
Abstract
Globally, it is estimated that 245 million women and girls aged 15 and over have experienced intimate partner violence (IPV) in the past 12 months. Moreover, research has highlighted the disproportionately high prevalence of IPV victimization among pregnant women. IPV can have serious health implications for women and their infants, yet little is known about maternal health-related decision-making by mothers exposed to IPV. To this end, the purpose of this scoping review was to examine what is known regarding health-related maternal decision-making among perinatal women in the context of IPV. Using Arksey and O’Malley’s framework, five electronic databases were searched, resulting in 630 articles. Eligible articles were primary studies written in English, included participants who experienced IPV at any time in their life, and reported results focused on maternal health-related decision-making in the context of IPV. Thirty-six articles were screened by the review team, resulting in seven included articles. Three main themes emerged regarding health-related maternal decision-making by mothers experiencing IPV, including suboptimal breastfeeding practices, under-utilization of maternal and child health services, and poor adherence to medical recommendations/regimens that impact health-related outcomes for mother and child. The well-established risk of poorer health outcomes among women experiencing IPV, alongside the findings of this scoping review, calls for further research specifically addressing health-related decision-making among perinatal women who experience IPV.
Keywords
Introduction
Intimate partner violence (IPV) is a global public health concern and a human rights violation reaching epidemic proportions (Chisholm et al., 2017; Krantz & Garcia-Moreno, 2005; Maheu-Giroux et al., 2022). Defined as a pattern of physical, sexual, or emotional violence perpetrated by a current or former intimate partner in the context of coercive control (Tjaden & Thoennes, 2000), IPV is one of the most common types of violence against women transcending all social and geographical locations and cultural backgrounds (Miller & McCaw, 2019). The World Health Organization (WHO) has declared IPV to be devastatingly pervasive, reporting global findings that one in three women experience violence by an intimate partner across their lifetime (WHO, 2021). Furthermore, research has highlighted the disproportionately high prevalence of IPV victimization among pregnant women, with global estimates ranging from 15% to 40.5% of pregnant women being impacted (Román-Gálvez et al., 2021).
Literature is abundant regarding the specific and harmful effects IPV exposure can have on the health and well-being of pregnant women, including serious physical, behavioral, and psychological issues (Hellmuth et al., 2012; Miller & McCaw, 2019). For example, these issues may be associated with unintended pregnancy, sexually transmitted infections, or human immunodeficiency virus infection (Hellmuth et al., 2012; Miller & McCaw, 2019). In addition, IPV exposure increases the risk of obstetrical and gynecological complications such as preterm birth, low birth weight, pregnancy-related death, and miscarriages (Miller & McCaw, 2019; WHO, 2013). Research has also demonstrated that stress related to IPV can impair immunological functioning; as such, IPV is linked to an increased risk of infectious complications in pregnancy such as pyelonephritis and chorioamnionitis (Chambliss, 2008). Given the risks associated with IPV, suspected or disclosed IPV during pregnancy results in the pregnancy itself being considered high-risk (Miller & McCaw, 2019).
Prenatal care is considered the most important mechanism for identifying possible adverse outcomes of pregnancy (WHO & UNICEF, 2003). Additionally, prenatal appointments may provide health care providers (HCPs) with an important opportunity for both IPV screening and connecting women with prenatal mental health interventions and IPV support services (Miller & McCaw, 2022). However, pregnant women who have experienced IPV often endure social and emotional barriers which may result in delaying or missing prenatal care (Alhusen et al., 2015; Tura & Licoze, 2019). As a result of poor uptake of prenatal care services, negative pregnancy outcomes can be exacerbated and simultaneously impacted by a partner’s controlling behaviors. Ultimately, this intersection of factors may limit a mother’s ability to make decisions regarding their health (Tura & Licoze, 2019).
