
Abstract
Adolescent dating violence (ADV) is a pervasive public health issue associated with numerous social, psychological, and physical health consequences. Thus, programs are often implemented to prevent ADV and promote healthy relationships. Although there is a growing body of literature on primary ADV prevention strategies (i.e., prevention), little is known about secondary (e.g., early intervention) and tertiary (e.g., manage and reduce impact once occurring) ADV prevention approaches. This systematic review, guided by Cochrane Review methodology, summarizes available evidence on secondary and tertiary ADV preventive interventions. The search had no date restriction and was conducted in eight databases in November 2022. Studies published in English and/or Spanish were included if they described the development, implementation, and/or evaluation of a secondary and/or tertiary preventive intervention for ADV. After screening the titles and abstracts of 3,645 articles, 31 articles were included in this study, reporting on 14 secondary, 3 primary/secondary, 6 secondary/tertiary, and 1 tertiary ADV preventive intervention. The included studies highlighted that available secondary ADV prevention strategies are quite effective in preventing ADV victimization and perpetration, and that the effects may be strongest for teens with a higher risk of being involved in an abusive relationship. The only included study that reported on a tertiary intervention was a program development study. Based on the lack of tertiary prevention strategies available for ADV, clinical interventions focusing on treating and reducing negative consequences after ADV are needed.
Intimate partner violence (IPV) is a global public health concern that can affect individuals regardless of their age, sexual or gender identity, or race/ethnicity (Centers for Disease Control and Prevention [CDC], 2019). In the past three decades, extensive research, policy, and program responses have focused on addressing IPV during adolescence, also known as teen or adolescent dating violence (ADV), respectively, as it has gained recognition as an adverse childhood experience affecting millions of young people worldwide (Offenhauer & Buchalter, 2011). Although much is known about primary ADV prevention programs (i.e., prevention), less is known about secondary (e.g., early intervention) and tertiary prevention approaches (e.g., interventions after involvement). Thus, this systematic review summarizes available research on the development, implementation, and/or evaluation of secondary and tertiary strategies for ADV prevention.
Adolescent Dating Violence
ADV includes sexual, physical, and/or psychological aggression, as well as stalking, that occurs between the ages of ~11 and 19 (CDC, 2019). It can occur both in-person and electronically and to youth of any gender or sexuality (CDC, 2019). Although there are recognized, distinct subtypes of ADV, they are interrelated and often occur together (Rubio-Garay et al., 2017). In a recent meta-analytic review, Wincentak et al. (2017) found that 1 in 5 and 1 in 10 adolescents experience physical and sexual ADV victimization, respectively. In Canada, approximately one in three mid-adolescents experience dating violence (Exner-Cortens et al., 2021).
Although ADV is considered a widespread problem that can affect individuals from all cultural, social, economic, and religious backgrounds, young people from minoritized groups are significantly more likely to experience ADV (Rubio-Garay et al., 2017). For example, Exner-Cortens et al. (2021) found that ADV victimization was greatest among nonbinary youth in their sample, as compared to cisgender boys and cisgender girls. Similarly, Johns et al. (2019) found that among a nationally representative sample of high school students in grades 9 to 12 from the United States, physical and sexual ADV victimization were significantly more likely to be experienced by transgender students than cisgender boys or girls.
ADV is also linked to serious adverse psychological and physical health consequences for those involved. Victim-survivors of ADV may experience psychological distress, poor life satisfaction, loss of positive self-image, loss of ability to trust self and others, as well as feelings of isolation, powerlessness, insecurity, and intimidation (Cava et al., 2022; Meadows et al., 2020). These internalizing symptoms can also affect an adolescent’s ability to manage social relationships and regulate negative emotions and stress, affecting their social functioning, academic adjustment, and school performance (Basch, 2011). Physical health consequences of ADV include the risk of sustaining injuries, such as burns, cuts, or broken bones (Tharp et al., 2017). In sum, the psychological and physical health effects of ADV can be profound, persistent, and clinically significant (Beidel and Frueh, 2018; Jouriles et al., 2017).
ADV Prevention and Intervention
Given these health consequences, there has been a focus over the past two decades on developing and evaluating ADV prevention approaches. Broadly, preventive interventions can be divided into three different types: primary, secondary, and tertiary (García-Moreno et al., 2015). Although there are different levels of prevention programs, the goals of these different levels are not mutually exclusive.
Primary Prevention
Most attention in the ADV literature has been directed toward primary prevention (McNaughton Reyes et al., 2021; Russell et al., 2021). Primary prevention programs aim to prevent youth involvement in dating violence before it occurs by promoting healthy relationships, challenging violence-supportive norms, and developing conflict negotiation skills (DeGue et al., 2014). These programs are offered to all youth, whether or not they have previously been involved in dating violence, and thus they are also called universal prevention programs (Finnie et al., 2022). They are often implemented in schools, given the vast reach to a majority of youth in this setting (McNaughton Reyes et al., 2021).
Secondary Prevention/Intervention
Secondary prevention strategies aim to circumvent a possible trajectory toward abusive relationships among adolescents who are at higher risk of being involved in ADV due to their life experiences or circumstances (Edwards & Hinsz, 2014; Murray et al., 2016). For instance, evidence has shown that being exposed to domestic violence (Toplu-Demirtaş & Aracı-İyiaydın, 2021), child maltreatment (Hébert et al., 2017), and substance use (Johnson et al., 2017) is associated with higher rates of involvement in ADV.
Tertiary Prevention/Intervention
Tertiary approaches aim to prevent long-term consequences for individuals who have experienced violence in their dating relationships and are typically directed to individuals who are or have been involved in an abusive/violent relationship. Tertiary interventions are considered successful when they minimize adverse impacts and restore the health, wellness, and/or safety of survivors and/or perpetrators (Murray & Graybeal, 2007). At the clinical level, tertiary interventions could potentially include one-to-one clinical services, support groups, or crisis intervention services. In general, much less is known about both secondary and tertiary ADV preventive interventions, even though these approaches are critical and necessary in preventing victimization and its long-term consequences (Krahé, 2021).
