
Abstract
Women who sell sex (WSS) are vulnerable to violence. We present a scoping review of the last decade of research on the prevalence and incidence of, factors associated with, and services regarding violence against WSS in Eastern and Southern African (ESA). A systematic search of various databases resulted in 20 papers being reviewed. Inclusion criteria, applied by the first two authors, were as follows: empirical papers, key research problem is violence against WSS, and conducted in ESA countries. The lifetime prevalence of violence revealed in the studies ranged from 21% to 82%. A pattern of generalized violence against WSS from paying clients, male partners, strangers, family members, friends/acquaintances, and the authorities emerged. Factors associated with violence included the context within which the sex work occurs, alcohol use, type of sex exchange interactions, and personal factors (low education, low income, marriage, youth, high client volume, time in sex work, forced sexual debut, and internalized sex work stigma). WSS seldom access services after violence. Evaluations of two programs, a woman-focused HIV intervention, and the Diagonal Interventions to Fast-Forward Reproductive Health project, showed improvements in gender-based violence services. Findings suggest that targeted programmes should be paired with improving general health services and focus on promoting collective agency among WSS.
Women who sell sex (WSS) in Africa often face criminalization, high mobility, hazardous substance use, limited economic opportunities, and many dependents (Scorgie et al., 2012). These factors, together with the occupational contexts of their work, have highlighted their vulnerability to violence. Indeed, a systematic review of international research on violence against WSS showed the lifetime prevalence of any or combined workplace violence ranged from 45% to 75%, and the incidence over the past year ranged from 32% to 55% (Deering et al., 2014).
Risk factors for violence identified in the studies reviewed by Deering et al. (2014) included the regulation of sex work (e.g., police harassment, arrest, and coercion), unfavourable work environments (e.g., outdoors or public places), economic constraints, social stigma attached to sex work, population movement (e.g., being a migrant sex worker), being coerced into sex work, personal factors (e.g., alcohol or substance use), and gender inequality. While some of these are specific to sex work, others, in particular gender inequality, forms the social backdrop within which sex work is carried out. Indeed, the World Health Organization (WHO) (2021) estimates that the lifetime prevalence of physical and/or sexual intimate partner violence among ever-married/partnered women aged 15 to 49 years in Sub-Saharan Africa is 33%, with the 12-month prevalence being 20%.
Addressing violence against WSS is important not only in and of itself, but also because of its association with other health issues. For example, in a modeling exercise using behavioral and epidemiological data drawn from quality surveillance reports, country reports, and published studies from Ukraine and Kenya, Decker et al. (2013) estimated an approximate 25% reduction in HIV incidence among sex workers when physical or sexual violence was reduced. Interventions that support community mobilization, rights promotion, address social norms, and overcome criminalization-related barriers to health services. The justice sector shows the most promise, as outlined in a review by Decker et al. (2022).
Sexual and reproductive health services for WSS in Africa are, however, underdeveloped. Most interventions are localized and small scale, operate with little coordination nationally or regionally, and have scanty government support (Dhana et al., 2014). They mostly address HIV and other sexually transmitted infections. Gender-based violence services are generally ignored.
Estimates of the percentage of female population engaged in sex work in Sub-Saharan Africa differ, from 0.76% to 1.0% in South Africa, to 5% among the urban female Kenyan population (Fearon et al., 2020). A review of studies from 1995 to 2005 found that between 0.4% and 4.3% of the 15 to 49-year-old female population residing in urban areas across the region were estimated to be engaged in sex work (Vandepitte et al., 2006).
As with other social phenomena, sex work in Africa is deeply embedded in the history of colonialism and postcolonial politics, as outlined by Mgbako (2019). During the colonial period, sex workers often achieved economic autonomy and were able to send remittances to their rural families. Colonial regulation was, however, mostly lax until World War II with the spread of sexually transmitted infections among European troops stationed in Africa. This move toward regulation was entrenched through the widespread criminalization of sex work in postcolonial African states. Such criminalization underpins human rights abuses against sex workers. In response to systemic abuses, an African sex worker rights movement emerged in the 1990s and has spread throughout the continent. Organizations associated with this movement have brought the violence perpetuated against sex workers to public attention.
In this paper, we present a scoping review of research conducted over the last decade on violence against WSS in the Eastern and Southern African (ESA) region. Given the colonial entanglement of sex work (and sexualities in general), the bringing together of knowledge about sex work and violence in the ESA region is important to shed light on what is currently known, gaps in knowledge, and contextually effective interventions. The review was commissioned by UNFPA East and Southern Africa Regional Office as part of a joint United Nations Programme, comprising of UNAIDS, UNICEF, UNFPA, and WHO, that aims to improve the sexual and reproductive health of all people in ESA. This regional focus is on line with the 2013 ESA Ministerial Commitment on comprehensive sexuality education and sexual and reproductive health (SRH) services for adolescents and young people in ESA (Watson et al., 2021). The countries of the ESA region are as follows: Angola, Botswana, Burundi, Comoros, Democratic Republic of the Congo, Eswatini (previously Swaziland), Eritrea, Ethiopia, Kenya, Lesotho, Madagascar, Mauritius, Mozambique, Malawi, Namibia, Rwanda, Seychelles, South Africa, South Sudan, Tanzania, Uganda, Zambia, and Zimbabwe. In all these countries, with the exception of Mozambique, sex work is illegal.
