
Abstract
Extensive research has been conducted on the link between trauma, child maltreatment (CM), and chronic pain. Although the risk of suffering from chronic pain among CM survivors has been established, much less is known about the experience of pain during CM incidents or whether such peritraumatic pain sensations are associated with later chronic pain. This scoping review was conducted to synthesize the existing literature on pain during and a short time following CM (i.e., peritraumatic pain). Utilizing the preferred reporting items for systematic reviews and meta-analyses guidelines, the current review included 11 manuscripts, which met the following criteria: (a) refer to physical pain experienced during or a short time after CM, (b) were published in peer-reviewed journals, and (c) were written in English. The review demonstrated that most of the included studies were not intentionally focused on peritraumatic pain, the majority used qualitative research methods, and all were cross-sectional. Furthermore, although validated questionnaires are available, most of the studies did not utilize such measures. Those that intentionally reported pain demonstrated its high intensity and prevalence in CM incidents, indicating that pain is inherently embedded in the experience of maltreatment. The findings spotlight an underdeveloped research realm on a phenomenon that may hold significant empirical, clinical, and legal implications. Research endeavors should initiate interdisciplinary bodies of knowledge to establish well-validated research methodologies that properly quantify peritraumatic pain in trauma and CM.
Introduction
Extensive empirical efforts have been dedicated to uncovering the short- and long-term implications of child maltreatment (CM; Hailes et al., 2019; Irish et al., 2010). Among these, substantial findings point to chronic pain as significantly related to trauma, posttraumatic stress disorder (PTSD; Asmundson & Katz, 2009; Sharp & Harvey, 2001), and CM (Finestone et al., 2000; Mehta et al., 2017; Nicol et al., 2016; Peles et al., 2016; Sachs-Ericsson et al., 2007; Spiegel et al., 2016). In fact, more than two decades ago, Kendall-Tackett (2001) argued that CM research should focus on pain as one of the main frontiers. Accordingly, previous findings have reported a significant link between child abuse and fibromyalgia (Häuser et al., 2014), genito-pelvic pain (Santerre-Baillargeon et al., 2017), interstitial cystitis/painful bladder syndrome (Mayson & Teichman, 2009), headaches (Lee Peterlin et al., 2007), irritable bowel syndrome (Beesley et al., 2010), and other chronic pain conditions (Walsh et al., 2007). Although this link has been extensively demonstrated, a recent systematic literature review on the prospective relationship between CM and chronic pain concluded the low quality of such prospective research (Marin et al., 2021).
The experience of pain comprises multifaceted aspects, involving physical, mental, and interpersonal propensities and the interactions between them (Edwards et al., 2016). Causal explanations about the link between the experience of CM and later chronic pain spotlight PTSD as one of the main underlying mechanisms (Marin et al., 2021). These findings are in line with the plethora of research delineating the comorbidity of PTSD and chronic pain (Reed II et al., 2021; Siqveland et al., 2017). This comorbidity has been suggested to result from mutual maintenance factors (Sharp & Harvey, 2001), as well as shared vulnerabilities (Asmundson & Katz, 2009). These explanations highlight the reaction to trauma as imperative in uncovering the link between CM and pain.
Further explanations point to other potential mechanisms for the trauma–pain link. Findings have implied alterations in the perception of pain sensations, pointing to dysfunctional pain perception and modulation among individuals with PTSD, demonstrated in dysfunctional inhibitory capacity (Defrin et al., 2014), as well as a paradoxical pain profile, combining reduced pain sensitivity and a hyper-responsivity to pain stimuli (Defrin et al., 2015). Such findings outline changes to the functioning of the central pain system, presumably caused by trauma and PTSD (Yarnitsky, 2010).
Another explanatory pathway highlights inflammation as a potential precursor for the CM–chronic pain link, which may be linked to impediments to the appropriate immune system functions related to increased activation of the hypothalamic–pituitary–adrenal axis (HPA axis) (Mayson & Teichman, 2009; Nicolson et al., 2010). Another explanation points to central sensitization, a process whereby the central pain system becomes chronically hypersensitive and signals pain despite the absence of peripheral damage (Latremoliere & Woolf, 2009).
Regardless of these important insights on the CM–pain link, very few investigations have considered the potential link between the experience of pain during and a short time following a CM incident (i.e., peritraumatic pain) and later chronic pain. Specifically, considering that CM may often involve pernicious physical offenses inflicted upon a child, it is possible that these pain sensations also play a role in explaining posttraumatic chronic pain. However, to the best of our knowledge, the association between peritraumatic pain in CM and chronic pain has yet to be examined. Previous findings of research among torture survivors have revealed that distinctive torture methods were implicated in neuropathic pain syndromes, such as painful feet among falanga (beating of the soles of feet) survivors (Olsen et al., 2006; Thomsen et al., 2000), and headaches among suffocation survivors (Olsen et al., 2007).
The association between peritraumatic pain and chronic pain may also be explained through other mechanisms. One pathway stems from the lens of central sensitization, which has been proposed as a substrate of chronic pain as well as other chronic morbidities (Woolf, 2011). With CM, which is often characterized by repeated victimization, the experience of intensive repeated pain may activate central sensitization. Posttraumatic pain symptoms may also play a role, involving intrusive pain symptoms and pain flashbacks (Macdonald et al., 2018; Salomons et al., 2004). Such symptoms may activate trauma reminders (Schreiber & Galai-Gat, 1993; Van der Kolk, 1998), as well as stress-induced hyperalgesia (Johnson & Greenwood-Van Meerveld, 2014). Taken together, peritraumatic pain sensations may instigate multifaceted physical and mental propensities underlying posttraumatic chronic pain.