Systematic Reviews on ADV Prevention and Intervention
In terms of prior reviews, to our knowledge, there is only one prior systematic review/meta-analysis that focuses solely on interventions targeting “at-risk” adolescents. Arrojo et al. (2023) included 17 studies in this systematic review, and 11 in a supplemental meta-analysis. Their results suggest that interventions for “at-risk” youth are effective in reducing physical and sexual ADV perpetration and physical ADV victimization. However, their study only included peer-reviewed articles with a randomized controlled trial (RCT) or quasi-experimental design, and focused searches on terms related to risk (e.g., at-risk or high-risk), rather than prevention type (e.g., secondary, tertiary). In addition, in a recent meta-analysis, Piolanti and Foran (2022) examined physical and sexual ADV preventive interventions and conducted an exploratory analysis with “at-risk” youth participating in the reviewed programs. These authors found that existing ADV programs were more effective in reducing physical ADV than sexual ADV, and that the effect sizes of ADV interventions delivered to adolescents at higher risk were larger than universally delivered interventions. To our knowledge, no reviews related to teriary ADV approaches exist in the literature.
Current Study
Little is known about the state of the science on secondary and tertiary preventive interventions for ADV, including evaluation evidence for existing programs. This lack of knowledge is a key challenge when identifying helpful resources for youth at risk (secondary) and victim-survivors (tertiary) of ADV. Thus, the objective of this study was to conduct a systematic review summarizing available information on the development, implementation, and/or evaluation of secondary and/or tertiary ADV prevention approaches. As compared to Arrojo et al. (2023), we included articles regardless of evaluation type and searched a wide variety of terms related to prevention to provide a more comprehensive picture of available evidence on existing ADV secondary and tertiary prevention approaches.
Methods
The review was guided by Cochrane Review methodology (Higgins et al., 2023) and followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA). The search protocol was uploaded to the Open Science Framework prior to any searches in order to register the review and increase transparency in research (https://osf.io/jp4y2/).
Search Strategy
The search protocol was developed with the assistance of two research librarians in fall 2022. First, six seed/key articles that met all inclusion criteria were located by conducting a nonsystematic search using Google Scholar. The seed articles were used to identify key terms that were then the basis for developing and running an initial search in APA PsycInfo. This search was tested and refined by the first author to maximize the precision and sensitivity of the overall search process. We based the final search terms on a combination of different clusters that reflected (a) the population (e.g., adolescence), (b) exposure (e.g., dating violence), and (c) intervention of interest (e.g., secondary and/or tertiary prevention) (Richardson et al., 1995). The search term strategy, which included truncated keywords, index terms, and synonyms, was then translated for eight different databases. On November 27, 2022, the first author conducted final searches in eight databases: APA PsycInfo, MEDLINE, Embase, CINAHL Plus with Full Text, ERIC, Academic Search Complete, Family and Society Studies Worldwide, and SocIndex. Complete versions of all search strategies are available in the optional Supplemental Material.
Inclusion and Exclusion Criteria
Eligibility criteria for this review were that studies (a) focus on ADV, defined as physical, sexual, psychological, and/or stalking aggression that occurred within a current or former dating and/or sexual relationship of young people ages 11 to 19 years and/or grades 6 to 12 either in-person or electronically; and (b) provide information relevant to the development, implementation, and/or evaluation of secondary and/or tertiary ADV prevention approaches. Secondary prevention approaches were defined as strategies that work to prevent ADV from occurring among adolescents who are at higher risk of future victimization/perpetration. To ensure we captured all relevant articles, we did not restrict types of risk factors and included any article that described their approach as secondary, selective, targeted, and/or Tier 2 (II) ADV prevention/intervention (i.e., categorization of interventions as secondary relied on how the authors themselves categorized and/or described the intervention in the article). Tertiary prevention approaches were defined as any clinical interventions implemented among adolescents involved in current or former abusive relationships in order to minimize the impact on and/or build their health, wellness, and/or safety. We did not restrict types of therapeutic approaches and included any article that described their approach as a tertiary, indicated, clinical, and/or Tier 3 (III) ADV prevention/intervention (i.e., categorization of interventions as tertiary relied on how the authors themselves categorized and/or described the intervention in the article).
Searches were restricted to peer-reviewed or gray literature studies (e.g., dissertations, book chapters) of any methodology published in English or Spanish by November 27, 2022. The search strategy did not include a lower publication date limit or any geographical limits. Given the anticipated limited research in this area, any form of evaluation was accepted for this systematic review. Studies were excluded if they (a) only examined primary prevention programs, (b) focused on college and/or adult populations, or (c) soley focused on interventions in the child protection system due to the overlap with multiple forms of violence (e.g., child abandonment, child maltreatment).
Review Procedures
Returns from all databases were exported to Covidence, a systematic review software, and duplicates were automatically removed. The first author then manually removed duplicate articles that were not caught by the Covidence system (Figure 1). Study selection occurred in two phases. Prior to each phase, all reviewers met with the first author to discuss inclusion/exclusion criteria and ensure the project team rigorously followed the systematic review methodology. In the first phase, tittles and abstract of all 3,645 studies emerging from the research strategy were reviewed in pairs (Figure 1; i.e., every article was reviewed by 2 independent coders). We were overly inclusive in this first phase in order to identify all articles with the potential for inclusion. Disagreements were then discussed and resolved among the reviewers.
