
Abstract
It is well-known that interpersonal traumatic events can impact the physical and mental health of those indirectly exposed to the events. Less studied are populations of loved ones who have been indirectly exposed to interpersonal trauma. We conducted a scoping review to synthesize literature related to potential consequences of indirect interpersonal trauma exposure, specifically vicarious traumatization (VT) and vicarious posttraumatic growth (VPTG). We used the Joanna Briggs Institute methodology. Inclusion criteria included: (1) participants were indirectly exposed to the interpersonal trauma of a loved one in adulthood, (2) discussion of VT, VPTG, or related terms, (3) published peer-reviewed empirical journal articles, and (4) available in English. We used a three-step search strategy to find relevant articles. Keywords found from the first two steps were entered into PsycINFO, PsycArticles, PubMed, Scopus, and Web of Science databases. Reference lists of the included articles were also examined. The identified articles were then screened using the inclusion and exclusion criteria. Twenty-eight articles met inclusion and exclusion criteria. Twenty-six articles referenced VT or related terms, one referenced VPTG, and one referenced vicarious trauma keywords. Results of this scoping review are summarized by definitions, measures, key findings, and knowledge gaps. Future research should focus on vocabulary management, diverse samples, and VPTG in this population, including the identification or creation of appropriate measures.
Keywords
Introduction
Interpersonal traumas are defined as exposure to actual or threatened death, serious injury, or sexual violence due to perpetration by another person (American Psychiatric Association [APA], 2013). It is well-known that interpersonal traumatic events can impact the physical and mental health of survivors (Gatov et al., 2020; López-Martínez et al., 2018) and those indirectly exposed to the events (Cieslak et al., 2014; Cyr et al., 2016, 2018). Indirect exposure to interpersonal trauma occurs when an individual learns about another person’s interpersonal traumatic event (APA, 2013), typically through professional duties or as a part of one’s support network. Researchers examining indirect trauma exposure have primarily focused on helping professionals who interact with traumatized individuals as part of their professional work (Cieslak et al., 2014; McCann & Pearlman, 1990). Less studied are populations of loved ones who have been indirectly exposed to interpersonal traumas (Gregory et al., 2021). We conducted a scoping review to synthesize the literature related to potential consequences of indirect interpersonal trauma exposure, specifically vicarious traumatization (VT) and vicarious posttraumatic growth (VPTG).
One unfortunate impact of indirect trauma exposure is VT. VT was first used by McCann and Pearlman (1990) to describe the psychological impact of listening to the descriptions of traumatic events when working with trauma survivors as a therapist. Since that time, the use of VT has been applied to populations of loved ones indirectly exposed to interpersonal traumas (Bux et al., 2016) and is used interchangeably with terms such as secondary traumatic stress (STS; see e.g., Gregory et al., 2017), secondary traumatization (see e.g., Manion et al., 1996; Manion et al., 1998), posttraumatic stress disorder (PTSD; see e.g., Burgess et al., 1990; Cyr et al., 2018), and posttraumatic stress (PTS) symptoms (see e.g., Davies, 1995; Vilvens et al., 2021). VT and related terms describe negative psychological symptoms such as intrusive imagery/memories, negative affect, arousal, avoidance behaviors, and negative changes to cognitions that follow indirect trauma exposure (Mangold et al., 2021; Sparks & Stoppa, 2022).
Another possible outcome related to indirect trauma exposure is VPTG. Posttraumatic growth was first described by Tedeschi and Calhoun (2004) as the positive changes in one’s life domains (e.g., appreciation of life, priorities, and possibilities, relationships, spirituality, and personal strength) due to cognitive processing and emotional engagement after a traumatic event. VPTG originated from researchers extending the definitions of posttraumatic growth (Tedeschi & Calhoun, 2004) to individuals who have experienced indirect trauma exposure and experience growth thereafter (Arnold et al., 2005; Manning-Jones et al., 2015). Instead of VPTG, other researchers use the term vicarious growth to describe the positive changes to oneself and worldviews following indirect trauma exposure (McCormack et al., 2011). Overall, VPTG and vicarious growth are defined as the positive changes that occur cognitively, emotionally, interpersonally, and/or spiritually because of indirect trauma exposure (Arnold et al., 2005; Cummings, 2018; Manning-Jones et al., 2015; McCormack et al., 2011). Nonetheless, it appears to be understudied in loved ones indirectly exposed to interpersonal trauma.
No reviews have collated and summarized the research on loved ones’ experiences of VT and VPTG following indirect interpersonal trauma exposure. Accordingly, a scoping review examining these outcomes was needed to fully understand and summarize these experiences among loved ones. Our scoping review mapped the relevant empirical literature on this topic guided by the question: what has been found in the published scholarly literature examining indirect exposure to interpersonal traumatic events among loved ones regarding VT and VPTG? Identifying the available information related to these outcomes was key to (1) clarifying the definitions in the literature, (2) examining how research is conducted on this topic, (3) identifying key findings related to the concepts, and (4) identifying knowledge gaps (Munn et al., 2018).
Method: A-Priori Protocol
We used the Joanna Briggs Institute (JBI) methodology (Peters et al., 2015, 2017) and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) for Scoping Reviews checklist for reporting guidelines (Tricco et al., 2018), both of which are considered “gold standard” approaches for scoping reviews. The JBI methodology begins with the development of an a-priori protocol which provides a plan for the review and reduces reporting bias (Peters et al., 2015). The protocol outlined the pre-defined objectives and research question(s), topic background, inclusion and exclusion criteria for articles, search strategy, data charting, and results presentation. We searched for, selected, extracted, charted, and then summarized the evidence gathered regarding the scoping review objectives and questions (Peters et al., 2017). Consultation with other researchers and librarians occurred throughout the scoping review process. For example, our disciplinary librarian reviewed the scoping protocol before it was finalized and assisted with decisions related to databases to search. We conducted a preliminary search for existing scoping reviews on this topic using the following databases: PsycINFO, PubMed, APA PsycArticles, Scopus, and Web of Science. We found no evidence to suggest that a scoping review on this topic had previously been conducted.
