
Abstract
Parenting programs are the most common intervention for preventing the lethal form of child maltreatment, abusive head trauma (AHT). However, certain results of the effects of these programs have not yet been compared across studies. A systematic review with meta-analysis is warranted to quantitively synthesize the available evidence to identify effective elements and strategies of the programs for preventing AHT. This review aims to estimate AHT preventive parenting programs’ pooled effect on the reduction of AHT incidence, the improvement of parental knowledge, and the increased use of safe strategies in response to infants’ inconsolable crying. Studies published in English and Mandarin were searched and retained if they were randomized control trials (RCTs) or with a quasi-experimental design, included an AHT preventive parenting program, and provided data that quantified targeted outcomes. Eighteen studies were included in this review. AHT preventive parenting programs had a pooled effect on improving parents’ knowledge and increasing the use of safe coping strategies in response to inconsolable crying but not on the incidence of AHT and parents’ emotional self-regulation. Subgroup analyses showed that the intervention effects were mostly present across study designs or measurements and emerged in the reduction of AHT incidence compared with historical controls. The findings suggest that AHT preventive parenting programs enhance parenting knowledge and skills to provide safe care for infants. Further efforts to evaluate AHT parenting programs on the reduction of AHT incidence are necessary for decision-making on allocating and disseminating interventions.
Keywords
Introduction
Preventing child abuse, especially for young children, is a public health priority worldwide (Gray et al., 2016). Abusive head trauma (AHT), a lethal form of child abuse, contributes to nearly one-third of the total child abuse fatalities (Palusci & Covington, 2014). More than two-thirds of AHT survivors experienced at least one neurodevelopmental disability (Jackson et al., 2021; Manfield et al., 2021; Nuño et al., 2018). Infants and young children, the main victims of AHT (Chang et al., 2021; Nuño et al., 2020), cannot protect themselves due to developmental immaturity. Therefore, prevention interventions are designed and targeted to reduce parental risk factors and improve parental knowledge and parenting skills. Many child maltreatment prevention interventions that have shown evidence in reducing child abuse and neglect have included parenting education strategies (MacMillan et al., 2009). For example, Nurse–Family Partnership, Early Start, and Healthy Families America are effective home-visiting programs (Avellar & Supplee, 2013); Triple P–Positive Parenting Program is one of the evidence-based parenting programs aimed at preventing child abuse and neglect (Sanders et al., 2014). Systematic reviews found that parenting interventions to prevent child maltreatment effectively reduced harsh and dysfunctional parenting (Chen & Chan, 2016) and improved parent–child interaction (Fang et al., 2022). Similarly, parenting programs could effectively prevent AHT by reducing unsafe rearing behaviors and enhancing parents’ awareness of AHT. Several individual studies (Barr et al., 2018; Cala Cala et al., 2020; Dias et al., 2005; Fujiwara, Isumi, Sampei, Yamada, et al., 2020) have found the effectiveness of parenting programs in preventing AHT, but the results have not been compared across studies. Thus, a systematic review with meta-analysis is imperative to comprehensively explore and synthesize the available evidence to identify effective elements and strategies of programs preventing AHT.
Parenting programs on the awareness of AHT are the most common preventive interventions (Lopes & Williams, 2018; Roygardner et al., 2021). Several well-known programs have been implemented nationwide or worldwide for decades, such as The Period of PURPLE Crying® (Barr, Barr, et al., 2009; Barr, Rivara, et al., 2009; Runyan et al., 2009), Prevent Shaken Baby Syndrome! (Dias et al., 2005), and Shaking Your Baby is Just Not the Deal (Tolliday et al., 2010). The ultimate goal of these parenting programs is to prevent or reduce the occurrence of AHT by helping parents cope with infants’ inconsolable crying, the primary trigger of AHT. The content of the programs includes characteristics of normal crying patterns, risks of shaking, causes and symptoms of AHT, and safe practices and strategies to cope (e.g., walking away when confronting unsoothable crying) under baby care stress (Lopes & Williams, 2018). The main outcome indicators in the preventive interventions on AHT include reducing the incidence of AHT, raising awareness of AHT (i.e., knowledge about normal crying patterns and dangers of shaking), and increasing parents’ safe coping behaviors and emotional self-regulation in response to inconsolable crying or frustration (Lopes & Williams, 2018).