Studies of this nature are used by UNFPA ESA regional office to inform work with regional economic communities, regional NGOs, networks of civil society, including, in this context, the African Sex Workers Alliance, Ministries of Health, national civil society organizations and networks, research institutions and others to advocate for and/or strengthen policy, public health, and community-based interventions to advance the SRH and rights of vulnerable populations.
Method
A scoping review methodology (Arksey & O’Malley, 2005) was used in this project. The general purpose of conducting scoping reviews is to identify and map the available evidence. In line with Munn et al. (2018), our scoping review sought to identify the types of available evidence in the field, and to identify knowledge gaps. This is different from a systematic review which, inter alia, uncovers evidence, confirms practices and investigates conflicting results.
As indicated by Schulkind et al. (2016) sex work is a broad concept with boundaries that are sometimes difficult to define. We follow the conceptualization of sex workers as used in a report by the World Health Organization et al. (2013, p. xii): Female . . . adults and young people who receive money or goods in exchange for sexual services, either regularly or occasionally. Sex work may vary in the degree to which it is “formal” or organized. It is important to note that sex work . . . takes many forms, and varies between and within countries and communities.
We specifically focused on studies reporting on sex work (both individually initiated and organized), rather than sexual exploitation or sex trafficking. Sex work is generally defined as voluntary labor, although, of course, sex work may also involve power relations and various levels of exploitation.
Many studies use the term female sex workers or the acronym FSWs. This defines them narrowly through their (mostly criminalized) labor. The first-person form is generally preferred in other fields (e.g., disabilities studies—people with disabilities; HIV research—people living with HIV). Hence, in line with Crankshaw et al. (2021), we use the term WSS in this article. We, thus, use the acronym WSS rather than FSWs, unless quoting directly from a study.
