
Abstract
Theoretical and empirical evidence has suggested that child maltreatment victimization is associated with rejection sensitivity. However, empirical evidence on this association is inconsistent. Therefore, this meta-analysis aimed to examine the overall association between child maltreatment and rejection sensitivity, and to investigate variables that may affect the strength of this association. Studies eligible for inclusion were searched in the databases: Web of Science, Science Direct, PubMed, MEDLINE, and China National Knowledge Infrastructure after which relevant studies were coded. Studies were synthesized in advanced three-level meta-analytic models in R. A total of 16 studies (N = 5,335 participants) yielding 41 effect sizes were included. Results showed that child maltreatment is significantly and positively related to rejection sensitivity (mean r = 0.230; p < .001), and to a small extent. Furthermore, this association is stronger for emotional abuse (r = 0.275) than for physical abuse (r = 0.157). It is not affected by the mean age and gender distribution of primary study samples nor by sample type (community sample versus clinical sample). It is concluded that child maltreatment is a risk factor for developing rejection sensitivity later in life. Therefore, interventions for rejection sensitivity should consider potential trauma resulting from prior child maltreatment experiences.
Rejection sensitivity has been defined as a personality disposition characterized by overreaction to social rejection (Downey & Feldman, 1996; Romero-Canyas et al., 2010). People with high levels of rejection sensitivity tend to anxiously expect, readily perceive, and overreact to social rejection (Downey & Feldman, 1996). Rejection sensitivity has been documented to be associated with a range of mental health problems, such as depression, anxiety, loneliness, borderline personality disorder, body dysmorphic disorder (Cavicchioli & Maffei, 2020; Gao et al., 2017), behavioral problems including aggression and victimization (Gao et al., 2021), and eating disorders (De Paoli et al., 2017). Because of the high negative impact of rejection sensitivity, it is important to explore its etiological factors to prevent the onset of rejection sensitivity. Researchers have proposed that rejection sensitivity may originate from child maltreatment (Downey et al., 1997; Romero-Canyas et al., 2010), which is often defined as any act of commission or omission by a caregiver that results in harm, potential for harm, or threat of harm to a child under 18 years of age (e.g., Gilbert et al., 2009). Empirical research on the association between child maltreatment and rejection sensitivity has increased in the last decade. However, until now a meta-analytic review in which empirical evidence on the association between child maltreatment and rejection sensitivity is statistically summarized was not available. This review therefore aimed to statistically synthesize primary studies on the association between child maltreatment and rejection sensitivity.
Different theories have been formulated to illustrate the mechanisms underlying the association between child maltreatment and rejection sensitivity. According to the defensive motivation system model, rejection sensitivity functions as a defensive motivation system (Romero-Canyas et al., 2010). It may result from previous rejection experiences (e.g., emotional neglect, harsh discipline, exposure to family violence, and conditional love by parents; Downey et al., 1997; Feldman & Downey, 1994) in the formative years and is intended to defend the self against future rejection. Rejection sensitivity therefore serves as a motive to avoid rejection by triggering quick defensive responses when potential social threats are perceived. According to this perspective, individuals with high levels of rejection sensitivity are vigilant toward social cues that may signal rejection. In behavioral and neurocognitive research, it was found that participants scoring high on a rejection sensitivity measure are equally vigilant to neutral and rejection faces, and that high rejection sensitivity is associated with increased activity in brain areas that indicate elevated attention and arousal to faces (Ehrlich et al., 2015).
The cognitive-affective processing system (CAPS) framework (Mischel & Shoda, 1995) can be used to explain the triggering situations of rejection sensitivity and individual differences in cognitive-affective processes. The CAPS emphasizes that the personality processes emerge in a specific Person × Situation interactions (Mischel & Shoda, 1995). Accordingly, individual’s rejection sensitivity may be elicited only in threatening situations (e.g., child maltreatment). Furthermore, the CAPS framework assumes that behavior is mediated by a dynamic network of cognitive-affective units including encodings, expectancies and beliefs, affects, and goals that guide responses to triggering cues in specific situations (Mischel & Shoda, 1995). Such a system in intrinsically interactionist and allows for personality change (Romero-Canyas et al., 2010). Therefore, the CAPS framework facilitates designing interventions aimed at reducing rejection sensitivity. Empirical evidence has suggested that using emotion regulation, maltreated adolescents can modulate amygdala responses to negative emotional stimuli to a degree similar to that of non-maltreated youths (McLaughlin et al., 2015).
Attachment theory has a particular focus on the social origins of individual differences in rejection sensitivity. From the attachment perspective, rejection sensitivity may be a key internalized legacy of child rejection experiences (Feldman & Downey, 1994). Attachment theorists proposed that each individual builds internal working models of the world and of himself in that world, with which the individual perceives events, forecasts the future, and constructs his plans (Bowlby, 1973). Working models of the primary attachment relationship(s), the self, and important caretakers are of special significance for social behavior (Bowlby, 1973). Children of rejecting caretakers tend to develop internal working models of attachment relationships as neglecting or overtly rejecting, of others as potentially unsupportive, and of the self as unworthy of love (Feldman & Downey, 1994). These children may develop insecure attachment with their caretakers who responded to their needs with overt or covert rejection and may learn to expect rejection in new situations. That is, an individual’s prior rejection experiences shape their anxious expectation that others will reject them in future social situations. This was empirically confirmed by Set (2019) who found in a sample of university students that as levels of anxious attachment increased, rejection sensitivity increased as well.