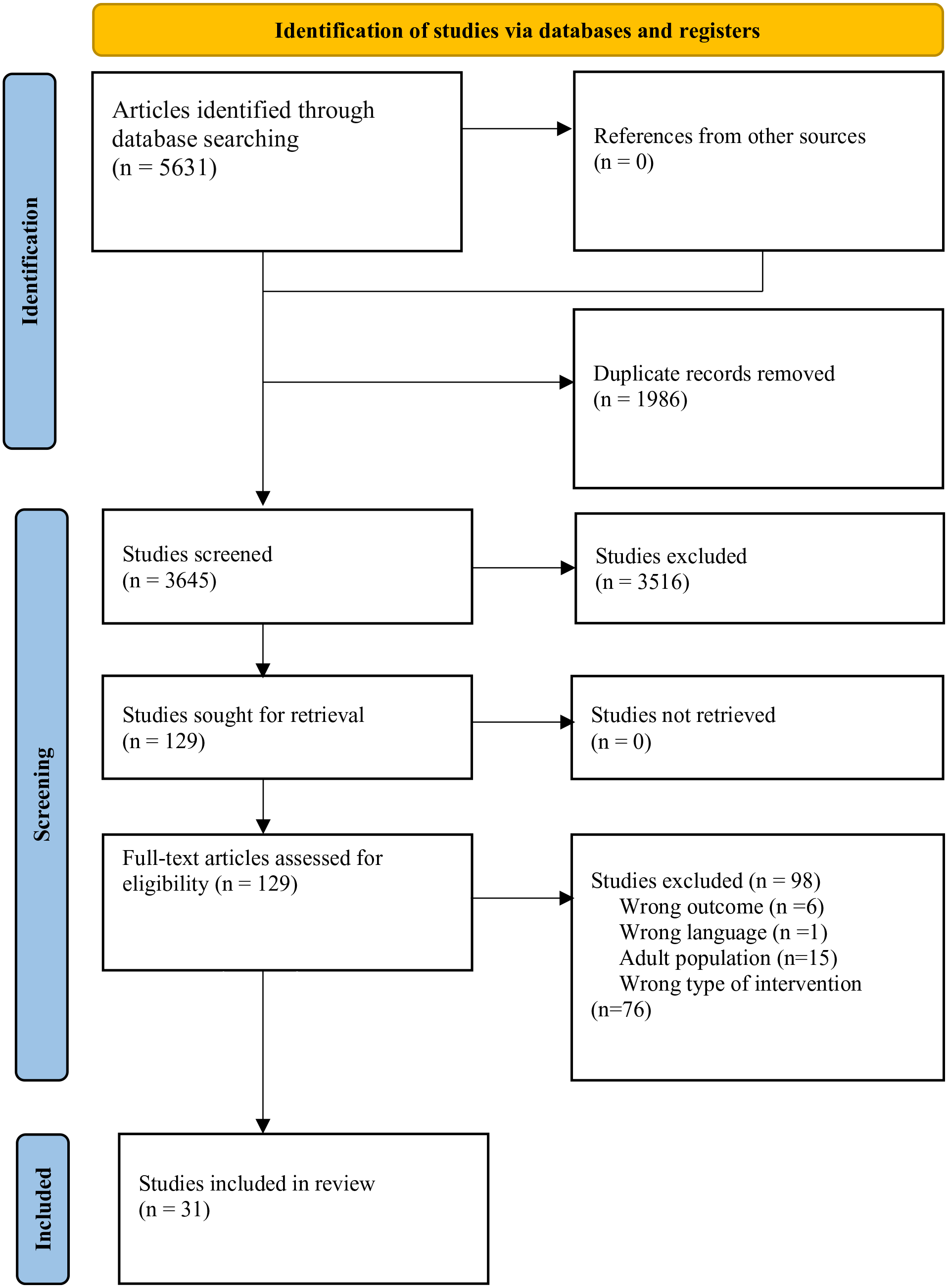
PRISMA diagram.
Following title and abstract screening, the full text of the 129 remaining potentially relevant studies was retrieved to proceed with the full-text review, which was also conducted in pairs (Figure 1). The first author reviewered all articles, and each pair member reviewed each article independently. Disagreements were then discussed and resolved among the reviewers. If a decision could not be made, the final decision was made by the second author. Following full-text review, 98 studies were excluded, leaving 31 articles for data abstraction (Figure 1). Extraction was conducted by a primary coder, and 40% of the studies were verified by a second coder. The intercoder agreement was 85% and discrepancies were resolves through consensus. Finally, the reference lists of all included studies and relevant review articles found during the search were also reviewed to capture any articles we may have missed. No additional articles were found in this step.
Data Extraction and Quality Assessment
Using the Patient/Population, Intervention, Comparison, Outcomes (PICO) study framework (Richardson et al., 1995), we developed a standardized data extraction form in Qualtrics. The form was pilot tested on three studies and subsequently refined. Final data extracted included sample characteristics (e.g., gender, age), intervention characteristics (e.g., setting, delivery method, facilitator training), study design and outcome measures, and key findings (see full extraction template in Supplemental Material). Data from the 31 articles were extracted independently by the first author. Following extraction by the first author, two undergraduate research assistants extracted information for 40% of the studies separately, and discrepancies were resolved through consensus. The intercoder agreement was 85%. Based on this high agreement, the extracted information of the remaining studies was not reviewed. Data from the extraction process were analyzed and summarized into tables by the first and second authors.
Quality Assessment
The quality of included evaluation studies was assessed based on a 7-item quality assessment tool adapted from the National Institutes of Health Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies (see Supplemental Material for items, scoring, and scores by study). We only assessed evaluation study quality as this study type was most relevant for the quality assessment process. Each item on the tool was scored as low (0), moderate (0.5), or high (1) quality. The first and second authors independently completed a quality assessment of all evaluation articles, and then met to discuss extractions and come to consensus. Intercoder agreement was 83%.