The following electronic databases were searched: Academic Search Premier; Health Source: Nursing/Academic Edition; Medline; PsyArticles; PsycINFO; SocINDEX; Sabinet; Web of Science; PubMed; and Google Scholar. The key word search terms for studies were as follows: female sex workers 1 OR sex workers AND gender-based violence (GBV) OR domestic abuse OR violence AND [list of countries] OR Eastern Africa OR Southern Africa. The search was restricted to the last 10 years (2010–March 2021) to ensure that the information is current and primary studies were peer reviewed to ensure rigour. No language restriction was placed on the search, in case there were relevant papers in another language (most likely French or Portuguese). The search, however, only surfaced papers written in English.
The initial search produced 84 papers. After 14 duplicates were removed, the first two authors went through the papers independently, determining whether the identified studies were relevant to the research aims. Inclusion criteria were that the papers should: (a) be empirical papers; conducted in ESA countries; and (b) address WSS in relation to violence as the key problem. We excluded nonempirical papers and those that addressed violence in relation to WSS in passing. Theoretical, review, commentary papers were excluded. Each author’s assessments were compared. If there were differences, then they were resolved through discussion. The papers were quality checked through the use of the mixed methods appraisal tool. On the basis of our joint appraisal of the series of methodological questions posed in the tool, including general questions, questions for qualitative, quantitative, and mixed methods studies, 1 no studies were discarded. The result was 20 papers. The process is displayed in a flowchart diagram in Figure 1.
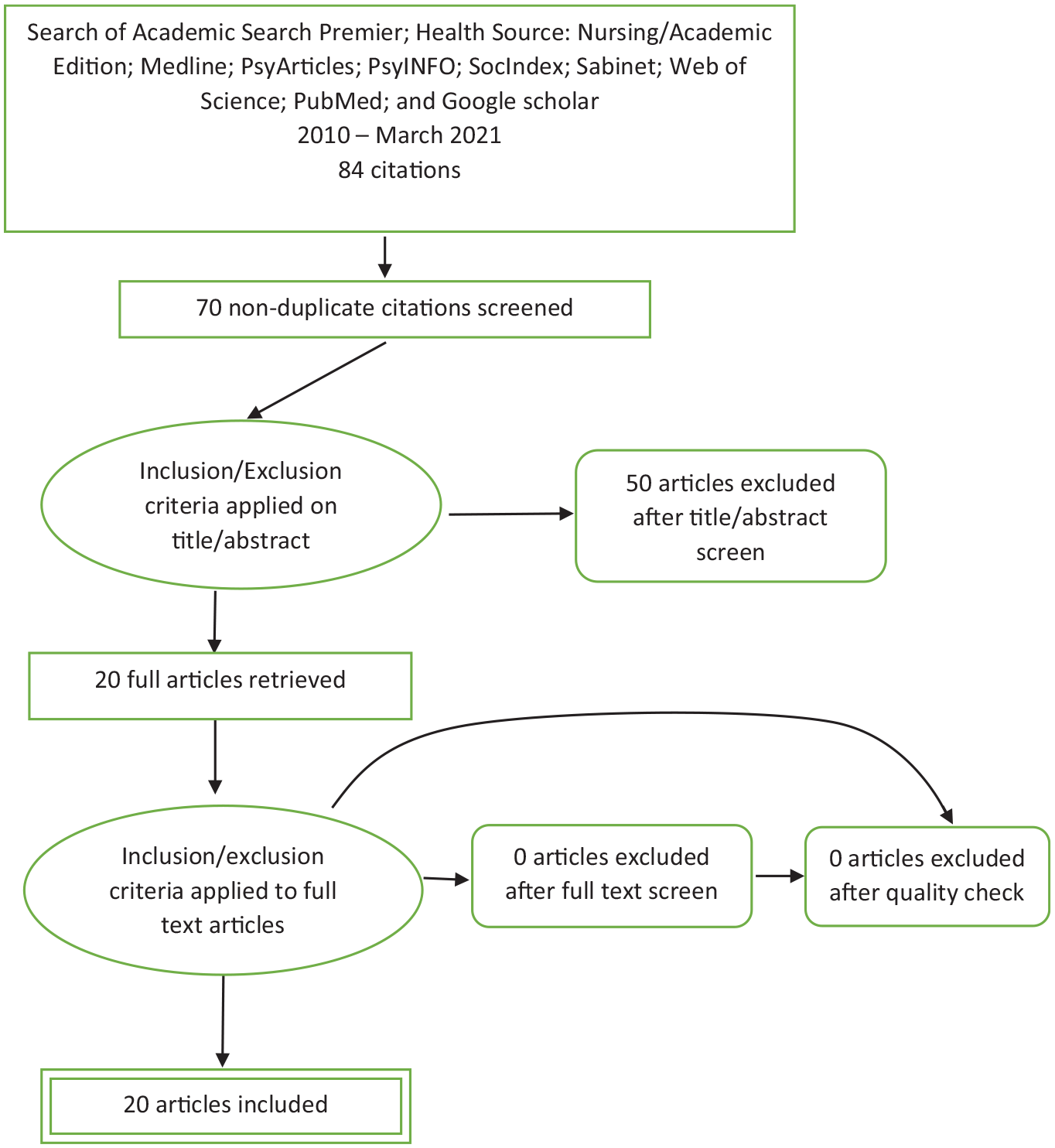
Preferred Reporting Items for Systematic Reviews and Meta-Analyses diagram.
The studies were charted as follows. First, eligible studies were summarized in an Excel form, including the following information for each publication: author(s), year of publication, study location, method, study populations, aims of the study, important results, and study recommendations. Second, the literature and information on programmes were organized thematically. Prevalence/incidence, factors associated with violence, and services emerged as the major overarching themes. In the results we present overall findings in these areas, fleshed out by insights (often gained through qualitative research) on the mechanisms underpinning these findings. We included all relevant insights found in the included articles.
Results