The theories and empirical evidence mentioned above provide powerful accounts of the association between child maltreatment victimization and rejection sensitivity. However, primary studies show a rather wide variation in the strength of the association between child maltreatment and rejection sensitivity. For example, some studies have found relatively strong associations between child maltreatment and rejection sensitivity (with correlations >0.450; e.g., Bungert et al., 2015; Chesin et al., 2015), but other studies reported relatively weak associations between child maltreatment and rejection sensitivity (with correlations <0.100; e.g., D. Fang et al., 2021; Massing-Schaffer et al., 2015; Ray, 2018). These inconsistent findings leave us puzzled about the true association between child maltreatment and rejection sensitivity in research and in practice. Therefore, it is necessary to statistically summarize the available primary research on the association between child maltreatment victimization and rejection sensitivity by conducting a meta-analysis. In this way, a better estimate of the true association can be obtained. Furthermore, a meta-analysis allows for testing variables as moderators so that more insight can be gained into what affects the association between child maltreatment and rejection sensitivity.
As for potential moderators, several study characteristics may influence the association between child maltreatment and rejection sensitivity. Child maltreatment includes emotional abuse, physical abuse, sexual abuse, and neglect (X. Fang et al., 2012; Gilbert et al., 2009; Stoltenborgh et al., 2015). Since different types of child maltreatment may contribute differently to rejection sensitivity, child maltreatment type was tested as a moderator. Furthermore, since research has suggested gender differences in consequences of child maltreatment (Moody et al., 2018), the gender distribution of the sampled child victims was examined as a potential moderator. Prior research has also revealed that younger adolescents with high levels of rejection sensitivity were less successful in emotion regulation than older adolescents (Silvers et al., 2012), and therefore the mean age of the included samples was tested as a moderator. Finally, several other study characteristics such as type of sample, the type of measure used for assessing rejection sensitivity, and the type of measure used for assessing child maltreatment were exploratively tested as moderators.
In sum, the available theories and the differences in empirical observations that have been reported emphasize the need for a quantitative synthesis of primary studies on the association between child maltreatment victimization and rejection sensitivity. Therefore, this review aimed to meta-analytically summarize the results of these studies, and to examine potential moderating variables of this association. To meet this aim, an overall association was estimated first, after which several variables were tested as moderators. Based on prior theory and research, we hypothesized that child maltreatment is significantly and positively associated with rejection sensitivity. Regarding potential moderating effects, we did not formulate any hypotheses, as firm and valid expectations cannot be drawn from previous theory or research.
Method
This meta-analytical review was conducted and reported in accordance with the PRISMA 2020 guidelines (Page et al., 2021).
Data Sources and Search Strategy
The electronic databases such as Web of Science, Science Direct, PubMed, MEDLINE, and China National Knowledge Infrastructure were searched for relevant records at first. These five electronic databases were selected as the vast majority of the relevant literature written in English and Chinese is indexed in these databases. The following two syntax components were used in searching the databases: (“child maltreatment” OR “child abuse” OR “child neglect” OR “child trauma” OR “harsh punishment”) AND (“rejection sensitivity” OR “interpersonal sensitivity”). In each search command, we used different combinations of these keywords. Given the language skills of the research team, the search was restricted to studies in English, Chinese, and Korean that were published up to June 30, 2022. Second, reference lists of included and review studies were manually screened to identify additional potentially eligible studies that did not come up in the database searches. Third, we contacted authors by email to request for full-text article if an article was not available but seemed eligible for inclusion given the title and abstract.
Eligibility Criteria
Studies were included if they met the following criteria: (1) The studies were quantitative in nature and reported on empirical findings. (2) The study had to be published in English, Chinese, or Korean. (3) The study design had to be cross-sectional or longitudinal. (4) The study had to examine the association between child maltreatment and rejection sensitivity. (5) The study had to report at least one effect size representing the association between child maltreatment and rejection sensitivity. (6) A study was available as journal article or as (part of a) thesis that could be accessed by the authors.
Study Selection and Coding of Studies
The title and abstract of the duplicated records were screened to remove clearly irrelevant studies. The full text of the remaining records was then thoroughly assessed by four blinded researchers to determine their eligibility for inclusion. Discrepancies between the researchers were resolved by discussion.