Maternal decision-making refers to mothers acting as the primary authorities on childrearing decisions and is defined by a lack of co-parental collaboration relative to shared decision-making (Kincaid, 2021). In contrast to shared parental decision-making—where parents pool their cognitive and emotional resources to make decisions for the well-being of their children—maternal decision-making refers to the reliance on only the woman’s mental labor and resources to make those decisions (Kincaid, 2021). Inherent in maternal decision-making is a woman’s autonomy. Women’s autonomy refers to a woman’s ability and freedom to act independently, which includes participating in decision-making and the capability to articulate strategic choices (Kincaid, 2021). While research suggests that highly autonomous women have the power to act independently for better health (Gautam & Jeong, 2019) in the context of IPV, exercising autonomy via health-related decision-making may actually increase the likelihood of all forms of IPV (Rahman et al., 2011). While the concept of maternal decision-making has not been well explored, it has been linked to the theory of reasoned action/planned behavior (Glanz et al., 2002; Velonis et al., 2017). This theory purports that the opinions of others (i.e., in the context of IPV, which generally refers to the partner) may have undue influence on an individual’s behavior (Glanz et al., 2002). This theory goes further to specify between three avenues that may influence one’s behavior, including: (1) behavioral beliefs (e.g., mother’s attitudes toward breastfeeding); (2) normative beliefs (e.g., partner/healthcare provider’s attitudes toward prenatal care uptake); and (3) control beliefs (e.g., mother’s perceived ability to make an informed, autonomous decision about immunization) (Etheridge et al., 2023). Overall, this theory provides a foundation for understanding the influences that may be present on a mother’s ability to make health-related decisions.
Although health-related decisions are an important part of maternal and child/fetal health and overall well-being, research examining maternal decision-making toward health-related issues in the context of IPV within the pregnancy and postpartum period is scant. While many studies have focused on the health-related decisions of service utilization among pregnant mothers (e.g., Metheny & Stephenson, 2017; Musa et al., 2019; Sebert Kuhlmann et al., 2017), fewer have focused on health-related decisions in general that extend beyond the use of services (e.g., immunization choices). For example, in a recent systematic review and meta-analysis by Musa and colleagues (2019), experiences of IPV were associated with a lower likelihood of receiving adequate antenatal care. While service utilization is an important factor in the health and well-being of mothers and children, solely focusing on this while ignoring other health-related decisions during the pregnancy and postpartum period may overestimate the impact of service utilization and/or fail to recognize equally important decisions that can impact health. Ultimately, gaining a thorough understanding of broad maternal health-related decisions in the context of IPV will allow for more effective and equitable support toward optimal health and well-being among mothers and children. To further generate knowledge and understanding of this understudied area, this scoping review aims to examine what is known from existing literature regarding health-related maternal decision-making among perinatal women in the context of IPV.
Methods
Design
This scoping review was in full accordance with the PRISMA guidelines (Tricco et al., 2018) and conducted using the five-step methodological framework developed by Arksey and O’Malley (2005) and further advanced by Levac et al. (2010). Given the very limited literature focused on the intersections of IPV and maternal decision-making among perinatal women, a scoping review was undertaken to determine the range, extent, and nature of research activity to-date and to identify gaps in the existing literature (Arksey & O’Malley, 2005). The five-step process includes identifying the research question, identifying relevant studies, selecting studies, charting the data, collating/summarizing, and reporting the results (Arksey & O’Malley, 2005). The broad objectives of scoping reviews aim to map the key concepts and empirical findings underpinning a research area (Arksey & O’Malley, 2005). In accordance, the purpose of this scoping review was to synthesize the current understanding of the ways in which IPV contributes to maternal health decision-making in the perinatal period, inclusive of conception to 12 months postpartum.
Stage 1: Identifying the Research Question
According to Levac et al. (2010), a broad research question with a clearly articulated scope of inquiry is recommended for identifying studies and discerning inclusion criteria to establish an effective search strategy. In accordance with this, the research question for this scoping review was, “What is known from existing literature about health-related maternal decision-making in the perinatal period in the context of IPV?”