Taking this question one step further, very few investigations have targeted peritraumatic pain in CM in general. Simply put, “is CM painful?” is a question rarely explored in the literature. Recent qualitative studies have demonstrated that children undergoing physical and sexual abuse reported significant and highly intense experiences of pain during and right after the abuse (Tsur et al., 2020; Tsur et al., 2021). Yet, these two explorations also showed that pain expressions are counterbalanced by the children claiming that, for example, “the pain was so, so bad, but not so much” (Tsur et al., 2021). In particular, regarding sexual abuse, the children found it difficult to describe where the pain sensation was located in their bodies (Tsur et al., 2020). Perhaps most importantly, the children portrayed a complex set of dynamics between the perpetrator and the child in the presence of the child’s expression of pain characterized by the perpetrator’s minimization of the child’s pain, distorted justification (“it hurts because your body is developing,” “this is how love feels”), and sometimes acknowledging the child’s pain and apologizing for it (Tsur et al., 2020; Tsur et al., 2021).
The above findings pinpoint that the experience of pain may be profound, deeply embedded in the subjective experience of CM, and presumably involved in later experiences of pain (Kendall-Tackett, 2001; Tsur, 2022). In line with the complexity portrayed regarding peritraumatic pain in CM, other findings have implied that medical staff who evaluated the pain intensity of young children who were abused was lower compared to children injured in accidents. Presumably, these findings may be explained by the expression of peritraumatic pain by the abused children, as well as the under-recognition of such pain by medical staff (Drouineau et al., 2017), a phenomenon also documented in other kinds of pediatric pain (Vetter & Heiner, 1996).
Considering earlier findings indicating that CM is implicated in an increased risk for chronic pain and opioid use in adulthood (Austin et al., 2018), exploring the underlying mechanisms involved in such posttraumatic morbidities is of great importance. The current systematic literature review aims to set the stage for exploring this link through the lens of peritraumatic pain in CM. Specifically, in the current study, literature including empirical findings referring to any pain sensations experienced during and a short time following CM incidents will be systematically analyzed and reviewed.
Method
This review was prepared in accordance with the preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement (Moher et al., 2009). The studies included in the current analysis were identified by searching the following primary databases: PsycNet, PubMed, and ScienceDirect. The PRISMA guidelines were implemented to filter the studies, in accordance with the PRISMA stages. First, all databases were searched with the following keywords: (a) Hurt, (b) Ache, (c) Acute pain, (d) Peritraumatic pain, (e) Physical pain, (f) Pain experience, (g) Pain assessment, (h) Pain perception, (i) Peritraumatic, (j) Peritraumatic dissociation, (k) Pain report, (l) Pain during trauma, and (m) Pain. These keywords were combined with (using “plus” +) the following keywords: (a) Child abuse, (b) Childhood abuse, (c) Physical Neglect, (d) Emotional neglect, (e) Child physical abuse, (f) Child sexual abuse, (g) Child emotional abuse, (h) Child physical neglect, (i) Child emotional neglect, (j) CM, and (k) Childhood maltreatment. As illustrated in Figure 1, the manuscripts were filtered using the stages in the PRISMA guidelines.
