
Abstract
The current research examines potentially morally injurious events (PMIEs) faced by healthcare professionals working in forensic and psychiatric environments. A systematic literature review was conducted to identify peer-reviewed articles reporting on sources of moral injury or similar concepts (e.g., moral distress) for healthcare workers in such settings. Thirty articles were included and analyzed using a meta-ethnographic approach. Synthesis yielded three third-order factors, each reflecting a moral dichotomy: (a) “between profession and system,” (b) “between relations with patients and relations with others,” and (c) “between principles and practices.” Findings illustrated the hierarchical relationships between dichotomies, with discordance between values of the healthcare profession and features of the healthcare system providing the conditions for PMIEs to occur. The review advances conceptual understandings of PMIEs in forensic and psychiatric settings, illustrating the multilayered dimensions within which morally injurious events are experienced. Theoretical and practical implications are offered that may support the early detection and prevention of moral injury in healthcare professionals.
Healthcare professionals in secure psychiatric settings arguably operate within a uniquely challenging environment that necessitates fine balance between care and security. Staff face direct exposure to distressing incidents, such as acts of patient aggression (e.g., Dickens et al., 2013), and are frequently exposed to the traumatic histories of their patients (Newman et al., 2019). Such traumatic experiences are associated with poorer psychological and physical wellbeing among staff (Kelly et al., 2016), burnout (Converso et al., 2021), secondary trauma (Mangoulia et al., 2015), and higher staff turnover (Beidas et al., 2016), which has been found to translate into a poorer quality of care for patients (Brandt et al., 2016).
Given the chronically stressful environment that such healthcare professionals operate within, burnout and secondary traumatic stress have been extensively explored in this population. Such concepts describe outcomes of distress arising from difficulty coping with chronic work pressures and traumatic material, respectively. Thus, the source of distress is internalized as one that resides in the individual and forms part of their personal ability to manage stressors (Dean et al., 2019). Equally, the duties and responsibilities of healthcare professionals in secure psychiatric settings are conducted in the context of highly restrictive environments and limited resources (Oates et al., 2021), as well as legal and ethical tensions (Bipeta, 2019).
In recognition of the external context in which healthcare workers operate, moral injury has been applied as a framework that has some value in accounting for the experiences of this population. In the absence of any standardized definition, moral injury is commonly conceptualized as a form of psychological distress, primarily characterized by feelings of guilt and shame, which can arise as a result of perpetrating, witnessing, learning about, or failing to prevent an act that defies an individual’s own moral values (Litz et al., 2009). Despite its origins in warfare (Shay, 2002), a growing body of evidence has illustrated the prevalence of this “syndrome” in a range of other occupational populations, including healthcare professionals (e.g., Stovall et al., 2020). As moral injury is not a formal diagnosis, establishing its prevalence has proven somewhat of a challenge. Nevertheless, moral injury symptoms that bear at least a moderate impact on social and occupational functioning have been reported in as many as 45.7% of healthcare professionals (Mantri et al., 2021). Thus, moral injury appears a highly relevant construct for describing presentations of distress among staff.
Moral injury is impactful and linked with a plethora of adverse psychological health outcomes. Specifically, positive associations between moral injury and anxiety, depression, post-traumatic stress disorder, and suicidality have been documented, albeit mostly in veteran samples (Hall et al., 2021). Of further concern are the behavioral outcomes associated with exposure to a potentially morally injurious event (PMIE), which include disturbances in sleep and reduced treatment-seeking (Hall et al., 2021). Such outcomes, taken together with the withdrawal, reduced compassion, and disillusionment that can result from experiencing a PMIE, arguably has the potential to bear impacts that extend beyond the individual staff member, to also affecting those within their care. Thus, addressing moral injury becomes positioned as a priority for healthcare organizations, for the benefit of the service, staff, and patients.
While interventions to treat symptoms of moral injury following exposure to a PMIE have begun to be developed (e.g., Murray & Ehlers, 2021), preventative strategies that inhibit the initial morally injurious event may prove of particular importance. Accordingly, insight into the PMIEs faced by healthcare staff in secure psychiatric settings is arguably a good foundation from which to consider the existence of moral injury in this occupational group, before making recommendations for intervention. Yet, while the relevance of moral injury to healthcare professionals appears clear, the specific sources of such injury remain less so.
Investigation of moral injury in healthcare, and particularly within a psychiatric context, has been predated by a wealth of literature on the morally distressing experiences of staff in this occupational field. Yet, despite the interchangeable use of these terms, moral distress and moral injury are positioned as separate concepts, with the former representing as a less severe presentation of the latter (Litz & Kerig, 2019). In the context of a lack of empirically-derived distinction between the two, it has been postulated that moral distress and moral injury may reflect individual points on a continuum (Litz & Kerig, 2019), with cumulative moral distress bearing the potential to accrue and present in the form of moral injury. Therefore, sources of moral distress may also be sources of moral injury, when occurring in tandem or pervasively. Nevertheless, studies have primarily focused on specific practices, namely restrictive practices (e.g., Moran et al., 2009). As such, current insights into the range of PMIEs that may precede the development of moral injury for healthcare workers in such an environment are limited.
A more comprehensive understanding of the multifarious PMIEs faced by this population is potentially critical to informing changes in policy and practice and offering recommendations for policy-makers and healthcare professionals at all levels. Thus, in consideration of the narrow scope of existing research and the potential utility in widening insight into the root sources of moral injury, the current review sought to explore the range of PMIEs that secure psychiatric healthcare workers are exposed to. A systematic review and meta-ethnography was conducted to identify and synthesize potential sources of moral injury relevant to forensic and psychiatric healthcare, with the aim of advancing a conceptual understanding of PMIEs in secure psychiatric settings and informing practical recommendations to reducing their occurrence and impact.
Method
Search Strategy
A systematic literature review was conducted to retrieve articles that identified potential sources of moral injury for staff in forensic and/or psychiatric settings, in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA; Page et al., 2021) guidance. Articles were searched from PsycInfo, PsycArticles, Medline and CINAHL databases, and Google Scholar, between April and June 2021. In consideration of the limited evidence base, articles reporting on similar concepts (e.g., moral distress) were also sought. The specific search terms used are provided in Supplemental File 1. The reference lists of studies considered eligible after the full-text screening stage were also examined for additional relevant articles.
Inclusion and Exclusion Criteria
Articles were included in the review if they (a) identified potential sources of moral injury for healthcare workers in a forensic (e.g., prison) and/or psychiatric service, (b) were peer-reviewed, empirical research, (c) were available in English, and (d) were accessible in full-text. Articles were excluded if they did not meet all of these criteria. No parameters were set regarding year of publication nor country of origin.