Data extraction was performed by one researcher and verified by a second independent researcher. To meaningfully synthesize and analyze the primary studies, a spreadsheet was developed to code and evaluate the included studies on the basis of the following characteristics: (a) study author(s), (b) year of publication, (c) research design (i.e., cross-sectional or longitudinal), (d) country in which a study was performed, (e) sample type (which was coded as “community” when participants were recruited from general community settings, or “clinical” when participants were recruited from clinical settings), (f) sample size, (g) gender (i.e., percentage of females), (h) mean age (if mean age was not reported, the median age was coded), (i) measurement of child maltreatment, (j) measurement of rejection sensitivity, (k) type of child maltreatment (i.e., physical abuse, emotional abuse, sexual abuse, and neglect), and (l) effect size (i.e., the zero-order correlation coefficient). All extracted effect sizes were unadjusted effect sizes.
Study Quality Assessment
In accordance with the quality assessment tool for observational cohort and cross-sectional studies (National Institute of Health, 2014), we assessed the study quality of all included primary studies. The first two authors of this review coded the study quality of each included study, and disagreements in study quality coding were resolved by discussion until consensus was reached for each included primary study.
Statistical Analyses
A correlation coefficient was extracted for each association between child maltreatment and rejection sensitivity that is reported in a primary study. Prior to data analysis, we transformed correlation coefficients into Fisher’s z-scores, as correlations are not normally distributed (Cooper et al., 2019). After the statistical analyses were completed, the Fisher’s z-scores were converted back into correlations to facilitate interpretability.
A three-level meta-analytic model was built to first determine the overall association between child maltreatment and rejection sensitivity. The three-level random effects model examined three sources of variance to model effect size dependency: the sampling variance of the observed effect sizes (Level 1), the variance between effect sizes extracted from the same study (Level 2), and the variance between studies (Assink & Wibbelink, 2016). We interpreted the overall association following Cohen’s (1992) guidelines for interpreting effect sizes, with the criteria 0.10, 0.30, and 0.50, for small, medium, and large correlations, respectively. Mixed-effect models were used to conduct bivariate moderator analyses. Duval and Tweedie’s trim-and-fill analysis (Duval & Tweedie, 2000) was performed to evaluate the risk and impact of publication bias.