Inclusion and Exclusion Criteria
Types of Participants
Participants were adults (age 18+) who had been indirectly exposed to the trauma of a loved one in adulthood, regardless of sex or gender. The participants must have known about (i.e., been exposed to) an interpersonal traumatic event that happened to a loved one (i.e., a family member, partner, spouse, child, or friend) to be included.
Concept
The core concepts were the outcomes of loved ones who have been indirectly exposed to an interpersonal traumatic event that happened to a friend, partner, or family member. Any studies focusing on war-, terrorism-, or intergenerational-traumas and any non-interpersonal traumas (e.g., accidents, natural disasters) were excluded. The focus had to be on the impact of the indirect interpersonal trauma exposure, specifically VT, secondary traumatization, STS, PTSD, PTS, VPTG, posttraumatic growth, and/or event centrality. The original data collection was a part of a larger project, and thus event centrality was present in the search terms. The articles looking at VT had to discuss posttraumatic symptoms such as intrusive imagery/memories, negative affect, arousal, avoidance behaviors, and negative changes to cognition; articles that solely focused on distress or stress were excluded.
Context
This scoping review excluded previously published evidence that was based on populations of individuals who experienced trauma through their profession (i.e., occupational traumas), including mental health workers, health care workers, military personnel, journalists, first-responders, and any other professionals that appeared in the search.
Types of Sources
Our scoping review included published peer-reviewed empirical (qualitative and/or quantitative) journal articles and excluded gray literature. This decision ensured that only high-quality, peer-reviewed research was included (Felthous & Wettstein, 2014). Reviews were excluded but were examined for relevant articles. Treatment outcome studies were also excluded.
Search Strategy
We used a three-step search strategy (Peters et al., 2015, 2017). The first step was a limited search of two online databases appropriate for the scoping review topic (PsycINFO and Scopus). This initial search examined the title, abstract, and index terms of articles related to the topic. This helped identify keywords and index terms then used in the second search strategy step. The second step involved entering the identified keywords and index terms into PsycINFO, PsycArticles, PubMed, Scopus, and Web of Science databases. The third step involved examining the reference lists of the included articles for additional studies.
We first screened the identified articles by examining the title and abstracts; the articles that did not meet the inclusion and exclusion criteria or were duplicates were removed. The remaining articles were then subjected to a full-text screening. The screening process was primarily undertaken by the first author, with the oversight of the second author until a consensus was reached on the included articles. Articles from which the full text could not be retrieved online or through the [redacted for blind review] library (including interlibrary loan) were excluded.
Results
Search Strategy Results
The keywords identified in the first search strategy step can be found in Table 1. Outcome terms were searched with population terms, and the relevant articles were scanned for their keywords. A list was compiled until saturation was reached (i.e., no more relevant keywords were found; see Table 2). These keywords were entered into the selected databases and the abstract, title, and citation for the articles were exported. Operators “OR”, “AND”, and “AND NOT” were used to broaden and narrow the search in their appropriate places. This created more accurate results that pertained to the outcomes and only the populations of interest (e.g., vicarious trauma AND parents). For two databases, we were able to enter all search terms together and export the abstracts. For three databases, we had to conduct four separate searches (i.e., one for indirect trauma exposure keywords, one for VT keywords, one for VPTG keywords, and one for vicarious event centrality keywords) and export the abstracts for each. The latter exporting method was necessary due to the size limitation for exporting files for these databases. We acknowledged that this resulted in additional duplicates.
Initial Search Terms Entered Into PsycINFO and Scopus.
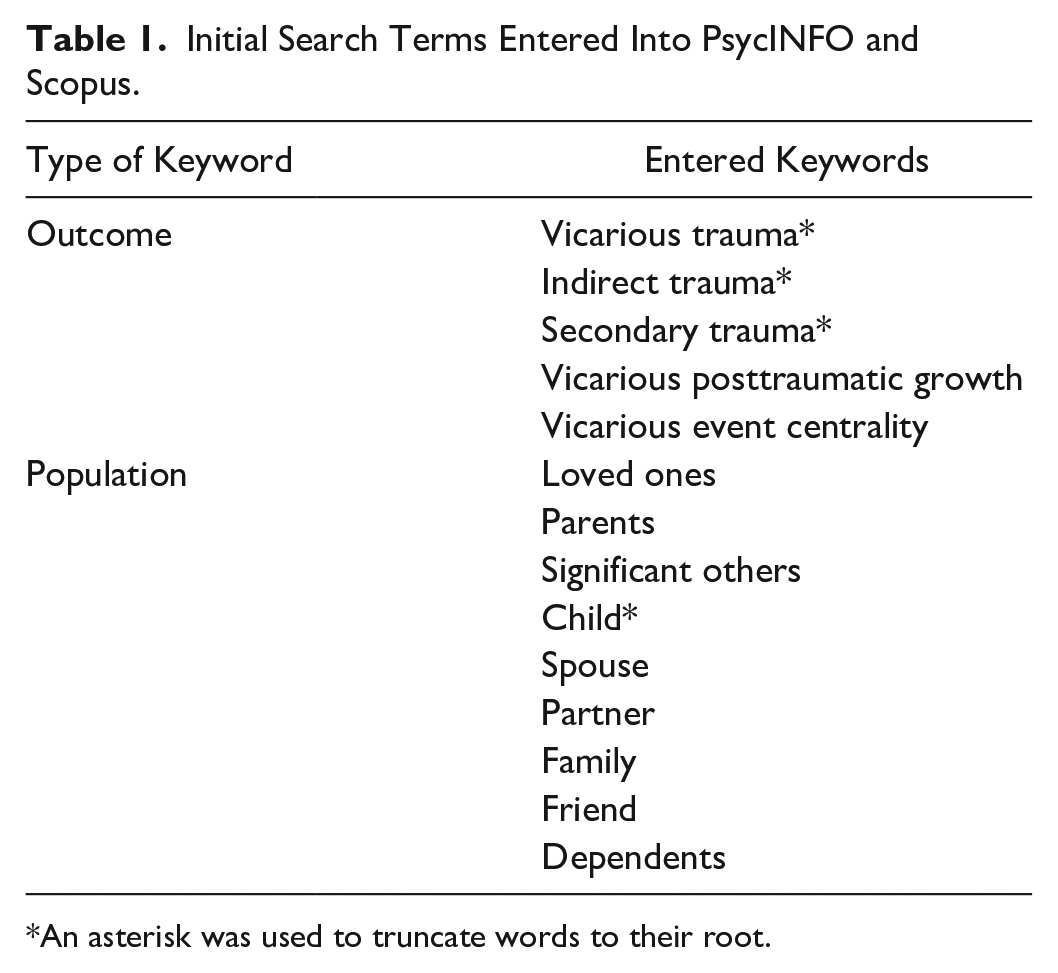
An asterisk was used to truncate words to their root.
