search terms were combined with Boolean logic (e.g., child maltreatment, abuse, pregnancy, obstetrical complications, outcomes, premature birth, and birth weight). See Supplemental Appendix A for the search strategy.
Inclusion/Exclusion Criteria
Peer-reviewed articles and dissertations were included if they: (a) measured participants’ history of CM (defined as physical, emotional, and sexual abuse, physical and emotional neglect by a caregiver, and exposure to domestic violence before the age of 18); (b) included participants with at least one lifetime pregnancy; (c) statistically examined relationships between maternal CM and pregnancy, labor and childbirth, or postpartum complications; and (d) recorded perinatal complications (pregnancy to a year post-delivery) using official health data. Studies were excluded if participants’ history of trauma was unclear (e.g., not able to distinguish between CM and other traumatic experiences) or if they were not published in French or English. No other restrictions were made on setting, date, or study design.
Selection of Studies
Articles meeting criteria were imported into Rayyan software (Ouzzani et al., 2016). Two raters independently screened titles and abstracts, achieving complete agreement through discussion. Subsequently, one researcher screened the full-text articles.
Charting the Data and Collating, Summarizing, and Reporting the Results
Data was extracted from full-text articles covering: (a) study aims, (b) design, (c) sample details, (d) relevant measures related to CM, perinatal outcomes, and official health data type, and (e), principal results, and relevant covariates. Following Levac et al. (2010), a narrative synthesis method was applied, identifying common themes and patterns across studies, and was then followed by the results being reported in a narrative format.
Methodological Quality Assessment
All the selected articles underwent critical appraisal by two independent raters using The National Heart, Lung, and Blood Institute’s Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies (NHLBI; National Heart, Lung, and Blood Institute, National Institutes of Health, 2014). The NHLBI assesses the sampling procedure, reliability and validity of the measures, data analysis, and covariates. Global quality ratings were designated as good, fair, and poor. Discrepancies were resolved through discussion.