Stage 2: Identifying Relevant Studies
In collaboration with our institutional librarian, the authors developed search terms to reflect the key concepts of perinatal, decision-making, and IPV (see Appendix A). Searches were completed from February to April, 2022, using the following five electronic databases: Medline, CINAHL, PsycINFO, SCOPUS, and EMBASE. No publication date parameters were set, and the search was restricted to articles written in English. Lastly, the search from each reference database was extracted in a RIS file and imported into Covidence Software (Covidence Systematic Review Software, 2019) for a robust review by two of the authors (see Appendix B).
Stage 3: Study Selection
Two authors independently conducted the initial screen of titles and abstracts (n = 433), with disagreements resolved through discussion until a consensus was reached. Levac et al. (2010) suggest two reviewers should independently review full articles for inclusion and exclusion criteria after performing reiterative stages of the abstract review process. As such, we modified inclusion and exclusion criteria as a team after gaining a more thorough understanding of the literature, representing a “best fit” with the proposed research question (Arksey & O’Malley, 2005). Inclusion criteria consisted of: (1) primary research studies, (2) articles written in English, (3) perinatal women who experienced IPV at any time, and (4) study results that focused on maternal health-related decision-making in the context of IPV. For the purpose of this review, maternal was defined as a biological mother within the perinatal period, specifically from the time of conception to 12 months postpartum. Maternal decision-making refers to a lack of co-parental collaboration relative to shared decision-making (Kincaid, 2021). IPV is commonly cited as a pattern of physical, sexual, and/or emotional violence by an intimate partner within the context of coercive control (Tjaden & Thoennes, 2000). Given that coercive control is a defining factor of IPV (Tjaden & Thoennes, 2000) and its potential impact on health-related decision-making, studies were excluded if they solely focused on shared decision-making. Finally, articles were excluded if maternal decision-making was not health-related in nature, if some form of the decision-making was not exclusive to the mother, or if IPV was not experienced by participants.
Stage 4: Charting the Data
The data extraction tool was collectively developed by team members with pertinent variables used to sufficiently answer the research question under purview (Levac et al., 2010). The data extraction tool included author(s), year of publication, country of origin, study purpose, sample size, participant demographics, stage of motherhood, methodology, intervention descriptions, conceptualization of IPV, and outcomes of maternal health decision-making. Data extraction was an iterative process in which team members continuously updated the data extraction tool. Researchers independently extracted data from the selected articles and met to ensure the approach to data extraction was sufficient at addressing the research question and purpose of the review. A descriptive analytical method—a narrative review used to extract contextual and process details from each study (Arksey & O’Malley, 2005)–was used to identify trends and relationships in the data. To enhance our analysis, and to further explore and organize the data into themes, we simultaneously employed an iterative and collaborative (across the three reviewers) qualitative content analysis approach as proposed by Levac and colleagues (2010). This approach assisted with elucidating consistencies and meaning across the data through the systematic identification of patterns and/or themes. No modifications were made to the original data in this review, meaning that all data found in the data extraction table are presented in the form of the original authors.
Stage 5: Collating, Summarizing, and Reporting the Data
Numerical and conceptual analyses were undertaken by two reviewers who then reviewed and compared the results. Numerical analysis identified the nature, extent, and distribution of included studies (e.g., sample size, mean age of participants, etc.) by arranging the findings across all seven studies included in this review. Thematic analysis (Braun & Clarke, 2006) was then conducted by two members of the research team to examine commonalities, differences and specific characteristics of health-related maternal decision-making in the context of IPV. The final themes were determined by reaching a consensus through discussion among the team.
Results
A total of seven articles met the eligibility criteria for inclusion in this review. The initial search yielded 630 articles which were imported for screening in Covidence (Covidence Systematic Review Software, 2019)—a primary screening and data extraction tool—removing 197 duplicates automatically. A total of 433 studies were screened using titles and abstracts, resulting in the exclusion of 396 articles that did not meet the inclusion criteria. Next, the 36 remaining eligible articles were screened for full-text eligibility, resulting in the exclusion of 29 studies. Seven articles remained for inclusion in this review (see Appendix B for a list of excluded studies and rationales for exclusion).