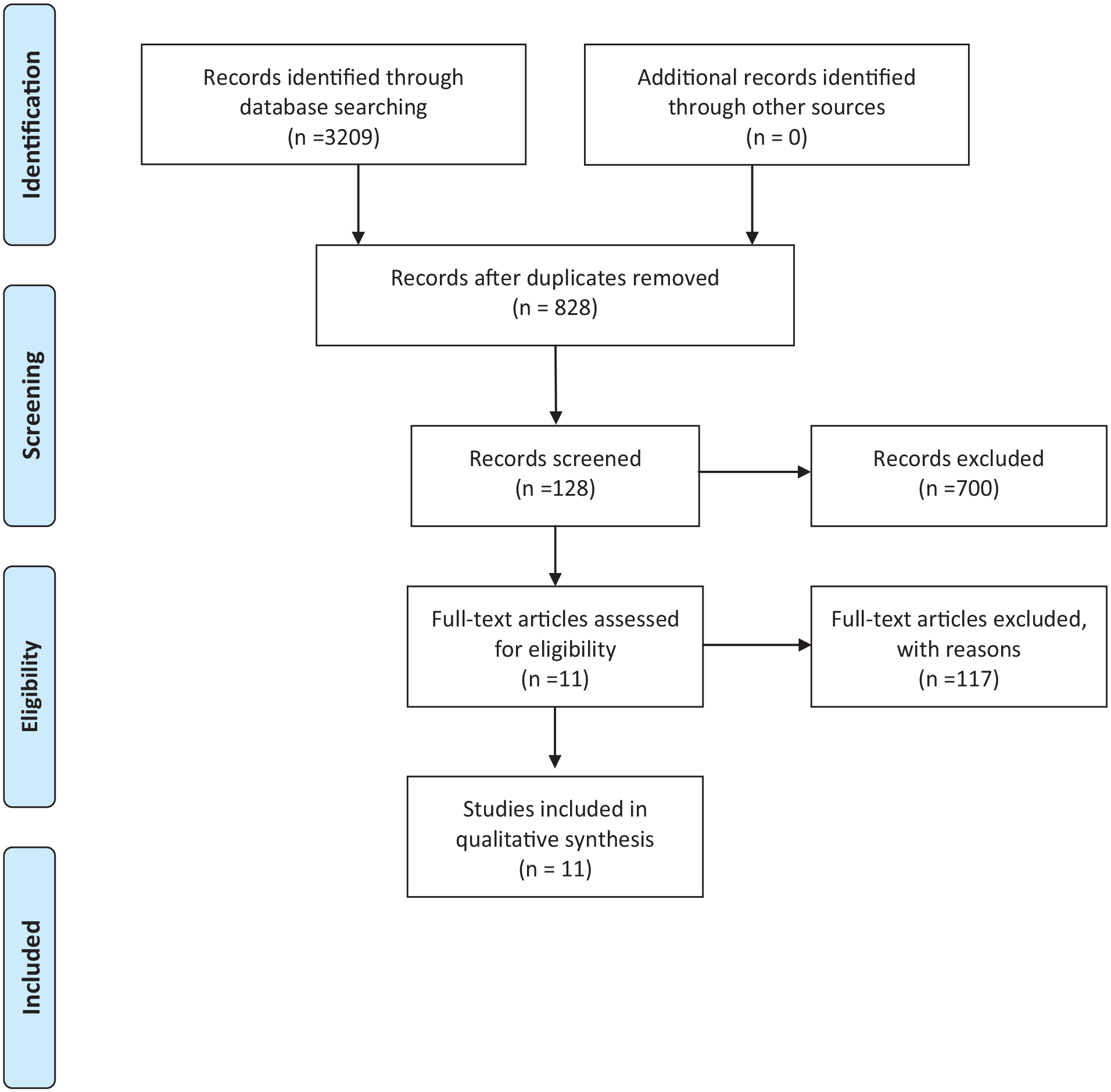
Preferred reporting items for systematic reviews and meta-analyses flow diagram.
To be included, articles needed to meet the following criteria: (a) refer to physical pain experienced during or a short time after child abuse, (b) were published in peer-reviewed journals, and (c) were written in English. Due to the limited number of studies published in this area, no limitation was implemented regarding the years during which the research was conducted. Via the keywords in the different databases, 828 manuscripts were identified; after screening by titles, 128 manuscripts were found potentially relevant for the review. Next, by screening abstracts, 47 manuscripts were found potentially relevant for the review. Finally, after reviewing full manuscripts, only 11 articles met the study's criteria (see Figure 1). Most excluded manuscripts were not included since they focused on pain occurring after (and not during) CM. In more detail, an extensive number of excluded manuscripts focused on different types of chronic pain syndromes in adulthood following CM, such as chronic pelvic pain (e.g., Özen et al., 2018; Poli-Neto et al., 2018) or fibromyalgia (e.g., Lee & Enright, 2014). A different pain outcome of CM was pain perception, again focusing on pain perception in adulthood but not during CM (e.g., Pieritz et al., 2015; Scarinci et al., 1994). Another central focus of the excluded manuscripts was emotional/psychological pain, rather than physical pain (e.g., Bakermans-Kranenburg & van IJzendoorn, 2013; Dorahy & Clearwater, 2012). Finally, an extensive number of excluded manuscripts focused on other posttraumatic symptomatology following CM, such as substance abuse (e.g., Adams et al., 2011), violent tendencies (e.g., Dong & Simon 2017), and self-injuries (e.g., Morris et al., 2015; Nock, 2009), all of which did not account for peritraumatic pain.
Results
Descriptive Information
A total of 11 manuscripts investigated peritraumatic pain in CM. A summary of the main findings is presented in Table 1. The majority of the manuscripts included samples from Israel (45.4%; Katz & Tener, 2021a, 2021b; Katz et al., 2020; Lev-Wiesel et al., 2014; Tsur et al., 2021, 2022), followed by the United States (36.3%; Carballo-Diéguez & Dolezal, 1995; Dolezal & Carballo-Diéguez, 2002; Simon et al., 2018; Taylor & Higginbotham, 2020), with one study from France (9.09%; Drouineau et al., 2017), and one from Iceland (9.09%; Sigurdardottir & Halldorsdottir, 2013). The sample sizes of the studies ranged from 35 to 13,050; the total number of participants across the studies was 14,060. Since 2013, this area has gained growing research interest, with nine (81.8%) of the manuscripts published between 2013 and 2021 (Drouineau et al., 2017; Katz & Tener, 2021a, 2021b; Katz et al., 2020; Lev-Wiesel et al., 2014; Sigurdardottir & Halldorsdottir, 2013; Simon et al., 2018; Taylor & Higginbotham, 2020; Tsur et al., 2021, 2022). The age range of the children in the samples was 0 to 17.
Summary of Main Findings.