Results
The preliminary search generated 8,870 articles. After deduplication, 7,517 articles were screened for abstract and title eligibility and 7,452 articles were excluded, leaving 65 articles for full-text examination; 21 articles remained. Additional searching in the reference sections of the included articles produced two more articles for a final sample of 23 included articles (see Figure 1 for the PRISMA flow diagram which includes detailed reasons for exclusions and Table 1 for summaries of the included studies).
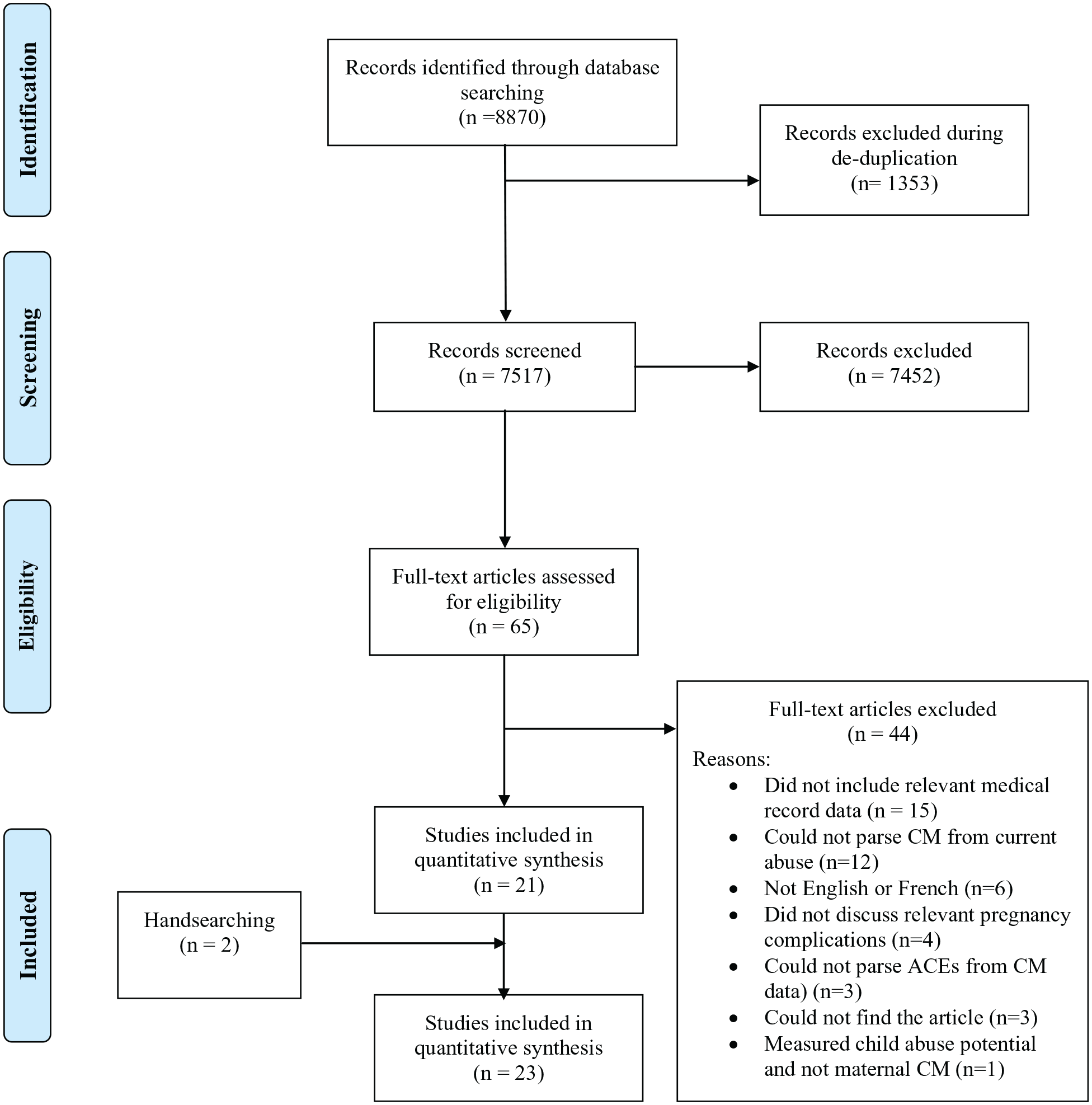
PRISMA flow diagram demonstrating identification and screening process.
Summary of Included Studies.
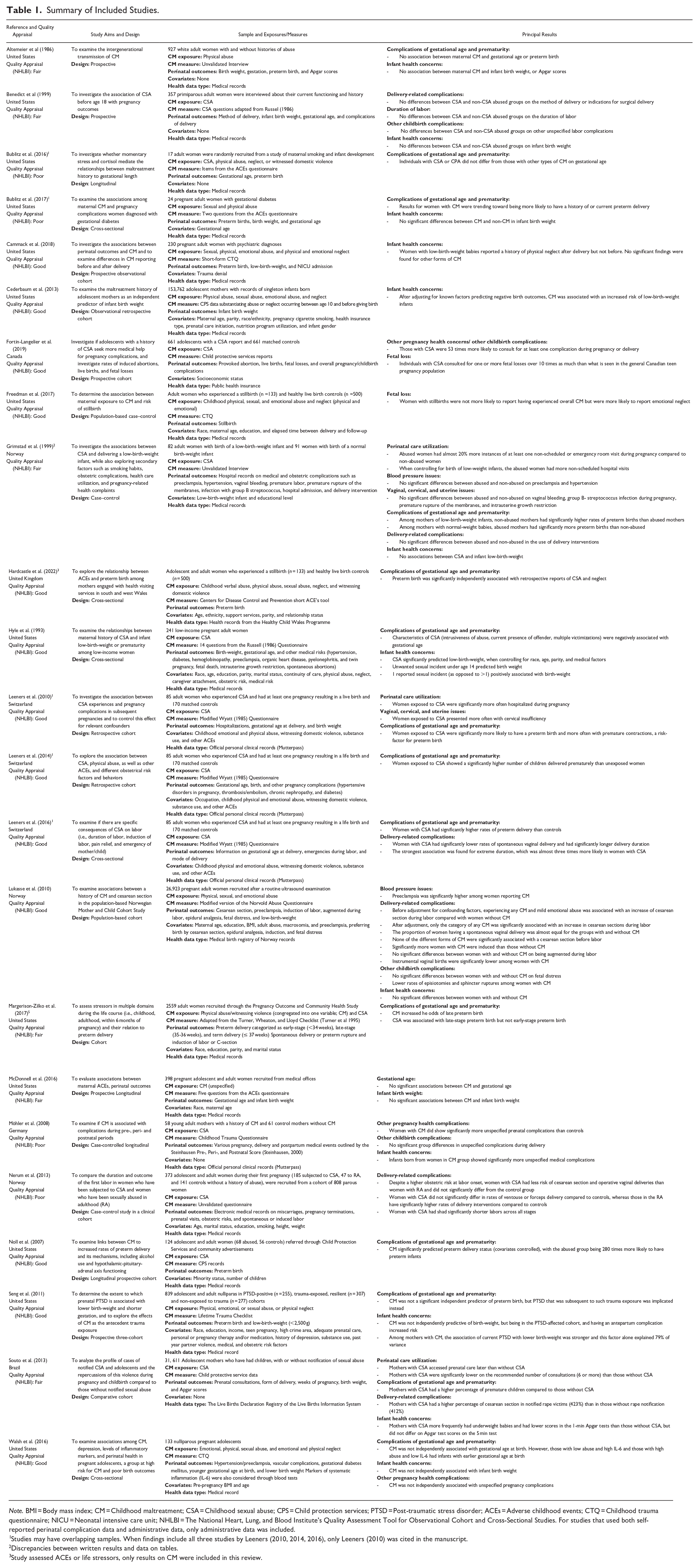
Note. BMI = Body mass index; CM = Childhood maltreatment; CSA = Childhood sexual abuse; CPS = Child protection services; PTSD = Post-traumatic stress disorder; ACEs = Adverse childhood events; CTQ = Childhood trauma questionnaire; NICU = Neonatal intensive care unit; NHLBI = The National Heart, Lung, and Blood Institute’s Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies. For studies that used both self-reported perinatal complication data and administrative data, only administrative data was included.
Studies may have overlapping samples. When findings include all three studies by Leeners (2010, 2014, 2016), only Leeners (2010) was cited in the manuscript.
Discrepancies between written results and data on tables.
Study assessed ACEs or life stressors, only results on CM were included in this review.
Four studies (17%) only included participants under age 18, 14 (61%) studies only included adults, and 5 (22%) studies used both adolescent and adult participants. Only four (17%) adopted a longitudinal design, with most studies being cross-sectional (n = 19; 83%). In terms of geographical locations, 14 studies were from North America (61%; 13 from the United States, one from Canada); eight (35%) derived from Europe (three (13%) from Norway, three (13%) from Switzerland, one (4%) from the United Kingdom, and one (4%) from Germany); and one study (4%) was from South America (Brazil). Sample sizes ranged from less than 100 (n = 2, 9%), between 100 and 500 (n = 7, 30%), to over 500 participants (n = 14, 61%).