The following section presents findings pertaining to diversity among the included studies. Next, the findings from the numerical and thematic analyses are described. There was a natural divide in the literature that emerged addressing maternal decision-making regarding breastfeeding practices and studies discussing the utilization of health care services. Two studies also discussed adherence to medical recommendations and treatment regimens in the antenatal and postpartum periods. A summary of critical findings can be found in Table 1.
Summary of Critical Findings.
IPV = intimate partner violence.
Diversity
The discussion of diversity was largely absent among the included studies. While age was considered by all of the included studies, characteristics such as religion, sexual orientation, and disability were not. All of the included studies focused on women who had given birth, yet none of the studies considered (either in the inclusion criteria or data collected) specifically asked about gender identity. Two of the included studies, both conducted in the United States, collected baseline demographic data on race (Bair-Merritt et al., 2008; Wallenborn et al., 2018), whereas the study conducted in in Nepal collected data on ethnic affiliation (caste). However, on whole, the literature included in this review failed to adequately consider diversity; as such, this remains a gap in the literature requiring further research.
Numerical Analysis
Study Design
Publication dates of included articles ranged from 2007 to 2020. Six studies included in this review employed quantitative methodologies (Caprara et al., 2020; Gautam & Jeong, 2019; Hampanda, 2016; Islam et al., 2017; Lau & Chan, 2007; Wallenborn et al., 2018), while one used mixed-methods (Bair-Merritt et al., 2008). With respect to the study design, five of the articles used cross-sectional data collection via surveys (Gautam & Jeong, 2019; Hampanda, 2016; Islam et al., 2017; Lau & Chan, 2007; Wallenborn et al., 2018), one article was a retrospective longitudinal study (Bair-Merritt et al., 2008), and another used a longitudinal observational study design across four time periods (Caprara et al., 2020).
Geographical Location and Patient Population
The seven studies included in this review spanned across the globe, with two based out of the United States (Bair-Merritt et al., 2008; Wallenborn et al., 2018) and one from each of the following countries: Zambia (Hampanda, 2016), China (Lau & Chan, 2007), Brazil (Caprara et al., 2020), Nepal (Gautam & Jeong, 2019), and Bangladesh (Islam et al., 2017). Participants in all studies included in this review included recent postpartum mothers exposed to IPV, with sample sizes ranging from 35 (Caprara et al., 2020) to 5002 (Wallenborn et al., 2018). Demographic characteristics are reported by each study in Table 2.