Final Search Terms Entered into All Databases.
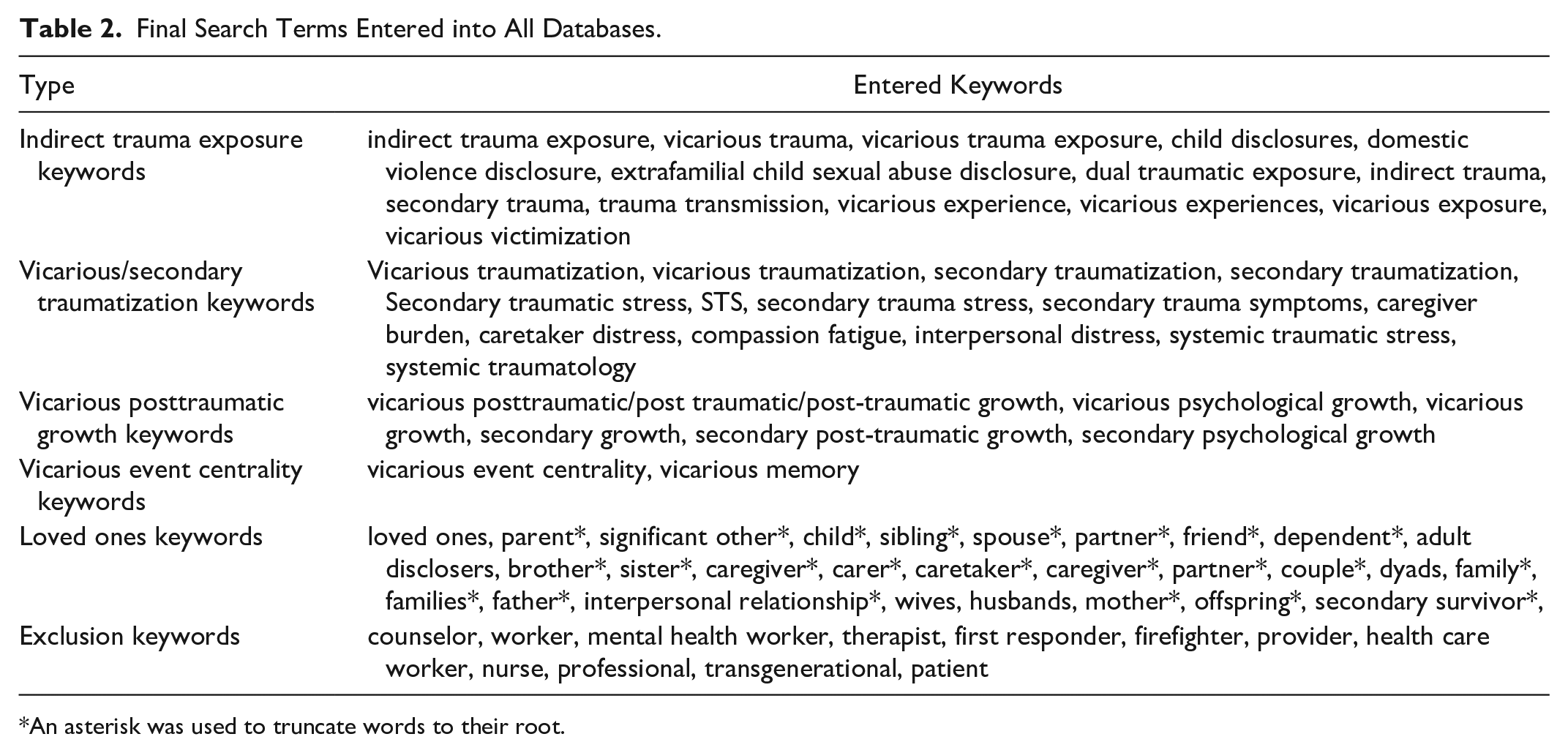
An asterisk was used to truncate words to their root.
Overall, a total of 11,591 abstracts were initially collected. During the screening process, we noted that the “AND” function had not worked for the PsycINFO database; thus, the search was not limited to the population of interest. The decision was made to continue screening with the PsycINFO dataset. This resulted in the collection of more irrelevant abstracts than intended; PsycINFO comprised almost 43% of the total abstracts. After the initial screening, 179 articles potentially met inclusion and exclusion criteria. After reviewing the full texts,
Descriptive Summaries
The 28 included articles were published between the years 1990 and 2022. The median year was 2016, when six articles were published. Studies were conducted in the USA (12/28), Canada (5/28), South Africa (3/28), the United Kingdom (2/28), Denmark (1/28), the Netherlands (1/28), Norway (1/28), Australia (1/28), the Republic of Ireland (1/28), and one was not specified. In total, 12 articles (12/28; ~43%) used qualitative research methods, and 16 articles used quantitative methods (16/28; ~57%; see Table 5). Most studies focused on parents/caregivers of individuals who had experienced an interpersonal trauma (22/28; ~79%) and on individuals indirectly exposed to child sexual abuse (CSA; 21/28; 75%; see Table 3). Unexpectedly, 50% of the studies did not comment on the ethnicity of participants. Of those reporting ethnicity, participants were predominantly White/Caucasian (see Table 4 for demographics).