Study Selection and Data Extraction
Screening and data extraction were completed by the primary author. The titles and abstracts of articles were initially screened, and those which met inclusion criteria were reviewed in full. Of articles which met inclusion criteria after full-text screening, data pertaining to the study aims, design and methodology, sample characteristics, measures of moral injury (quantitative studies only), and relevant findings were extracted by the primary author.
The current study utilized a meta-ethnographic approach for the synthesis. Primary participant quotations (first-order constructs) and author interpretations (second-order constructs) were extracted from qualitative papers. While meta-ethnography was originally developed for the synthesis of qualitative studies, it has since been utilized to synthesize quantitative research in several studies (e.g., Feast et al., 2018). In line with these studies, a coherent threshold was implemented to ensure that data extraction for quantitative papers was systematic. Specifically, items on measures of morally distressing events for which the average sample score indicated a tendency toward moral distress were extracted.
Quality Assessment
Study quality was assessed using the National Institute for Health and Clinical Excellence ([NICE], 2012) Quality Appraisal Checklist – Qualitative Studies (3rd edition) tool for qualitative articles and the AXIS appraisal tool (Downes et al., 2016) for quantitative articles. Articles were independently appraised by two raters, with discrepancies resolved through discussion.
Data Synthesis
As noted, meta-ethnography (Noblit & Hare, 1988) was employed to synthesize the findings of included articles. This covered the phases of (a) Getting started; (b) Deciding what is relevant to the initial interest (e.g., search strategy adopted, as noted earlier); (c) Reading the studies and in this instance extracting “concepts” relevant to the focus of the review; (d) Determining how the studies are related. This mirrored the approach described elsewhere (e.g., Atkins et al., 2008), whereby a thematic analysis of themes was conducted, grouping concepts into overarching categories. This produced several categories, of which a sample were co-rated (10%) leading to moderate agreement (Kappa = .53, p < .001). A concept grid was then created for each category, which highlighted similarities in meaning across studies; thus, a reciprocal approach was employed in the next phase; (e) Translating the studies, where concepts from studies are juxtaposed. In line with Franzel et al. (2013), concepts within categories were translated into one another to develop “secondary key concepts” that reflected PMIEs evident across studies. A primary data synthesis (Sattar et al., 2021) was developed for each category, as a commentary of the similarities and differences in data between studies, with articles translated chronologically; (f) Synthesizing translations, involved moving to a higher order interpretation of the data that goes beyond what is implied in the articles, individually. In the current review, “third-order constructs” emerged through interpretation of the previously captured concepts; and (g) Expressing the synthesis, where the findings were expressed in both written word and figures.
Results
Critical findings of the systematic review and meta-ethnography are summarized in Table 1.
Summary of Critical Findings.

Systematic Literature Search
The initial search produced 10,638 articles. After removing duplicates, 10,063 articles remained. Figure 1 indicates the process by which a final sample of 30 studies was achieved.
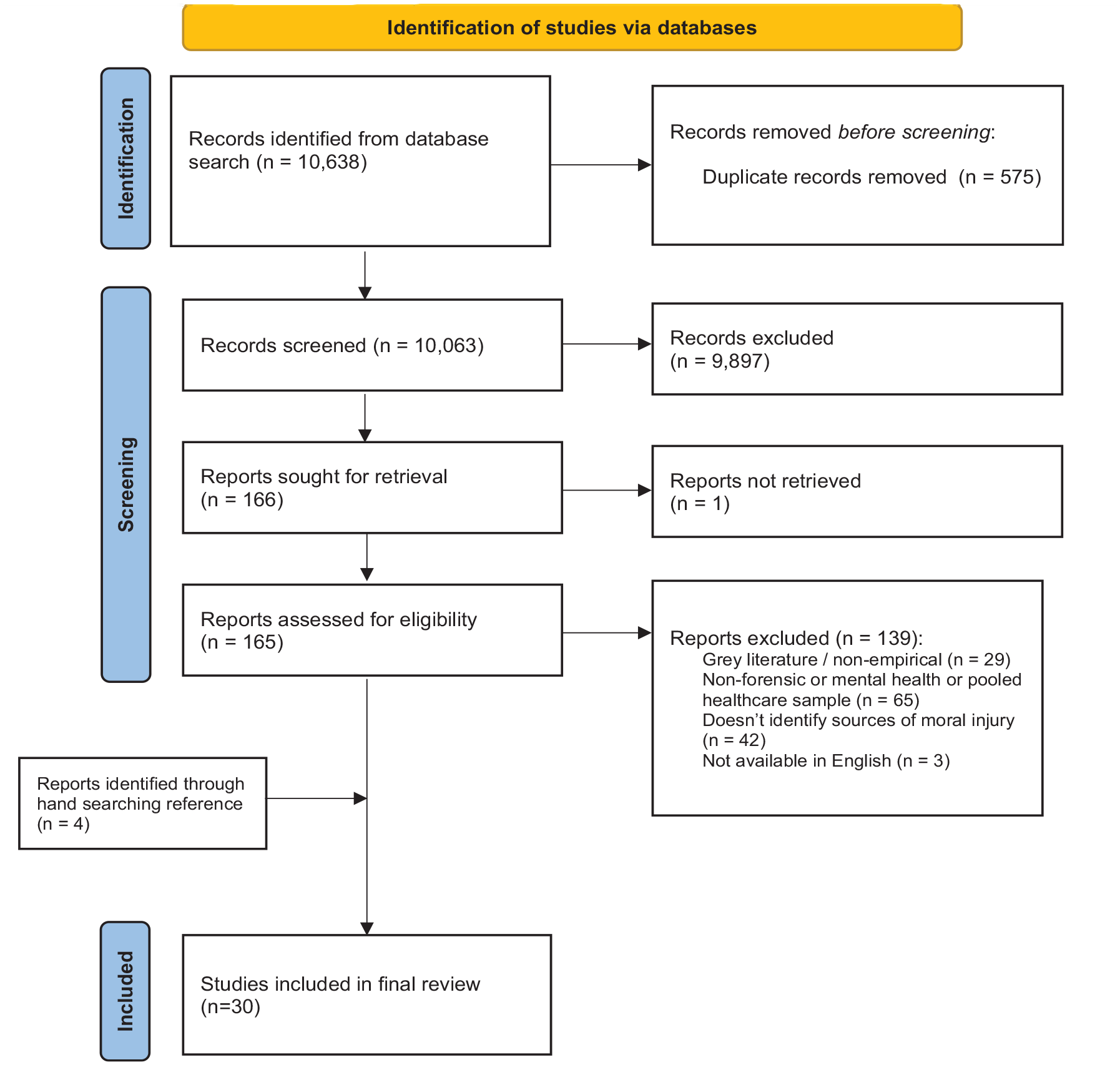
Preferred reporting items for systematic reviews and meta-analyses flow diagram.