The reduction of AHT incidents is an important indicator for evaluating the effectiveness of parenting programs after implementing regional and national prevention strategies (Altman et al., 2011; Barr et al., 2018; Dias et al., 2005, 2017). Barr et al. (2018) evaluated the effectiveness of The Period of PURPLE Crying® and revealed a 35% reduction in the AHT incident rate among children < 2 years old after an 8-year implementation. A 47% reduction in the incidence of AHT (p = .017) among children <36 months old was also found after implementing Prevent Shaken Baby Syndrome! in Western New York State for 5.5 years (Dias et al., 2005). However, no difference in the incidence of AHT was found between Pennsylvania State which implemented the Pennsylvania Shaken Baby Syndrome Prevention Program and five other states without AHT parenting education (Dias et al., 2017). The inconsistent finding of the AHT preventive interventions warrants a comprehensive quantitative synthesis to examine their effect on reducing the incidence of AHT.
Although the literature has shown the effectiveness of parenting programs in improving knowledge on normal crying patterns or dangers of shaking (Barr, Rivara, et al., 2009; Cala Cala et al., 2020; Groisberg et al., 2020; Kaya et al., 2022; Taşar et al., 2014), these individual study results were not systematically analyzed and summarized. Cala Cala et al. (2020) implemented All Babies Cry in a women-and-infants hospital for low-income mothers of newborns. The result showed that mothers’ knowledge of the peak of crying improved in the intervention group than in the control group (percentage of improvement: 31% vs. 13%, p = .026). The effectiveness of The Period of PURPLE Crying® evaluated by Barr, Rivara, et al. (2009) and Fujiwara, Isumi, Sampei, Miyazaki, et al. (2020) also showed improved knowledge of mothers of newborns on normal crying patterns and dangers of shaking. However, in some studies, the same program did not improve parents’ knowledge of the dangers of shaking (Barr, Barr, et al., 2009; Fujiwara et al., 2012).
Using safe strategies and emotional self-regulation in response to inconsolable crying and/or parental frustration is another common outcome indicator for evaluating the effectiveness of parenting programs in preventing AHT (Bechtel et al., 2011; Coster, 2017; Lopes et al., 2018). However, the results with this indicator were inconsistent across studies. Bechtel et al. (2011) revealed that parents receiving the Take 5 Safety Plan for Crying were more likely to take a break to cope with the situation when frustrated with inconsolable crying than those in the control group (adjusted odds ratio [aOR] = 3.10, 95% confidence interval [CI] [1.62, 5.93]). On the contrary, Barr, Barr, et al. (2009) and Fujiwara et al. (2012) reported an insignificant difference in the frequency of maternal behaviors, including taking a break in response to inconsolable crying, between the intervention and control groups. Similarly, parents who received AHT preventive programs involving strategies for responding to inconsolable crying may either use more self-talk to gain control over their emotions (Fujiwara, Isumi, Sampei, Yamada, et al., 2020; Morrill et al., 2015) or not (Barr, Barr, et al., 2009; Fujiwara, Isumi, Sampei, Miyazaki, et al., 2020). A synthesis of the effectiveness of AHT preventive parenting programs can provide a basis to optimize the design of future research and interventions to prevent AHT. Efforts should be made to comprehensively organize and analyze the evidence to identify the effectiveness of parenting programs in preventing AHT.