Type of Loved One and Interpersonal Trauma.
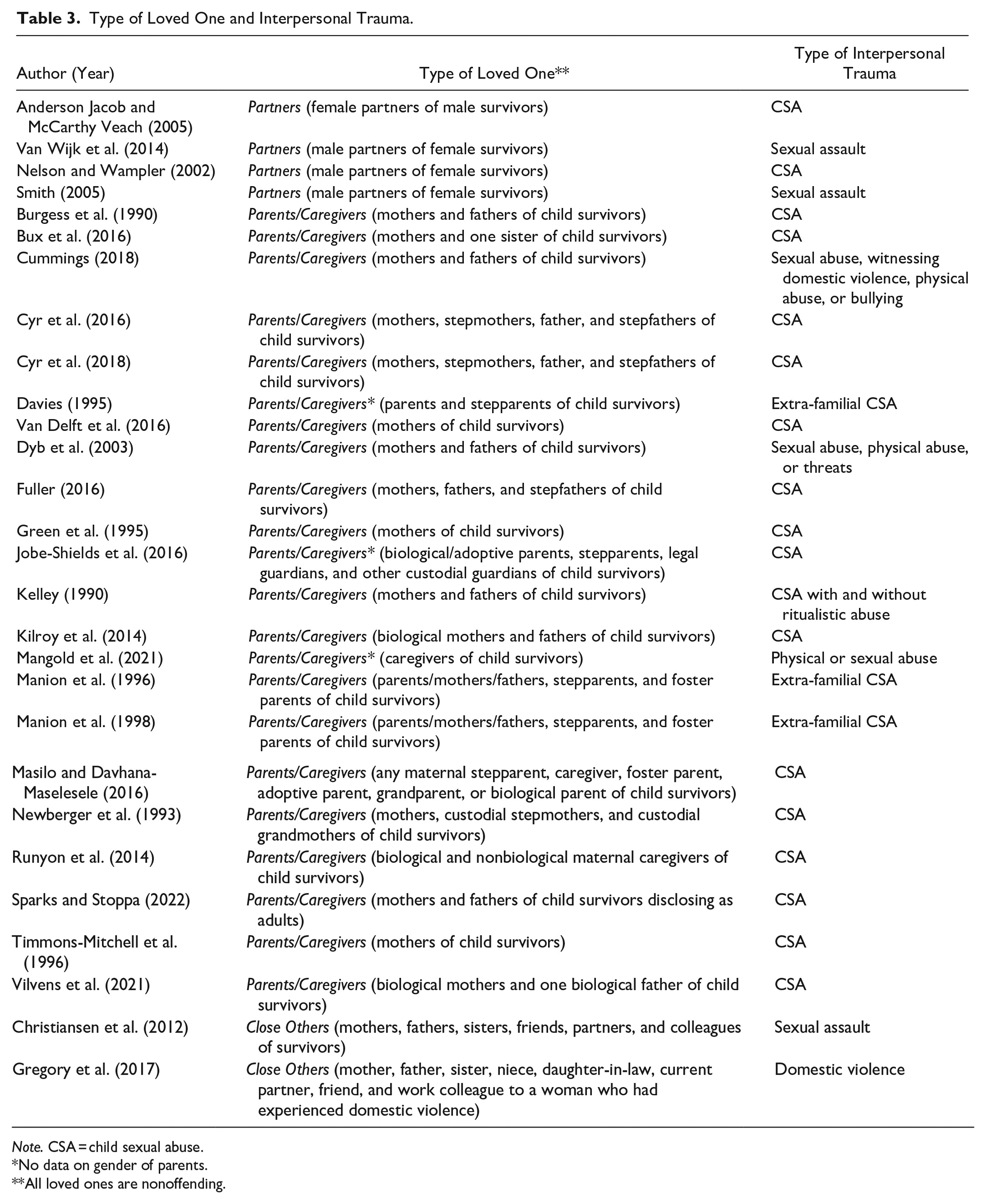
Note. CSA = child sexual abuse.
No data on gender of parents.
All loved ones are nonoffending.
Demographics.
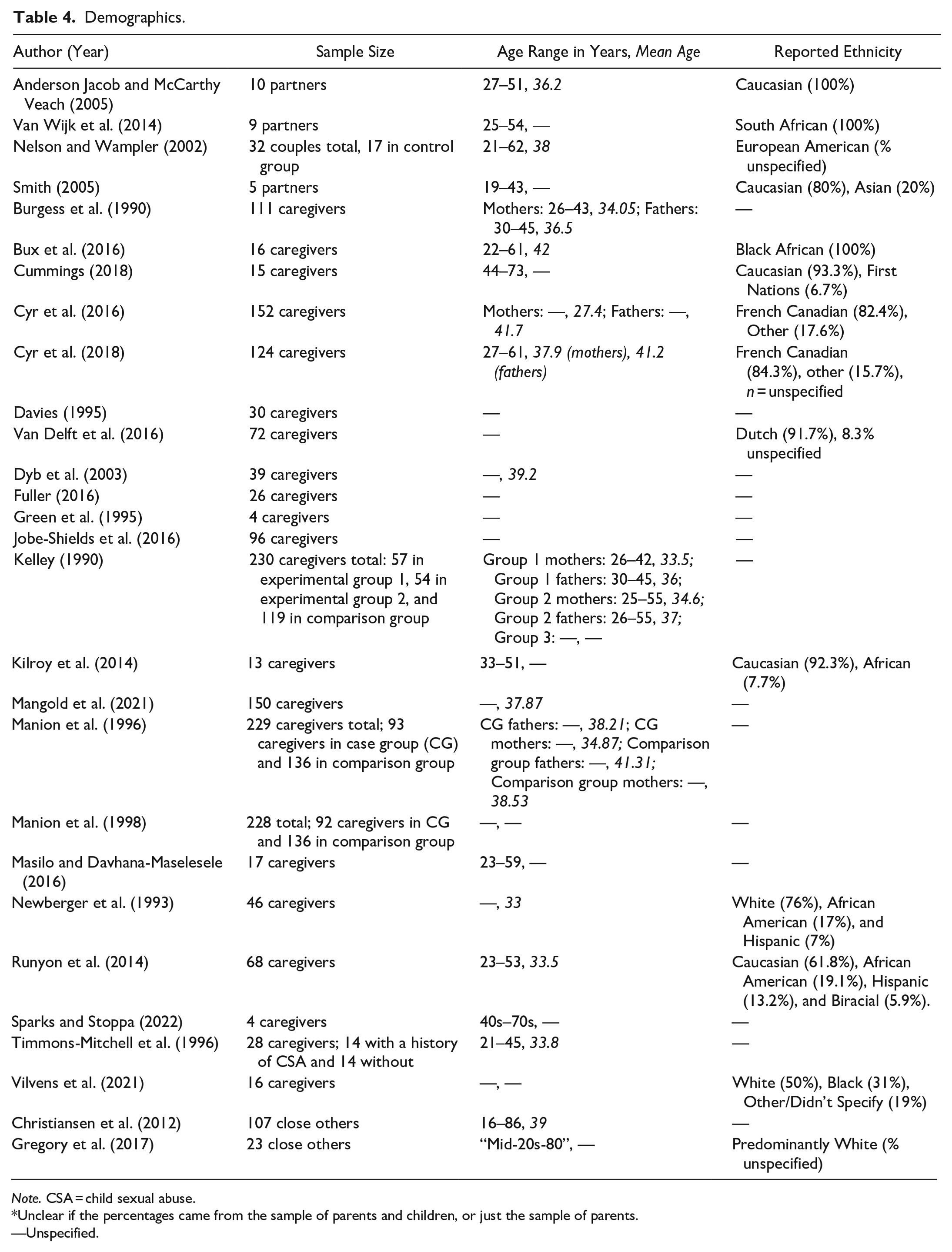
Note. CSA = child sexual abuse.
Unclear if the percentages came from the sample of parents and children, or just the sample of parents.
—Unspecified.
There were 26 articles that referenced outcomes of VT and related terms in populations of loved ones following indirect interpersonal trauma exposure that met inclusion and exclusion criteria. These 26 articles used terms such as trauma contagion, PTS/PTSD, VT, secondary traumatization, STS, and systemic trauma to describe the negative sequela of being indirectly exposed to a loved one’s interpersonal trauma (see Table 5 for key findings related to outcomes). Although trauma contagion was not an original key search term for VT, it was decided that this term was likely overlooked when gathering search terms (Anderson Jacob & McCarthy Veach, 2005). There was one article that used indirect trauma keywords but did not use any VT keywords to describe their findings (Van Wijk et al., 2014), despite citing similar findings to other studies. As their participants exhibited similar symptoms to VT, the article was included. There was only one article that discussed VPTG, although one other article referenced “healing” themes. The definitions, tools, and knowledge gaps are highlighted below.
Data Summary.
Note. ANOVA = Analysis of variance; BSI = Brief Symptom Inventory; CSA = child sexual abuse; HTQ = Harvard Trauma Questionnaire; IES = Impact of Event Scale; MANOVA = Multivariate analysis of variance; PTS = posttraumatic stress; PTSD = posttraumatic stress disorder; PPTSD-R = Purdue Posttraumatic Stress Disorder, Revised; SCL-90-R = Symptom Checklist 90-Revised; VPTG = Vicarious posttraumatic growth; VT = vicarious traumatization.
Definitions
Trauma Contagion