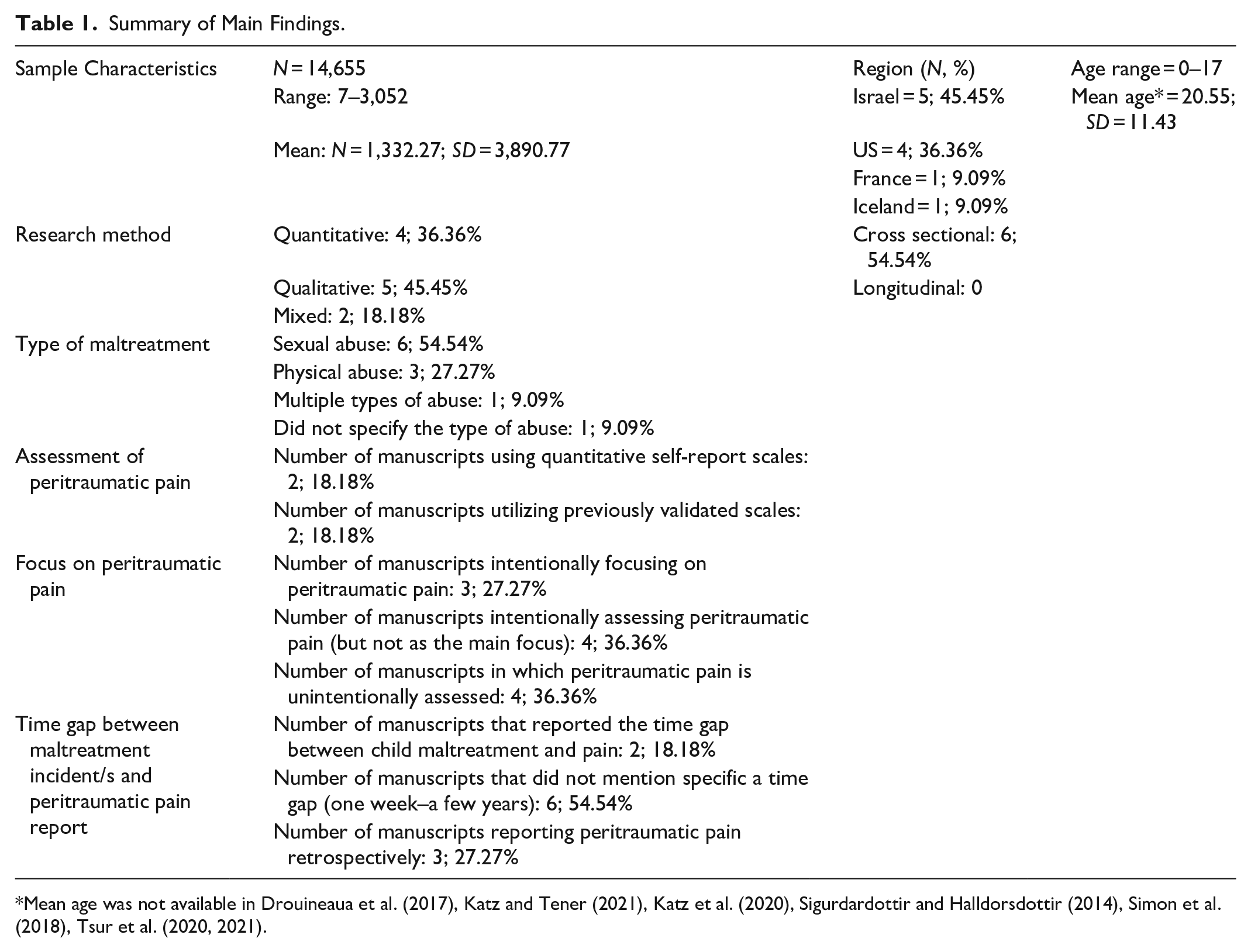
Mean age was not available in Drouineaua et al. (2017), Katz and Tener (2021), Katz et al. (2020), Sigurdardottir and Halldorsdottir (2014), Simon et al. (2018), Tsur et al. (2020, 2021).
Research Design
The review indicated that the majority of the manuscripts utilized a qualitative research design (n = 5; 45.45%), with four applying a thematic analysis (Katz & Tener, 2021a, 2021b; Katz et al., 2020; Tsur et al., 2021, 2022) and one using phenomenology methods (Sigurdardottir & Halldorsdottir, 2013). The remainder of the manuscripts used a quantitative cross-sectional research design (n = 4; 36.36%; Drouineau et al., 2017; Lev-Wiesel et al., 2014; Simon et al., 2018; Taylor & Higginbotham, 2020) or mixed methods of qualitative and quantitative research methods (n = 2; 18.18%; Carballo-Diéguez & Dolezal, 1995; Dolezal & Carballo-Diéguez, 2002). No longitudinal studies were included in the review. Considering the vast research demonstrating chronic pain following CM (e.g., Finestone et al., 2000; Mehta et al., 2017) and the possible link between peri- and posttraumatic pain, the lack of longitudinal investigations is alarming.
Sample Characteristics and Types of Maltreatment
Most of the samples (n = 8; 72.72%) included were children (Drouineau et al., 2017; Katz & Tener, 2021a, 2021b; Katz et al., 2020; Lev-Wiesel et al., 2014; Simon et al., 2018; Taylor & Higginbotham, 2020; Tsur et al., 2021, 2022). The remaining three studies included adults who were sexually abused as children. Of these samples, six (75%) were children who were maltreated by a parent or caregiver (Katz & Tener, 2021a, 2021b; Katz et al., 2020; Lev-Wiesel et al., 2014; Simon et al., 2018; Tsur et al., 2021, 2022) and two (25%) were of children evaluated due to allegations or concerns of abuse by parents, caregivers, family members, or family friends (Drouineau et al., 2017; Taylor & Higginbotham, 2020).
Three (37.5%) of the eight children’s samples studied sexual abuse (Katz et al., 2020; Taylor & Higginbotham, 2020; Tsur et al., 2022), three (37.5%) studied physical abuse (Katz & Tener, 2021a, 2021b; Simon et al., 2018; Tsur et al., 2021), one (12.5%) did not specify the type of the maltreatment (Drouineau et al., 2017), and one studied multiple types of abuse (physical, sexual, emotional, neglect, and witnessing domestic violence; Lev-Wiesel et al., 2014). The remaining three (27.27%) samples were of adults who retrospectively reported childhood sexual abuse (Carballo-Diéguez & Dolezal, 1995; Dolezal & Carballo-Diéguez, 2002; Sigurdardottir & Halldorsdottir, 2013).