Characteristics of included studies
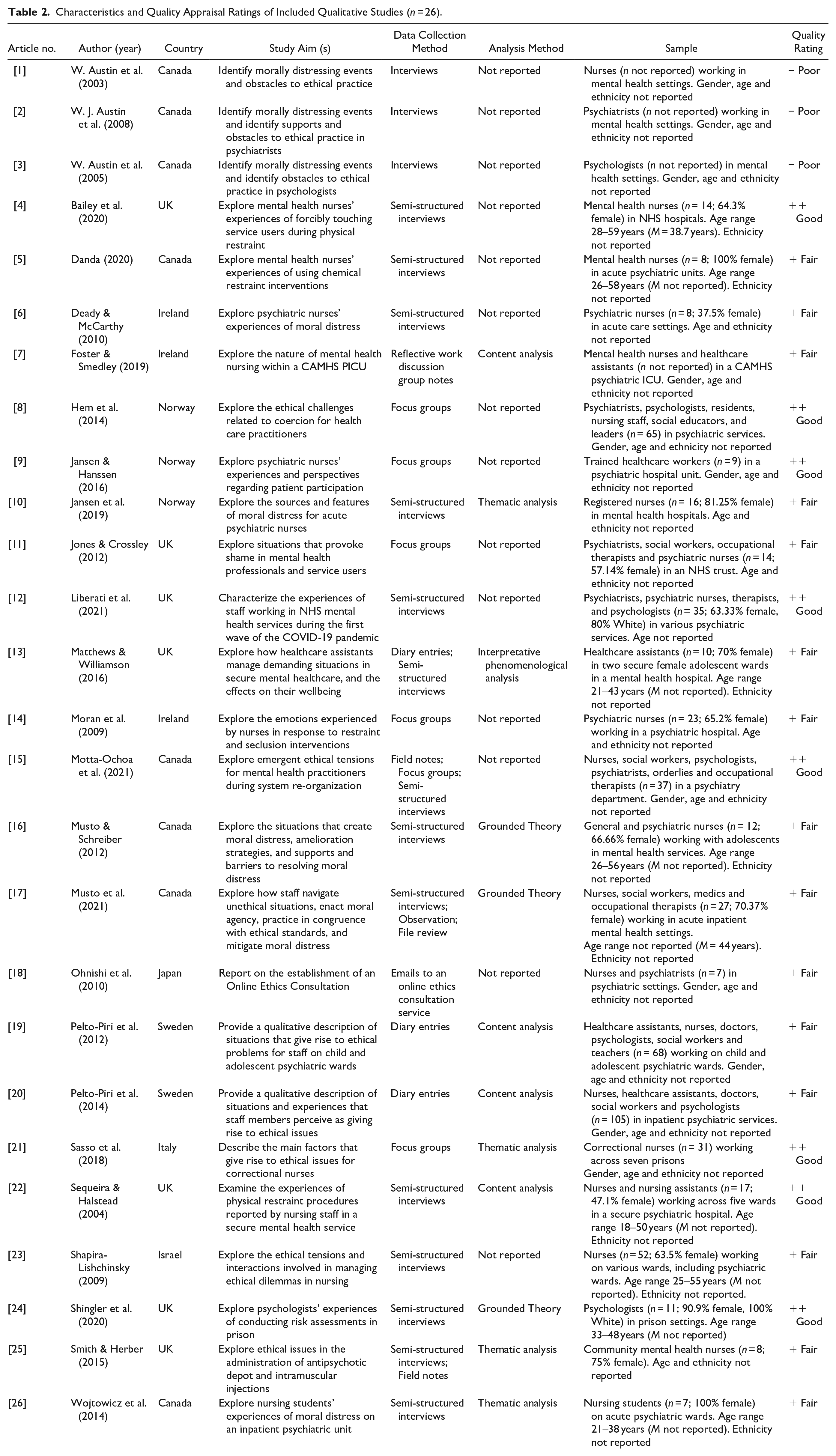
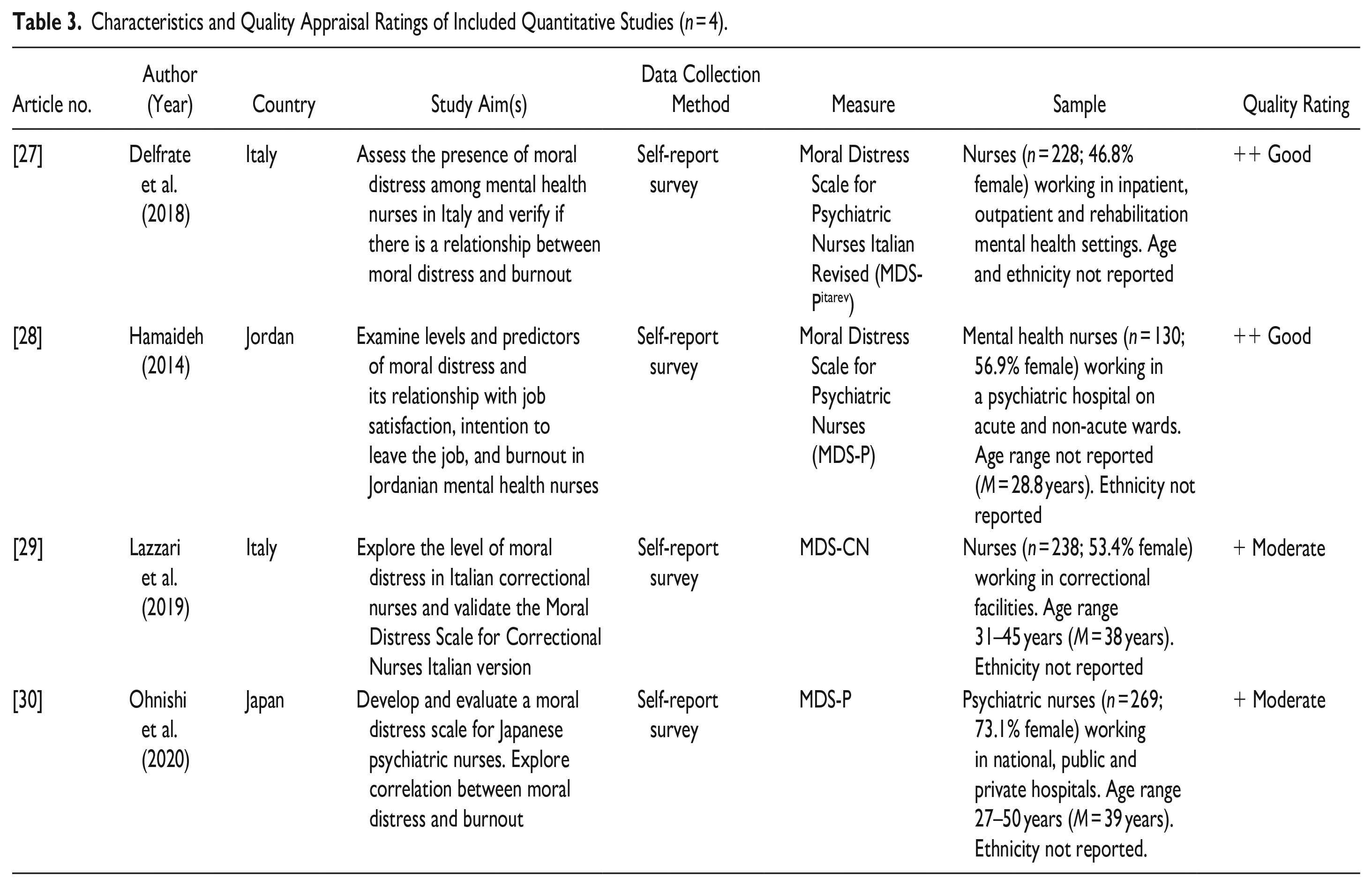
Studies were conducted between 1994 and 2021. Just one study specifically explored moral injury, with the majority focusing on moral distress (k = 20) or ethical challenges (k = 9). Most were conducted in westernized countries (k = 26) and utilized a nursing sample (k = 16). Three articles utilized staff working exclusively within correctional forensic settings, with remaining articles (k = 27) utilizing samples of staff from various psychiatric services. Of articles reporting on gender (k = 19), fourteen utilized a predominantly female sample, while two used a female-only sample, and three used a predominantly male sample. Of the two articles reporting on ethnicity, one utilized an exclusively White sample and the other utilized a predominantly White sample (80%). Quantitative articles were rated as of moderate (k = 2) or good (k = 2) quality, while qualitative papers were of either poor (k = 3), fair (k = 15), or good (k = 8) quality. Agreement between raters was moderate for quantitative papers (weighted Kappa = .50, p < .05) and almost perfect for qualitative papers (weighted Kappa = .88, p < .001). Table 2 presents the qualitative studies and Table 3 the quantitative, capturing characteristics, and quality appraisal.