Data Extraction Chart.
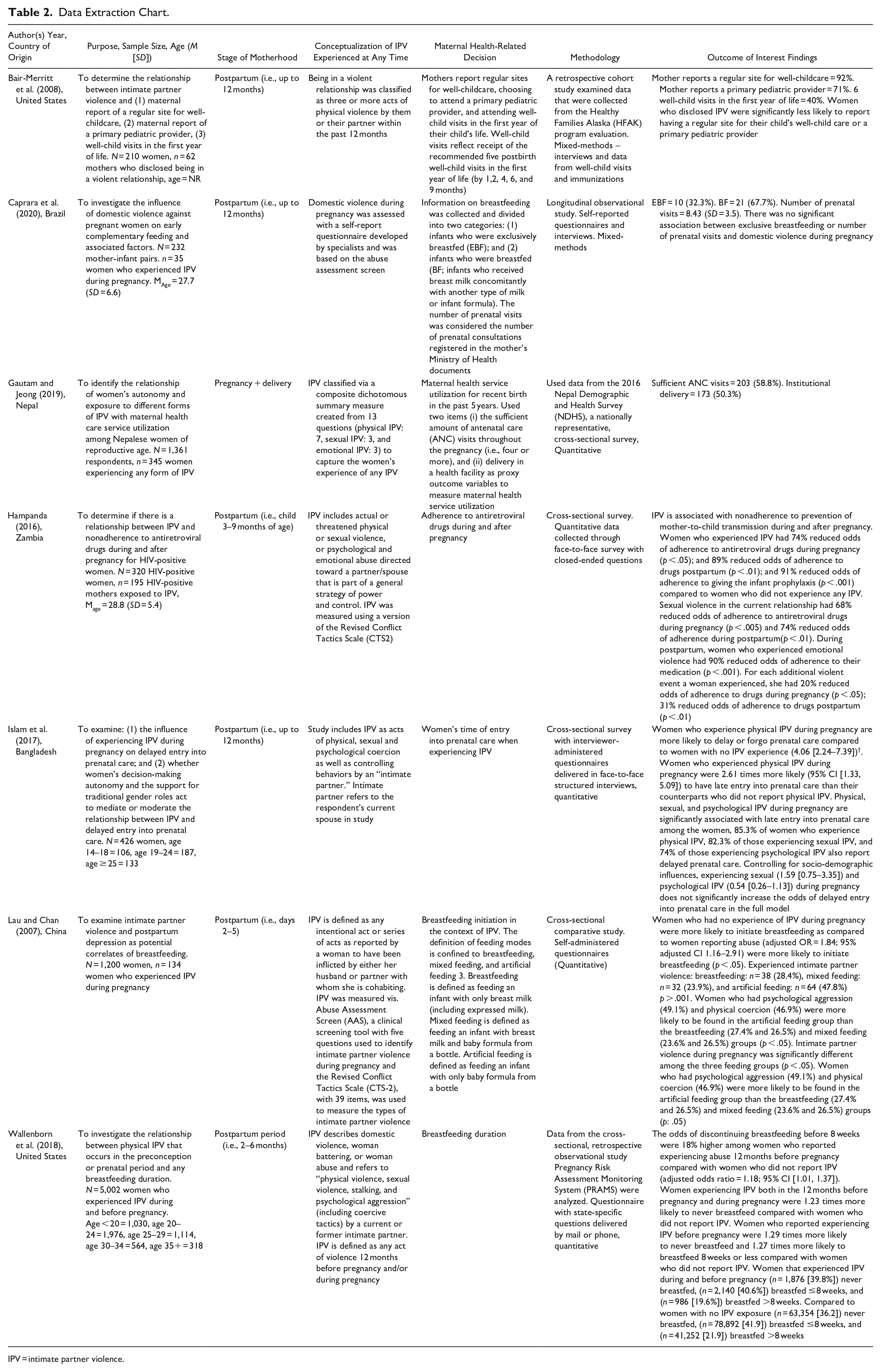
IPV = intimate partner violence.
Thematic Analysis
Enhancing Arskey and O’Malley’s scoping review methodology, Levac and colleagues (2010) recommended adding a qualitative thematic analysis to identify patterns and for meaning-making of the data. As such, we employed a thematic analysis across the extracted data from the included studies. This was an iterative, reflexive, and collaborative process conducted by the three reviewers, with discussions to reach a consensus. Analysis of studies included in this review revealed maternal health-related decisions in the pregnancy and postpartum period occurred around four predominant health-related themes with associated subthemes, including: (1) breastfeeding practices; (2) utilization of perinatal and well-baby appointments; (3) adherence to medical recommendations/regimes (with subtheme: trust in care provider); and (4) level of education.
Breastfeeding Practices
Three articles discussed decisions regarding breastfeeding practices and specifically examined the role of IPV on suboptimal breastfeeding practices (Caprara et al., 2020; Lau & Chan, 2007; Wallenborn et al., 2018). Findings indicated that mothers reporting IPV exposure were less likely to initiate breastfeeding in the immediate postpartum period, breastfed for shorter durations (i.e., 8 weeks or less), and were more likely to use mixed or formula feeding methods compared to mothers who did not experience IPV (Caprara et al., 2020; Lau & Chan, 2007; Wallenborn et al., 2018).
The issue of underlying stress in relation to breastfeeding practices by mothers exposed to IPV was also evident throughout the studies in this review. In the study by Lau and Chan (2007), partner support for breastfeeding practices was less commonly found in abusive relationships; in addition, stress stemming from abusive situations was linked to temporary disruption of milk production. In addition, mothers experiencing poor breastfeeding outcomes resulting from IPV-related stress were more likely to have poorer mental health outcomes (Wallenborn, et al., 2018). Wallenborn and colleagues (2018) found IPV affects perceived stress, and stress was a mediator to shorter breastfeeding duration.