The metafor package (Viechtbauer, 2010) was used to conduct all analyses in the statistical software R, version 4.1.2 (R Core Team, 2016). The R syntax was written following the tutorial of Assink and Wibbelink (2016). The restricted maximum likelihood method (Viechtbauer, 2005) was applied to estimate all model parameters, and a two-tailed p value smaller than .05 was considered as statistically significant.
Results
Literature Search and Study Characteristics
The PRISMA flow chart of the study selection process is presented in Supplemental Appendix A. At first, 1,342 studies were identified through electronic searches of the five databases. Of these studies, 16 studies met our inclusion criteria and were subsequently included. The study quality assessment revealed that quality scores of all included studies were fair to good (see Table 1 and Supplemental Appendix B). In terms of country where the primary studies were conducted, eight (50.0%) were conducted in the United States, five (31.3%) in China, two (12.5%) in Korea, and one (6.3%) in Germany. In total, 15 studies (93.8%) examined community samples and two studies (12.5%) examined clinical samples. The mean age of participants in the included studies ranged from 16.0 to 32.0 years (M = 22.92, SD = 4.33). Table 1 presents several study characteristics of the included studies. Supplemental Appendix C presents the formulas that were used in the data analysis and references to the included studies are shown in Supplemental Appendix D. In all, 16 primary studies examining N = 5,335 participants could be synthesized, and these studies produced 41 effect sizes in total.
Studies Included in the Meta-Analysis.
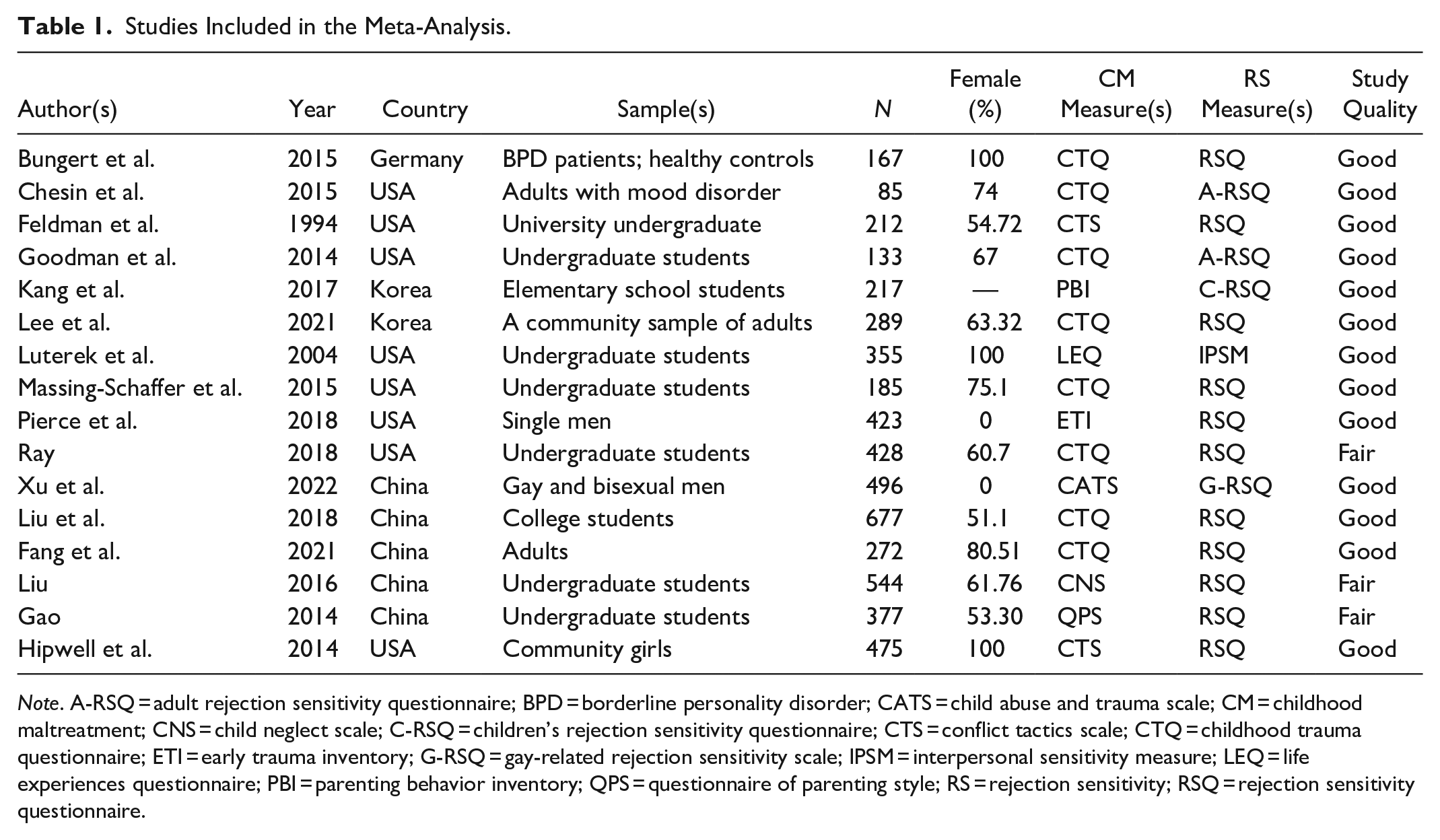
Note. A-RSQ = adult rejection sensitivity questionnaire; BPD = borderline personality disorder; CATS = child abuse and trauma scale; CM = childhood maltreatment; CNS = child neglect scale; C-RSQ = children’s rejection sensitivity questionnaire; CTS = conflict tactics scale; CTQ = childhood trauma questionnaire; ETI = early trauma inventory; G-RSQ = gay-related rejection sensitivity scale; IPSM = interpersonal sensitivity measure; LEQ = life experiences questionnaire; PBI = parenting behavior inventory; QPS = questionnaire of parenting style; RS = rejection sensitivity; RSQ = rejection sensitivity questionnaire.
Overall Association and Publication Bias
Table 2 displays the overall association between child maltreatment and rejection sensitivity (r = 0.230, p < .001), which is significant, positive, and small according to Cohen’s (1992) criteria for interpreting the strength of correlations.
Results for the Overall Association Between Child Maltreatment and Rejection Sensitivity.
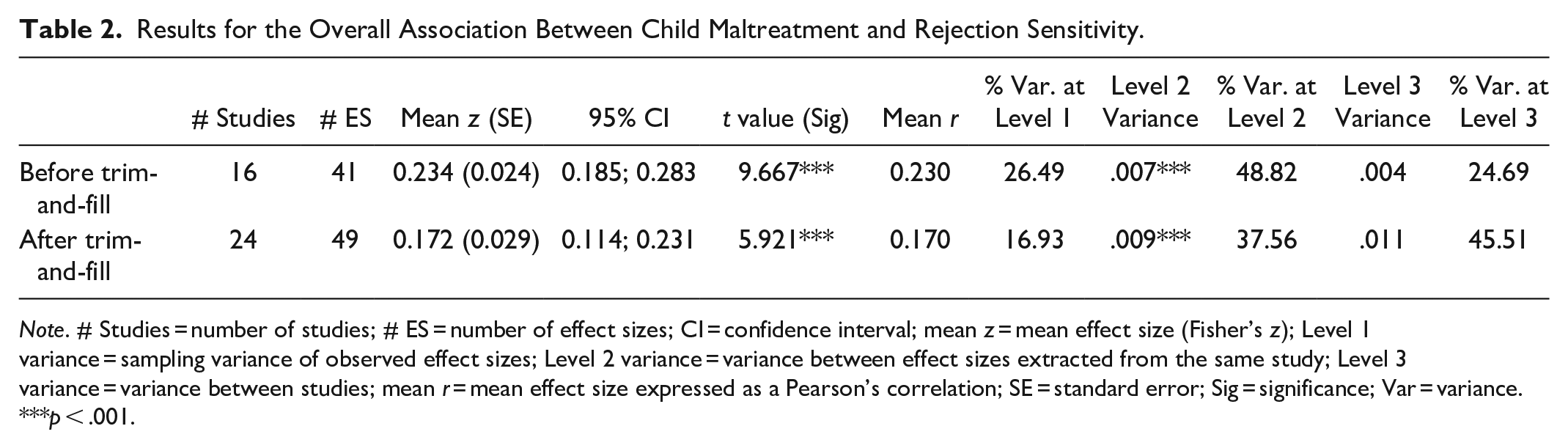
Note. # Studies = number of studies; # ES = number of effect sizes; CI = confidence interval; mean z = mean effect size (Fisher’s z); Level 1 variance = sampling variance of observed effect sizes; Level 2 variance = variance between effect sizes extracted from the same study; Level 3 variance = variance between studies; mean r = mean effect size expressed as a Pearson’s correlation; SE = standard error; Sig = significance; Var = variance.