Three main themes emerged from included studies: (a) pregnancy complications (n = 8); (b) labor and childbirth complications (n = 18); and c) puerperium and postpartum complications (n = 13). See Supplemental Appendix B for a summary of the themes.
Pregnancy Complications (n = 8)
Eight studies (adult-only samples n = 5; adolescent-only samples n = 3) examined pregnancy complications which included prenatal care utilization (n = 3), vaginal, cervical, and uterine complications (n = 2), blood pressure issues (n = 2), fetal loss (n = 2), and other pregnancy health complications (n = 4).
Prenatal Care Utilization (n = 3)
Evidence from the included studies suggests that adolescents with CM histories are more likely than non-abused adolescents to delay seeking prenatal care and less likely to obtain the recommended six or more consultations (Souto et al., 2017). Findings support that adult CM survivors are also more likely to have at least one non-scheduled visit, and have significantly more triage visits and hospitalizations during their pregnancies (Grimstad & Schei, 1999; Leeners et al., 2010).
Vaginal, Cervical, and Uterine Issues (n = 2)
Studies investigating vaginal bleeding during adult pregnancy found no significant differences between CM and non-CM groups (Grimstad & Schei, 1999). Limited data on vaginal or endocervical pathogens found that adult CM survivors reported no observed disparities concerning group B streptococcus infection during pregnancy (Grimstad and Schei, 1999). Findings insinuated that there are no group differences between abused and non-abused individuals on premature rupturing of the membranes during pregnancy or intrauterine growth retardation for adults (Grimstad & Schei, 1999), but did suggest that adults with CSA histories presented more often with cervical insufficiency. (Leeners et al., 2010).
