
Abstract
We undertook a scoping review of published research literature that reported on adult sexual assault patients’ experience of the physical examination component of the medical forensic examination (MFE). Eligible papers were those reporting data about the physical examination component of the MFE from the adult patient’s perspective, published in the period January 2000 to March 2022 in peer reviewed journals and reports containing original research data published from a tertiary institution. Twelve papers were identified. The review identified a gap in the literature regarding the patient’s experience of the physical examination component of the MFE. The existing literature is limited but suggests that some patients find the examination empowering and reassuring, restoring a sense of bodily control; however, for others it is an intrusive, violating experience that they endure. A more patient-centered sexual assault service appears to have a therapeutic value in itself, but more research is warranted as existing research is very limited and often from a proxy. In particular, more research on patients’ self-reported experience of the MFE, including specific aspects of the examination and the experience of male and gender nonconforming victim-survivors, is needed. A better understanding, from the point of view of the patient, of the benefits of attending, may encourage victim-survivors to seek a health response and, possibly, report to police. It may also be time to assess the impacts of certain aspects of the forensic examination, rethink standard evidence collection processes, and consider enabling more acceptable options for victim-survivors including self-collection of intimate samples.
Keywords
Background
Many countries now provide specialized multidisciplinary services for victim-survivors following sexual assault (Eogan et al., 2013; Greeson & Campbell, 2013; NSW Government, 2020; The Royal College of Emergency Medicine UK, 2015; Welch & Mason, 2007; Zijlstra et al., 2017). The medical forensic consultation offered to victim-survivors of sexual assault by these specialized, integrated, multidisciplinary services is multifaceted and is guided by patient choice and assault characteristics. This medical forensic consultation typically includes immediate psychosocial support and an assessment of health needs depending on the individual patient (assessment and management of injuries, pregnancy risk, and sexually transmissible infection [STI] risk). It also includes the offer of forensic documentation and evidence collection for potential use in criminal proceedings, guided by a history of the assault (Mein et al., 2003). The forensic examination (MFE) and evidence collection component is commonly labeled as “the rape kit” and often portrayed erroneously in the media and popular crime series (Hust et al., 2015) as a stand-alone examination under police supervision (Alptraum, 2020) instead of being part of a more holistic medical consultation. There is literature to support the benefits of the integrated, multidisciplinary approach that has become more widely adopted (Caswell et al., 2019; Du Mont et al., 2014; Ericksen et al., 2002; Martin et al., 2007). Increasingly victim-survivors’ experience is being explored. This scoping review sought to ascertain what research data is available from victim-survivors on their experience of the physical components of the MFE; for example, the taking of forensic samples, physical examination practices, and what can be done to minimize retraumatization. Better understanding of the experience of patients who seek a healthcare response after sexual assault can help to inform services to be more helpful and encourage victim-survivors to seek help, manage the impacts of sexual assault, and support reporting.
The forensic examination is usually comprehensive and includes a “top to toe” examination including an anogenital examination and can include collection of blood and urine samples, mouth swab and rinse, anal swabs (sometimes aided by an anoscope 1 ) and external and internal vulvo-vaginal swabs (often aided by a speculum 2 ), or penile swabs (in the case of a male victim-survivor) and other skin swabs to detect possible DNA evidence. Injuries may be photographed, and items of clothing may be collected, including underwear, and possibly other samples such as fingernail scrapings or clippings, hair, or foreign material such as vegetation. Urine can sometimes be processed for DNA evidence but is often only used for toxicology purposes, when appropriate, as is the blood sample.
Most published research on the immediate care of sexually assaulted adults has focused on services in North America (Campbell, 2006; Campbell et al., 2006, 2020; Du Mont et al., 2008, 2013, 2014; Ericksen et al., 2002; Fehler-Cabral et al., 2011; Lewis-O’Connor & Chadwick, 2015) and a small body of research in the United Kingdom (Kumari et al., 2019; Walker et al., 2020), other European countries (Denis et al., 2018; Gilles et al., 2019; Hagemann et al., 2011, 2013, 2014), Australia (Astbury, 2006; Lievore, 2005), and New Zealand (Jordan, 2001). Understandably, the vast majority of study subjects have been female. This research has informed clinical practice to be more patient-focused (Alpert, 2018; Campbell et al., 2006; Lewis-O’Connor & Chadwick, 2015; McGregor et al., 2009). By providing specialized and integrated multidisciplinary sexual assault services to patients, there have been significant improvements in patient-centered care in the last two decades compared to the traditional police-facilitated emergency department response from busy doctors with mixed and urgent caseloads (Campbell et al., 2006; Campbell, Adams & Patterson, 2008). However, there are differences in service provision in different settings. Research by Campbell et al. in the United States investigating the patient experience of nonspecialized services reported secondary victimization that left most women feeling “bad about themselves, depressed, guilty, anxious, violated, disappointed, distrustful of others and reluctant to seek further help” after their contact with the medical system (Campbell, 2005). In another paper by the same author, “Preventing the ‘Second Rape’: Rape Survivors’ Experiences With Community Service Providers,” Campbell notes that those who felt most victimized by the medical service were not necessarily those who received a forensic examination, but rather those who did not receive the holistic medical care they expected such as emergency contraception or STI risk assessment (Campbell et al., 2001). Campbell’s later research on the psychological recovery of sexual assault patients found that victims’ recoveries were facilitated when they were supported to access the services they need. However, when this did not happen “system personnel can magnify victims’ feelings of powerlessness, shame, and guilt” (Campbell, 2008). This can lead to reluctance to engage further with health and criminal justice systems (Fehler-Cabral et al., 2011).