Utilization of Health Care Services
An under-utilization of maternal health care services was an emerging theme in this review. Two articles found expectant mothers exposed to IPV during pregnancy were more likely to delay entry to prenatal care services (Gautam & Jeong, 2019; Islam et al., 2017). In addition to insufficient prenatal care, there was a lower utilization of institutional delivery among women who had experienced IPV (Gautam & Jeong, 2019). Women who reported a controlling partner were also less likely to use the recommended antenatal care services at regular intervals during their pregnancy (Gautam & Jeong, 2019). Finally, Bair-Merritt et al. (2008) found that women who experienced IPV were significantly less likely to have their children attend the recommended number of well-child checkups in the first year of life and were less likely to have a primary pediatric care provider.
Women with limited decision-making autonomy were found to delay seeking prenatal care, and this effect was exacerbated with exposure to physical IPV during pregnancy (Islam et al., 2017). Women experiencing abuse often had less decision-making autonomy, limiting one’s ability to make decisions regarding choices centering around health care services (Islam et al., 2017). Autonomy in the context of IPV was also found to be influenced by gender-based beliefs, education level, and age among participants included in the studies (Gautam & Jeong, 2019; Islam et al., 2017). For example, low levels of women’s autonomy associated with IPV were correlated with lower utilization of maternal health care services, particularly prenatal and postnatal care (Gautam & Jeong, 2019). Interestingly, Gautam and Jeong (2019) revealed sufficient utilization of ANC visits was found among couples who were equally educated, while women who were more educated than their partner were more likely to deliver in a health facility despite IPV exposure in the relationship.
Adherence to Medical Recommendations/Regimens
A final theme that emerged from the data was poor maternal adherence to medical recommendations for maternal and infant health when exposed to IPV. Medical recommendations refer to best practices that promote optimal health and well-being for both mothers and their infants. For example, Bair-Merritt et al. (2008) found children born to women experiencing IPV were significantly less likely than their peers to be up-to-date on recommended immunizations by 24 months of age. Further, Hampanda (2016) found that HIV-positive women exposed to IPV were significantly associated with nonadherence to antiretroviral medication to prevent mother-to-child transmission during and after pregnancy and 91% reduced odds of adherence to infant prophylaxis compared to women not experiencing IPV. Finally, the severity of IPV resulting in physical injury was directly associated with nonadherence to infant HIV prophylaxis, whereby the severity of violence was shown to have a direct dose-response relationship with IPV, where more frequent and severe exposure to IPV increased the likelihood a woman would be nonadherent to a prolonged medication regimen (Hampanda, 2016).
Trust in Care Provider
The concept of trust was a common theme among studies related to nonadherence to perinatal medical recommendations experienced by pregnant and postpartum women experiencing IPV. For example, for optimal maternal and child health outcomes a trusted primary health care provider was critical to ensuring regular attendance of child wellness visits (Bair-Merritt et al., 2008). Bair-Marritt et al. (2008) found that women exposed to IPV tended to trust their child’s HCP less, driven by less favorable communication with their provider and an overall lower quality provider-caregiver relationship. Additionally, Hampanda (2016) found longer duration of antiretroviral therapy treatment regimens to prevent maternal-to-infant HIV transmission during and after pregnancy were more difficult to adhere to without the knowledge, support, and permission of a partner.
Level of Education
Level of education was the most common subtheme that emerged across all the main health-related themes for maternal decision-making in the context of IPV. Higher levels of maternal education attainment were linked to increased uptake of health-related services and participation in optimal breastfeeding practices (Caprara et al., 2020; Hampanda, 2016; Gautam & Jeong, 2019). Caprara et al. (2020) found each additional year of any level of education was a protective factor against breastfeeding cessation. Gautam and Jeong (2019) found women with a higher level of education compared to their partner were more likely to use a health facility with a skilled provider for delivery, and women with equal levels of education to their partner had sufficient utilization of ANC services in pregnancy (Gautam & Jeong, 2019). Interestingly, a study of heterosexual couples by Islam et al. (2017) found a husband’s level of education influenced the uptake of prenatal care visits; specifically, those with higher levels of education (beyond secondary) were more likely to have partners who accessed early prenatal care.