Kenya features as the country in which the most research on this topic has been conducted: six of the papers were conducted in this country. Four of the studies were conducted in Tanzania, three in Uganda, two in Mozambique, and one in the Democratic Republic of the Congo, Eswatini, Ethiopia, South Africa, and Zambia each. Table 1 outlines the major findings of each study.
Summary of Each Reviewed Study.
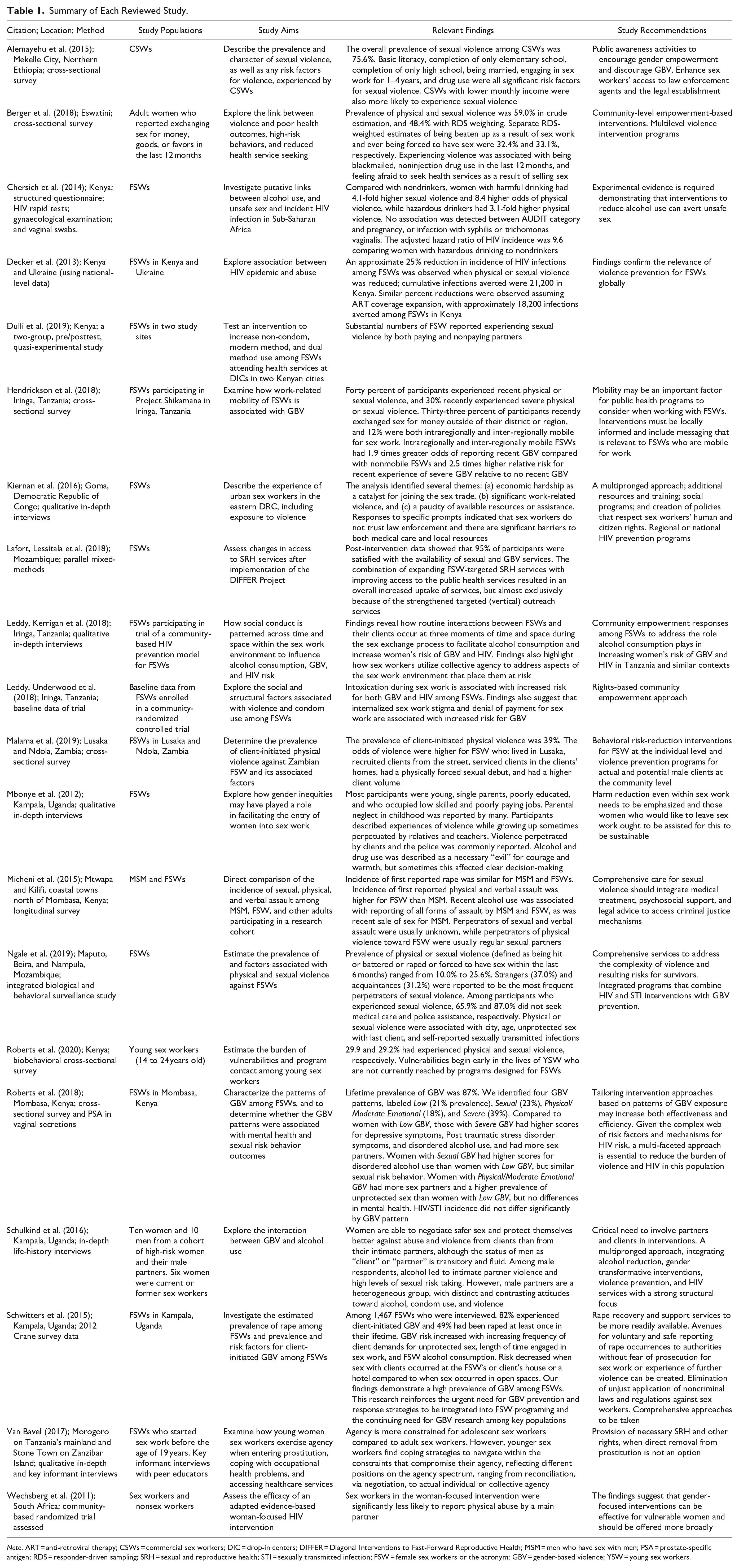
Note. ART = anti-retroviral therapy; CSWs = commercial sex workers; DIC = drop-in centers; DIFFER = Diagonal Interventions to Fast-Forward Reproductive Health; MSM = men who have sex with men; PSA = prostate-specific antigen; RDS = responder-driven sampling; SRH = sexual and reproductive health; STI = sexually transmitted infection; FSW = female sex workers or the acronym; GBV = gender-based violence; YSW = young sex workers.
WSS are known as a hard-to-reach population. Recruitment for studies consisted of accessing potential participants through outreach services, drop-in centers, their known places of business, or street outreach. Participants were located in cities in all but three studies (two studies were conducted in towns, one used national data, and one did not specify the location). Two of the studies (Roberts et al., 2020; Van Bavel, 2017) used young sex workers. One study (Hendrickson et al., 2018) included intra- or inter-regionally mobile WSS.
Prevalence
Measures and definitions of violence differ across the studies surveyed, which makes direct comparison across the studies difficult. Nevertheless, it is clear that WSS in the region experience high levels of violence, both as a result of their work, and in their lives in general, as illustrated in Table 2.
Prevalence, Incidence, and Perpetrators of Various Types of Violence.
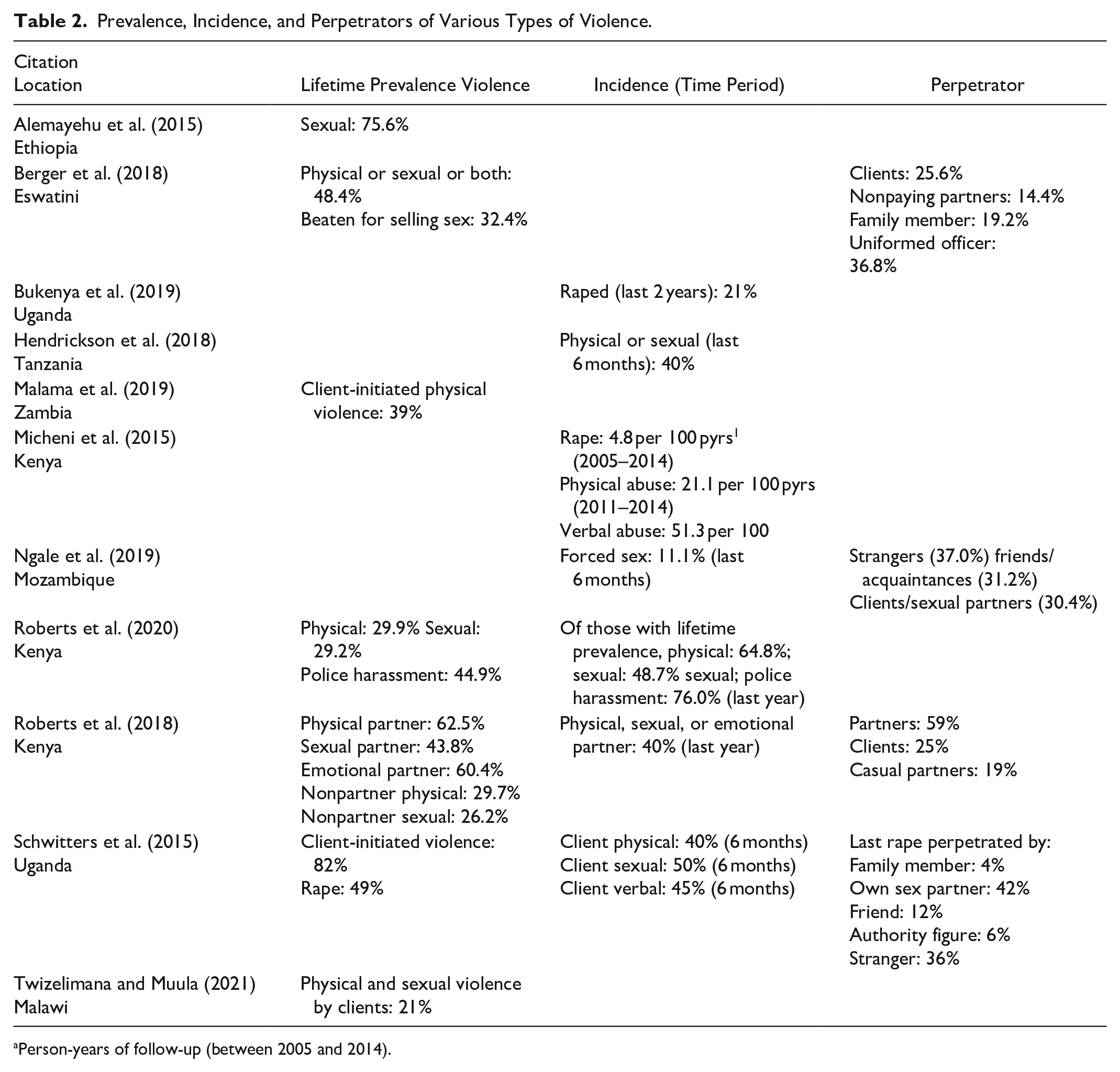
Person-years of follow-up (between 2005 and 2014).
The lowest lifetime prevalence of a particular form of violence reported in the studies was 21% and the highest was 82% (both for client-initiated violence). The lowest reported incidence of a particular form of violence was 11.1% (forced sex), and the highest was 76% (police harassment). Lifetime prevalence of sexual and physical violence was reported in one study (Berger et al., 2018) at 48.4%, and incidence in the last 6 months at 40% in another (Hendrickson et al., 2018).