Anderson Jacob and McCarthy Veach (2005) were the only researchers to use the term “trauma contagion”. Specifically, Anderson Jacob and McCarthy Veach (2005) cited that this term came from Maltas and Shay’s (1995) trauma contagion model, which describes trauma contagion as consisting of (1) threatened beliefs and shattered assumptions, (2) chronic stress, and (3) repetition and re-enactment of facets of the vicarious trauma. Overall, the researchers concluded that their qualitative study supported the trauma contagion model, as female partners of male CSA survivors described each of the three aspects of trauma contagion.
Posttraumatic Stress/Posttraumatic Stress Disorder
PTS and PTSD were the most common terms used to describe the effect of exposure to a loved one’s interpersonal trauma. However, the definition of PTS/PTSD varied between articles. Moreover, despite noting that participants experienced PTSD symptoms, some researchers failed to define this (e.g., Masilo & Davhana-Maselesele, 2016; Smith, 2005; Vilvens et al., 2021).
Many researchers conceptualized PTS/PTSD in line with a Diagnostic Statistical Manual of Mental Disorders (DSM). For example, Newberger et al. (1993) referenced the DSM-III-R (APA, 1987) and reported that their findings were consistent with the diagnostic criteria for PTSD. Newberger et al. (1993) reported that their participants demonstrated avoidance (e.g., avoidance of trauma reminders), arousal (e.g., irritability), and diminished responsiveness (e.g., isolation). More recently, researchers referenced the DSM-IV (APA, 2000) definition of PTSD to describe participants’ symptoms of re-experiencing, avoidance, and arousal (Christiansen et al., 2012; Cyr et al., 2016; Timmons-Mitchell et al., 1996).
Other researchers defined PTS/PTSD in line with their measure of choice. This included defining PTSD/PTS as involving symptoms of intrusions and avoidance (Burgess et al., 1990; Cyr et al., 2018; Davies, 1995; Dyb et al., 2003; Kelley, 1990) or intrusions, avoidance, and hyperarousal (Jobe-Shields et al., 2016; Runyon et al., 2014; Van Delft et al., 2016). Although Fuller (2016) did not use any quantitative measures, they similarly discussed symptoms of intrusions as indicating the presence of PTSD.