Characteristics and Quality Appraisal Ratings of Included Qualitative Studies (n = 26).
Characteristics and Quality Appraisal Ratings of Included Quantitative Studies (n = 4).
Synthesis
Translation of the concepts developed at phase three led to the identification of 19 secondary key concepts, encompassed under three third-order constructs: (a) between profession and system, which describes the moral challenges of working in a system and environment that is at odds with their professional moral code, (b) between relations with patients and relations with others, which describes the moral challenges of having to manage multiple relationships within their role, and (c) between principles and practices, which describes practices being carried out by themselves and colleagues that are discordant with their professional moral code. These constructs and their associated concepts are presented in Figure 2.
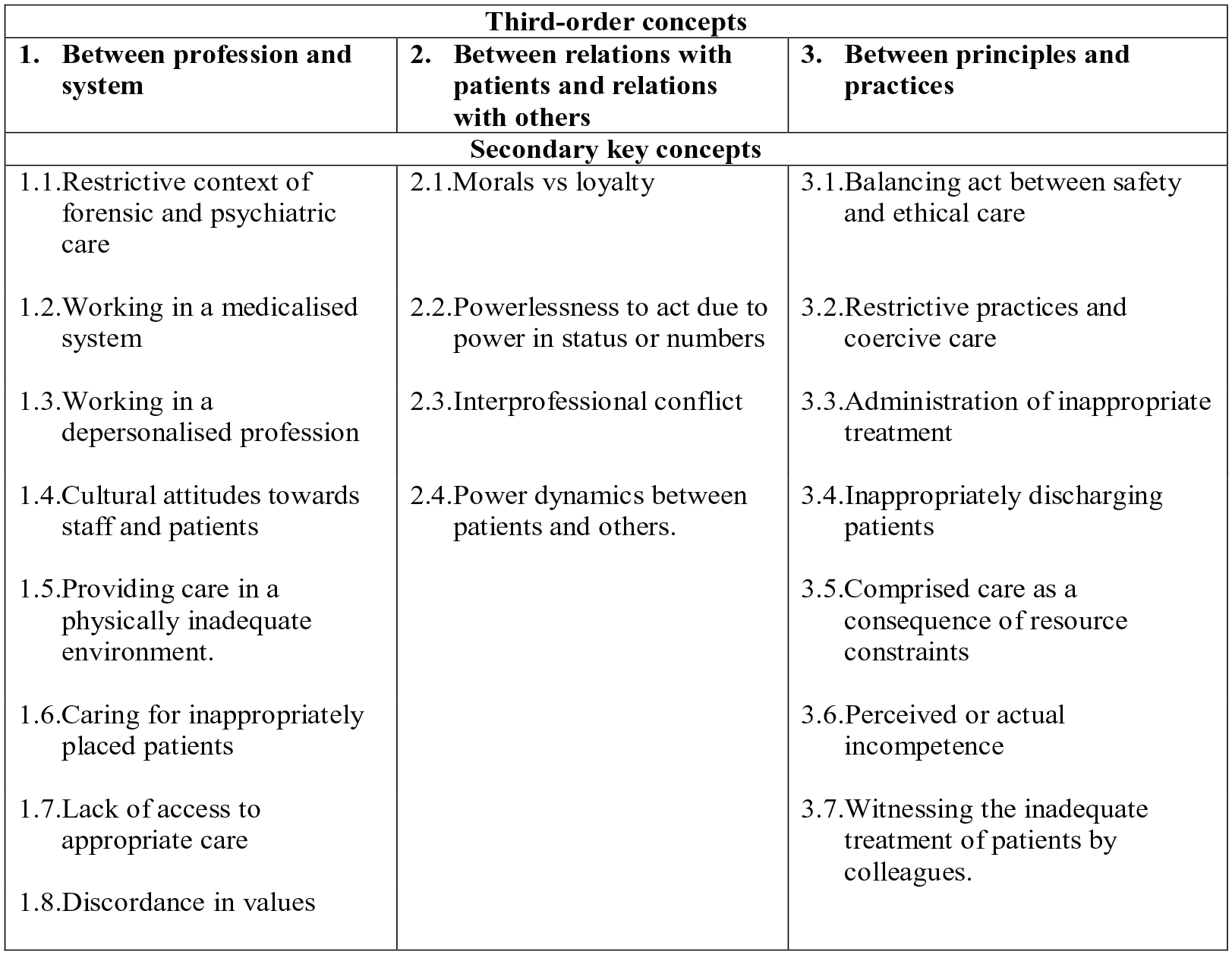
Third-order and second-order concepts from the synthesis.