Table 2 provides a picture of generalized violence toward WSS from a range of perpetrators: clients, nonpaying partners, family, friends/acquaintances, strangers, and authorities. While intimate partner violence in Sub-Saharan Africa, of which ESA is a part, is estimated to be high among the general population (Imasiku et al., 2017), WSS are faced additionally by violence from clients and authorities.
In a qualitative life-history study conducted in Uganda, Mbonye et al. (2012) suggest that violence is not new to WSS: Their participants described experiences of violence while growing up, sometimes perpetuated by relatives and teachers. While clients are a major source of violence, some women in Schulkind et al.’s (2016) Ugandan study reported being faced with abuse from managers. Sexual harassment and violence from the police (demanding bribes or sex) was said to be commonplace and taken as inevitable.
Factors Associated With Violence Against WSS
The factors associated with violence against WSS or that put WSS at greater risk of experiencing violence, as found in the reviewed studies, include: location, mobility, alcohol or substance use, particular sex exchange interactions, and various personal variables. These are discussed below.
The location or context within which sex work occurs is important in terms of violence. As pointed out by Schulkind et al. (2016), street-based WSS are generally perceived to be of lower social status and, hence, are at greater risk of violence and abuse. Informal security arrangements within lodges or bars offer some form of protection. Research in Zambia (Malama et al., 2019) confirms that recruiting clients from the streets is a risk factor for violence. Sex taking place in open spaces rather than houses or hotels (Schwitters et al., 2015), and sex occurring in clients’ homes (Malama et al., 2019) were found to be associated with violence. Malama et al.(2019) report that the odds of client-initiated physical violence were higher for Zambian WSS who lived in the capital of Lusaka than those living in the second largest city, Ndola. Ngale et al. (2019) also report that physical and sexual violence were associated with different locations, in this case various cities in Mozambique (Maputo, Beira, and Nampula).
Hendrickson et al. (2018) found that intra- and inter-regionally mobile sex workers had 1.9 times greater odds of reporting recent violence than nonmobile ones, particularly severe violence. This factor did not feature in other research reviewed, but is confirmed in the international review by Deering et al. (2014).