Green et al. (1995) differed from other studies as they primarily referenced delayed PTSD. Green and colleagues conceptualized the parent’s experience of hyperarousal, intrusive memories and affect, and “psychic numbing” (undefined in the article) as delayed PTSD from their sexual abuse, which was catalyzed by their child’s abuse. In the discussion, Green et al. (1995) report that their findings are consistent with Herman’s (1992) definition of complex PTSD. This included having alterations in (1) affect regulation, (2) consciousness (e.g., amnesia, re-living experiences), (3) self-concept (e.g., feelings of guilt, shame, helplessness), (4) perception of the perpetrator, (5) relationships (e.g., withdrawal, distrust), and (6) systems of meaning (e.g., hopelessness, loss of faith).
Vicarious Traumatization
Bux et al. (2016) highlighted a previous definition of VT from Pearlman and Mac Ian (1995) that described it as the exhaustion and dysfunction that results from empathic engagement with another’s traumatic experience. In their discussion, however, Bux et al. (2016) described VT as the disruption of participant’s beliefs/representations about trust, control, sense of self-worth, and sense of safety.
Secondary Traumatization
Manion et al. (1996, 1998) primarily used the term secondary traumatization. They first highlight that they modified the “developmental lifespan model” (Newberger & De Vos, 1988) of child sexual victimization to create the framework from which they understood secondary traumatization. This model recognized that the trauma experience begins with the abuse event, continues throughout the disclosure, and integrates individual, cognitive, and familial variables to predict parental functioning (Manion et al., 1996, 1998). In each article’s discussion, secondary traumatization was represented as the emotional distress parents experienced following the disclosure of their child’s sexual abuse (Manion et al., 1996, 1998). Bux et al. (2016) parallel VT to Manion et al. (1996) definition of secondary traumatization. Sparks and Stoppa (2022) gave a more specific definition of secondary traumatization, referencing that it involves participants’ re-experiencing of the abuse, hyperarousal, and negative thoughts and emotions. Lastly, other researchers mention secondary traumatization (e.g., Christiansen et al., 2012) without defining it.
Secondary Traumatic Stress
Four studies mentioned STS. First, Gregory et al. (2017) referenced STS but did not define it; however, in their discussion, they described that their participants experienced anger, fear, sadness, helplessness, disruptions to sleep, and disruptions to core beliefs. They suggested that this supports that individuals providing informal support to survivors of DV are at risk for STS. Mangold et al. (2021) also researched STS, specifically with nonoffending caregivers of children who endured sexual or physical abuse. They defined it as a “set of psychological symptoms that mimic posttraumatic stress disorder” (p. 553) in the parents. Third, Nelson and Wampler (2002) vacillated in their study between the terms theory of secondary trauma, secondary traumatization, and STS, where each term was used to describe the intrapersonal and interpersonal problems suffered by partners of trauma survivors. Finally, Van Delft et al. (2016) mentioned STS, but they did not define it.
Systemic Trauma
Kilroy et al. (2014) defined systemic trauma as the experience of going through an event that causes disruption and distress to systems within and outside the person that experienced the trauma. For instance, they conceptualized that “systemic trauma” means that family context, abuse characteristics, emotions, cognitions, support systems, daily life, coping, and family dynamics are all either impacted by or are moderators of having your child experience sexual abuse. Similarly, Sparks and Stoppa (2022) reference Kilroy et al. (2014) findings on systemic trauma in their discussion.
Vicarious Posttraumatic Growth
Cummings (2018) was the only researcher to define VPTG. Cummings (2018) suggested that the last stage of their model, Thriving Recovery, is consistent with models of posttraumatic growth (e.g., Arnold et al., 2005; Tedeschi & Calhoun, 2004) as parents met the three necessary qualities: (1) challenges to schemas, (2) distress caused by a stressor, and (3) cognitive processing. Additionally, Cummings (2018) noted two differences between their model of parental recovery and posttraumatic growth. First, their model described the purpose of shattered views/schemas, which was to give the parent the energy and motivation to heal the child. Second, parents did not discuss meaning-making, which is typically a component of posttraumatic growth. Vilvens et al. (2021) and Anderson Jacob and McCarthy Veach (2005) described recovery and healing, respectively, but did not mention VPTG.
Measures
The measures used to examine the terms were the Impact of Event Scale (IES; Horowitz et al., 1979), Impact of Event Scale-Revised (IES-R; Weiss & Marmar, 1997), Harvard Trauma Questionnaire (HTQ; Mollica et al., 1992), Modified PTSD Symptom Scale-Self-Report (MPSS-SR; Falsetti, et al., 1993), French-Canadian Modified PTSD Symptom Scale (MPSS-FC; Stephenson et al., 2000), Posttraumatic Stress Disorder Symptom Scale-Self Report (PSS-SR; Foa et al., 1993), Purdue Posttraumatic Stress Disorder, Revised (PPTSD-R; Lauterbach & Vrana, 1996), Symptom Checklist 90-Revised (SCL-90-R; Derogatis, 1977), Brief Symptom Inventory (BSI; Derogatis & Spencer, 1982), Structured Clinical Interview for DSM-IV (SCID; First et al., 1995), and Posttraumatic Stress Disorder Checklist for the DSM‑5 (PCL-5; Blevins et al., 2015). The most frequently used measure was the IES.
Knowledge Gaps
There were several knowledge gaps identified in this scoping review. These included: (1) unified definitions of trauma contagion, systemic trauma, secondary traumatization, STS, PTS/PTSD, and VT, (2) clarification on the differences, if any, between each of the terms, (3) quantitative research on VPTG in this population, including identification or creation and validation of an appropriate measure, (d) samples that focus on paternal parents, LGBTQIA+ partners, siblings, and friends, and (e) samples, particularly in the USA and Canada, that focus on the experience of Black, Indigenous, and People of Color (BIPOC).