Between profession and system was apparent in 53% of papers. It encompassed concepts relating to features of the healthcare system that do not align with the values of the profession chosen by an individual. Eight secondary key concepts were situated within this construct, as follows, with cited studies indicated using brackets and aligning to study numbers presented in Tables 2 and 3:
(1) Restrictive context of forensic and psychiatric care, which appeared to be a moral challenge in itself. For staff in psychiatric settings, it was the restrictions placed on patients’ daily living that was morally challenging [11, 20]. For nurses in prison settings, restrictions on their interactions with patients, resulting from enhanced security needs, created moral distress [21]. Regardless, in both instances, the limited freedoms of patients opposed the ethical ideals held by healthcare professionals, that is,
It’s like a prison and the whole idea that you have to get up at certain times, and you have to eat what your told to eat and all of the routine . . . people who go in a psychiatric inpatient ward might feel like it is prison. [11]
(2) Working in a medicalized system where emphasis is on medication and risk management presented as an issue [6, 13, 26]. Ensuring the safety of patients and others had become the core focus of nursing staff, at the cost of other principles of care, that is,
The medicalisation approach of care for psychiatric patients has overlooked the principles of “care” in the context of nursing, and consequently the emphasis seems to have shifted more towards safety management. . .. [13]
(3) Working in a depersonalized profession created moral distress across disciplines. The focus on organizational tasks led them to feel as though they were “doing to” rather than “being with” patients [11, 13]. In both instances, the failure to provide the care that they felt they should be giving reflects a potential self-perpetrated moral transgression, that is,
I find that institutional constraints do not promote person centred values, but rather are punitive to a group of vulnerable, damaged young people. . .. [13]
(4) Cultural attitudes toward staff and patients were also apparent. Working in a service that arguably “dehumanized” nurses was morally distressing for this professional group [27, 28, 30]. An acceptance of bullying toward staff and patients was also an ethical challenge across professions [17]. Linked to this was the inability or unwillingness to challenge such a culture, which reflected an additional layer of moral distress, that is,
I think that it has become so engrained and that’s the language that people have heard in terms of the behaviour that they’re seeing and that is bullying, but it’s been labeled as strong personalities or “suck it up” or “that's how we do it here.” [17]
(5) Discordance in values between staff and their workplace [3, 6, 17, 26]. Such lack of concordance created a sense of division between the healthcare professional and service provider. Additionally, discordance in values within the healthcare system was also discussed, with nurses associating their distress with the inconsistencies in practices and values between services within an organization [16], that is,
The overall goal is not the health and welfare of the client, and sometimes we have to advocate for the client at risk of alienating the institution of which we are a member, because their priorities are slightly different than our priorities as health care providers. [3]
(6) Caring for inappropriately placed patients who had been diverted away from the most appropriate services was another ethical challenge [17], that is,
So that’s where the ethical dilemma lies. We kept somebody certified when they didn’t necessarily have an Axis 1. . .. [17]
(7) On the other side of this, moral distress was also linked to the patients that staff were not seeing, with the initial Lack of access to appropriate care presenting as a moral dilemma [12]. The act of caring or, in some instances, not caring for patients, in the knowledge that they are not receiving the necessary care, may be appraised as a self-transgression, that is,
To other services . . . we’ve been saying, if you even suspect psychosis, talk to us, you know, we want to know about it. . .. And then at the moment, people are referring to us, and we’re saying we won’t even assess a lot of those referrals. [12]
(8) Providing care in a physically inadequate environment, as a consequence of the under-funded healthcare system. For nurses, the issues of the physical environment related to their size, lighting, sparsity, and the inadequacy of operations [1, 5]. For psychologists, working in a service in which its physical design hindered their ability to uphold confidentiality was morally distressing [3]. In both instances, staff found themselves operating in ways that were against the ethical code of their profession. That is,
The seclusion rooms are like prison cell blocks. . .. So there’s a lot of medication given in there just because physically if they had a better set up they would be able to calm themselves a little bit easier. [5]
Between relations with patients and relations with others was apparent in 40% of papers. It encompassed concepts relating to the distress that arises from having to work between patients, colleagues, and carers. Four secondary key concepts were situated within this construct as follows:
(1) Morals versus loyalty. Healthcare professionals reported the difficulties in acting in accordance with their moral values when it threatened their loyalty to the team [2, 6, 19, 20], that is,
What stops me from acting was I am part of a team . . . if I intervene in these situations I’m interfering with primary nursing, and I think I would be seen as splitting the team by taking the side of the patient. [6]
(2) Powerlessness to act due to power in numbers or status was a source of moral distress [6, 13, 17, 19, 26], which captured hierarchical relational structures as inhibiting staff from challenging decisions related to patient care and staff welfare, that is,
When I expressed my concern over what seemed like a blatant error in diagnosis, my instructor . . . who I held in really high esteem . . . just said “Docs don’t misdiagnose . . . there’s no misdiagnosing here,” and I was thinking, “Are you kidding me? Like, isn’t that against everything we’ve ever learned about critical thinking and looking at the specifics and questioning. . .?” [26]
(3) Interprofessional conflict [21, 27, 29] appeared as another source of distress. Nurses reported a minimization of their role by staff working in other healthcare professions [27, 29]. In correctional settings, conflict appeared to arise with non-healthcare staff (e.g., prison officers) due to differential priorities (care vs. security), which posed as an obstacle to the provision of quality care, that is,