Assessment Tools for Measuring Peritraumatic Pain
All but one study used self-report methods to assess children’s peritraumatic pain in CM. Among these, five were qualitative and, therefore, did not utilize quantitative assessments. Among the manuscripts using quantitative research (N = 6), the review revealed limited use of well-validated measures for assessing peritraumatic pain in CM. Drouineau et al. (2017) used the Children’s Hospital of Eastern Ontario Pain Scale (McGrath et al., 2003). Surprisingly, of the manuscripts using self-report methods, only one (Lev-Wiesel et al., 2014) used a validated scale to assess abused children’s peritraumatic pain using an item from the Disclosure of Trauma Questionnaire (DTQ): “Couldn’t suffer pain anymore” (Mueller et al., 2008). The other manuscript using a self-report measure (Simon et al., 2018) used a self-report single-item scale to assess pain: “Were you physically hurt when this happened? Hurt means you could still feel pain in your body the next day. You are also hurt when you have a bruise, a cut that bleeds, or a broken bone.”
In most of the manuscripts, the pain was reported directly by the participants in the study (n = 10, 90.9%). Only one study detailed peritraumatic assessments, as reported by medical staff (Drouineau et al., 2017).
Bottom-up Versus Top-down Focus on Peritraumatic Pain
Of the manuscripts included in the review, only three (27.27%) aimed to assess experiences of peritraumatic pain in CM (Drouineau et al., 2017). Two of these manuscripts examined pain from the perspectives of children conveyed in forensic interviews following parental physical or sexual abuse (Tsur et al., 2021, 2022). The third manuscript investigated whether abused children’s peritraumatic pain was under-recognized by the medical staff in hospitals (Drouineau et al., 2017). The remainder of the studies (n = 8, 72.72%) focused on other aspects of CM (e.g., disclosure of CM, the sibling subsystem, and adult sexual risk behaviors) but mentioned peritraumatic pain in various ways. Of these, only four assessed the pains of the participants, although this was not the main focus of the investigation (Dolezal & Carballo-Diéguez., 2002; Lev-Wiesel et al., 2014; Simon et al., 2018; Taylor & Higginbotham, 2020). For example, via a national survey, one study asked whether the child was physically hurt during the abuse. Being physically hurt was defined as still feeling pain in the body the next day, or having a bruise, cut, bleeding, or broken bones following the abuse (Simon et al., 2018). Another manuscript, which employed the DTQ (Mueller et al., 2008), assessed whether intolerable physical pain was a factor in deciding to disclose the abuse (Lev-Wiesel et al., 2014). The remaining manuscripts (n = 4, 36.36%), although not intentionally assessing pain, reported the participants’ descriptions of it. For example, one manuscript that analyzed children’s perception of their responses during sexual abuse showed that in the children’s experiences, fighting the perpetrator caused them more pain (Katz et al., 2020).
Retrospective Reports Versus Reports a Short Time Following CM
Of the samples consisting of children, the majority reported pain and other aspects of CM a short time after the maltreatment incidents (n = 8; 72.72%; Drouineau et al., 2017; Katz & Tener, 2021a, 2021b; Katz et al., 2020; Lev-Wiesel et al., 2014; Simon et al., 2018; Taylor & Higginbotham, 2020; Tsur et al., 2021, 2022). The time gap between the CM and the pain reports ranged from 1 week following an abusive incident to a few years. As the passage of time may cause memory biases when examining peritraumatic pain, the review explored the attention given in the manuscripts to the gaps between the CM and the reports of pain. The review indicated that this matter did not receive adequate attention in most of the manuscripts. Namely, the majority of studies did not mention or define a specific time gap between the report of peritraumatic pain and the incident of CM. Only two manuscripts mentioned the time that passed between the CM incident and the reported pain. One manuscript on medical staff’s recognition of pain in abused children included children who were admitted to the hospital up to 1 week after the injury (Drouineau et al., 2017). Another study of medical exams of children suspected to have been sexually abused displayed the timing of the exams included in the study. For most of the participants (N = 499; 87.1%), the exam took place more than 1 week after the last sexual abuse incident, and only 4 (0.7%) of the participants were examined within 7 days of the last reported abuse (Taylor & Higginbotham, 2020). However, the rest of the manuscripts in this review (n = 3, 27.27%) included retrospective reports of CM and peritraumatic pain, without referring to the time gap between the report and the experience of peritraumatic pain (Carballo-Diéguez & Dolezal, 1995; Dolezal & Carballo-Diéguez, 2002; Sigurdardottir & Halldorsdottir, 2013).
Peritraumatic Pain Characteristics in CM
Consistent with the finding that most of the manuscripts did not intentionally examine pain, the characteristics of peritraumatic pain have been narrowly assessed and presented. The absence of information regarding pain characteristics is reflected by the lack of attention to different qualities of pain. For example, only three (27.27%) studies explicitly referred to the intensity of the physical pain experienced by children during and shortly after being abused (Drouineau et al., 2017; Tsur et al., 2021, 2022). Two other manuscripts presented a limited approach to pain intensity, using the intensity suffered during the abuse as an indicator for other variables. Specifically, one study referred to pain intensity as a factor in disclosing the abuse (Lev-Wiesel et al., 2014). The other study used pain intensity to assess whether a child was injured or not, using one level of intensity (i.e., feeling pain the next day; Simon et al., 2018). Another aspect of peritraumatic pain characteristics that lacked attention was pain regions during and after CM. Three (27.27%) manuscripts mentioned pain areas; one showed that children experienced vulvar and anal pain after sexual abuse (Taylor & Higginbotham, 2020). Two other manuscripts presented children’s descriptions of sexual and physical abuse, including the areas they felt pain (Tsur et al., 2021, 2022). One of the manuscripts found that the children sometimes described pain in areas where they were not physically injured, such as the head, abdomen, and legs (Tsur et al., 2021).