Much has been learned over the past two decades by investigating patient experiences of sexual assault medical forensic services. This has resulted in better understanding of the components of patient-centered (McGregor et al., 2009), trauma-informed care (Lewis-O’Connor & Chadwick, 2015) in the context of a sexual assault presentation. Evidence from prior research suggests empowering patients can lead to positive psychological outcomes (Campbell, Patterson, Adams, Deigel & Coats, 2008), high levels of satisfaction with sexual assault services (Du Mont et al., 2008) and, for some, encourage further engagement with criminal justice processes (Fehler-Cabral et al., 2011). There is evidence of the important role of the MFE in this empowerment and increased criminal justice participation (Fehler-Cabral et al., 2011). This is despite the fact that evidence collected from the MFE often does not lead to successful legal outcomes (Du Mont & Parnis, 2000; Du Mont & White, 2007), particularly when the defense rests on the sexual intercourse being consensual (Alderden et al., 2021). Indeed, the detection of sperm is not associated with conviction (Du Mont & White, 2007; Ingemann-Hansen et al., 2008). However, there is also evidence that having a forensic examination is regarded favorably in legal processes that view the “true” rape victim as one who will participate in a forensic examination and for those who do, it is more likely that their case will proceed through the criminal justice system from police reporting to court (Alderden et al., 2021).
There are many reasons why victims have an MFE including a desire for criminal justice, a duty to prevent sexual assault from happening to others by the same perpetrator, to validate their claims of victimization, to find out what happened, to access healthcare and due to pressure from family, friends, police, and healthcare providers (Campbell et al., 2020; Du Mont et al., 2008). Victims who receive a forensic examination might access services primarily for a healthcare response, not a criminal justice one but believe they have to participate in the forensic examination to obtain the care they need (Du Mont et al., 2008). There is some evidence to support the view that the physical examination itself may be reassuring and empowering when provided in a multidisciplinary service with patient choice, support, and explanation (Du Mont et al., 2008; Ericksen et al., 2002); however, the physical examination may still be experienced as retraumatizing, invasive, humiliating, and distressing (Du Mont et al., 2008; Greeson & Campbell, 2011), and some may regret undergoing such an examination (Lewis-O’Connor & Chadwick, 2015). A recently published U.S. study, in which sexual assault nurse examiners (SANEs) reported on patient decision-making (not the patients reporting themselves), found that although the vast majority of patients agreed to all components of an MFE, 19% declined at least one aspect of the examination. Of those women, one-half declined the speculum examination, one-third declined forensic photography, and one-quarter declined the anogenital examination (Campbell et al., 2021). It would be useful to know why so that this can be evaluated and addressed.
There seems to have been little research focus on the experience of the physical procedures to which patients are subjected as part of the integrated response to sexual assault. Do patients feel reassured and empowered by having a thorough examination and forensic collection or is this retraumatizing? Do we need to re-evaluate the necessity of a thorough MFE for acute presentations? It is critical to better understand how patients view different parts of the examination to guide service delivery and assist forensic medical examiners in gaining accurately informed patient consent to the examination.
This scoping review aimed to examine the existing published research specifically on the physical examination component of the medical-forensic service from the point of view of the adult patient. The review sought to identify if there is a gap in the research on this aspect of care after sexual assault, from the perspective of victim-survivors and what, if any, research exists where those of marginalized gender and sexualities, and men, are the victim survivors.
Methodology
A scoping review of the literature was performed to identify knowledge gaps in published research regarding the physical component of evidence collection during the MFE of adult (over 18 years old) patients who have been recently sexually assaulted.
What Is a “Scoping Review”?
According to Arksey and O’Malley, the scoping review is a technique to “map” relevant literature in the field of interest. A scoping review can provide a narrative or descriptive account of available research and can identify research gaps (Arksey & O’Malley, 2005). Arksey and O’Malley identify five steps in the scoping review: Stage 1: identifying the research question; Stage 2: identifying relevant studies; Stage 3: study selection; Stage 4: charting the data; and Stage 5: collating, summarizing, and reporting the results. They explain that this process not only allows for identification of gaps in the evidence base but also allows for an accessible summary to disseminate research findings to policy makers, practitioners, and consumers. A scoping review does not aim to analyze the quality or relevant weight of interventions. A scoping review typically synthesizes data in tabular form with some narrative commentary and characterizes the literature by study design and other key features (Grant & Booth, 2009).
Research Question
The research question for this scoping review was: “In adult patients who present after a sexual assault for an acute medical forensic response, what evidence do we have from the patients as research subjects about their experience of the physical examination component of the medical forensic examination?”
Search Strategy
The search strategy identified relevant literature by utilizing the first author’s (Dr Stewart) existing Endnote library collated over 10 years through her research and professional work as a medical forensic examiner and educator and by Dr Stewart performing a comprehensive Library Search, 3 searching online databases on the patient experience of the MFE after sexual assault, online journals, references from identified papers, papers citing identified papers, papers by the same author as identified papers, online libraries of organizations working in the field of sexual violence, online researcher networks, and Google Scholar. Additionally, an academic librarian ran a search through Scopus and Ovid Medline using the search terms (“forensic medical exam*” OR forensic* OR “Medical System*”) and (rape OR raped OR raping OR rapes OR “second rape” OR “sexual violenc*” OR “Sexual assault*” OR “Sexual crime*” OR “Sex offense*”) and (victim* OR survivo?rs* OR patient*). The same search terms were used in the PsycINFO database to identify any further papers.