Blood Pressure Issues (n = 2)
Mixed findings emerged for blood pressure issues in adult samples. Findings propose that histories of CM are not associated with diagnoses of preeclampsia and hypertension (Grimstad & Schei, 1999), while others note higher preeclampsia in pregnant women reporting CM (Lukasse et al., 2010).
Fetal Loss (n = 2)
Limited information on fetal loss showcased some evidence toward associations between CM and fetal losses, suggesting that adult CM survivors, particularly those with emotional neglect, are more likely to report a fetal loss (Freedman et al. 2017). Additionally, abused adolescents with CM are approximately ten times more likely than the Canadian teenage pregnancy population to seek out a consultation for one or more fetal loss (Fortin-Langelier, 2019).
Unspecified Pregnancy Complications (n = 4)
Adult CM survivors reported higher rates of overall pregnancy complications (Leeners et al., 2010; Möhler et al., 2008). Studies revealed mixed findings for unspecified complications in adolescents, with some findings higher rates of complications (Fortin-Langelier et al., 2019;) while others did not (Walsh et al., 2016).
Labor and Childbirth Complications (n = 18)
Eighteen studies (adult-only samples n = 9; adolescent-only samples n = 3, combined samples n = 5) investigated labor and childbirth complications including complications of gestational age and prematurity (n = 13), delivery-related complications (n = 6), and other childbirth complications (n = 4).
Gestational Age and Preterm Births (n = 13)
CM survivors are more prone to experiencing preterm births compared to those without CM (adult samples: Grimstad & Schei, 1999; Leeners et al., 2010; Margerison-Zilko et al., 2017; adolescent samples: Souto et al., 2017; combined adult/adolescent samples: Hardcastle et al., 2022; Noll et al., 2007). Some evidence for nonsignificant associations between preterm births and overall CM or physical abuse emerged in samples with adults (Altemeier et al., 1986; Bublitz et al., 2017), adolescents (McDonnell & Valentino, 2016), as well as combined adult and adolescent samples but became significant associations with the addition of mediators, such as the presence of post-traumatic stress disorder after CM-related trauma (Seng et al., 2011).
Inconclusive evidence regarding gestational age at birth appeared, with some studies not finding clear group differences or direct relationships in adults (Altemeier et al., 1986; Bublitz et al, 2016;) and combined adolescent and adult (McDonnell & Valentino, 2016) samples, while others found relationships when investigating nuances such as younger gestational age in teens (Walsh et al., 2016) and specific CM histories, including the severity and frequency of abuse and the current presence of the abuser in adults (Hyle, 1993).
Delivery-Related Complications (n = 6)
Studies found that adult (Lukasse et al., 2010) and adolescent (Souto et al., 2017) CM survivors are more likely than those without CM to undergo cesarean sections, particularly emergency cesarean sections, during labor but did not find significant differences in elective cesarean sections in adult (Lukasse et al., 2010) and combined adolescent and adult (Nerum et al., 2013) samples. Mixed findings appeared for spontaneous vaginal delivery, in that CSA was associated with higher rates of spontaneous vaginal delivery in adults (Leeners et al., 2016), potentially due to a higher prevalence of cesarean sections among this group, and that rates of spontaneous vaginal delivery are almost equal between adult CM and non-CM groups (Lukasse et al. 2010). No noteworthy differences between adult groups across all the various delivery methods were reported (Benedict et al.,1999).
No clear consensus emerged given CM’s impact on various delivery interventions. Adult CM survivors do not exhibit higher rates of overall delivery interventions (Grimstad & Schei, 1999), are less likely to undergo augmentation during labor but are more frequently induced than those without CM histories (Lukasse et al., 2010). Findings on instrumental deliveries in adult and adolescent samples found no differences in rates of ventouse or forceps deliveries (Nerum et al., 2013), and lower rates of instrumental deliveries among adult CM survivors also being reported (Lukasse et al., 2010).