Results
Of the 3,645 references returned in our initial search, 31 ultimately met inclusion criteria. Full characteristics of included studies are detailed in Table 1. The majority of studies were quantitative (64.5%, n = 20; Table 1). All evaluation studies were quantitative. Most of the included articles were evaluation studies (61.3%; n = 19), followed by intervention development studies (n = 7), implementation studies (n = 3), and evaluation protocols (n = 2; Table 1). Studies were all published between 2000 and 2022 (Table 1).
Description of Included Studies (N = 31).
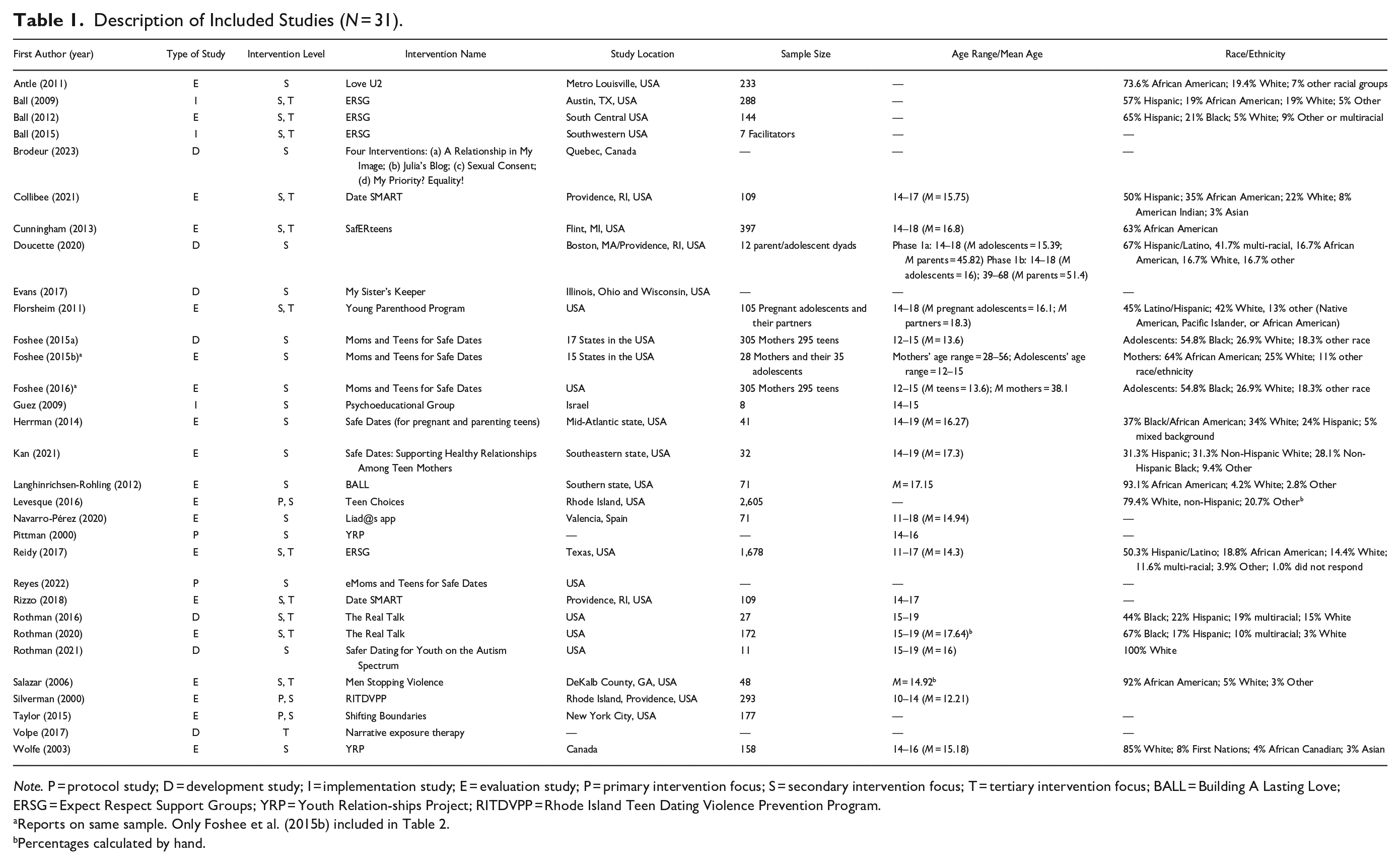
Note. P = protocol study; D = development study; I = implementation study; E = evaluation study; P = primary intervention focus; S = secondary intervention focus; T = tertiary intervention focus; BALL = Building A Lasting Love; ERSG = Expect Respect Support Groups; YRP = Youth Relation-ships Project; RITDVPP = Rhode Island Teen Dating Violence Prevention Program.
Percentages calculated by hand.
The majority of studies (n = 24; 77.4%) were conducted in the United States (Table 1). Two studies were conducted in Canada, one in Spain, and one in Israel. The remaining studies did not include the study location. The total sample size of included articles was 7,119 adolescents, with individual samples that ranged from 11 to 2,605 adolescents ages 11 to 19 years (Table 1). Among the studies that reported participant gender, girls constituted the majority of the sample in most studies (Table 1). The samples across studies were ethnically diverse, with African American/Black youth constituting the majority of the population in 10 out of 31 studies.
Across the 31 studies, we identified 24 ADV preventive interventions: 14 secondary only, 1 tertiary only, 3 that had elements of both primary and secondary prevention (primary/secondary), and 6 that had elements of both secondary and tertiary intervention (secondary/tertiary; Table 1). Studies were classified as primary/secondary when an intervention was developed for all youth but was implemented fully or in part among at-risk adolescents. Interventions were classified as secondary/tertiary when they were designed for youth who had previously experienced ADV but who were not currently involved in an abusive relationship. For space, full information on intervention characteristics, including target population, goal of intervention, setting and delivery, number of sessions, and facilitator information is available in optional Supplemental Material. Below, we report on evaluation and quality assessment findings.