The attention given by children to the areas where they felt pain, and the lack of attention given to this aspect in the manuscripts, emphasizes the gap between children’s experiences and empirical knowledge. One explanation for this gap is the complexity of the children’s expressions of pain, as shown in some of the included manuscripts. For example, Drouineau et al. (2017) found that the expression of pain by children has been under-recognized by doctors and nurses, which suggests that abused children may have a reduced ability to pain expression. Another indication of this complexity is manifested by the children’s struggle to localize their pain, instead of using words such as “inside” and “deep” (Tsur et al., 2022). In addition, children were often silenced while trying to communicate their pain to their abusers, presumably receiving a “message” that their experiences were not important or legitimate (Tsur et al., 2021, 2022). Moreover, when communicating their pain in forensic interviews, their expressions were mostly not attended to by the interviewers (Tsur et al., 2021).
The Link Between Peritraumatic Pain and Posttraumatic Manifestations
The link between peritraumatic pain and posttraumatic pain or other posttraumatic manifestations did not receive much attention in the manuscripts included in this review. The only manuscripts to include posttraumatic manifestations were those that were retrospective, consisting of adult samples (Carballo-Diéguez & Dolezal, 1995; Dolezal & Carballo-Diéguez, 2002; Sigurdardottir & Halldorsdottir, 2013). Carballo-Diéguez and Dolezal (1995) found that Puerto Rican men who were physically hurt or unwilling to participate during experiences of child sexual abuse were more likely to have unsafe sexual behavior in adulthood. In a later study, Dolezal and Carballo-Diéguez (2002) found that men who considered themselves victims of childhood sexual abuse were more likely to have been physically hurt during sexual experiences in childhood. Sigurdardottir and Halldorsdottir (2013) found that all women in the study described different aspects of posttraumatic manifestations of pain throughout their lives. As children, they suffered unexplained physical symptoms and, in adulthood, all the women dealt with fibromyalgia or chronic and widespread pain, of which some women specifically related to the experiences of peritraumatic pain. As seen, the findings regarding posttraumatic manifestations of pain in the review’s included manuscripts are scarce, and the examination of the link between CM and peritraumatic pain has only been shown to be coincidental. Considering CM is an interpersonal traumatic event, the lack of attention to its posttraumatic physical and phycological manifestations and the absence of a systematic assessment of the potential link between peri- and posttraumatic pain are alarming.
Discussion
The current literature review spotlights an inherent biopsychosocial ingredient of the experience of CM, peritraumatic pain. The findings demonstrated that, although children may experience significant and intense pain during CM, our understanding of this experience is substantially limited. Considering the proliferation of research on posttraumatic chronic pain, such a limited understanding of peritraumatic pain is quite surprising.
The findings revealed that, except for three manuscripts included in the review, all other manuscripts were not conducted with a clear intent to study CM pain experiences. Rather, the pain was brought up by participants when asked to talk about their experiences with CM. In fact, although participants explicitly referred to their pain sensations, it was scarcely attended to in the analyses nor presented or discussed in other parts of the manuscript. When the authors did refer to peritraumatic pain, it most often was used to imply injury or other tissue damage. Seemingly, although not intentionally, these findings echo the disregard for children’s subjective experiences, a salient manifestation of abusive relationships.
Furthermore, peritraumatic pain during CM may hold significant information about the perpetrator–victim dynamic. Acute pain serves the survival of organisms by signifying potential danger and tissue damage. Stemming from this evolutionary perspective, the experience of peritraumatic pain in CM may signify to the child that “something wrong” is taking place. Considering that one of the core ingredients of CM is the denial and suppression of the child’s needs (Herman, 1997), it is proposed that the way the child experiences and expresses peritraumatic pain, and the way the perpetrator responds to these pain expressions may reflect a microcosmos of the victimizing dynamic in general.
Recent findings reveal that about 23% of adult child abuse survivors report experiencing pain flashbacks, which correspond with the pain areas in which they have reported pain during the abuse (Tsur, 2023). These findings are in line with the understanding that sensory input from the victimizing incident may be experienced repeatedly through intrusive posttraumatic symptoms, that is, flashbacks (American Psychiatric Association, 2013; Cloitre et al., 2018), sometimes including pain sensations (Macdonald et al., 2018; Tsur, 2023; Whalley et al., 2007). A question then arises as to whether these intrusive pain sensations may be related to posttraumatic chronic pain. Initial findings show that the report of pain flashbacks was associated with a higher risk of chronic pain in adulthood (Tsur, 2023), thus providing initial direction for further needed exploration.
Diversity as Applied to the Reviewed Manuscripts
Although pain is a universal experience, its perception is affected by various biological, psychological, and social factors (Gatchel et al., 2014). However, this review demonstrates that diversity is rarely addressed. First, all reviewed manuscripts reported research conducted in Western cultures. However, the literature demonstrates that cultural differences are seen in the ways in which individuals perceive, cope, and express pain (Miller & Abu-Alhaija, 2019). Furthermore, cultural differences apply to the basic perception of the mind–body link, with Western cultures embracing a Cartesian dualism, that is, viewing mind and body as essentially separated entities (Mehta, 2011). As such, the findings arising from this review cannot be generalized to other cultures. Future research should explore non-Western cultures, as well as explicitly target cultural dis/similarities in the experience and report of peritraumatic pain in CM.