Eligible papers were those reporting data about the physical component of the MFE from the adult (>18 years) patient’s perspective, published from January 2000 until March 2022 in peer-reviewed journals. A decision was made to include a government-funded report containing original research data as it was published by authors from a tertiary institution and was assessed by the four authors as being of equivalent quality to a peer-reviewed publication. Papers published prior to 2000 were excluded so that the search was limited to papers reporting recent or current practices.
Dr Stewart identified 231 relevant papers published from 2000 of the adult patient’s experience after sexual assault. Of those studies Dr Stewart excluded 185 papers that were reviews or opinion pieces and studies that explored patient experiences after a sexual assault from a proxy (e.g., a healthcare provider) rather than the patient directly. This resulted in 46 papers. Dr Stewart then limited the remaining papers, which reported directly from patients, to only those in acute sexual assault settings that offer a medical forensic response (32 papers). Dr Stewart then further explored the remaining papers to identify any existing research knowledge specifically on the physical examination. Papers were excluded that provided no data on the physical examination. Three studies that used duplicate datasets to other papers, and did not add any new data, were also excluded (Campbell, 2005; Campbell, Patterson, Adams, Deigel & Coats, 2008; Greeson, 2009). One was a published thesis (Greeson, 2009) that resulted in a peer-reviewed paper that was included (Greeson & Campbell, 2011)). This review process was supervised by the other three authors, one of whom also reviewed all the papers, the other two reviewed papers where there was a question regarding inclusion, such as the report that was not published in a peer-reviewed journal and those with duplicate data (See Figure 1. Flowchart for selection of eligible research articles).
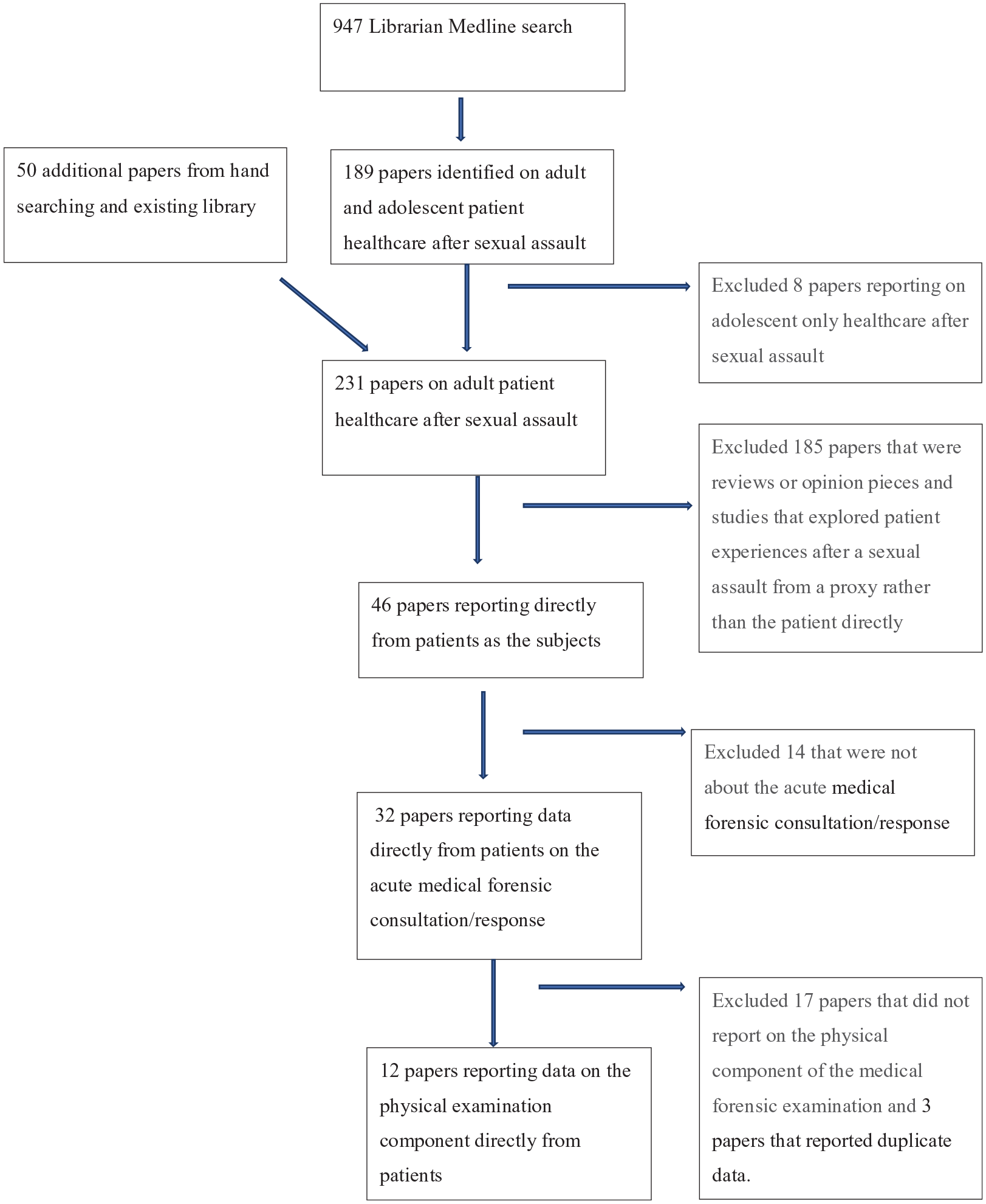
Flowchart for selection of eligible research articles.