For duration of labor, specifically for adult women who experienced child sexual abuse, no clear pattern emerged with studies reporting longer labor, particularly in extreme durations (Leeners et al., 2016), shorter labor durations (Nerum et al., 2013) and no significant differences in labor durations (Benedict et al., 1999).
Other Childbirth Complications (n = 4)
The included studies also revealed interesting but inconclusive information about various other childbirth complications. For instance, adult CM survivors do not differ significantly from those without CM on medically reported fetal distress but do exhibit significantly lower rates of episiotomies and sphincter ruptures (Lukasse et al., 2010). For reports on unspecified labor complications, no significant differences were found between adults with and without CM experiences (Benedict et al., 1999; Möhler et al., 2008) but adolescent child sexual abuse survivors more frequently have at least one complication (Fortin-Langelier et al., 2019). It is important to note that this result was based on an aggregate variable that included both pregnancy and delivery complications, which may have skewed results.
Puerperium and Postpartum Complications (n = 13)
Thirteen studies (adult-only samples; n = 8; adolescent-only samples; n = 3, combined samples n = 2) discussed puerperium and postpartum complications, particularly related to infant health concerns (n = 13)
Infant Health Concerns (n = 13)
Conflicting evidence emerged regarding infant weight and size. Low-weight babies were found in studies with CM survivors samples investigating adults (Cammack et al., 2018; Hyle, 1993), combined adolescent/adult (McDonnell & Valentino, 2016; Seng et al., 2011; ), and adolescent-only (Cederbaum et al., 2013; Souto et al., 2017) samples. Conversely, other studies did not find differences in infant birth weight between those with and without CM histories in adults (Benedict et al., 1999; Bublitz et al., 2017; Grimstad & Schei, 1999; Lukasse et al., 2010), combined adolescent/adult (McDonnell & Valentino, 2016) and adolescent (Walsh et al., 2016) samples. One study (Cammack et al., 2018) did not precisely discern differences between CM and non-CM groups but mentioned that adult women who have low-birth-weight infants significantly reported childhood physical neglect after delivery. This difference was not apparent for CM reports measured before delivery.
Infants born to adolescent CM survivors had lower 1-min Apgar scores (Souto et al., 2017) but the same association was not found in adult samples (Altemeier et al., 1986). Studies found that adult CM survivors’ infants have more general neonatal problems and medical complications in postpartum (Möhler et al., 2008).
Quality Assessment and Summary of Study Methods
Of the 23 studies, 13 (57%) were rated as having good methodological quality, six as fair (26%), and four as poor (17%). Studies graded as fair or poor had the following limitations: no sample size justification or power description (n = 10), did not control for important confounding variables (n = 7), did not measure different types or levels of exposure to CM (n = 6, had less than 50% eligible participation rate (n = 6), or used unvalidated or unreliable measures (n = 3).
Discussion
The goal of the current systematic scoping review was to comprehensively assess the extent and scope of the published quantitative literature using official health data on the relationships between CM and perinatal complications. The review of 23 articles revealed various prenatal and pregnancy, labor and childbirth, and puerperium and postpartum complications. Throughout various studies, substantial evidence connects CM to certain perinatal complications while presenting inconclusive findings for several others. Similarities and differences between adult and adolescent samples were also present.
Findings of the review provide convincing evidence that both adult and adolescent CM survivors are prone to delaying or having less prenatal care utilization, more fetal losses, having a higher incidence of preterm births, and an increased likelihood of emergency cesarean sections during labor. Evidence also supports that adults with CM histories experience more cervical insufficiency, lower episiotomies and sphincter ruptures, and overall pregnancy and postpartum complications while adolescents had lower Apgar scores. Past research provides potential explanations for these findings. For instance, highlighting how CM survivors delay seeking prenatal care due to triggering past abuse memories during pelvic exam (Roller 2011). The increased susceptibility of CM survivors to perinatal complications like preterm births has been associated with their tendency to engage in risky health behaviors during pregnancy, including cigarette smoking, alcohol, and drug use, and nutrition-related concerns (Chung et al., 2010; Kern, Frederickson et al., 2022, Osofsky et al., 2021; Svikis et al., 2005). Moreover, adolescents with CM are likely to engage in risky behaviors that may be related to perinatal complications (Brunton & Dryer, 2021; Diaz et al., 2020). Delays in seeking perinatal care combined with risky behaviors could result in heightened emergency room visits and may increase the risk of various health issues and pregnancy-related complications (Roelands et al., 2009). As CM survivors are more likely to experience intense pain when related to their physical health (Sachs-Ericsson et al., 2006), pain associated with childbirth may halt labor progression, necessitating consideration of emergency cesarean (Leeners et al., 2006).