In a South African study on the effects of alcohol use on sexual behavior, Chersich et al. (2014) found that WSS who drank at hazardous or harmful levels (as per World Health Organization definitions) experienced higher levels of physical or sexual violence. These findings are also noted in two papers by Leddy, Kerrigan et al. (2018), and Leddy, Underwood et al. (2018) in Tanzania, by Schulkind et al. (2016) in Uganda, and by Micheni et al. (2015) in Kenya. These authors indicate that alcohol intoxication poses direct risks for violence through behavioral disinhibition, but also through the women’s misreading of the risks implicit in intimate contact with strangers. In a qualitative study conducted in Uganda (Mbonye et al., 2012), participants indicated that alcohol and drug use was a necessary “evil” for courage and warmth. Drug use was also found to be a factor (Alemayehu et al., 2015; Berger et al., 2018).
Various sex exchange interactions were associated with violence. These included the following: client demands for unprotected sex (Schwitters et al., 2015), denial of payment for sex or pay disputes (Leddy, Underwood, et al., 2018; Schulkind et al., 2016), and disputes between clients over “possession” of a woman who sells sex (Schulkind et al., 2016). In their Tanzanian study, Leddy, Kerrigan, et al. (2018) show that the routine interactions between clients and WSS in bars or lodges may exacerbate violence. These interactions occur at three moments of time and space: the bar/meeting space which sex workers use to attract clients, and in which clients purchase alcohol for the women to initiate the exchange of sex; the transition/negotiation space where clients may become violent if the woman refuses sex after consuming alcohol purchased by the client; the room/sex exchange space, in which the client may become violent if the woman changes her mind, may sexually abuse a woman too drunk to respond, and may refuse previously negotiated condom use.
Personal factors included the following: lower educational attainment (Alemayehu et al., 2015), being married (Alemayehu et al., 2015), being younger (Ngale et al., 2019; Van Bavel, 2017), lower monthly income (Alemayehu et al., 2015), self-reported STI (Ngale et al., 2019), having had a forced sexual debut (Malama et al., 2019), high client volume (Malama et al., 2019), and longer time engaged in sex work (Alemayehu et al., 2015; Schwitters et al., 2015). At a more subtle level, findings in a Tanzanian study (Leddy, Underwood, et al., 2018) suggest that internalized sex work stigma (“acceptance of the negative attitudes society holds about them” [p. 3298]) are associated with increased risk for violence. The authors conclude, “In contexts where sex work is criminalized and highly stigmatized, violence against FSWs is often a form of enacted sex work stigma, and regularly occurs with impunity” (p. 3303). Internalization of this stigma results in women remaining in abusive relationships. Finally, being blackmailed as a result of selling sex was found to be associated with violence (Berger et al., 2018).
Services and Interventions
The studies under review addressed the following in relation to services: lack of access to services, interventions to reduce violence, and agentic actions taken by WSS that could be used in interventions. A number of papers refer to interventions that address violence against WSS as part of a program mix. Some, however, do not report on the effects of the interventions on violence per se (e.g., Dulli et al., 2019; Mbita et al., 2020).
Concern was expressed by researchers about WSS not accessing services post violence. Of participants in a Mozambiquan study (Ngale et al., 2019) who experienced sexual violence, 65.9% did not seek medical care, and 87.0% did not seek police assistance. Kiernan et al. (2016), in their Ugandan study (Goma), show, “As law enforcement in the area remains ineffective, and the medical care inaccessible, sex workers have few means to manage the hazards of their work” (p. 244). Schwitters et al (2015) argue that there are few avenues for voluntary and safe reporting of rape occurrences to authorities without fear of prosecution for sex work or experience of further violence.
Wechsberg et al. (2011) conducted a randomized trial to assess the efficacy of an adapted woman-focused HIV intervention in addressing HIV, substance use, and GBV among WSS and women in general in South Africa. The adapted woman-focused intervention is an empowerment-based two-session HIV intervention that aims to increase knowledge about alcohol and other drug use associated with sex risk and GBV, increase personal power by reducing substance use, increase communication skills with partners as well as condom use competency, and teach specific violence prevention strategies. WSS who participated in the program were significantly less likely to report physical abuse by a main partner and their clients than those who did not.
Lafort, Lessitala, et al. (2018) report on the Diagonal Interventions to Fast-Forward Reproductive Health. This project developed, piloted, and tested diagonal models to improve uptake of SRH services by WSS in four cities: Mysore, India; Mombasa, Kenya; Durban, South Africa; and Tete, Mozambique. Key components are (a) strengthening targeted services, (b) improving access to the general health services, and (c) creating better linkages between interventions targeted at WSS and the general health services. The project started with a detailed situation and policy analysis, which allowed for the development of context-specific interventions in each city. Post-intervention data showed the 95% of participants were satisfied with the availability of sexual and GBV services.
Paying attention to strategies already used by WSS may prove useful in programs. Findings from the study by Leddy, Kerrigan, et al. (2018) highlight how sex workers may utilize collective agency to address aspects of the sex work environment that place them at risk of alcohol abuse, violence, and HIV. For example, sex workers spoke about covering shifts for intoxicated colleagues or taking them home, paying back money to clients for drinks, disguising water in beer bottles so as to avoid drinking alcohol, yelling, screaming, or using whistles for colleagues when experiencing violence in private rooms.