Second, although the studies included both female and male participants, gender differences in experiences of peritraumatic pain in CM are barely noted. Findings stemming from pain perception research have identified some gender differences in the perception of acute pain (Sorge & Strath, 2018), which implies the need to include gender differences in the study of peritraumatic pain as well. Taylor and Higginbotham (2020) reported that female children were more likely to have significant findings in medical evaluations due to child sexual abuse allegations compared to males and that reports of pain significantly increased the likelihood of having significant exam findings for female, but not male children. However, Dolezal and Carballo-Diéguez (2002) showed that 34% of males who had sexual experiences as children with older men reported being physically hurt during the incident/s. These findings imply that gender differences warrant further investigation.
Taken together, future research should directly assess contextual factors potentially affecting the ways in which children experience and report peritraumatic pain, and the ways by which such pain is involved within the perpetrator–victim dynamic. Finally, as contextual diversity can be seen with respect to peritraumatic pain, its implications for posttraumatic manifestations throughout the lifespan should also be explored.
Implications for Research
A summary of the study implications is presented in Table 2. Although pain has been pinpointed as a necessary focus in CM research (Kendall-Tackett, 2001), and the study of posttraumatic chronic pain in trauma in general, the current review underlines the need to further explore the experience of pain during CM acts. One significant barrier to such research efforts is the methodological obstacles embedded in retrospective investigations. While findings provide sufficient evidence for the validity of adult retrospective reports of CM (Hardt & Rutter, 2004), it has been argued that more emphasis should be given to child and adolescent reports, as these entail less memory bias (Jud et al., 2016). For example, a multicentre study assessing pain perception at the time of presentation of CM along with a longer-term follow-up documenting the incidence of chronic pain in relation to a comparison group could provide much-needed information regarding the link between peritraumatic and posttraumatic pain in CM, as well as provide indications for the underlying mechanisms of this association.
Study Implications.
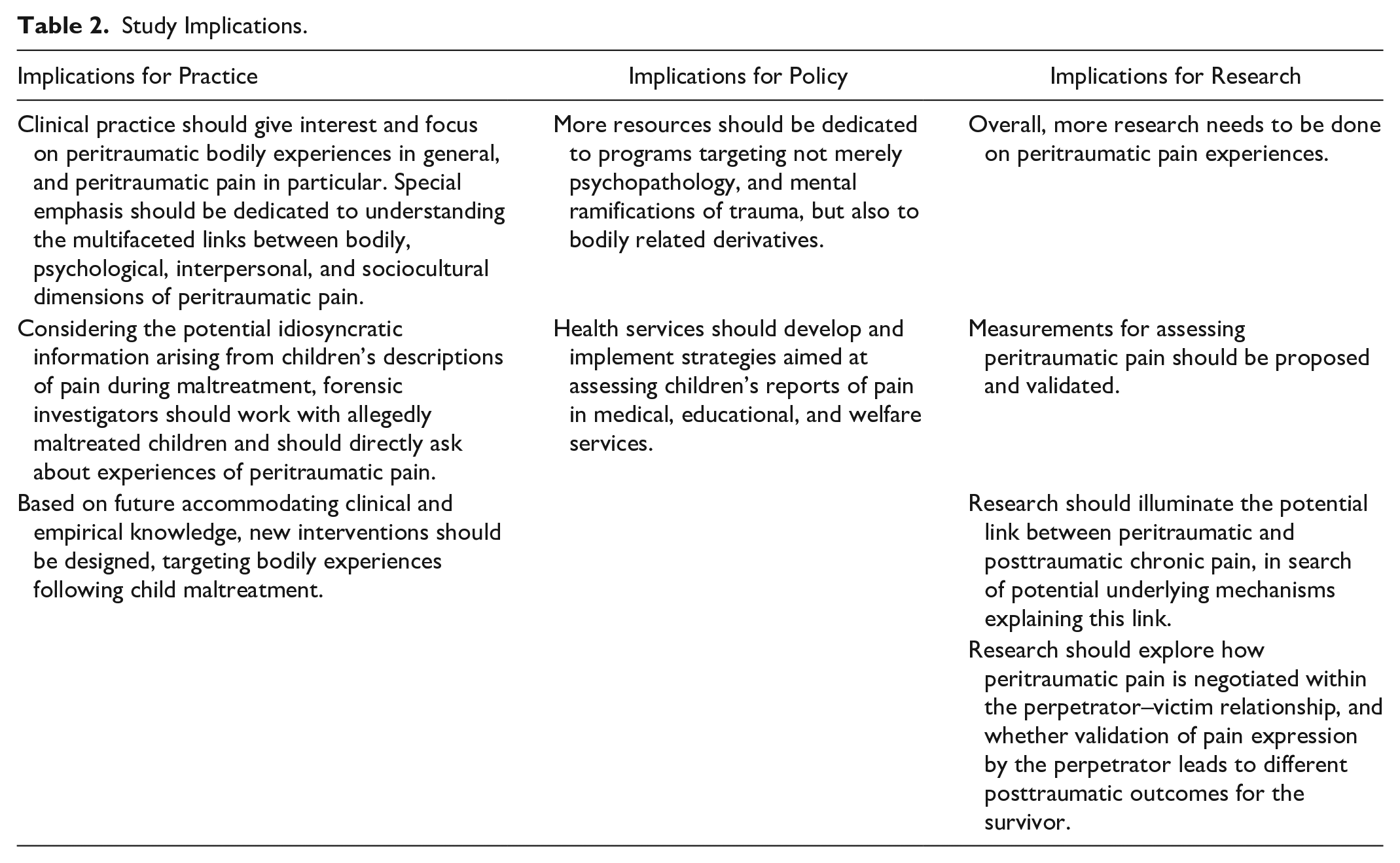
In addition, the findings further revealed that peritraumatic pain assessment tools and methods are underdeveloped, leading to a lack of well-validated quantitative measures. Therefore, research efforts should be dedicated to developing measures that will enable quantitative assessment of peritraumatic pain. Quantitative assessments of chronic pain are well established, including instruments such as the McGill pain questionnaires (Melzack, 1975), and others. However, to the best of our knowledge, except for the Visual Analog Scale, used in one study included in this review (Drouineau et al., 2017), no other manuscripts reported a systematic quantitative assessment of peritraumatic pain. Future studies should explore the possibility that the McGill pain questionnaire could be used for such research purposes, should its validity for CM peritraumatic pain be tested and reported.