While evidence points to numerous connections between CM and various perinatal complications, the included studies did not establish a clear link with other complications. Nonsignificant associations were found between CM experiences and vaginal bleeding, group B streptococcus, premature rupturing of the membranes, fetal distress, Apgar scores, and unspecified childbirth complications in adults, and in cesarean sections in combined adult and adolescent samples. However, it’s worth noting that the small number of studies on these topics limits the conclusiveness of these findings. Regardless, these findings were surprising, as premature rupturing of the membranes typically corresponds with cigarette smoking and insufficient nutrition, which are more common in CM survivors. However, previous research has shown that other factors may contribute, including genitourinary infections, overexertion, poor hygiene, anemia, breech positions of the infant, and being overweight (Choudhary et al., 2015). Therefore, it is possible that important confounding factors that could influence accurate testing of direct and indirect associations may not have been considered.
Although evidence emerged for clear associations between CM and perinatal complications, the current review failed to yield conclusive evidence on the presence of blood pressure issues, vaginal deliveries, delivery interventions, and duration of labor in adults, and overall pregnancy complications in adolescents, and low-weight births in both adults and adolescents. Inconclusive evidence was largely due to a dearth of literature or could be due to methodological factors. For instance, variations in the use of interviews, self-reported questionnaires, and official records (such as child protection service data) and differences in assessing one form of CM versus multiple forms of CM could have resulted in these variations of findings. The mixed findings concerning low-birth-weight were somewhat unexpected since we did find associations between CM and preterm birth. Preterm birth is an important factor to consider when examining low-birth-weight and is sometimes used as a covariate. However, no patterns emerged between studies that did and did not control for preterm birth, indicating that more studies are needed to better disentangle the associations between CM, low-birth-weight, and preterm births.
Comparing our findings to other reviews that use both official health and self-reported data (Kern, Khoury, et al., 2022; Nesari et al., 2018; Souch et al., 2022), there are some similarities and differences. One notable similarity is that preterm birth and infant birth weight are some of the most frequently discussed perinatal complications, and findings on these topics were mainly aligned. All three of these past reviews stated that CM might increase the likelihood of preterm birth, and Kern, Khoury, et al. (2022) and Souch et al. (2022) found mixed evidence for infant birth weight. Differences include research methodology and scope of investigation. Our review considered a wider range of perinatal complications, such as prenatal care initiation, vaginal complications, intrauterine growth retardation, method and duration of labor, and other infant health concerns, which are crucial in fully understanding CM's impact on perinatal outcomes.
However, the current review found no information on gestational diabetes, signifying that official health data research has not investigated this particular outcome. Our review employed a focused approach by exclusively considering results directly related to CM. Unlike other reviews that encompassed a broader spectrum, such as adverse childhood experiences (ACEs) (e.g., parental separation, household mental illness) or adult abuse, our specific focus on CM aimed to disentangle the unique effects on perinatal complications. This approach clarified the associations uniquely attributed to CM without potential confounding influences from other types of adverse experiences.
Strengths and Limitations
This review's notable strength lies in its exclusive use of official health data, a novel approach offering larger samples and more objectivity. Official health data also covers a broader range of perinatal complications compared to studies that solely utilize self-reports, including underrepresented aspects like hospital admissions and care utilization. An official health data approach also reduces participant burden, which is particularly important when exploring sensitive topics such as perinatal health and CM.