Prison officers are supposed to collaborate with you but this spirit of collaboration is very difficult to see. . .. In the end all this makes it more difficult to provide proper care. [21]
(4) Power dynamics between patients and others. Healthcare professionals appeared to have greatest power over the care of patients [2, 8, 9], which was exacerbated when staff failed to advocate for patient participation in decision-making. For staff in adolescent services, the involvement of guardians in care decisions brought further challenges [8]; both the inclusion of family members as advocates for patients under the age of 16 years and the exclusion of family members once patients were of age to consent to treatment had the potential to cause moral distress, that is,
When the consent from the parents is valid, they are “inside” and begin to influence what is going on. . .. How many parents have insight into what they are agreeing to when hospitalising their youth? It is not easy. [8]
Between principles and practices was apparent in 83% of papers, encompassing concepts relating to conflicts between the principles of healthcare and the practices of healthcare professionals. Seven secondary key concepts were situated within this construct as follows:
(1) Balancing act between safety and ethical care [8, 10, 12, 21, 23, 25], and thus discordance in the principles of the healthcare profession itself. For example, upholding one bioethical principle (e.g., patient autonomy) risks the violation of another (e.g., non-maleficence). Thus, moral injury may develop even in circumstances where the transgression has occurred as a consequence of upholding one moral value, that is,
It is very difficult, it is the patients’ safety and the staff’s safety, while there is a continuous pressure to use as little coercion as possible—that is perhaps our greatest moral dilemma. [10]
(2) Restrictive practices and coercive care also commonly emerged as difficulties. Some healthcare professionals discussed restrictive practices [4, 5, 14, 18, 22] and coercion [8, 10, 20, 26, 28] as challenging due to their conflict with the principles of care. Despite acknowledging the necessity of such practices, restraint and coercion led to feelings of shame and guilt, which are characteristic of moral injury. Alternatively, others attached specific conditions to which coercion and restrictive practices became morally distressing. For some, restrictive practices were distressing when used beyond the confines in which they are justified [6, 12, 18], while coercive care was a moral challenge when used against patient’s wishes [2], inappropriately [6, 10, 23], such as to attain consent from a patient with limited capacity, or to deliver treatments that they did not agree with [10], that is,
It’s not to be taken lightly when you put your hands on somebody. It’s wrong really. It’s like the opposite of therapeutic touch. [4]
(3) Connected to the earlier concept, the administration of inappropriate treatment [2, 21] was also a source of moral distress in itself, that is,
I’m not willing to necessarily give this woman who’s in the final stages of her life ECT, to certify her, to make her psychiatric, to force treatment upon her. [2]
(4) Inappropriately discharging patients, due to pressure to free up beds for new admissions [12, 15, 20] was another source of moral distress, that is,
I think it’s important to say that we had a suicide of a patient a month after he was discharged. . . .I think it’s tricky because you start kind of reviewing your decisions. I know it was a month before . . . but you always question, like, was he really ready, were things in the community really ready for this kind of risk management. [12]
(5) Compromised care as a consequence of resource constraints was also a prevalent source of moral distress, due to the alterations in usual practice that healthcare professionals were forced to make [1, 12, 19, 24, 27, 29], as well as the subsequent risks to safety [27, 28, 30] and impacts on engagement with patients [1, 10, 15, 21, 28, 30], that is,
A lot of things are missed, you know, and that’s frustrating because you want to provide the care and yet things just fall through the cracks. [1]
(6) Perceived or actual incompetence of the self, linked to a lack of skills, was also reported as contributing to moral distress. For example, working beyond the scope and responsibilities of the professional role presented as a moral dilemma [27, 29]. Additionally, healthcare professionals experienced moral distress when they perceived that they lacked the competence to ensure the safety of patients and colleagues [2, 16, 20], that is,
That’s a safety issue, so there’s my responsibility, to keep the patient safe . . . so the distress for me was . . . did I put my patient and our unit at risk? . . . And it put me in distress because I doubted my practice, I doubted my decisions, I doubted what I had done with this patient. [16]
Beyond the self, moral distress also arose from the perceived or actual incompetence of colleagues. For nurses, working with colleagues whose standards of care placed patients at risk was morally challenging [10, 27].
(7) Witnessing the inadequate treatment of patients by colleagues, was a source of moral distress transcending across papers [1, 17, 20, 26]. Healthcare professionals discussed the difficulties of being exposed to abusive behaviors that compromised the dignity of patients, as well as displays of neglect, in which colleagues had given up on caring for patients, that is,
I run to another ward when we hear the assault alarm and find a half-naked woman lying on the floor. As I understand it, the patient has “moved into top gear” and will be given an injection. . .. I’m distressed about the woman lying there half naked (why didn’t anyone think of covering her with a blanket?) [20]
Discussion
Through a systematic literature review and meta-ethnographic synthesis, insights into the situations and experiences posing as sources of moral or ethical distress and potentially, moral injury, emerged. While articles commonly focused on the moral issues of a specific aspect of care, such as physical restraint, the findings indicate that PMIEs extend beyond this and can be formulated as a multilayered system of dichotomies. Specifically, potential sources of moral injury were located in features of the healthcare system, in relationships with patients, staff, and carers, and in specific practices displayed by the self and colleagues. A line of argument synthesis can also be proposed from these findings and is theorized in Figure 3, where a funnel model of moral distress is presented.
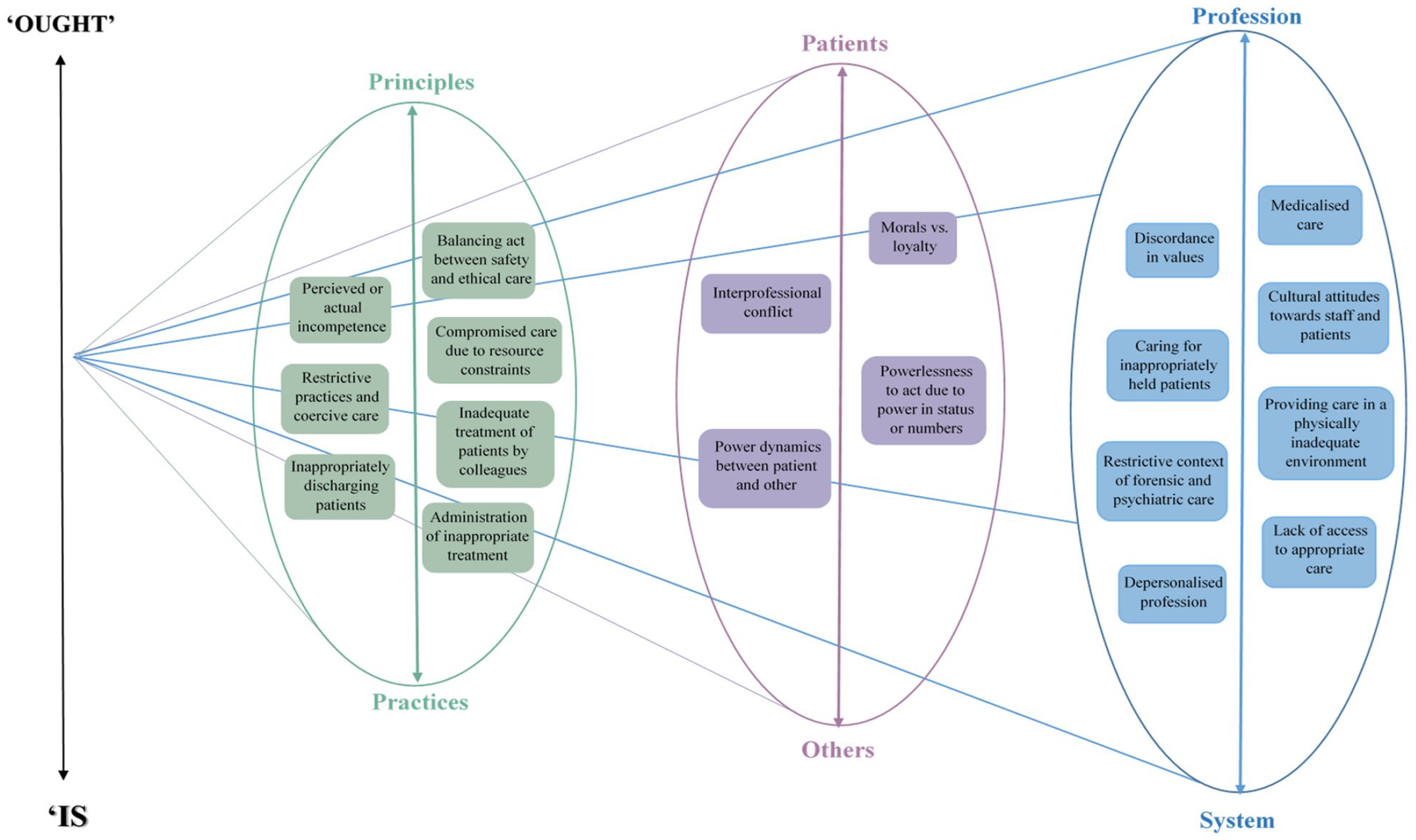
A funnel model of sources of moral distress for healthcare professionals in forensic and psychiatric settings.