Evaluation Findings
Of the 24 programs, 15 (3 primary/secondary, 6 secondary, and 6 secondary/tertiary) were tested as part of 19 evaluation studies (Table 2). The four programs that were the focus of two evaluation studies were Expect Respect; Moms and Teens for Safe Dates; Date Smart; and Safe Dates for Pregnant & Parenting Teens. Since Foshee et al. (2016) reports on the same dataset for Moms and Teens for Safe Dates as Foshee et al. (2015b), only Foshee et al. (2015b) is reported in Table 2, leaving a total of 18 evaluation studies for analysis.
Outcomes at Longest Follow-Up Period for Evaluation Studies (n = 18).
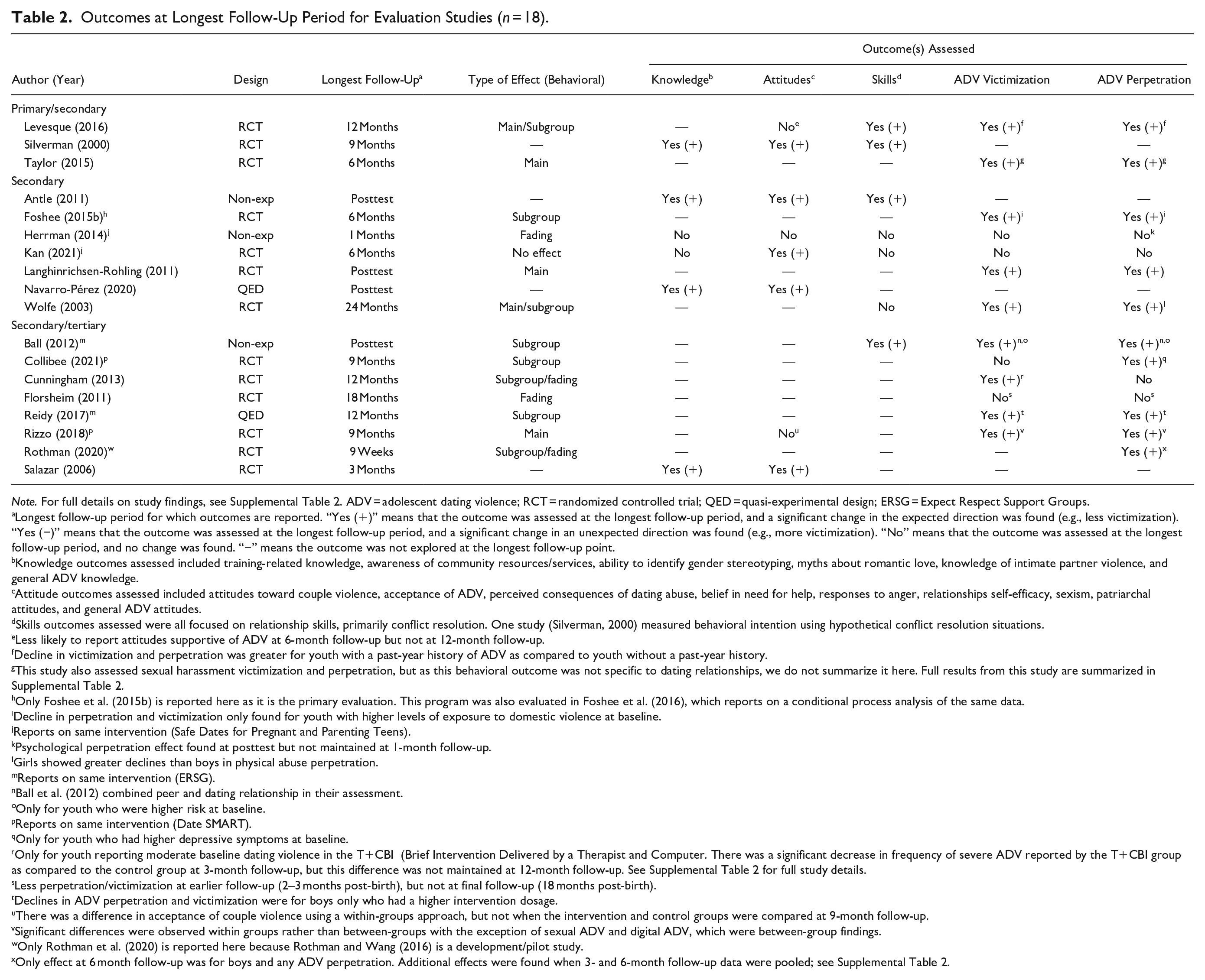
Note. For full details on study findings, see Supplemental Table 2. ADV = adolescent dating violence; RCT = randomized controlled trial; QED = quasi-experimental design; ERSG = Expect Respect Support Groups.
Longest follow-up period for which outcomes are reported. “Yes (+)” means that the outcome was assessed at the longest follow-up period, and a significant change in the expected direction was found (e.g., less victimization). “Yes (−)” means that the outcome was assessed at the longest follow-up period, and a significant change in an unexpected direction was found (e.g., more victimization). “No” means that the outcome was assessed at the longest follow-up period, and no change was found. “−” means the outcome was not explored at the longest follow-up point.
Knowledge outcomes assessed included training-related knowledge, awareness of community resources/services, ability to identify gender stereotyping, myths about romantic love, knowledge of intimate partner violence, and general ADV knowledge.
Attitude outcomes assessed included attitudes toward couple violence, acceptance of ADV, perceived consequences of dating abuse, belief in need for help, responses to anger, relationships self-efficacy, sexism, patriarchal attitudes, and general ADV attitudes.
Skills outcomes assessed were all focused on relationship skills, primarily conflict resolution. One study (Silverman, 2000) measured behavioral intention using hypothetical conflict resolution situations.
Less likely to report attitudes supportive of ADV at 6-month follow-up but not at 12-month follow-up.