p < .001.
Figure 1 shows the funnel plot in which the effect sizes are plotted against their standard error. The plot reveals asymmetry in the observed effect sizes and that the trim-and-fill algorithm imputed effect sizes to restore the symmetry in the plot. The effect sizes were imputed to the left of the estimated overall effect, implying that the current results may have been affected by publication bias. In Table 2, we can see that after the estimated “missing” effect sizes were imputed, the association between child maltreatment and rejection sensitivity became smaller in magnitude (adjusted mean r = 0.170, p < .001), but still significant and in the positive direction.
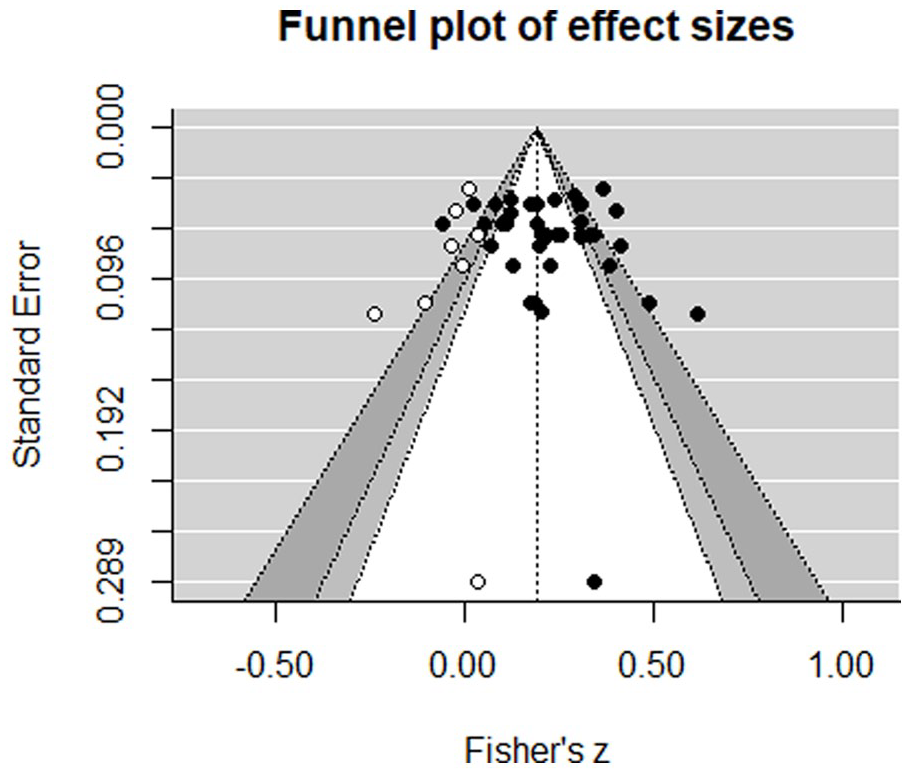
Trim-and-fill plot for the association between child maltreatment and rejection sensitivity.
Moderator Analyses
The results of the moderator analyses are shown in Table 3. We found a significant moderating effect of type of abuse, F (3, 28) = 5.568, p < .01. Specifically, the association between child maltreatment and rejection sensitivity is stronger for emotional abuse (mean r = 0.275) than for physical abuse (mean r = 0.157). For each type of abuse, we found a significant mean association in the positive direction (see Table 3). No other significant moderating effects were found.
Results of Categorical and Continuous Moderator Analyses (Bivariate Models).