Discussion
A picture of generalized violence against WSS in ESA countries, perpetrated by a range of people, emerged in the studies reviewed. Factors associated with such violence included context, alcohol use, sex exchange interactions, and a number of personal variables. These risk factors as similar to the ones found in Deering et al.’s (2014) review of international literature. Services in the ESA region are minimal and WSS seldom access them after violence. Table 3 outlines the key findings of this review.
Critical Findings.
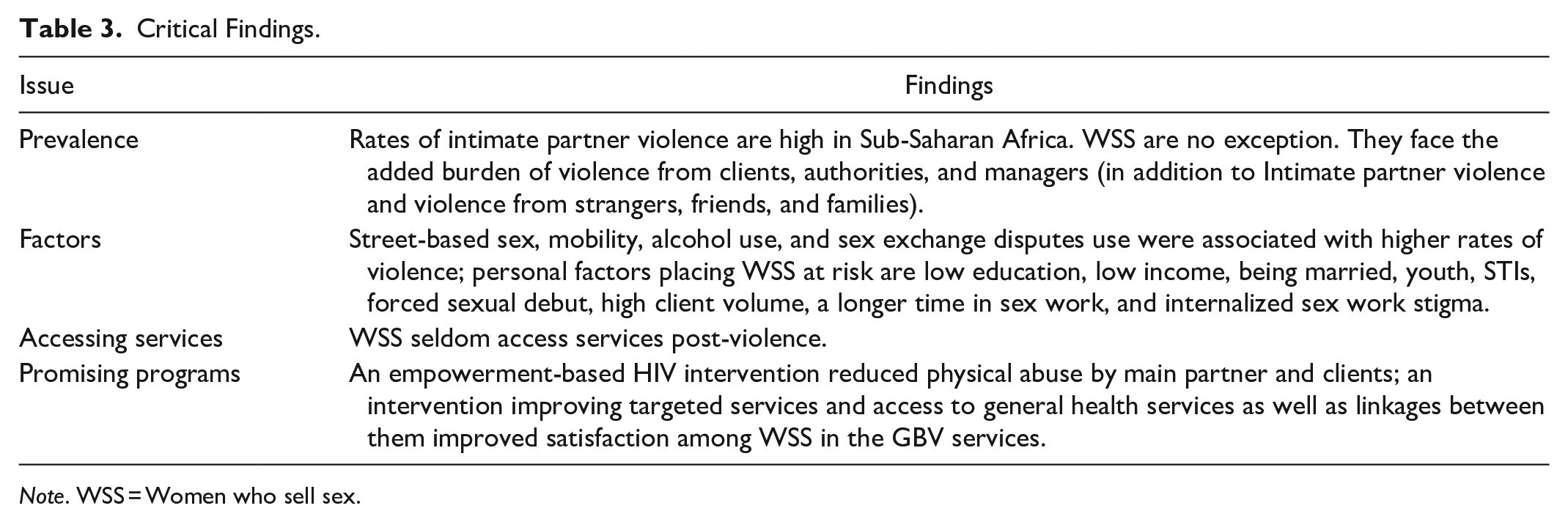
Note. WSS = Women who sell sex.
Two programs were reported as having positive effects in reducing abuse and improving satisfaction with services related to violence (Lafort, Lessitala, et al., 2018; Wechsberg et al., 2011). Importantly, one study showed ways in which WSS form a collective agency to reduce violence (Leddy, Kerrigan, et al., 2018).
These findings have implications for practice, policy, and research, as outlined in Table 4. Programs for WSS should include both targeted services and improvements in general services, address risk reduction, and include relevant messaging. Equally important are interventions aimed at actual or potential clients. Policies should improve the access WSS have to the policing and legal system. Evaluative research and research in more ESA countries are needed.
Implications for Policy, Practice, and Research.