Discussion
To our knowledge, this is the first scoping review on VT and VPTG in loved ones indirectly exposed to interpersonal trauma. Scoping reviews do not evaluate the quality or conclusions of the literature; rather, they provide a novel inventory of the research on a topic. Thus, this scoping review is an easily accessible catalog of literature on experiences of VT and VPTG for loved ones indirectly exposed to interpersonal trauma. This resource may be used to transfer knowledge to researchers and clinicians and illustrate areas needing further elucidation, cohesiveness, or future research. Specifically, our scoping review aimed to map the definitions, methods, tools/measures, demographics, key findings, and knowledge gaps related to the outcomes of interest. Tables 3, 4, 5, and 6 summarize our data and illustrate that there was a variety of research on VT in loved ones indirectly exposed to interpersonal trauma, which also meant variability in the terms, definitions, tools, and key findings related to VT. On the other hand, there was a paucity of research on VPTG and samples with diverse demographics. Provided below is an overview of the key findings and the associated recommendations. Table 7 summarizes these key findings.
Implications for Research, Practice, and Policy.
Note. STS = secondary traumatic stress; VPTG = Vicarious posttraumatic growth; VT = vicarious traumatization.
Summary of Major Findings.
Note. PTS = posttraumatic stress; PTSD = posttraumatic stress disorder; STS = secondary traumatic stress; VPTG = Vicarious posttraumatic growth; VT = vicarious traumatization.
Key Findings and Recommendations
Demographics
Majority of the studies examined samples of parents/caregivers (22 articles or 79%), with minimal research on siblings (2 articles), friends (2 articles), partners (4 articles), and paternal caregivers (14 articles). This is surprising, considering that siblings, partners, and friends are often disclosed to for interpersonal traumatic events (Dworkin et al., 2016; Orchowski & Gidyca, 2012). This indirect interpersonal trauma exposure then leaves them at risk for VT, yet we found limited research on VT and VPTG for these populations. Furthermore, most studies had samples that were predominantly White/Caucasian, and there were no studies with gender- or sexuality-diverse samples. This leaves gaps in certain demographics that should be studied in future research. Research with individuals identifying as LGBTQIA+ and BIPOC is particularly important considering that individuals with these identities are at an increased risk of experiencing violence (Statistics Canada, 2020, 2021a, 2021b). This means that family, partners, and friends of these individuals, who may also be a part of the same communities, are at an increased risk of being indirectly exposed to interpersonal trauma. There may also be important cultural differences in the experiences of VT and VPTG that will not be elucidated if there is no research in these populations.
Definitions
One finding was the variable vocabulary used to describe the traumatization of a loved one after indirect interpersonal trauma exposure. For example, the terms trauma contagion, PTS/PTSD, VT, secondary traumatization, STS, and systemic trauma were used. Even further, researchers who used similar terms often had variability in their definitions. This variance in the indirect trauma literature has been noted previously by Branson (2019), although their literature review focused on clinicians being affected by their clients’ trauma(s).
Furthermore, the symptom profiles for VT terms were relatively similar: most described some variation of PTSD symptoms. Hence, should there be different definitions based on how the symptoms were acquired? Wies and Coy (2013) argued that the difference between vicarious trauma and PTSD was that the former involved the traumatic event being acquired indirectly while the latter involved firsthand experience. However, the DSM-5 (APA, 2013) includes indirect exposure to a loved one’s trauma in criterion A of PTSD rather than giving a separate diagnosis based on exposure. Consequently, it may neither be necessary to have a separate term that delineates the timeline nor type of exposure if the pathology remains the same. This then raises the question of whether using PTS/PTSD alone is sufficient in the literature. However, there is utility in the quick access to research in the population of interest when terms such as VT are used, as PTS/PTSD is likely to bring up research on primary trauma survivors.
Overall, vocabulary management is a necessary step forward in this area of research, potentially through the collaboration of an expert panel of researchers and stakeholders in this area. Clearly delineating the definitions of each term, operationalizing them, using the correct terms in future research, and halting the interchanging of terms is necessary for researchers and clinicians to easily find applicable research. Without it, researchers may be overlooking relevant articles in their literature reviews or unnecessarily duplicating previous research.
Measures
We found no studies in this scoping review that used specific measures of VT. This is despite 16 quantitative studies of VT where researchers used measures originally developed for direct trauma survivors. This was surprising considering there are measures that assess VT in the literature. For example, the STS Scale, a 17-item self-report scale whose items correspond to the 17 PTSD symptoms on the DSM-IV-TR (APA, 2000), was developed by Bride et al. (2004). Another measure in the literature on professionals indirectly exposed to trauma is the Vicarious Trauma Scale (Aparicio et al., 2013). However, neither of these measures were used by researchers in this scoping review. If terms apart from PTSD/PTS continue to be used for research on loved ones, researchers should apply the above measures to this population and assess the psychometric properties.
There were no quantitative studies that examined VPTG in this scoping review, and thus there were no measures of VPTG highlighted. The lack of validated measures for VPTG seems to be similar in populations beyond loved ones. For example, Manning-Jones et al.’s (2015) review of 28 articles on VPTG in working professionals, and Tsirimokou et al.’s (2023) review of 15 articles on VPTG in mental health professionals both noted that there were no validated quantitative measures on VPTG. These results indicate that it would be worthwhile for researchers to develop and validate measures of VPTG in populations of loved ones indirectly exposed to an interpersonal trauma.