While a few reviews have summarized the content of AHT preventive programs (Lopes & Williams, 2018; Roygardner et al., 2021; Stoll & Anderson, 2013), no study has systematically examined the effectiveness of parenting programs in preventing AHT. Lopes and Williams (2018) searched 21 databases and reviewed 20 AHT prevention initiatives among 34 studies. Detailed information on the strengths, limitations, and empirical evidence of each initiative (i.e., three types of initiatives: reduction in infant crying, targeting caregiver’s emotional regulation, and raising awareness about AHT) were reported, and a summary of implications for research and practice was provided. The other two reviews on AHT prevention conducted by Roygardner et al. (2021) and Stoll and Anderson (2013) identified three critical components of AHT prevention, including parental education, community services involvement, and health professional education. However, the effectiveness of parenting programs in preventing AHT was not integrated and analyzed. All three reviews did not incorporate meta-analyses. The review conducted by Lopes and Williams (2018) did not appraise the research quality. The study design and level of evidence rather than a critical appraisal of study validity were used to judge the research quality in the remaining two reviews (Roygardner et al., 2021; Stoll & Anderson, 2013). With the external validity of the individual studies being limited by their small sample size, especially the randomized trials, a systematic review and meta-analysis that integrates and appraises the existing evidence and increases the sample size is crucial to improving the rigor of the review and the precision of the estimates of intervention effects (Akobeng, 2005). Therefore, this systematic review aims to address the gap in the effectiveness of parenting programs in preventing AHT through a comprehensive search and the inclusion of updated evidence.
Objective
This systematic review aims to evaluate the effectiveness of parenting programs in preventing AHT in (a) reducing the incidence of AHT, (b) improving parents’ knowledge of normal crying patterns and dangers of shaking, and (c) improving the parents’ safe coping strategies and emotional self-regulation in response to inconsolable crying.
Methods
Protocol and Registration
This systematic review was registered in the international prospective register of systematic reviews (PROSPERO, CRD 42020201613) and was performed and reported according to the preferred reporting items for systematic review and meta-analysis (PRISMA) 2020 statements (Page et al., 2021).
Information Sources and Search Strategy
A systematic literature search was conducted in six electronic databases: PubMed, Cumulative Index to Nursing and Allied Health Literature (CINAHL) [EBSCOhost], Ovid Medline, Embase, Cochrane Library, and Airiti Library (a Mandarin-language integrated academic resources platform), from inception to March 3, 2022. Hand-searching was conducted by checking the reference lists of included studies for eligibility to increase the comprehensibility of literature searching.
Four types of keywords were “parent/caregiver,” “abusive head trauma/shaken baby syndrome/crying/shaking,” “intervention/prevention,” and “outcome/effectiveness” and their synonyms (Supplemental Table S1 in Appendix A). Search strategies were further developed with a combination of free-text terms and a controlled vocabulary of keywords: medical subject headings (Mesh), Embase subject headings (Emtree), and CINAHL subject headings via Boolean operators (Supplemental Table S1 in Appendix A). A librarian helped carefully examine the keyword and search process to ensure the reproduction of the review.
Eligibility Criteria for Inclusion/Exclusion in This Review
AHT for this review is defined as “an injury to the intracranial contents or skull of an infant or child younger than 5 years old due to violent shaking and/or inflicted blunt impact” (Joyce et al., 2022; Parks et al., 2012). Studies were included for further screening and scanning if the following criteria were met: (a) Research methodology: The research designs were randomized control trials (RCT) or quasi-experimental studies; (b) Characteristics of participants: The subjects were parents or expectant parents; (c) Content of interventions: The interventions were aimed at AHT prevention; (d) Content of controls: The comparisons were standard treatment/routine care, no treatment, or non-AHT-related preventive interventions; (e) Types of outcome measures: Three outcome variables were: the incidence of AHT, parents’ knowledge of normal crying patterns and dangers of shaking, and safe coping strategies and self-emotional regulation in response to inconsolable crying. Studies not published in English or Mandarin were excluded.
Selection Process and Data Extraction
EndNote X9 was used to manage the search results. Two independent reviewers (HC and PW) completed the initial title and abstract screening, followed by a full-text screening. Any discrepancies between the authors were resolved by a group discussion or by consulting the third reviewer (YC).
For the studies included, three reviewers (HC, YC, and PW) extracted the information using a standardized data extraction form on Microsoft Excel. The information comprises the first author, year of publication, country, setting, participants and sample size, research design, intervention (program name, elements and structure, dose, and timing), comparison, measurements, and results. If the required information for data analysis, such as mean or standard deviation (SD), was not presented, the authors of the original articles were contacted for detailed information.