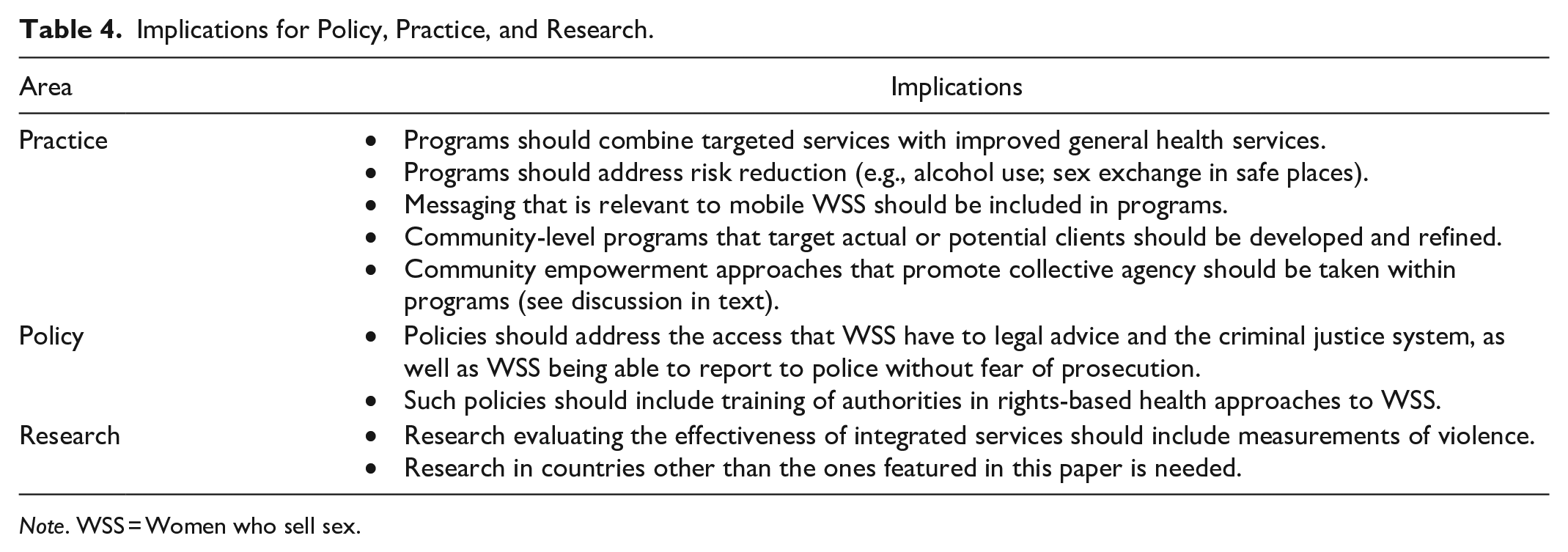
Note. WSS = Women who sell sex.
We argue that the findings of WSS demonstrating collective agency, together with evidence of what worked in programs, need the most attention in reducing violence against WSS in the region. Collective agency approaches have shown promise in India, as outlined by Dasgupta (2020), who discusses the Sonagachi Project. In addition to targeted goals (e.g., reduction of sexually transmitted infections), the project focused on unionization of the sex workers, establishing microcredit societies, and vocational training. A decade after the initiation of the project, sex workers indicated that violence had decreased substantially. They outlined the following multilayered strategy to reduce violence: unionization and formation of a collective platform for voicing common concerns; identification of stakeholders and stakeholder negotiation, including pimps, clients, law enforcement agencies, and members of political parties; and mutual transmission of knowledge through the peer education process (as a result of distrust of expert intervention).
These kinds of programs that draw on an already existing collective agency may hold promise in the ESA region. Indeed, as pointed out by Van Bavel (2017), in their study on how young WSS exercise agency, “The respondents on Zanzibar, who could rely on sensitisation and outreach by an empowering organization and on peer networks, demonstrated more agency than their peers in Morogoro, for whom these benefits were unavailable, suggesting that collective agency indeed offers a way to cope with structural constraints and to challenge unequal power relations” (p. 84).
Strengths and Limitations
Because WSS are a hard-to-reach population, samples may not reflect the general population of WSS. While samples were diverse across the papers reviewed, including urban based WSS, mobile WSS, and younger WSS, WSS living in rural areas were not included. Some studies in the region address rural-based WSS (e.g., Afzal et al., 2020), but these do not address violence. This limits diversity across the review, and hence the generalizability of the findings in relation to WSS in rural areas.
While the fact that the studies were conducted in diverse countries is a strength, caution should be taken in applying the findings across all countries in the region. This is exacerbated by the fact that no studies in French or Portuguese were surfaced. French is an official language in six of the ESA countries and Portuguese in two of them.
Nevertheless, this scoping review brings together current knowledge about violence perpetrated against WSS in the ESA region. It points to the extent of the problem, various factors associated with the violence, and promising interventions. This consolidation of current knowledge can be used by NGOs and health services in planning programs and supporting WSS.
Conclusion
This scoping review confirmed, in line with international literature, that WSS in ESA face high levels of violence from a range of perpetrators. While these findings should be viewed in the context of GBV experienced by the general population of women in the region, WSS are at an increased risk for violence from the authorities and managers and in their workplace—particularly if the sex exchange occurs in public spaces and client recruitment happens in the street. WSS who are already marginalized through lack of education and income are at higher risk of violence. Violence increases, unsurprisingly, with a higher volume of clients and a longer time in sex work. Mobility, alcohol use, being married or younger, having an STI, and forced sexual debut are also associated with violence. The fact that internalized sex work stigma is a risk factor for violence points to the compound effects of sexual violence and discriminatory practices.
This paper provides additional evidence-based support for making violence against WSS a public health and human rights priority, as called for by other researchers (Deering et al., 2014). The need for interventions to respond to the contextual factors shaping violence against WSS is clear and should include decriminalization and supportive policing practices. As WSS seldom access services after experiencing violence, it is crucial that targeted services are developed and maintained, and that they focus on empowerment. This, however, must be accompanied by the strengthening of general health services, police responses, and legal avenues open to WSS. The promotion of collective agency among WSS holds promise. Interventions focussing on actual or potential clients are also needed.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is based on research supported by the UNFPA’s 2gether 4 SRHR programme in ESA, and the South African Research Chairs initiative of the Department of Science and Technology and National Research Foundation of South Africa (grant no. 87582).