Outcomes
Overall, there were 26 articles involving VT and related terms in this scoping review. Although analyzing the outcomes of these studies was beyond the scope of this review, the key findings ranged from quantifying VT (e.g., PTS symptoms), qualitatively describing the experience of VT, and examining variables related to VT (Table 5). These studies illustrated that VT is possible for loved ones indirectly exposed to trauma across populations of caregivers, significant others, friends, and other close individuals. For example, the prevalence of meeting criteria for PTSD across studies ranged from 13.1% to 32% for mothers, 7.1% to 7.3% for fathers, and 26% for close others (Christiansen et al., 2012; Cyr et al., 2016). Likewise, when researchers discussed high or clinically significant PTS/PTSD symptom scores, the prevalence ranged from 0% to 3.3% for fathers, 10.2% to 38.9% for mothers, and 14% to 24% for caregivers overall (Cyr et al., 2018; Jobe-Shields et al., 2016; Mangold et al., 2021; Van Delft et al., 2016). Other studies used similar classifications to look at prevalence rates for specific symptoms (Davies, 1995; Dyb et al., 2003). Quantitatively, VT commonly involved examining intrusions/re-experiencing, avoidance, and/or arousal symptoms (Burgess et al., 1990; Christiansen et al., 2012; Cyr et al., 2016, 2018; Davies, 1995; Dyb et al., 2003; Jobe-Shields et al., 2016; Manion et al., 1996, 1998; Nelson & Wampler, 2002; Runyon et al., 2014; Timmons-Mitchell et al., 1996; Van Delft et al., 2016), which differs from the current DSM-5 criteria of intrusion symptoms, avoidance, negative alterations to cognitions and mood, and changes to arousal and reactivity (APA, 2013). Only Mangold et al. (2021) using the PCL-5 reported on all DSM-5 PTSD symptoms. Qualitatively, outcomes of VT spanned cognitive, relational, emotional, spiritual, behavioral, and physical domains for participants (Anderson Jacob & McCarthy Veach, 2005; Bux et al., 2016; Fuller, 2016; Green et al., 1995; Gregory et al., 2017; Kilroy et al., 2014; Masilo & Davhana-Maselesele, 2016; Smith, 2005; Sparks & Stoppa, 2022; Van Wijk et al., 2014; Vilvens et al., 2021).
Furthermore, there were a variety of variables examined for their relationship to VT. These included, but are not limited to, testifying in court (Burgess et al., 1990; Dyb et al., 2003), time since disclosure (Cyr et al., 2018; Mangold et al., 2021; Manion et al., 1998), gender of participants (Cyr et al., 2016; Dyb et al., 2003; Kelley, 1990; Mangold et al., 2021; Manion et al., 1996, 1998; Nelson & Wampler, 2002), parental discipline (Jobe-Shields et al., 2016), stress (Cyr et al., 2016; Kelley, 1990), general psychological well-being (Dyb et al., 2003), depression (Runyon et al., 2014), locus of control (Dyb et al., 2003), secondary life changes (Dyb et al., 2003), perceived child symptomology (Mangold et al., 2021; Manion et al., 1996), sexual disgust sensitivity (Van Delft et al., 2016), abuse characteristics (Dyb et al., 2003; Kelley, 1990; Manion et al., 1996; Van Delft et al., 2016), and parental trauma history (Mangold et al., 2021; Manion et al., 1996; Timmons-Mitchell et al., 1996; Van Delft et al., 2016).
There was minimal research on VPTG in this population; VPTG was only discussed by Cummings (2018). In a systematic literature review by Manning-Jones et al. in 2015, they found 28 articles related to VPTG. However, family members of direct trauma survivors were excluded from this review, as their experience was seen as direct rather than indirect trauma exposure. Therefore, it could be the case that researchers were not using the term VPTG to describe positive changes to cognitions, emotions, relationships, and spirituality following loved ones’ indirect interpersonal trauma exposure or that loved ones are an overlooked population in the field of VPTG research. Furthermore, because there is minimal research on VPTG in the population of interest, there is not yet literature that describes the relation of VPTG to other factors (e.g., STS). Consequently, this current study further emphasized the need for more research in this area.
Limitations
A limitation of this scoping review was the narrow definition of interpersonal trauma at an individual level. Research on intergenerational trauma, community-, war-, and terrorism-based traumas were therefore excluded from this study as they represent collective traumas (Hirschberger, 2018). Further, majority of the articles were identified from the string search; this may indicate that the search terms were not broad enough. As well, the limitation of the overrepresentation of articles from Canada and the USA may be due to the English language inclusion criteria. Another limitation was that research discussing experiences such as improved relationships without using the terms of interest (e.g., VPTG) were excluded. For that reason, these outcomes may be discussed in research that captures them under other constructs. Lastly, scoping reviews do not evaluate the collated research, nor do they perform thematic analyses of the collected data; thus, a higher-level analysis of the data beyond the presentation of what is known and needs to be known was beyond the scope of this review.
Implications
The major implications for practice, policy, and research are outlined in Table 6. Overall, this scoping review informs future research to fill necessary knowledge gaps to further this area of study. In terms of practical implications, this scoping review validates that loved ones are a population deserving of attention and intervention following indirect trauma exposure, as they experience VT and could benefit from direct services to address PTSD symptoms. This is particularly important given that loved ones are often the people that survivors turn to for support following interpersonal trauma. Previous research has demonstrated that caregivers of children who have experienced trauma are often met with blame by professionals who are meant to help the family recover (Plummer & Eastin, 2007). By mapping the literature, practitioners can be informed of target areas for intervention such as PTSD. Our scoping review indicates that siblings, friends, paternal caregivers, and partners are particularly overlooked in this area. In addition, there is a paucity of research involving gender- and sexuality-diverse participants as well as BIPOC.
Our scoping review also reveals implications for using terms and definitions within this subfield, as researchers used various terms to refer to the same constructs. It is necessary to delineate the terms’ definitions and operationalize them. In addition, halting the interchanging of terms will streamline research in this area and allow for easier access by researchers and clinicians seeking information in this area.
Our results also have implications for measuring vicarious experiences after interpersonal trauma. Two priorities emerge from our results: creating and validating a measure for VT and VPTG in loved ones and assessing the psychometric properties of existing measures for STS and VT in loved ones.
Conclusion
This scoping review was the first study to compile and summarize the literature on VT and VPTG of loved ones indirectly exposed to interpersonal trauma. It clarified the variety of definitions, methods, tools/measures, demographics, and key findings in these areas. By doing so, important knowledge gaps and issues pertaining to these constructs were illuminated. Further discussed were areas warranting future research related to these knowledge gaps and practical implications for those working with families who have experienced interpersonal trauma.
Footnotes
Author Note
This research was completed as part of the doctoral dissertation of Whitney Willcott-Benoit. Funding was provided by the Centre for Forensic Behavioral Sciences and Justice Studies at the University of Saskatchewan and the Social Science & Humanities Research Council of Canada, both awarded to Whitney Willcott-Benoit.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.