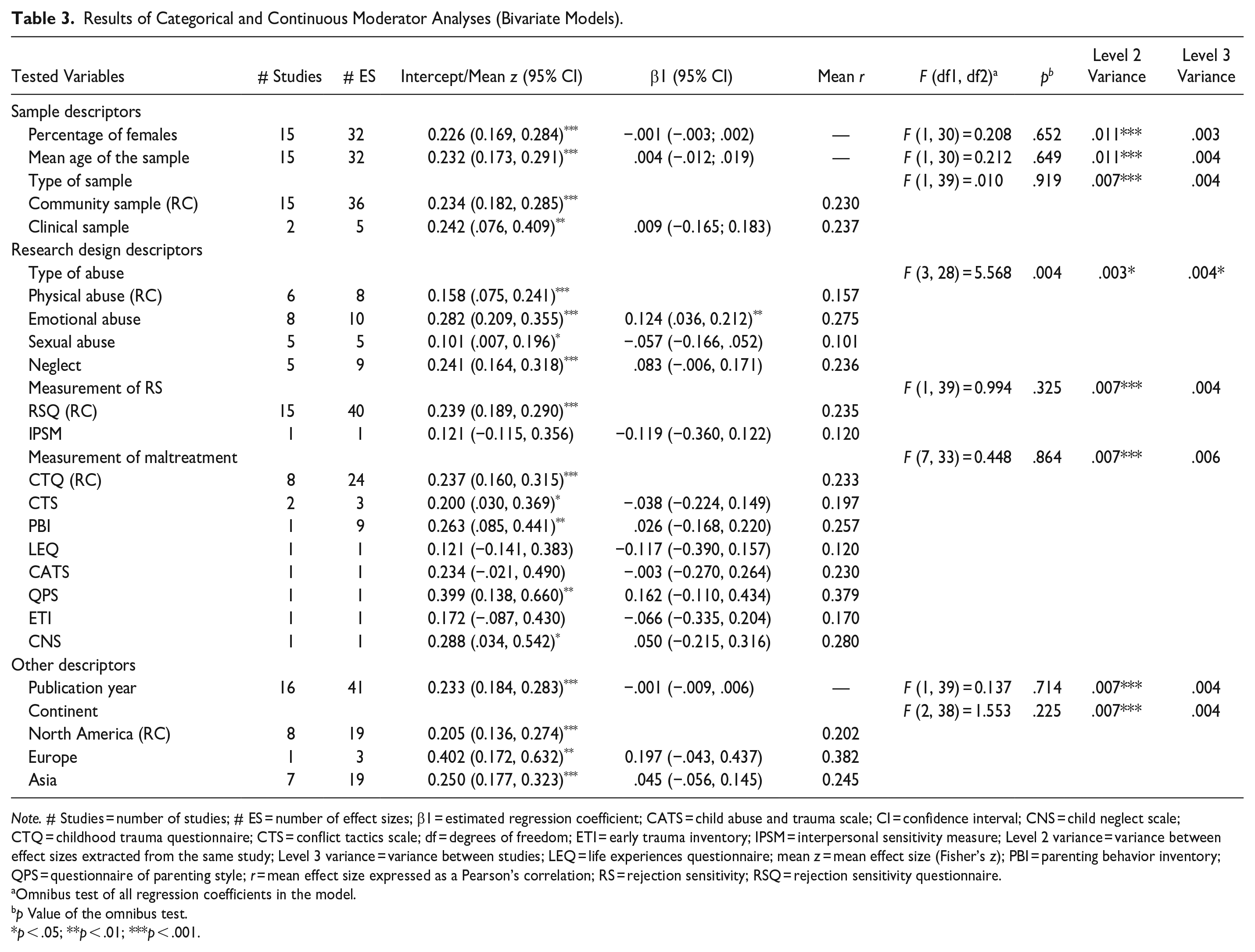
Note. # Studies = number of studies; # ES = number of effect sizes; β1 = estimated regression coefficient; CATS = child abuse and trauma scale; CI = confidence interval; CNS = child neglect scale; CTQ = childhood trauma questionnaire; CTS = conflict tactics scale; df = degrees of freedom; ETI = early trauma inventory; IPSM = interpersonal sensitivity measure; Level 2 variance = variance between effect sizes extracted from the same study; Level 3 variance = variance between studies; LEQ = life experiences questionnaire; mean z = mean effect size (Fisher’s z); PBI = parenting behavior inventory; QPS = questionnaire of parenting style; r = mean effect size expressed as a Pearson’s correlation; RS = rejection sensitivity; RSQ = rejection sensitivity questionnaire.
Omnibus test of all regression coefficients in the model.
p Value of the omnibus test.
p < .05; **p < .01; ***p < .001.
Discussion
This review comprises the first quantitative synthesis of primary studies on the association between child maltreatment victimization and rejection sensitivity. The current results contribute to our insight into the social origins of rejection sensitivity and provide implications for prevention and intervention practices.
Overall Association
The results suggest that child maltreatment is significantly and positively associated with rejection sensitivity. This finding is consistent with previous research suggesting that early interpersonal trauma can lead to rejection sensitivity (Downey et al., 1997). This finding also lent support to the defensive motivation system model (Romero-Canyas et al., 2010), the CAPS framework (Mischel & Shoda, 1995), and the attachment theory framework (Bowlby, 1973; Feldman & Downey, 1994). Notably, the magnitude of this association (r = 0.230) is small according to Cohen’s (1992) criteria. Despite this small effect size, the results convey that child maltreatment victimization is a risk factor for rejection sensitivity. The relatively small magnitude of the overall association may be explained by recall bias and positive interpretation bias. On the one hand, it is likely that a substantial amount of time passes between the age at which the maltreatment occurred and the time at which rejection sensitivity was measured in the primary studies (i.e., the mean age of the included samples is 22.92 years). As time passes, participants may not clearly remember traumatic childhood experiences, such as episodes of child maltreatment. On the other hand, as positive interpretation bias is related to well-being and resilience (Kleim et al., 2014), individuals might be prone to make less negative judgments of traumatic childhood experiences. Therefore, these biases may attenuate the strength of the association between child maltreatment and rejection sensitivity.