Results
Only twelve papers (Campbell, 2006; Campbell, Patterson, Adams, Deigel & Coats, 2008; Du Mont et al., 2008; Ericksen et al., 2002; Fehler-Cabral et al., 2011; Greeson & Campbell, 2011; Jordan, 2001; Lovett et al., 2004; Majeed-Ariss et al., 2019; Miyamoto et al., 2021; Nittis & Hughes, 2021; Peeters et al., 2019) were identified as having relevant data from patients themselves on their experiences of the physical component of the MFE. Of these only two (Du Mont et al., 2008; Fehler-Cabral et al., 2011) were specifically designed to explore the experience of the MFE after sexual assault, a further five papers (Campbell, Patterson, Adams, Deigel & Coats, 2008; Ericksen et al., 2002; Jordan, 2001; Lovett et al., 2004; Nittis & Hughes, 2021) had relevant data collected as part of a broader research project and five of the papers had very limited, but still relevant, data reporting on the physical component of the MFE (Campbell, 2006; Greeson & Campbell, 2011; Majeed-Ariss et al., 2019; Miyamoto et al., 2021; Peeters et al., 2019).
Only four of the papers included men as participants (and there were only small numbers in comparison to women participants in those studies) (Lovett et al., 2004; Majeed-Ariss et al., 2019; Miyamoto et al., 2021; Peeters et al., 2019) and only one paper had any representation from participants identifying as nonbinary (Miyamoto et al., 2021). There is no indication in any of the papers of the participants’ sexuality except that one quoted interview subject, in the report by Lovett et al., is referred to as a gay man.
None of the research studies focused specifically on particular aspects of the examination, such as the use of the speculum or anoscope, surrendering underwear and the taking of swabs, blood tests, and urine samples. We have, however, included one paper that focused specifically on forensic photography and its acceptability (Nittis & Hughes, 2021).
With regard to methodology, five papers utilized semi-structured interviews (Du Mont et al., 2008; Ericksen et al., 2002; Fehler-Cabral et al., 2011; Greeson & Campbell, 2011; Jordan, 2001), one used a verbal checklist (Campbell, 2006), one a face-to-face survey (Campbell, Patterson, Adams, Deigel & Coats, 2008), one used a paper survey (Majeed-Ariss et al., 2019), and two used an electronic and/or paper survey (Miyamoto et al., 2021; Nittis & Hughes, 2021). Two studies utilized both a series of questionnaires and in-depth interviews (Lovett et al., 2004; Peeters et al., 2019). Details from the twelve papers were charted in an Excel sheet and then tabulated (see Table 1). Two of the included papers (Fehler-Cabral et al., 2011; Greeson & Campbell, 2011) reported on data derived from the same sample of women who were subjects of a larger, separate project (Campbell et al., 2009).
Studies Included and Critical Findings.
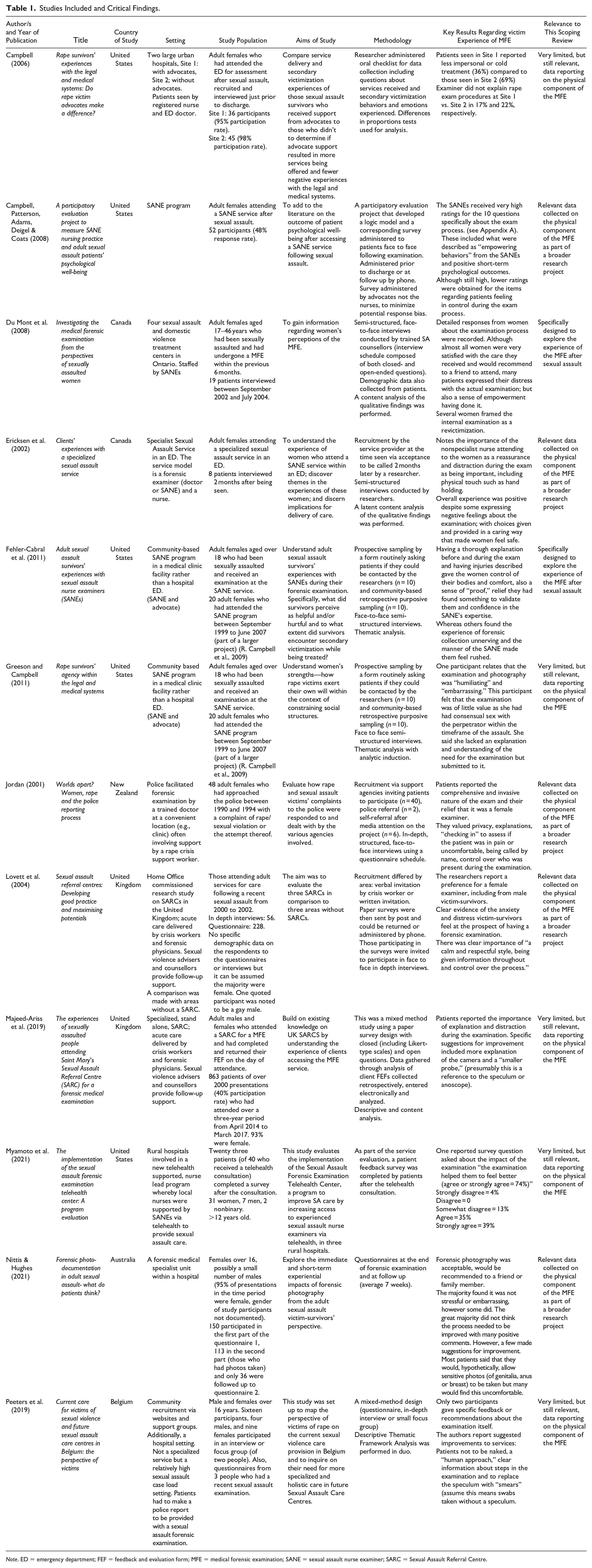
Note. ED = emergency department; FEF = feedback and evaluation form; MFE = medical forensic examination; SANE = sexual assault nurse examiner; SARC = Sexual Assault Referral Centre.