Discussion
This scoping review examined the extent, range, and nature of research activity related to health-related maternal decision-making for mothers experiencing IPV. The findings of this review reveal the complexities of maternal health decision-making in the context of IPV. The major findings of this scoping review revealed that IPV may play a role in how women in the perinatal period make health-related decisions, particularly with respect to breastfeeding practices, utilization of health services, and adherence to medical recommendations related to childbearing and children’s health. A summary of implications for practice, policy, and research can be found in Table 3.
Summary of Implications for Practice, Policy, and Research.
IPV = intimate partner violence.
Suboptimal breastfeeding practices, including low initiation, exclusivity, and early discontinuation rates of breastfeeding exclusivity found in this review, are echoed in other studies where women experienced IPV before or during their pregnancy. Misch and Yount (2014) examined the association of IPV with early initiation and exclusive breastfeeding in eight African countries and found that regardless of the type of IPV (e.g., physical, emotional, or sexual)—which varied across countries—breastfeeding initiation and exclusivity rates were negatively impacted by all forms of IPV exposure in at least one setting. Conversely, one Brazil-based study included in our review found there was no relationship between IPV against pregnant women and the early introduction of complementary feeding and/or breast milk substitutes. A potential rationale for the study’s findings was the sample of mothers participating in the study were young, under-educated women who are more likely to formula feed regardless of IPV exposure (Caprara et al., 2020).
The theme of under-utilization of maternal health services for expectant and postpartum mothers with histories of IPV emerged in three articles in this scoping review. Similar findings were also revealed in other studies. A population-based study in Brazil found that physical IPV was significantly associated with delayed onset of prenatal care, attending less than the six recommended prenatal care visits, and inappropriate use of prenatal care resources (Carneiro et al., 2016). Interestingly, a scoping review (Metheny & Stephenson, 2017) examining the utilization of ANC services by those experiencing IPV found a lack of attendance in recommended ANC visits was associated with low levels of decision-making autonomy – an identified subtheme underscoring poor utilization of health care services found within this review. Our scoping review also highlighted the limitations IPV places on woman’s autonomy, which impacts health-related decision-making. Together, these findings suggest that the effect of IPV on women’s autonomy may lead to under-utilization of antenatal health care supports and less favorable health outcomes for both mothers and infants.
Another major finding of this review pertained to the linkage between maternal experiences of IPV and attendance at well-baby visits. For example, the U.S.-based study included in this scoping review (Bair-Merritt et al., 2008) reported that children of IPV-exposed mothers were less likely to attend the recommended five well-child visits within the first year of life, obtain a primary pediatric care provider, and were significantly less likely to be fully immunized by 2 years of age compared to children of mothers not exposed to IPV. In this study, a lack of engagement in proactive pediatric care was associated with a lack of trust and an overall poorly perceived quality of the caregiver-provider relationship. However, contrasting findings were also found in the literature (Kornfeld et al., 2012; Martin et al., 2001), where two U.S. studies found no differences in infant/child well-visits within the first 2 years of life between children of IPV and nonexposed mothers. While literature on the utilization of well-child visits in the first year of life in the context of IPV is limited, it has been identified that women who experience IPV are less likely to seek health care for fear of repercussions and child-protection concerns (Taket et al., 2003). Given this, further research addressing this area is required.
The final theme of adherence to maternal and child medical recommendations and treatment regimens emerged in two of the seven articles included in this review pertaining to infant immunizations and HIV preventive medications. Lack of adherence to medical recommendations, specifically regarding antiretroviral therapy (ART) was also discovered in a recent Kenyan study by Biomndo et al. (2021) identifying IPV as an independent risk factor for suboptimal ART adherence. Similar to the findings of our scoping review, this study also found that education was a significant variable in the context of IPV and ART adherence, whereby higher educational attainment was positively correlated with optimal adherence (Biomndo et al., 2021). Finally, similar to the findings of this scoping review, trust in HCPs was also found to increase optimal adherence for HIV mothers, particularly if women did not have to conceal their HIV status to their HIV-positive partner (Biomndo et al., 2021).