It is also likely that most participants were sampled from general populations and may not have experienced severe child maltreatment, which, in turn, may have led to an overall association that is rather small in magnitude. Moreover, across the life span there may be other more important factors influencing rejection sensitivity. For instance, Zanolie and Crone (2021) found that ranking status differentially affected rejection sensitivity in adolescents. In addition, there may be other vital factors that influence rejection sensitivity among adults, such as different and/or multiple forms of discrimination (Feinstein et al., 2012), obesity (Albano et al., 2019), and other adversities that need further exploration.
The trim-and-fill analysis suggested that our results may have been affected by publication bias, but after re-estimating the overall association in which bias was taken into account, the association between child maltreatment and rejection sensitivity was still significant, confirming that child maltreatment is a risk factor for rejection sensitivity although with a modest impact.
Moderating Variables
We found that the strength of the association between child maltreatment and rejection sensitivity was invariant across types of child abuse. Specifically, this association was stronger for emotional abuse victimization than for physical abuse victimization. This finding is in line with neuroimaging findings reported in previous research (Cassiers et al., 2018), suggesting that childhood trauma subtypes such as physical abuse, emotional maltreatment, sexual abuse, and neglect have differential effects on the human brain. Specifically, Cassiers et al. (2018) found that emotional maltreatment correlated with abnormalities in fronto-limbic socioemotional networks. The structural change in socioemotional networks may lead to functional changes in the brain, such as emotional dysregulation in rejection sensitivity. We found that the magnitude of the association between child maltreatment and rejection sensitivity did not vary across sexual abuse and neglect compared to physical abuse, but still, for each of the child abuse types that we examined, we found a significant and positive (small) association. Important to note is that the mean associations found for sexual abuse and neglect were based on only five studies, so these mean associations as well as their non-significant differences with other forms of child abuse should be interpreted cautiously.
With respect to gender, we did not find a moderating effect of the gender distribution of primary study samples. In other words, when exposed to child maltreatment, both females and males seem to have a similar risk for developing rejection sensitivity. Also, no moderating effect of mean sample age was found, suggesting that the strength of the association between child maltreatment and rejection sensitivity is similar across age.
According to our results, the strength of the association between child maltreatment and rejection sensitivity is also similar across sample type (tested as clinical vs. community samples), instruments for measuring rejection sensitivity, instruments for measuring child maltreatment, publication year of primary studies, and continents in which primary studies were conducted. These results point toward stability in the impact child maltreatment has on rejection sensitivity. However, rather small number of primary studies were analyzed in the moderator analyses which limits the statistical power to detect a true moderating effect. Therefore, more primary studies are required to examine variables as potential moderators in a more robust way.
Limitations
Several limitations warrant discussion. First, since all synthesized studies were cross-sectional, this study does not permit drawing conclusions about temporal or causal relations between child maltreatment and rejection sensitivity. To delineate temporal relations between variables, more longitudinal studies with sufficient follow-up are needed.
Second, due to the rather small number of primary studies that could be included, there were limitations in the coding procedure that should be acknowledged. Accordingly, we had to combine physical neglect and emotional neglect into a single neglect category in coding type of child abuse. However, physical neglect and emotional neglect may have distinct effects on the association between child maltreatment and rejection sensitivity. For instance, Grummitt et al. (2022) reported in their study that emotional neglect is a risk factor for mental health problems (i.e., depression, anxiety, and stress) in early adulthood, whereas physical neglect was not found to be associated with any outcome. Furthermore, for two primary studies (Chesin et al., 2015; Goodman et al., 2014), we classified occurrences of both emotional abuse and neglect into the single category of emotional abuse, which may have influenced the results. Finally, we could include one longitudinal association (Pierce et al., 2018) between child maltreatment and rejection sensitivity (r = 0.170) in the data analysis. This may have reduced the (overall) association between child maltreatment and rejection sensitivity, as generally longitudinal associations are smaller than cross-sectional associations between variables. However, longitudinal correlations probably provide a better picture of the true association than cross-sectional correlations. Future (longitudinal) studies are needed to further examine differences in how emotional neglect and physical neglect are associated with rejection sensitivity.