An overview of the main findings reported in the studies, including detailed results, and the researchers’ recommendations are discussed. We have grouped the findings under relevant headings (drawn from the studies) to help with synthesis of the findings.
Explanations
The importance of offering and/or providing “explanations” to patients before examination, during examination, of photography, and of injuries was a common theme (Campbell, 2006; Campbell, Patterson, Adams, Deigel & Coats, 2008; Fehler-Cabral et al., 2011; Greeson & Campbell, 2011; Jordan, 2001; Lovett et al., 2004; Majeed-Ariss et al., 2019; Peeters et al., 2019). Lovett et al.’s research indicated that the Sexual Assault Referral Centre (SARC) patients were more likely to report that having the examination explained to them made it less traumatic, compared to the comparison areas without an integrated specialist service. One of the SARC patients stated, “because of the way the doctor handled me and explained I didn’t find it traumatic.” The patients appreciated having step-by-step details of components of the examination explained such as having swabs taken (Lovett et al., 2004).
When the forensic examiner explained that injuries had been identified, some patients reported being relieved that their situation was validated, the value of “proof” was seen as a positive outcome and receiving feedback from the examination gave some women a sense of bodily control (Fehler-Cabral et al., 2011). Explanation during the examination and “checking in” to assess if patients were uncomfortable or in pain was reported as being valuable and gave some patients a sense of safety (Jordan, 2001). In Campbell et al.’s paper on an evaluation project of a specialized service of SANEs, the authors found that all 52 patients surveyed agreed that they felt completely informed about what was happening during the examination and all agreed that the nurses showed “a lot” of “care and compassion” (Campbell, Patterson, Adams, Deigel & Coats, 2008).
Some patients noted the importance of the examination as a way of explaining or validating what had happened during the assault (Fehler-Cabral et al., 2011) with an expectation that the examination findings would subsequently be discussed with them.
Professionalism
Some patients valued the expertise and professionalism (Fehler-Cabral et al., 2011; Lovett et al., 2004) of the examiner and support personnel during the examination and it was important that this was exhibited in a warm and caring manner (Ericksen et al., 2002; Jordan, 2001).
She was lovely, she was really, really nice. I’m not quite sure how long it lasted, it was quite a long time, it was about an hour, but she was very professional and considerate, throughout . . . But her approach made a big difference to me. (Lovett et al., 2004)
When the examiner was perceived to be too “business like,” rushed or cold patients found it a more negative experience (Campbell, 2006; Fehler-Cabral et al., 2011; Lovett et al., 2004).
I would say more like the evidence collection. It was, you know . . . She got all her stuff out, and you know, it was really pretty bizarre. I’ve never been through anything like that in my life . . . And so, it was more of a business type thing, you know, like, and she was trying to hurry and get me out of there, too, so . . . Yeah. She wasn’t rude about it. She was just trying to get it done. (Fehler-Cabral et al., 2011)
Similarly, one of the patients seen in a non-integrated service, where forensic examiners are not part of a dedicated team felt that the examiner was rushed and unsympathetic and hence found the examination difficult, He could have been a lot gentler over it. I know they’re rushed, I know they’re busy, and they’re understaffed and overworked, but he knew the circumstances. And he didn’t make any allowances for it whatsoever . . . (Lovett et al., 2004)
Reassurance and Distraction
Reassurance and distraction (Ericksen et al., 2002; Majeed-Ariss et al., 2019) during the physical examination gave some patients a sense of safety and calm but this didn’t necessarily mean that patients felt the experience was not challenging. Rather, for some patients, despite the examination, they felt safe and cared for (Ericksen et al., 2002). Patients appreciated literal “hand holding” (Ericksen et al., 2002) and the use of their own name (Jordan, 2001). There was “relief” for some that the examiner was a woman (Ericksen et al., 2002; Jordan, 2001; Lovett et al., 2004), 4 even though some of the patients interviewed by Lovett et al. noted that a calm, gentle, and respectful style was more important than the gender of the examiner.