Decline in victimization and perpetration was greater for youth with a past-year history of ADV as compared to youth without a past-year history.
This study also assessed sexual harassment victimization and perpetration, but as this behavioral outcome was not specific to dating relationships, we do not summarize it here. Full results from this study are summarized in Supplemental Table 2.
Only Foshee et al. (2015b) is reported here as it is the primary evaluation. This program was also evaluated in Foshee et al. (2016), which reports on a conditional process analysis of the same data.
Decline in perpetration and victimization only found for youth with higher levels of exposure to domestic violence at baseline.
Reports on same intervention (Safe Dates for Pregnant and Parenting Teens).
Psychological perpetration effect found at posttest but not maintained at 1-month follow-up.
Girls showed greater declines than boys in physical abuse perpetration.
Reports on same intervention (ERSG).
Ball et al. (2012) combined peer and dating relationship in their assessment.
Only for youth who were higher risk at baseline.
Reports on same intervention (Date SMART).
Only for youth who had higher depressive symptoms at baseline.
Only for youth reporting moderate baseline dating violence in the T+CBI (Brief Intervention Delivered by a Therapist and Computer. There was a significant decrease in frequency of severe ADV reported by the T+CBI group as compared to the control group at 3-month follow-up, but this difference was not maintained at 12-month follow-up. See Supplemental Table 2 for full study details.
Less perpetration/victimization at earlier follow-up (2–3 months post-birth), but not at final follow-up (18 months post-birth).
Declines in ADV perpetration and victimization were for boys only who had a higher intervention dosage.
There was a difference in acceptance of couple violence using a within-groups approach, but not when the intervention and control groups were compared at 9-month follow-up.
Significant differences were observed within groups rather than between-groups with the exception of sexual ADV and digital ADV, which were between-group findings.
Only Rothman et al. (2020) is reported here because Rothman and Wang (2016) is a development/pilot study.
Only effect at 6 month follow-up was for boys and any ADV perpetration. Additional effects were found when 3- and 6-month follow-up data were pooled; see Supplemental Table 2.
All evaluation studies were quantitative and the majority (72.2%, n = 13) used an RCT design, while 2 (11.1%) were quasi-experimental and 3 (16.7%) were nonexperimental (Table 2). Table 2 summarizes knowledge, attitudes, skills, and behavioral outcomes at the longest follow-up period for all evaluation studies (full details on findings for all included studies are reported in optional Supplemental Material). For four studies, the longest-follow up period was immediate posttest (22.2%). Most studies had a follow-up period between 3 and 12 months (55.6%, n = 10). Other follow-up periods were between 1 and 2 months (11.1%, n = 2) and more than 12 months (11.1%, n = 2).
Only 6 of the 18 studies reported on knowledge outcomes at the longest follow-up period. Of these studies, four found a positive, significant change in knowledge outcomes (i.e., 66.7% of studies that measured knowledge; Table 2). Eight studies explored attitude changes at the longest follow-up, with five of these reporting a significant, positive change (i.e., 62.5% of studies that measured attitudes; Table 2). Seven studies measured skills changes at the longest follow-up, with four reporting a significant, positive change (57.1% of all studies that measured skills; Table 2). For behavioral (i.e., ADV perpetration and/or victimization) outcomes, 13 studies assessed victimization (physical, psychological, sexual, cyber, and/or any), and of these, 9 found a significant reduction in victimization rates at the longest follow-up (69.2% of all studies that assessed victimization). Fourteen studies assessed perpetration outcomes (physical, psychological, sexual, cyber, and/or any), of which 10 reported a significant reduction in perpetration rates at the longest follow-up (71.4% of all studies that assessed perpetration; Table 2).
For behavioral outcomes, we also explored the type(s) of effect that were reported at the longest follow-up: main effects, subgroup effects, and/or fading effects (i.e., effects found at an early follow-up period, but not maintained at the longest follow-up), or no effect. Of the 14 total studies that reported on a behavioral outcome, 21.4% (n = 3) found main effects only, 28.6% (n = 4) found subgroup effects only, and 14.3% (n = 2) found fading effects (i.e., variation of effect over time). Other studies found a combination of effects: 14.3% (n = 2) found both main and subgroup effects and 14.3% (n = 2) found both subgroup and fading effects. Only one study (7.1%) found no effect (Table 2).
For those studies that found subgroup effects, this generally meant that the frequency of ADV perpetration and victimization decreased most for a subset of youth who were at higher risk of being involved in an abusive relationship at baseline as compared to the rest of the sample. For instance, Foshee et al. (2015b, 2016) conducted an RCT to assess the influence of the level of teen exposure to domestic violence on the effects of the Moms and Teens for Safe Dates intervention, finding that the intervention had a greater effect on preventing ADV for teens with higher exposure to domestic violence than teens with lower exposure to domestic violence at baseline. Other evaluations showed that interventions were more beneficial for higher risk subgroups including youth who had higher depressive symptoms at baseline (Collibee et al., 2021), youth with a history of violence/harassment (Levesque et al., 2016; Taylor et al., 2015), for boys with a higher intervention dosage (Reidy et al., 2017), and for girls with a history of child maltreatment (Table 2 and Supplemental Material) (Wolfe et al., 2003). Overall, results from these studies suggest that the included programs are promising in terms of reducing perpetration and victimization, particularly among groups who have higher initial risk of ADV.
Quality Assessment
Just over half of the evaluation studies (n = 10) fell in the moderate-quality range. Four studies fell in the low-quality range and four fell in the high-quality range (Supplemental Material). The highest average score was for study population, which was assessed as high quality for all articles. The lowest average score was for sample size, on which less than half of studies were scored as high quality.