Another implication for research arising from the current review points to the need to conduct multidisciplinary research on peritraumatic pain. Presumably, it is not surprising that peritraumatic pain has been insufficiently examined, as the majority of the manuscripts concerning CM originate from the social sciences, therefore, primarily addressing emotional, cognitive, interpersonal, and social aspects of CM. Although the study of chronic pain has been extensively researched and linked with psychosocial factors (e.g., Asmundson & Katz, 2009; Lerman et al., 2015; Marin et al., 2021), much less is known about acute pain within the psychosocial research realm. Conversely, acute pain has been extensively studied in the medical sciences, demonstrating a proliferation of methodologies and knowledge regarding the assessment of acute pain. As such, it is recommended that research efforts on CM strive to integrate these distinct bodies of knowledge through fruitful multidisciplinary collaborations.
Implications for Policy and Practice
Understandings regarding peritraumatic pain during CM pose potential new avenues for clinical efforts. First, medical assessments with CM victims should include a better assessment of peritraumatic pain. Although CM pediatricians often prefer to avoid trauma reminders during the medical examination, targeting the child’s experience of pain may also be perceived by the child as a validating experience of what they have been through, thus promoting trust in the medical staff and procedure. A recent literature review provides recommendations for a few single-item self-report pain intensity scales in children and adolescents, such as the 11-point numeric rating scale (NRS-11; Farrar et al., 2001), Faces Pain Scale–Revised (FPS-R; Hicks et al., 2001), and the Color Analogue Scale (McGrath et al., 1996). These short and simple assessments tools are easy to adhere to and may provide valuable medical and legal information. However, as the above review shows, more research is needed to validate assessments of pain in children younger than 6 years. In addition, the use of pain assessment in CM victims should be assessed for its validity, as well as the potential stress-triggering effect.
The past few decades have brought advances in the development of mind–body integrative perspectives to clinical practice. Such perspectives are implemented with trauma survivors in somatic experiencing (Levine, 1997), eye movement desensitization and reprocessing (Shapiro, 2017), mindfulness-based stress reduction (Kabat-Zinn & Hanh, 2009), and others. The current findings convey that more emphasis should be dedicated to understanding the experience of the body in general, and pain in particular, in trauma-focused therapies. Such clinical endeavors should target specific peritraumatic bodily experiences and the ways they may affect the experience of the body later on, as well as how they may be repeatedly experienced in intrusive symptoms/flashbacks. Moreover, the subjective experience of peritraumatic pain should be targeted in all therapeutic methods and not limited to those considered mind–body techniques. It is recommended that these understandings be further developed into clinical interventions with survivors of CM.
Developing our understanding of peritraumatic bodily experiences may also facilitate forensic processes in alleged child abuse cases. As seen in the two studies assessing reports concerning pain in forensic interviews with children of alleged abuse (Tsur et al., 2020, 2021), communicating about pain may provide a rich and idiosyncratic testimony that could augment the child’s testimony and, through this, facilitate the prosecution process.
Relatedly, one study showed that almost half of the participants disclosed the abuse they endured because they “couldn’t suffer pain anymore” (Lev-Wiesel et al., 2014). This finding introduces the need to target pain in the design of CM prevention and child protection services. Although simple pain assessments are available in pediatric medical settings (Baxt et al., 2004; Blount & Loiselle, 2009; Merkel & Malviya, 2000), to the best of our knowledge, such assessments are not used in child protection services.
Conclusion
Is CM painful? Basic common knowledge would suggest that it may indeed be painful. Surprisingly, despite a decent number of studies on chronic pain following CM, research on peritraumatic CM is scarce. The current systematic literature review provides a scope of the existing knowledge on this topic. In summary, although the findings showed that CM survivors report the experience of intensive peritraumatic pain, in research, this phenomenon is mostly tested unintentionally. Therefore, an intentional focus and proper research methodologies to assess it systematically are lacking. With chronic pain widely acknowledged in the trauma research field, perhaps it is time to set the stage for the study of peritraumatic pain.
Research Data
sj-xlsx-1-tva-10.1177_15248380231194069 – Supplemental material for Peritraumatic Pain in Child Maltreatment: A Systematic Literature Review
sj-xlsx-1-tva-10.1177_15248380231194069 for Peritraumatic Pain in Child Maltreatment: A Systematic Literature Review by Noga Tsur, Ada Talmon and Nofar Shemesh in Trauma, Violence, & Abuse
Footnotes
Acknowledgements
The authors would like to sincerely thank Ms. Laura Crompton for the language editing of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.