This model captures a pattern that emerged across all three third-order constructs and represented the discrepancy between “ought” and “is.” Healthcare professionals described a series of ideals—the “ought” —and discussed how these contrasted to the reality—the “is” —of their experiences. This finding is not novel to this research but has been extensively described within the nursing literature as the “theory–practice gap” (Rolfe, 1993). The findings of the current review widen its applicability and relevance to other professions beyond nursing. Consequences of this gap are reported to include reduced credibility of the nursing profession, poor motivation of staff, and reduced quality of patient care (Ajani & Moez, 2011), all of which were again paradoxically found to be potential sources of moral injury.
Furthermore, the third-order constructs appeared interlinked in a hierarchical structure. Principally, the “between profession and system” concept appeared as the overarching construct, transcending through sources of moral distress situated within the lower-level third-order concepts of “between relations with patients and relations with others” and “between principles and practices.” For example, the power dynamics between patients and others described by healthcare professionals was grounded in system-level factors. While staff recognized the importance of asymmetry in power for safeguarding and upholding patient dignity, the coercive culture existing in psychiatric settings challenged their ability to exercise authority positively. The moral distress resulting from imbalances in power was therefore problematic due to the cultural context in which such imbalances were existing. At a secondary level, discordance between the principles of healthcare and actual practices by staff, represented in the “between principles and practices” concept, appeared rooted as a consequence of relational conflicts, as reflected in the “between relations with patients and relations with others” concept. For example, the administration of inappropriate treatment primarily occurred as a result of external pressures, namely the views of colleagues. Staff engaged in immoral practices due to their desire to avoid conflict with colleagues. Such findings support the notion that moral injury arises as a “slippery slope” (Welsh et al., 2015), suggesting that an immoral system provides the mechanisms for moral disengagement and transgressions by individuals.
Importantly, at its core, the current review demonstrated how moral distress arose from a misalignment between the values of the healthcare profession and the actual healthcare system, as has been previously theorized (Dean et al., 2019), though not evidenced. Staff reported on the challenges of operating within a system that was at odds with what they believed to be at the heart of their role. This third-order construct, and the concepts encompassed within it, contest the dominant definitions of a PMIE that conceptualize such sources as overt “acts” of transgression and betrayal (Litz et al., 2009). Indeed, the most frequently identified PMIEs were those that reflected direct behaviors enacted by the self or others, as present in 83% of articles. Yet, whereas direct displays of transgressions and betrayals involve a culpable act of perpetration by the self or another, concepts situated within the “between profession and system” construct involved no direct act of culpability by an individual. Such instances arguably reflected the notion of a “moral paradox,” in which no transgressive act has occurred, but rather there is discordance in values or conflict in moral paradigms. Whether morally paradoxical situations are PMIEs themselves or rather a precondition to PMIEs remains an area of debate, though the line of argument (see Figure 3) suggests that many of the contextual concepts identified within the “between profession and system” construct may provide the conditions for PMIEs to occur.
Such systemic incompatibilities gave rise to relational conflicts, with staff having to operate between multiple parties and, by virtue, often acting against the best interests of those in their care. Relationships with colleagues have long been noted as a source of stress for healthcare workers (e.g., Menzies Lyth, 1959), which is perhaps unsurprising given the collaborative and interdisciplinary nature of psychiatric healthcare. Unique to this review, however, was the additional relational dynamics brought about by the forensic context, due to the obligation to abide by rules dictated by security demands, rather than care needs. Sherif’s (1966) Realistic Conflict Theory accounts for such competing priorities, noting that hostility may arise when groups’ goals are independent. Thus, such circumstances may profit from a salient multidisciplinary team identity and the generation of shared goals to facilitate congruence.
These two upper layers of PMIEs, positioned at a systemic and a relational level, created the conditions for staff to engage in practices that contrasted with the principles of their profession (“between principles and practices”). Staff working in a range of professional roles battled with the seemingly impossible task of ensuring the safety of patients, staff, and public while simultaneously providing the most ethical care. A temporary stage of moral distress has been framed as inherent to newly qualified nurses entering the profession (Kramer, 1974). However, the moral challenges reported by Wojtowicz et al. (2014), who utilized a sample of nursing students, thematically aligned with those reported in other articles utilizing samples of qualified professionals with much greater lengths of experience in healthcare. Thus, the findings of this review suggest that many PMIEs do not dissipate with experience.
Implications for Practice
Addressing the systemic root in which PMIEs occur is likely to be key in mitigating sources of moral injury, with effects at every layer (see Table 4). Establishing safe avenues for staff to speak out about immoral practices may be important for reducing barriers to challenging moral transgressions by others and thus, the likelihood of an event being appraised as a self-transgression. Equally, providing opportunities for staff to discuss self-transgressions through mediums, such as supervision and ethics consultation groups, may enable them to work through unresolved moral conflicts. There is need for psychological safety to first be established within an organization, however. Given the effects of the healthcare culture on staff wellbeing evidenced in the current review, monitoring organizational climate may also reflect an important priority for healthcare services and their regulators. Furthermore, education and training may be powerful tools that serve to inoculate healthcare staff, to some extent, against moral injury by better preparing them for the realities of the profession and equipping them with greater skills to manage moral challenges, when they arise. Nevertheless, given the multilayered dimensions within which PMIEs occur in healthcare, strategies put in place to tackle this issue need to reflect this. Changes in individual behavior and practice, as a result of systemic modifications, will likely reinforce developments in culture through bottom-up processes (Erez & Gati, 2004).