In the paper by Ericksen et al., the researchers report on the importance of reassuring “touch” during the examination; being consoling, and nurturing. One participant stated: They had to do some of the physical examination—and having somebody else inside of me that was horrible, and you know, while she was doing that (the nurse) was holding my hand and making me feel at ease as much as possible. (Ericksen et al., 2002)
Choice and Control
Having a choice about who was present for support during the examination gave some patients a sense of control (Jordan, 2001) as did feedback during the examination (Fehler-Cabral et al., 2011). Being told what was happening and being allowed to manage the pace of the examination gave some patients a sense of choice and control (Campbell et al., 2013; Ericksen et al., 2002; Lovett et al., 2004). Campbell et al.’s paper reported on a checklist of empowering behaviors that the SANE service had identified as being important including helping with the examination if they wanted to, and/or taking a break or saying no at any time (see Appendix A for a list of these behaviors). A large majority of patients agreed that the SANEs engaged in these behaviors “the whole time” throughout the exam process. Although the SANE service is rated highly in all areas, one of the areas that is rated lower than others was how much control patients felt they had during the examination (Campbell, Patterson, Adams, Deigel & Coats, 2008). A perception of being in control was seen as important but not all patients felt they were allowed this during the examination itself (Campbell, Patterson, Adams, Deigel & Coats, 2008; Fehler-Cabral et al., 2011). Some patients refused certain aspects of the examination (blood taking, photography, and internal swabs for semen, especially anal swabs) while others regretted having them (Du Mont et al., 2008). Fehler-Cabral et al. summarized their results into aspects of care that were “helpful” or “harmful” and noted that those who found the process helpful “were provided a clear and thorough explanation of the exam process and findings . . . (and) . . . they were given choices during the exam.” They were given choice about whether to continue with, and certain aspects of, the examination. Having such control over the examination was believed to be a fundamental component of healing following their experience of an assault (Fehler-Cabral et al., 2011). Similarly, Lovett et al. found having the examination process explained step by step, being able to stop at any point and feeling in control emerged as an important factor in making the examination less traumatic as one of the SARC patients described, The doctor was really nice. And then she also asked me was it all right if she did this, she told me everything before she was going to do it, every single thing, even down to “This swab now, I’m going to take a swab of the bruising that’s, you know, inside,” etc. Yeah, before she did anything she explained to me and shown me what was going to happen. (Lovett et al., 2004)
Patients expressed a sense of empowerment by undergoing the examination. Some of Du Mont’s interviewees commented that they felt, “more in control,” “more powerful,” and actively “doing something.” One stated it was “something [she] had to do for [herself].” (Du Mont et al., 2008)
Another said: It kind of made me feel like it was all about me. It wasn’t about prosecuting somebody in the future, maybe it did have something to do with that, but I just felt good about doing something. Doing [the Kit] gave me more clarity, it helped take back my power [and] ease the emotions I was feeling. (Du Mont et al., 2008)
Some of Fehler-Cabral’s research participants also expressed a sense of having to endure the exam which was made easier by knowing what was happening: It is really uncomfortable to begin with, especially after what happened and I’d rather know what they are doing and why they are doing it, then you know . . . I thought more informed of what was going on. I didn’t feel so like I was in the dark about everything, you know. (Fehler-Cabral et al., 2011)
Fehler-Cabral and colleagues interpreted their findings as revealing that the examination itself was restorative for victims because they have control over, and consent to, being examined in a respectful way after an assault that had taken away their control. They postulated that “this ‘humanizing’ experience seemed to be instrumental in facilitating the victim’s recovery” (Fehler-Cabral et al., 2011).
Similarly, one of the patients in Majeed-Ariss’ patient survey voiced how the positive experience of the forensic examination in some ways countered the negative experience of the sexual assault, I would just like to say, that following on from such a traumatic experience, I have now experienced, a caring, helpful, meaningful experience. (Majeed-Ariss et al., 2019)
Further one paper also reported that 74% of patients agreed the examination “helped them feel better,” although 4% strongly disagreed (Miyamoto et al., 2021).
On Photography
One recent paper has reported on the patient acceptability of the use of photography during the medical forensic examination after sexual assault (Nittis & Hughes, 2021). As discussed in the paper, photography is not always a component of the forensic examination of adults, and there are perceived concerns about the impact on victim-survivors. The authors found that photography was acceptable, and that the majority found it was not stressful (54.6% said it was not stressful at all, 25% said it had been a little stressful, 10.2% were not sure, 6.5% thought the process was quite stressful, and 3.7% extremely stressful) and not embarrassing (59% said it was not embarrassing, 21% it was a little embarrassing, 6% quite embarrassing, 3% extremely embarrassing, and 11% said “don’t know”). However, some felt otherwise. The great majority (96.3%) did not think there was anything that the examiner might have done to make the process more pleasant or less stressful with many positive comments such as, She was very respectful – felt reassured, asks repeatedly, informed I can change my mind.
However, a few made suggestions for improvement such as avoiding photos of the face, having a female examiner, and communicating better. Most patients said that they would, hypothetically, allow sensitive photos (of genitalia, anus, or breast) to be taken but many indicated that they would find this uncomfortable.
A Negative Experience
The examination was definitely viewed as a negative experience by many but with acknowledged benefits for some. It was described as “distressing” but empowering (Du Mont et al., 2008), “horrible” but reassuring (Ericksen et al., 2002), “degrading” but “no more degrading than a cancer smear.” That same patient described how comprehensive the examination was: “she took everything, it was really gung-ho” (Jordan, 2001). Others also described the examination as comprehensive and invasive (Jordan, 2001). Some were clearly re-traumatized by the examination calling it a “bad experience that reminds you of the thing that happened” (Du Mont et al., 2008), and the examination and photography as “embarrassing” and “humiliating” (Greeson & Campbell, 2011) and “very uncomfortable, very degrading” (Fehler-Cabral et al., 2011). The patients interviewed for Du Mont’s research were generally very satisfied with the care they received and would recommend others attend the service; however, they still found the actual examination difficult and described feeling “scared,” “upset,” “stressed,” “nervous,” “embarrassed,” “angry,” “very exposed, very vulnerable, uncomfortable,” “horrible,” “violated,” and it being “traumatising” (Du Mont et al., 2008).