Discussion
The focus of this systematic review was to assess existing secondary and tertiary preventive interventions for ADV, including available evaluation evidence. We included quantitative, qualitative, and mixed-methods studies to ensure the inclusion of all relevant work, although all evaluation studies were quantitative. In total, 31 articles were included in this review. The majority of the studies were focused on program evaluation and used an RCT design. Notably, although samples were fairly diverse, most included studies were conducted in the United States. Other study locations included Spain, Israel, and Canada.
This review identified 24 interventions, of which all but 1 were focused on secondary prevention. Interventions were found to be implemented remotely and in person and facilitated by health-care professionals, nonhealthcare professionals, and caregivers. Our findings suggest that secondary prevention programs have mostly been implemented in school settings. Even though school settings are fundamental for ADV prevention, the further development, implementation, and testing of prevention programs in community and health-care settings is critical to the holistic prevention of ADV, especially for reaching higher risk youth who may not be enrolled in schools (e.g., pregnant and parenting youth, houseless youth).
Of the 15 evaluated programs we found, these targeted a wide diversity of youth, including autistic youth, pregnant and parenting teens, youth exposed to domestic violence, and youth with a prior history of ADV, child maltreatment, and child sexual abuse. However, we did not identify any implemented clinical intervention targeting youth who were involved in ongoing abusive relationships. This is concerning as youth who are experiencing ADV need interventions that provide them with harm-reduction strategies and supports to safeguard their mental and physical well-being. Considering the association between ADV victimization, depression, and trauma symptoms (Jouriles et al., 2017), future research could focus on testing the effectiveness of trauma-informed therapeutic approaches for addressing mental health issues among ADV victim-survivors (Exner-Cortens et al., 2013; Kulkarni, 2019), including one-to-one clinical work and/or support groups.
Overall, 15 of the 24 interventions were evaluated (4 in more than 1 study), and generally found to show promise of effectiveness for reducing ADV victimization and perpetration. Specifically, we found that of the 14 studies reporting on behavioral outcomes, about two-thirds found a significant reduction in perpetration and/or victimization at the longest follow-up. Findings across studies also suggested that a number of interventions were most effective for youth at higher risk of ADV as compared to their peers. These results are encouraging as reducing the likelihood of ADV among youth who are most at risk moves us closer to reducing the cycle of violence (Piolanti et al., 2023). In their meta-analysis, Arrojo et al. (2023) also found significant pooled effects for perpetration and victimization, specifically for physical ADV perpetration and victimization, sexual ADV perpetration, and any ADV victimization. Our findings concur with those of Arrojo et al. (2023) in terms of the promise of secondary prevention programs for reducing the risk for ADV victimization and perpetration among youth who are at higher risk because of their circumstances or life experiences. Our review also adds to the findings of Arrojo et al. (2023) by reviewing six additional programs, and looking specifically at subgroup effects, which may explain some of the heterogeneity in pooled effects found in their meta-analysis. However, additional research is needed to continue to develop and evaluate secondary prevention programs, particularly for psychological and cyber ADV outcomes (Arrojo et al., 2023).
As noted above, this review did not identify any tested intervention with the goal of enhancing the psychological well-being of victim-survivors by generating positive changes in their cognitive, behavioral, or interaction patterns (i.e., tertiary interventions). Considering the adverse psychological outcomes associated with ADV (Piolanti et al., 2023), it is important to develop and implement therapeutic interventions to address impacts and prevent future ADV victimization, as ADV in adolescence and continued physical ADV victimization in early adulthood may be mediated by trauma symptoms (Jouriles et al., 2017). Findings from our review regarding the lack of interventions for youth currently experiencing ADV also align with those from a recent review on therapeutic intervention for victims and perpetrators of dating violence for young people between the ages of 12 and 31 years old conducted by Yanez-Peñúñuri et al. (2019). Similar to our review, the authors did not find any clinical intervention targeting adolescents involved in abusive relationships, even though they also considered French and Portugese language literature. In conducting this needed work, ADV researchers might look to the adult domestic violence literature for potential tertiary intervention strategies (Emalia et al., 2023; Kirk et al., 2017). However, given the key developmental differences between adolescents and adults and how these differences shape experiences of ADV (Exner-Cortens, 2014), any strategies developed with adults must first be tested with teens for effectivenss prior to any wider-scale use.
Limitations
This systematic review followed a rigorous method to ensure the appropriate inclusion of studies. However, given that there is not standardized terminology for ADV, it is still possible we missed some relevant studies. Another strength of this work is that the search strategy did not have any restrictions related to location, time, or publication dates, unlike prior reviews. We also searched for studies published in both English and Spanish, though would have missed any research not published in these two languages. Given the nature of the systematic review, this study does not account for potential follow-up and subsequent interventions provided by facilitators of primary and secondary prevention programs in the evaluated programs, who may have been contacted by youth experiencing ADV. Future research could explore the frequency of contacts made by victim-survivors and evaluate the subsequent interventions provided to contribute to a more comprehensive understanding of available tertiary prevention strategies. While we did complete a quality assessment, we concluded that a meta-analysis was not feasible given the differences in interventions and heterogeneity of outcome measures across evaluations. In addition, as all evaluation studies were quantitative, we were restricted in assessing the quality of quantitative studies only. The use of mixed-methods in future research is thus strongly encouraged. Finally, for tertiary prevention, we chose to focus on clincal services, to align with the focus of most primary and secondary ADV prevention programs, but acknowledge that there are other approaches to intervention at this level (e.g., orders of protection) (Adhia et al., 2020).