This scoping review found that adherence to pediatric/public health recommendations for childhood immunization was negatively influenced by IPV in the perinatal period. Similar findings have been reported in other literature, whereby lower childhood immunization rates were associated with maternal exposure to IPV. A large population-based study in India found maternal exposure to physical and emotional violence was significantly associated with a decreased likelihood of children receiving full immunization status (Paul & Mondal, 2021). Similarly, another India-based study found a significant relationship between IPV and child immunization, where children of women experiencing IPV were less likely to be fully immunized than children of women who did not experience IPV (Hasan et al., 2015). Both of these studies also found that child immunization status improved as parental education levels increased (Hasan et al., 2015), thus aligning with the findings of this scoping review, suggesting that maternal education may be a protective factor in maternal health-related decision-making in the context of IPV.
The findings from this review add to the existing body of literature on IPV and maternal and child health and strengthen the understanding of how IPV impacts maternal health-related decision-making during the perinatal period. However, while there are various studies that pertain to the health-related outcomes of women and children exposed to IPV, there are a limited number of studies that specifically address how IPV impacts maternal decision-making regarding women and children’s health, particularly within the North American context. As such, further research is called for to better understand how IPV plays a role in maternal decision-making around woman and child health. For example, research aimed at better understanding the mechanisms by which IPV may affect health care utilization, or research to evaluate the effect of interventions aimed at supporting women in their health-related decision-making in the context of IPV, could be of great benefit to policy and practice in this context.
Limitations
This scoping review is the first to provide a clearer understanding of what is currently known regarding maternal health-related decision-making in the context of IPV. Although rigorous methods were applied to this review, it was not without limitations. While a newly emerging area of research, the inclusion of only seven studies in this review implies that caution should be taken when generalizing findings more broadly. For example, in many instances, each theme was supported by only three or fewer studies. Furthermore, since the studies in this review originated in varying geographical locations globally and largely from countries of varying economic levels, results may only be representative of their respective regions. This suggests that further research is called for across lower-income to higher-income countries. Finally, although quality assessments are not requisite for a robust scoping review (Levac et al., 2010), the lack of quality assessment may also limit the generalizability of the findings.
This review lends a better understanding of maternal decision-making toward health-related matters in the context of IPV. The actual and potential health-related outcomes for both mothers and infants related to maternal decision-making are particularly important to explore within the pervasive context of IPV (Chisholm et al., 2017). This review provides a foundation for further research to fully explore health-related decisions for pregnant and postpartum mothers who have experienced IPV. Further research is required to best support women to make well-informed health care decisions in the face of IPV.
Conclusion
The findings from this scoping review add to a small but growing body of knowledge describing how health-related decisions by childbearing women are impacted by the experience of IPV. Experiencing IPV may affect how pregnant and postpartum women make health-related decisions, for example, those centered around breastfeeding practices, utilization of health services, and the capacity to adhere to medical recommendations related to women's and children’s health. Given the importance of health-promoting practices antenatally, postpartum, and during early childhood, further research is required to more clearly understand the complex interplay of variables that serve to enable or constrain health-related decision-making in the context of childbearing and IPV. Further, an increased understanding of the factors involved in health-related maternal decision-making in the context of IPV may provide further impetus to implement additional, accessible, health and social service resources to ensure childbearing women are empowered and supported to make the best health choices for themselves and their children to optimize health and well-being.
Supplemental Material
sj-docx-1-tva-10.1177_15248380231198876 – Supplemental material for Health-Related Maternal Decision-Making Among Perinatal Women in the Context of Intimate Partner Violence: A Scoping Review
Supplemental material, sj-docx-1-tva-10.1177_15248380231198876 for Health-Related Maternal Decision-Making Among Perinatal Women in the Context of Intimate Partner Violence: A Scoping Review by Kimberley T. Jackson, Cheryl Marshall and Julia Yates in Trauma, Violence, & Abuse
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.