Summary of Implications for Research and Practice.
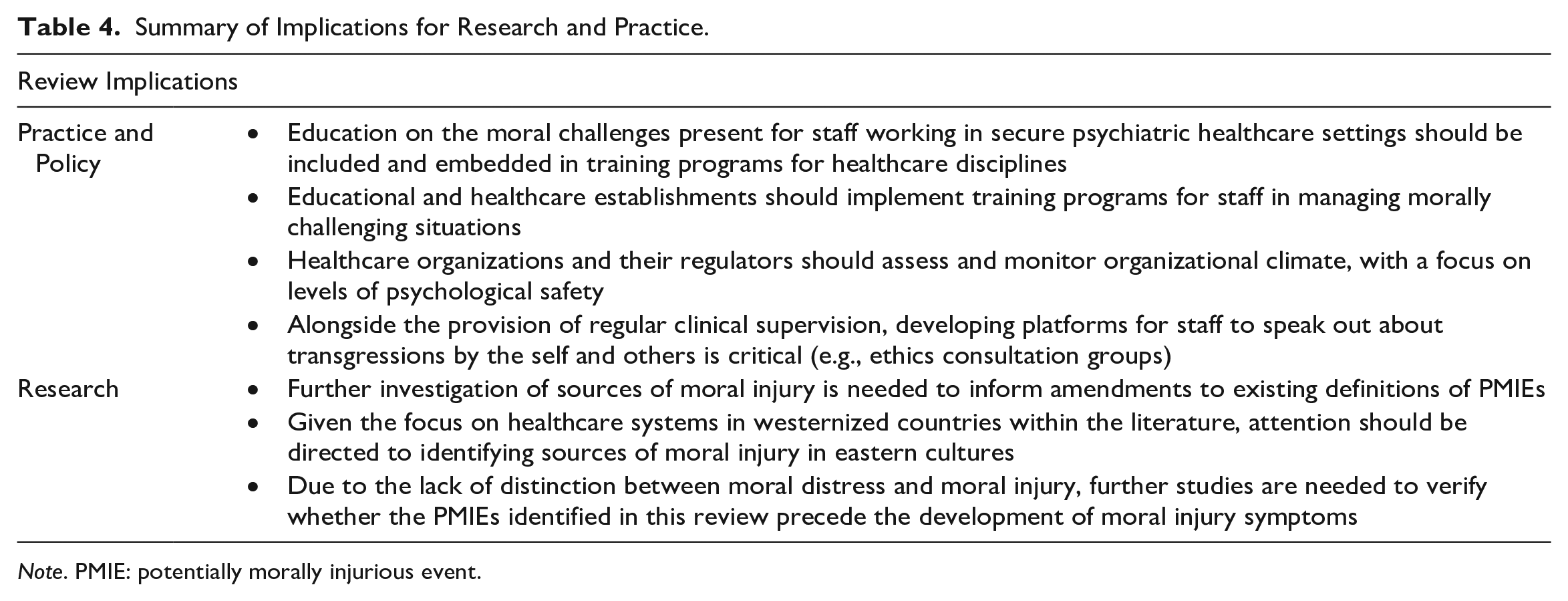
Note. PMIE: potentially morally injurious event.
Conceptually, the findings challenge the dominant understanding of moral injury appraisals. Current tools (e.g., Moral Injury Events Scale; Nash et al., 2013) distinguish between self- and other-perpetrated transgressions. Nevertheless, the two may not be entirely independent, with many of the concepts emanating from the meta-ethnography highlighting overlap in “self” and “other” appraisals. This is consistent with Hoffman et al. (2019) who identified three moral injury appraisal profiles, including a “Moral Injury Other and Self” subgroup. As such, “self” and “other” appraised transgressions may not be mutually exclusive.
Limitations
The findings should be considered in light of several limitations. In the first instance, the current study was conducted as part of an independent doctoral program of study, and thus screening, data extraction, and synthesis were primarily completed by one author. Taken in consideration with the moderate level of rater agreement on the themes generated from the synthesis, the findings reported in this review may be subject to greater level of bias than had multiple reviewers been employed. Furthermore, a primary aspect of the philosophy underlying meta-ethnography is the continual consideration of the context of data. However, it was not possible to comparatively analyze ethnic or cultural differences in sources of moral injury as few studies reported on the ethnic backgrounds of participants, and articles were almost exclusively conducted in westernized countries. Thus, the findings may reflect a western-centric model. The review is also limited by the lack of distinction between “moral distress” and “moral injury.” While this review offers preliminary insight into potential sources of moral injury, associations between the PMIEs identified here and moral injury symptomology warrant exploration.
Future Research Directions
The review also raises a number of priorities for driving the research agenda forward. In the first instance, empirical, prospective investigation is necessary to determine whether the PMIEs identified in this review do in fact precede the development of moral injury symptoms. Secondly, the review illustrates the ethnocentric state of the literature in this field, with studies primarily focused on the experiences of staff working in western healthcare systems. As healthcare systems differ both between and within cultures, there is need for greater examination of sources of moral injury in non-westernized healthcare systems. Previous literature has documented differences in the types of events experienced as morally injurious dependent on characteristics such as ethnicity (e.g., Webb et al., 2023). Thus, intersectionality may prove a fruitful framework for application in future investigation of PMIEs in healthcare.
Conclusions
The findings advance conceptual insights into the potential sources of moral injury for healthcare workers in forensic and psychiatric settings. Through the utilization of a meta-ethnographic approach, the multiple layers across which PMIEs may occur became apparent. The findings indicate that potential sources of moral injury faced by healthcare professionals in forensic and psychiatric settings, which appear to occur in the context of wider contextual facilitators, may not be sufficiently understood through current conceptualizations of a PMIE. Further research is thus necessary to enhance conceptual clarity of this term and to explore the utility of widening the scope of current definitions to account for morally paradoxical experiences.
Supplemental Material
sj-docx-1-tva-10.1177_15248380231167390 – Supplemental material for Potential Sources of Moral Injury for Healthcare Workers in Forensic and Psychiatric Settings: A Systematic Review and Meta-ethnography
Supplemental material, sj-docx-1-tva-10.1177_15248380231167390 for Potential Sources of Moral Injury for Healthcare Workers in Forensic and Psychiatric Settings: A Systematic Review and Meta-ethnography by Elanor Lucy Webb, Jane L. Ireland, Michael Lewis and Deborah Morris in Trauma, Violence, & Abuse
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.