Certain aspects of the examination such as the drawing of blood and the vaginal examination were noted by Du Mont et al. to be particularly upsetting (Du Mont et al., 2008).
Du Mont’s research was one of only three studies (Du Mont et al., 2008; Ericksen et al., 2002; Lovett et al., 2004) that specifically reported on the internal examination and the negative impact it had. Du Mont quoted two patients who referred to the vaginal examination itself, She tried about three times [to insert a speculum], and I really didn’t want to do that at the time, ’cause I think I was reliving the whole experience and just wanted to put my clothes on after a while. (Du Mont et al., 2008) You feel like a piece of crap. I felt violated. Sitting naked on a table with your legs spread, and someone in between your legs, and you’re just like “what the hell this isn’t right” it was hell. I didn’t deserve to be put through that. And the last thing I wanted is to be violated, sitting in a room half-naked having blood-work done and being touched. (Du Mont et al., 2008)
Having a female examiner did not guarantee a sensitive examination, as Lovett et al. documented, I felt with it being a female, she would have been more sensitive to the way I felt. But she were rough, she were very rough. You know, like when they do the swabs, they were more or less shoved in rather than, you know, gently put in . . . She should have talked first and gone into detail [about] what they have to do, and been a lot more sensitive to the person. (Lovett et al., 2004)
Peeters reported on two patients’ experience of the examination itself which was perceived as “unpleasant,” particularly when having to remove clothing. Peeters quoted a 30–39-year-old female patient, I just counted the seconds until I was allowed to put my clothes back on.
A recommendation was made to ensure that patients are never required to be naked during the examination (Peeters et al., 2019).
None of the papers reported on asking patients specifically about their experience of having an internal examination with the use of a speculum or anoscope. Although Peeter’s small study reported that patients recommended avoidance of speculum use.
Majeed-Ariss’ paper, utilizing a feedback questionnaire design, reported that patients had many suggestions for improvement of the service (including more visibility and an STI follow-up service), but very few about the examination. One comment for improvement about the examination suggested the use of a “smaller probe” (Majeed-Ariss et al., 2019) which may have been referring to speculum use or anoscope.
Some of the patients interviewed by Lovett et al. identified the negative impact of perceiving that they were not believed by the forensic examiner and that this impacted the examination.
As far as the examination, she was very respectful in terms of, you know, making sure I was covered up and explaining things . . . But obviously we’d just had this conversation five minutes before in which I felt she didn’t believe me, and it’s very hard being examined by someone that, you know, has just implied they didn’t believe you . . . The thing that lasts . . . is whether you were believed or not. (Lovett et al., 2004)
Researchers’ Recommendations
From the reviewed papers, there are “lessons learnt” for service providers. Campbell et al. recommended incorporating evaluation of sexual assault services into the service’s standard practice, with expert input from researchers. This could improve service provision for patients and provide encouragement to staff which can help avoid burn out. The researchers commented on the benefits of opening “new channels of communication between nurses and their patients, which can be personally and professionally rewarding” (Campbell, Patterson, Adams, Deigel & Coats, 2008). Fehler-Cabral et al. recognized the importance of service providers incorporating into their forensic practice and training what they call “emotional care” (helping survivors feel safe, respected, and “humanized” through clear communication and explanation of choices) (Fehler-Cabral et al., 2011). Similarly, Peeters noted the need for what is described as a “human approach” (Peeters et al., 2019) with clear information about steps in the examination and care in avoiding the patient being completely naked at any point.
The researchers also made recommendations for future areas that should be explored. Du Mont et al. questioned the importance of certain components of sexual assault MFE protocols such as routinely testing for alcohol and drugs and the use of a colposcope 5 which “add length and a further level of intrusiveness to the internal examination without clear evidence of benefit” (Du Mont et al., 2008). Peeters went further to question the need for speculum examination. Du Mont et al. not only believed that their findings can assist in understanding how the MFE plays a role in creating a feeling of empowerment but also acknowledged that there was work to be done to facilitate patients’ “sense of agency following sexual assault” (Du Mont et al., 2008). The authors recommended further exploration of these issues in a larger sample of patients and across different settings. They also suggested more qualitative research to explore the views of patients on the MFE after they have moved through the criminal justice system as well as the views of those who choose not to engage in the medical forensic process (Du Mont et al., 2008). Similarly, Ericksen et al. supported the need for research on a larger sample of survivors looking at short and longer-term effects of different service models (Ericksen et al., 2002). Greeson et al. recognized the importance of exploring survivors’ experience as they progress through the system and suggested future studies use of “repeated observation to understand survivors’ expressions of agency as they unfold over time” (Greeson & Campbell, 2011).
Lovett et al. reported on the benefits of specialized sexual assault services in being able to provide a more professional service which they put down to “training, as well as the greater potential for developing expertise and monitoring practice” (Lovett et al., 2004). This was borne out in the more positive experiences of patients being examined in a SARC compared to areas where the examiner was a general practitioner enlisted by police to perform a forensic service at a police station. They found SARC examiners were “more likely to conduct the examination with care and sensitivity, including offering as much control as possible to the victim/survivor” (Lovett et al., 2004).
Discussion
This scoping review identified a dearth of research directly from patients on how they experience physical examination procedures when they present for a sexual assault MFE. The few identified research studies contain some common themes including the complex experience of an MFE that can be reassuring, empowering, and restorative but can also be distressing and retraumatizing even when delivered in a patient-centered and trauma-informed manner. The existing research identified the importance of patients having some choice and control over the process.