Practice, Policy, and Research Recommendations
Recommendations for future practice, policy, and research in ADV literature are listed in Table 3. First, the majority of interventions that we found used samples from North America. Thus, in future work, it is critical to use more geographically diverse samples to explore the effectiveness of these interventions in other countries (e.g., in the Global South), and to assess if existing interventions are culturally relevant and sensitive. Second, although there was substantial racial/ethnic diversity in the papers included in this review, we found no interventions that specifically focused on youth who identify outside of the imposed gender binary, or as sexually diverse. Given high ADV prevalence rates and the unique challenges faced by gender and sexually diverse youth with regards to ADV, including discrimination, help-seeking barriers, and fears around confidentiality (Johns et al., 2019), future studies need to actively center the needs and voices of these youth and explore the effectiveness of interventions for this population. In addition, high rates of cyber ADV have been reported (Caridade et al., 2019); however, there were only four studies that evaluated the effectiveness of interventions on cyber ADV victimization and perpetration. Thus, researchers should also aim to assess the effectiveness of interventions in preventing cyber ADV. The present results also suggest that more attention is needed on supporting victim-survivors of ADV through tertiary approaches. As noted above, lessons from the literature on adult IPV and tertiary prevention strategies can potentially inform tertiary interventions for youth, but these strategies must first be adapted for and evaluated with youth samples. Finally, the majority of studies in this review used quantitative methods. Further research should consider using qualitative and mixed-methods evaluative research as these methods can offer a nuanced understanding of prevention strategies by delving into the lived experiences, perspectives, and contextual factors involved. Draucker et al. (2016) note that qualitative studies provide unique and in-depth information about outcomes that are hard to predict and are only visible through the narratives of participants. This is particularly critical for work focused on tertiary prevention/intervention, as qualitative narratives can highlight strategies to develop victim-survivors’ resiliencies and strengths as they heal.
Recommendations for Future Practice, Policy, and Research on ADV Prevention Programs.
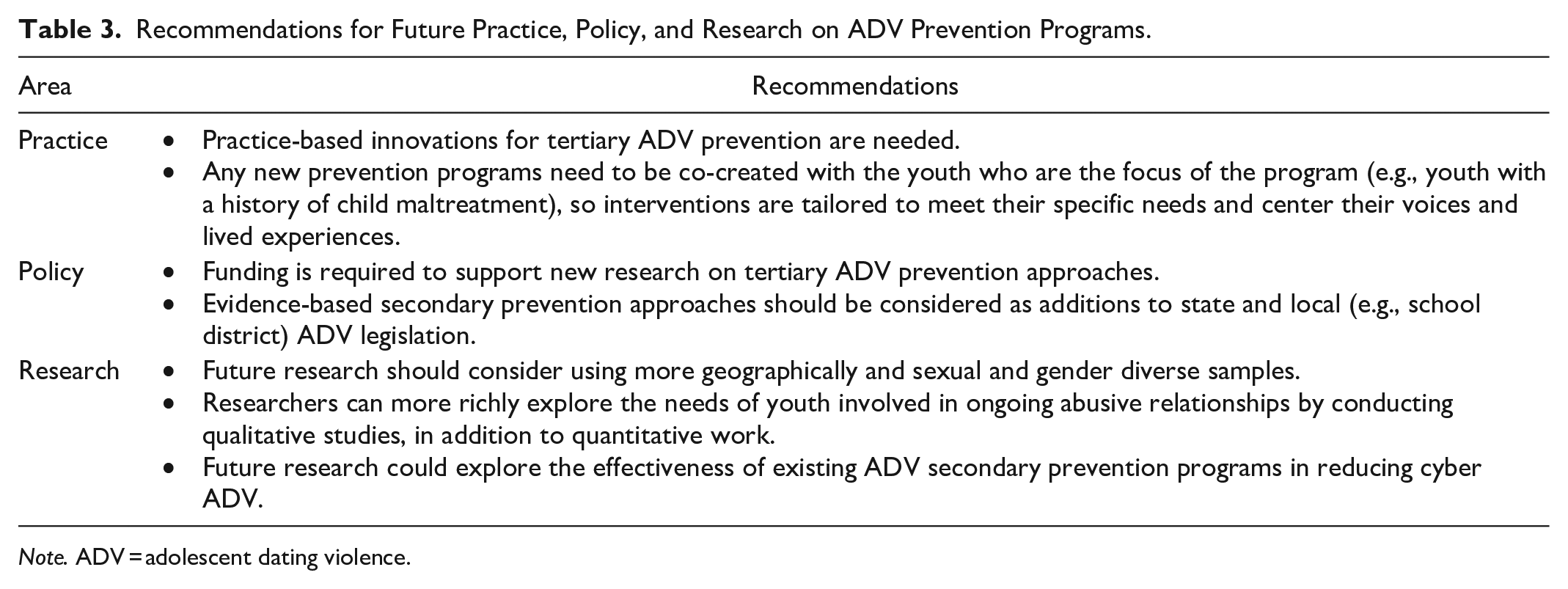
Note. ADV = adolescent dating violence.
Conclusion
The present review describes the availability of and evaluation evidence for secondary and tertiary ADV prevention programs. The findings of this review suggest that secondary prevention programs have promise for reducing ADV perpetration and victimization, particulary among youth at highest risk at baseline. These findings also demonstrate the limited evidence that exists for tertiary ADV prevention programs. More research focusing on the development and implementation of tertiary prevention approaches is needed to support youth in ongoing abusive relationships and improve victim-survivors’ safety and well-being.
Supplemental Material
sj-docx-1-tva-10.1177_15248380241265384 – Supplemental material for Secondary and Tertiary Prevention for Adolescent Dating Violence: A Systematic Review
Supplemental material, sj-docx-1-tva-10.1177_15248380241265384 for Secondary and Tertiary Prevention for Adolescent Dating Violence: A Systematic Review by Jeniffer Nicole Camacho Soto, Deinera Exner-Cortens, Carly McMorris and Sheri Madigan in Trauma, Violence, & Abuse
Footnotes
Acknowledgements
The author wishes to thank Loyce Sakuhuni, Jenna Himer, and Saskia Groot, for their assistant during the article screening process.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Exner-Cortens’ work was partially supported by the Canada Research Chairs program and the Alberta Children’s Hospital Research Institute (ACHRI).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.