Although this study had many notable strengths, there were also mentionable limitations. While the included studies comprised participants from various countries, there is still a lack of diversity of participants. Most studies took place in industrialized countries, with primarily White or Black participants, and there was no study that specified if pregnant individuals identified as gender diverse. Potential variations from the diversity of countries may also have introduced healthcare system disparities (i.e., complication classification, prenatal care practices, and private versus public healthcare) that could impact outcomes. For example, in countries without universal healthcare, individuals with histories of maltreatment may encounter greater challenges in accessing perinatal medical care. Research has shown that CM survivors are more likely to experience socioeconomic disadvantages, including low income, living below the poverty line, unemployment, and lower rates of healthcare coverage (Zielinski, 2009). These socioeconomic factors can exacerbate barriers to healthcare access, potentially leading to disparities in perinatal outcomes among CM survivors. The scarcity of recent literature may have missed advancements and societal changes in CM and perinatal complications and may also hint at a move away from official health data. Another important limitation stems from methodological issues including the diversity and lack of validated measures used in assessing CM. Although (un)validated interviews can allow participants to self-report CM or express their personal understanding of CM, there remains a possibility that inclusion in the CM group was subject to the discretion of the research team. Information regarding this process was unclear and could have impacted the findings. Additionally, the inclusion of both adolescent and adult participants in several studies posed challenges in separating findings between adult and adolescent participants. A lack of thoroughly assessing CM intricacies, including diverse forms, frequencies, poly-victimization, and often overlooked childhood neglect may have also impacted findings. Other differences in study design, including longitudinal and cross-sectional methods, may have led to differences in findings and contributed to mixed or inconclusive findings. The systematic appraisal also revealed that twelve of the studies’ ratings were of good quality, sixteen of fair quality, and five of poor quality, which signifies issues with validity, rigor, and reliability.
Implications
The findings of the current review have important implications for research, medical care, psychosocial practice, and policy (see Table 2). Future research should focus on using validated measures that assess CM objectively and subjectively to further explore the complexities of CM. Past research has noted low agreement between official CM data and self-reported CM and that subjective self-reports were more strongly associated with psychopathology in youth (Francis et al., 2023). Similar findings in adult samples indicated that self-reported CM had stronger associations with psychopathology than official CM reports and that the highest rates of emotional disorders were found in participants with congruence between official and self-reported CM (Danese & Widom, 2020, 2023). Therefore, research should aim to collect CM data through various methods to decrease the likelihood of underestimating rates of CM, such as in official data (Gilbert et al., 2009), but also decrease potential recall biases, such as when self-reporting CM (Hardt et al., 2004). Also, research should leverage official health data to gain insights into potential associations between CM and perinatal complications, building upon recent studies (Brunton & Dryer, 2021; Kern, Frederickson, et al., 2022) that have started exploring how some forms of CM might increase the risk factors for pregnancy complications, especially when coupled with CM-related PTSD symptoms. Using official health data allows more ease in conducting longitudinal studies with large and diverse samples, and its objectivity may carry a more significant impact in shaping policies. Future research should explore whether the associations between CM and perinatal complications differ across different healthcare contexts and investigate potential mechanisms underlying these differences. More research is also needed on adolescent samples and comparing and contrasting differences between pregnant adult and adolescent CM survivors. Despite some inconsistent findings, healthcare providers, particularly those from the United States of America, where the bulk of the included studies were performed, can utilize the insights from this study to thoroughly assess the history of CM. This information can be used to anticipate the possibility of complications and to justify providing trauma-related interventions during pregnancy to potentially reduce CM survivors’ likelihood of engaging in behaviors that could pose risks for perinatal complications. In sum, the current review is a first step in better understanding the perinatal complications experienced by CM survivors and can give insights for enhancing practice, policy, and client care.
Summary of Critical Findings and Implications.