Quality Assessment
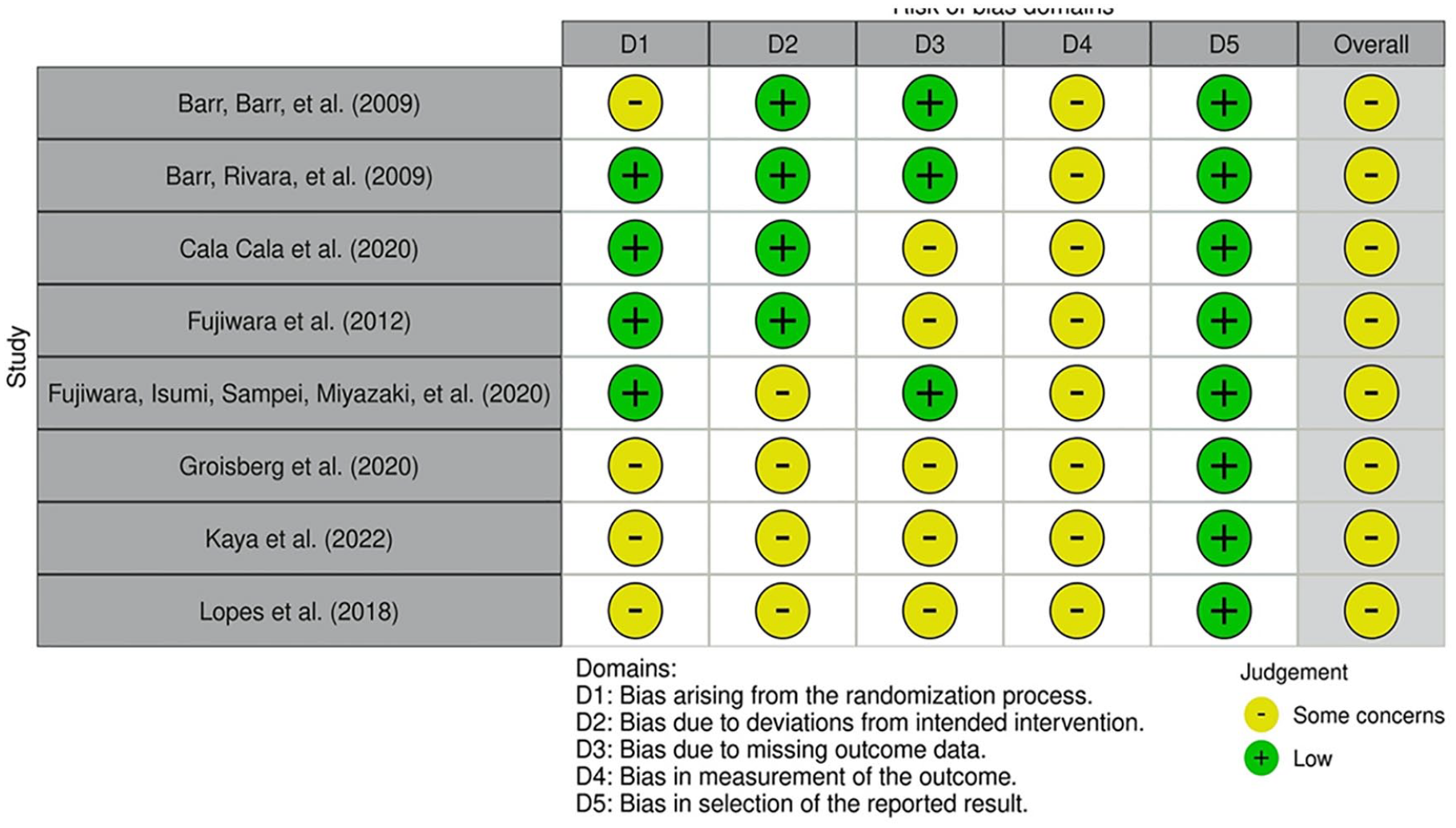
The methodological quality appraisal for the included studies was performed by two independent reviewers (HC and YC). For the randomized trials, the Risk of Bias 2.0 (RoB 2.0) tool was applied; for the non-randomized studies of interventions, the Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I) tool was used (Sterne et al., 2016, 2019). RoB 2.0 comprises five domains and an overall judgment. The five domains are as follows: (a) bias arising from the randomization process; (b) bias due to deviations from the intended interventions; (c) bias due to missing outcome data; (d) bias in the measurement of the outcome; and (e) bias in the selection of the reported result. The judgments for each domain can be rated as “high risk of bias,”, “some concerns,” or “low risk of bias,” based on the answers to a series of questions (i.e., yes, probably yes, probably no, no, and no information) within each domain.