Third, all primary studies included in this review relied on self-report, which may have led to inflated results due to common method variance (MacKenzie & Podsakoff, 2012). Moreover, self-report is often affected by social desirability, as individuals may have different reasons (e.g., feelings of shame and/or guilt) for not disclosing their maltreatment experiences. In addition, the retrospective self-report methods that were used in the primary studies may have caused recall bias. It may be difficult for participants to recall maltreatment episodes because of the amount of time that has passed since the maltreatment episodes, the traumatic nature of the experience, or because participants were too young to remember the maltreatment experience later on.
Finally, we examined the moderating effect of child maltreatment type (physical abuse, emotional abuse, sexual abuse, and neglect) but child maltreatment types are interrelated and often occur simultaneously (Higgins & McCabe, 2001). It may be that associations between child maltreatment and rejection sensitivity are stronger when children are exposed to multiple types or combinations of specific types of maltreatment. This should be investigated in future research.
Implications for Research and Practice
The current findings give more insight into the association between child maltreatment and rejection sensitivity than previous primary research, and as such provide important implications for research and practice. Our study found that compared to physical abuse, emotional abuse has a stronger impact on rejection sensitivity. This may be explained by the fact that particularly emotional abuse is characterized by severe and ongoing assaults of the child’s sense of self (Gilbert et al., 2009) with a higher risk for rejection sensitivity relative to physical abuse victimization. Differences in neurodevelopmental processes between victimization of emotional and physical abuse might also occur. McLaughlin et al. (2015) found differences between maltreated and non-maltreated adolescents in neural responses of the amygdala and other brain structures to negative emotional stimuli relative to neutral stimuli. Whether these differences exist within maltreated children that were exposed to different forms of child maltreatment has not been extensively studied. Thus, future studies could examine these differences and potentially shed light on the neurobiological mechanisms through which different forms of maltreatment are related to rejection sensitivity. Future behavioral studies could also examine potential relevant moderating and mediating factors in the association between child maltreatment and rejection sensitivity, such as supportive relationships (Jittayuthd & Karl, 2022; McDonald et al., 2010) that may play a key role in attempts to break the intergenerational transmission of rejection sensitivity. From a gene–environment interaction perspective, future research exploring the influences of gene and environment on rejection sensitivity seems promising. For example, existing research has reported that variation in the mu-opioid receptor gene (OPRM1) is associated with dispositional and neural sensitivity to social rejection (Way et al., 2009).
In searching the literature for primary studies, we identified both Western studies and studies conducted in Asia. As the continent in which a study was conducted does not moderate the association between child maltreatment and rejection sensitivity, it may be that the current findings are generalizable across continents and not only hold for Western populations. However, this needs to be validated in future research. Further research is also warranted among marginalized and disadvantaged groups (e.g., disabled populations, orphans, people with special health needs, ethnic minorities, and sexual minority groups). These people are vulnerable to being discriminated, neglected, and/or stigmatized by caregivers or others and thus may have experienced more rejection and adversity during child and/or adulthood than the general population. Exploring their experiences of social rejection and performing comparative research on their rejection sensitivity with their counterparts would offer new insights into our understanding of rejection sensitivity.
In terms of practice, the findings highlight that early prevention of (the recurrence of) child maltreatment is most important. This study showed that child maltreatment is a risk factor for rejection sensitivity even though the impact is not that large. Still, early detection and prevention of child maltreatment deserves continuous attention in (clinical) practice to prevent mental health problems, such as rejection sensitivity. As the association between child maltreatment and rejection sensitivity differs across types of child maltreatment, intervention efforts tailored to the needs of individual victims are probably more effective than general interventions offered to victims of all types of child maltreatment. Empirical studies have revealed that the effectiveness of interventions is dependent on how these interventions are implemented, and in particular on how interventions are personalized to meet the specific needs of their target group (Law et al., 2009). Furthermore, intervention programs could be developed based on the CAPS framework (Mischel & Shoda, 1995) to reduce the effect of child maltreatment victimization on rejection sensitivity through strengthening the emotion regulation skills of child maltreatment victims.
Conclusion
This review quantitatively synthesized primary studies on the association between child maltreatment victimization and rejection sensitivity using advanced three-level meta-analytic methods. The results support our hypothesis that child maltreatment victimization is a risk factor for rejection sensitivity. The strength of the association differs by type of abuse, as emotional abuse was found to be more strongly associated with rejection sensitivity than physical abuse. The strength of the association seems stable across age and across men and women. Interventions aiming at reducing rejection sensitivity should consider potential trauma resulting from prior child maltreatment experiences.

Supplemental Material
sj-docx-1-tva-10.1177_15248380231162979 – Supplemental material for Child Maltreatment as a Risk Factor for Rejection Sensitivity: A Three-Level Meta-Analytic Review
Supplemental material, sj-docx-1-tva-10.1177_15248380231162979 for Child Maltreatment as a Risk Factor for Rejection Sensitivity: A Three-Level Meta-Analytic Review by Shuling Gao, Mark Assink, Chongzeng Bi and Ko Ling Chan in Trauma, Violence, & Abuse
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Humanities and Social Science Research Fund of Ministry of Education of China (Grant No. 20YJC840012) and Shanghai Academy.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.