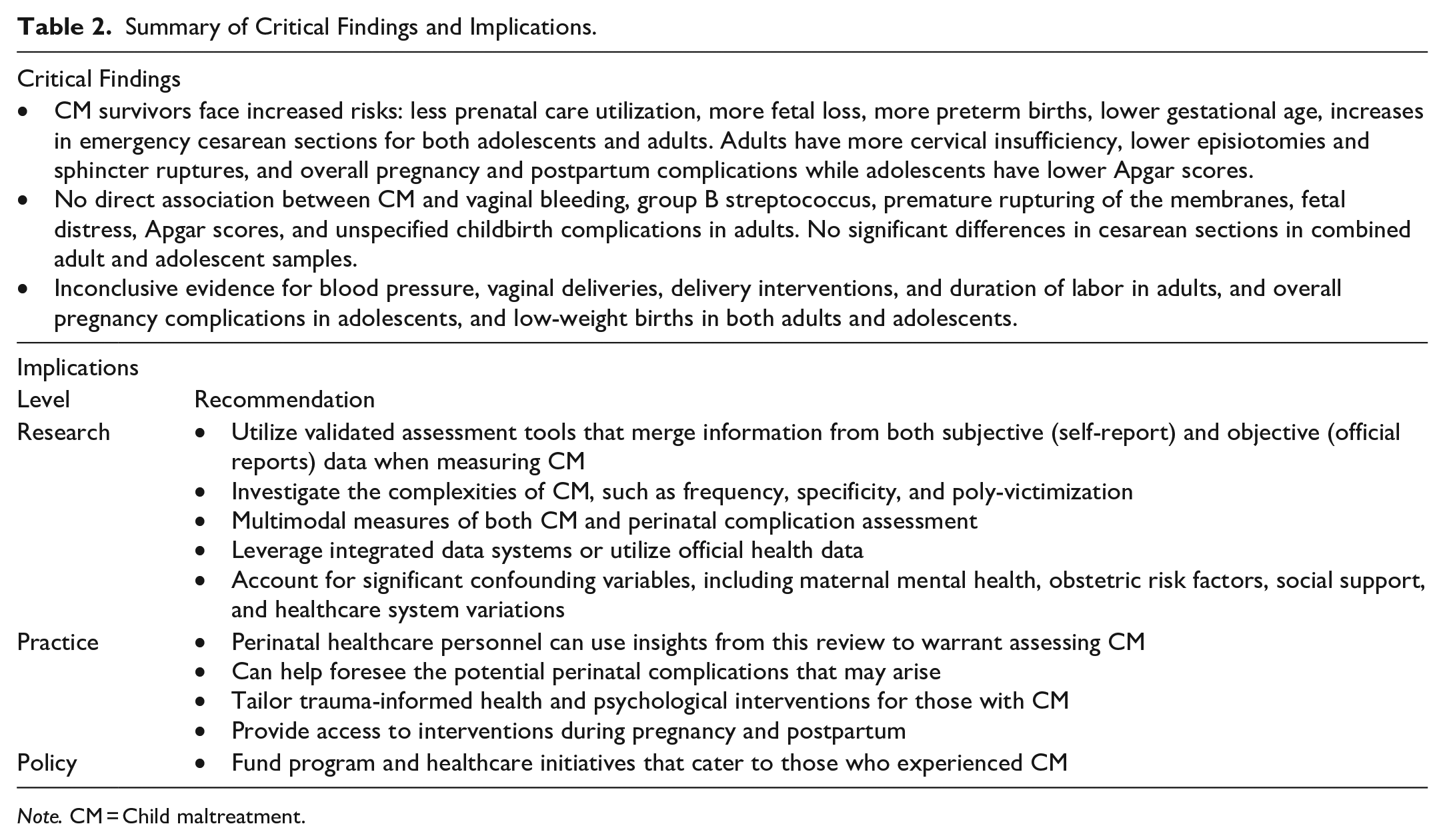
Note. CM = Child maltreatment.
Supplemental Material
sj-docx-1-tva-10.1177_15248380241270017 – Supplemental material for Childhood Maltreatment and Perinatal Complications: A Scoping Review of Official Health Data
Supplemental material, sj-docx-1-tva-10.1177_15248380241270017 for Childhood Maltreatment and Perinatal Complications: A Scoping Review of Official Health Data by Alesha Frederickson, Olivia Mazzarello and Rachel Langevin in Trauma, Violence, & Abuse
Supplemental Material
sj-docx-2-tva-10.1177_15248380241270017 – Supplemental material for Childhood Maltreatment and Perinatal Complications: A Scoping Review of Official Health Data
Supplemental material, sj-docx-2-tva-10.1177_15248380241270017 for Childhood Maltreatment and Perinatal Complications: A Scoping Review of Official Health Data by Alesha Frederickson, Olivia Mazzarello and Rachel Langevin in Trauma, Violence, & Abuse
Footnotes
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Alesha Frederickson is supported by scholarships from the Fonds de Recherche du Québec—Société Culture and the Social Sciences and Humanities Research Council of Canada. Dr. Langevin is supported by a salary award from the Fonds de Recherche du Québec—Santé and a William Dawson Scholar Award from McGill University.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.