The few data that exist demonstrate that it is possible to perform in-depth research with victims of sexual assault on their experiences of the MFE. There is a need for better understanding, specifically, about aspects of the MFE such as blood sampling and internal examination, and for this research to include a greater diversity of patients, including those from diverse sexualities, gender nonconforming victim-survivors, and male victim-survivors.
If more can be learned about which aspects of the sexual assault MFE are most upsetting for patients/victim-survivors, it may be possible to re-evaluate the necessity for, and alternatives to, those components of the examination. The existing literature suggests that even among patients who found the examination empowering, some aspects appear to be viewed as an unpleasant necessity, such as the internal examination. Being able to give patients choice and control over the MFE and the components they consent to is important and warrants further exploration.
According to forensic collection guidelines, women can be offered the alternative of a “blind” high vaginal swab taken by the clinician without the use of a speculum (NSW Police Force, 2021; Royal College of Pathologists Australia, 2018; The Faculty of Forensic and Legal Medicine of the Royal College of Physicians, 2021); particularly those without any symptoms of injury, who decline a speculum, or when the examiner determines it would be too traumatic. Current guidelines for forensic sampling do not recommend patient self-collected vaginal swabs such as those which can be used in STI testing and cervical screening (Arbyn et al., 2019; Cancer Council Australia Cervical Cancer Screening Guidelines Working Party, 2021; Garland & Tabrizi, 2004; Ogale et al., 2019). A recent study explored the feasibility of a novel self-collection system using a device similar to a tampon applicator for self-collection of high vaginal samples for DNA recovery after sexual activity (Smith et al., 2017). Although the focus of this study was use of the device in settings without trained forensic clinicians, this highlights the future possibility of a more victim-centered approach by use of a self-sampling device.
As far as we are aware, this is the first review exploring the patient perspective of the MFE. Given that so few relevant data were identified, this highlights a crucial area in need of further research to inform and guide sexual assault services in providing the best possible patient-centered care.
Limitations
As a scoping review directed to identify research gaps, this paper did not attempt to assess the quality of the research. The eligibility criteria limited the literature included to those in peer-reviewed journals and reports containing original research data published by authors from a tertiary institution, in an attempt to ensure inclusion of only high quality studies. Accordingly, a relatively small number of eligible papers were analyzed and summarized, and many of these were published over a decade ago. Nonetheless, we believe combining and summarizing key findings in our scoping review is informative for policy and practice, and we identify important issues that are able to be further explored in future research. The author, Dr Stewart, was primarily responsible for the literature search and review process but was assisted by a university librarian and adjudication for inclusion was a joint responsibility of all authors.
Conclusions
This scoping review identified a significant gap in the research on the patient experience of the physical component of the MFE from the perspective of the patient. Most of the research that has been published was undertaken more than 10 years ago and did not include diverse patient groups such as those from diverse sexualities, gender nonconforming victim-survivors, and male victim-survivors.
There is an urgent need for current, quantitative, and qualitative research to explore the patient experience of the MFE, particularly the physical examination, identify aspects that can be retraumatizing and barriers to presentation as well as highlighting any patient perceived benefits of presenting for a health and forensic response.
Implications for Practice, Policy, and Future Research
When performed in a way that provides patients with informed choice and control, the MFE can be a positive experience and an important part of a sexual assault patient’s recovery and pathway to justice. A calm, sensitive but professional approach using strategies such as reassurance and distraction are appreciated by patients faced with what can be an anxiety provoking experience. However, more can still be learned about how best to provide a sexual assault forensic service that avoids retraumatization.
Future research should explore the patient’s experience of the medical forensic examination and sexual assault kit collection. Campbell’s work on qualitative research methodology that increases participation of victim-survivors can inform future qualitative research (Campbell & Adams, 2008; Campbell, Patterson, Adams, Deigel & Coats, 2008, 2009a, 2009b, 2019).
The potentially restorative impact of having an MFE and the benefit of the integrated health response may not be apparent to victims or their allies when faced with the immediate aftermath of a sexual assault and consideration of response options. More research could help to demonstrate the beneficial effects of the medical forensic response for victims of sexual assault. This could inform public education to increase visibility of, and attendance at, medical forensic sexual assault services.
Improved patient attendance and outcomes may be possible by reframing the “Rape Kit” to reduce victims’ concerns of retraumatization and reassure them of the benefits of a holistic health-led response.
Critical Findings
There is very little research on the patient experience of the medical forensic examination in the current model of care that incorporates medical, forensic, and psychosocial support to victims of sexual assault.
When provided in a patient centered way, the MFE can be a positive experience which is empowering and reassuring but it can also be retraumatizing.
More research is needed to gain a better understanding of how patients experience the medical forensic examination and what aspects are in need of improvement.
Footnotes
Appendix A
Questions related to the examination from Campbell, Patterson, Adams, Deigel & Coats’s (2008) paper.
In your interaction with the nurse, how often did (none of the time, some of the time, most of the time):
Acknowledgements
We would like to acknowledge the support of the librarian services at the University of Sydney, in particular Kanchana Ekanayake and the librarian services at the Northern Clinical School, University of Sydney and academic support from the Learning Centre, University of Sydney.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: As a domestic PhD candidate, Dr. Stewart has been awarded a tuition fee scholarship for a higher degree by research (HDR) program under the Australian Government’s Research Training Program (RTP). Dr. Stewart is also a recipient of a Ramsay Research and Education Grant at the Northern Sydney Local Health District.