The ROBINS-I tool contains seven domains: (a) bias due to confounding; (b) bias in the selection of participants into the study; (c) Bias in the classification of interventions; (d) bias due to deviations from intended interventions; (e) bias due to missing data; (f) bias in the measurement of outcomes; and (g) bias in the selection of the reported result. Each domain consists of a series of questions with the response options: yes, probably yes, probably no, no, and no information. Each domain has recommended criteria for judging as “low risk of bias,” “moderate risk of bias,” “serious risk of bias,” “critical risk of bias,” and “no information.” The overall risk of bias is judged by a comprehensive consideration of the five domains in RoB 2.0 (Sterne et al., 2019) and seven domains in ROBINS-I tools (Sterne et al., 2016), respectively. A visualization tool for creating plots of RoB 2.0 and ROBINS-I was used in this review (McGuinness & Higgins, 2021).
Assessment of Heterogeneity
Statistical heterogeneity between studies was quantified using the I2 statistics. I2 > 30%, I2 > 50%, and I2 > 75% were regarded to indicate moderate, substantial, and considerable heterogeneity, respectively (Deeks et al., 2022).
Data Synthesis and Statistical Analysis
Meta-analyses using the Review Manager 5.3 software were undertaken to synthesize the effects of parenting programs on preventing AHT (The Nordic Cochrane Centre, Copenhagen). Random effect models with the DerSimonian–Laird method were used for all meta-analyses in this study. For continuous outcomes, standardized mean differences (SMD) with 95% CIs were calculated as the difference in means between groups divided by the pooled SD. The standard error (SE), CI, or t values were used to calculate whether SD was unavailable. For dichotomous outcomes, risk ratios (RR) with 95% CI were calculated. Forest plots were generated for all meta-analyses.
Subgroup analyses were performed based on different types of intervention or participant characteristics. Sensitivity analyses were conducted to test the robustness of the pooled estimates on the outcomes of parental knowledge and safe coping strategies in response to inconsolable crying. The sensitivity analyses using the strategies of excluding quasi-experimental studies or studies with overall high or serious risk of bias were performed to assess the robustness or consistency of the conclusions of meta-analyses. A narrative synthesis was done when a quantitative synthesis was not feasible. A test for publication bias was performed in a meta-analysis containing at least 10 studies.
Results
Search Results
The search process is illustrated in Figure 1. An initial search resulted in 7,625 records, of which 38 studies via databases were assessed for eligibility. An additional search from the reference lists retrieved three studies for further assessment. A total of 18 studies were included in this review.

Flow diagram of the review process and article identification.
Characteristics and Designs of Included Studies
The years of publication ranged from 2005 to 2022 (Supplemental Table S2 in Appendix B). Of 18 studies included, nine were conducted in the USA, three in Japan, two in Canada and Turkey, and one in Brazil and the United Kingdom. Seven trials randomized individual participants, and one trial randomized participating hospitals (clusters) into treatment and control groups. The remaining 10 studies were quasi-experimental designs. The majority of the included studies involved a two-arm trial. Only one study used a four-arm design with three intervention groups and one matched comparison group (Coster, 2017).
Content of Intervention and Comparison
A total of nine different parenting programs for preventing AHT were identified among 18 studies in this review, including The Period of PURPLE Crying® (eight studies), All Babies Cry© (two studies), The Shaken Baby Prevention Project in Western Sydney: Shaking Your Baby is Just Not the Deal (two studies), state- or community-mandated AHT educations (four studies), and other hospital-based AHT educational programs (two studies).
Among the eight RCTs, four used placebo controls (i.e., another intervention without elements of AHT prevention), one used usual-care control with verbal information about AHT prevention, and the rest of the three RCTs used a cross-over design. Among the ten quasi-experimental studies, six used usual-care controls, and four used historical controls. Given the focus of this review on parenting programs and interest in outcomes about crying, shaking, and parents’ behavior and emotional regulation in response to inconsolable crying, all included studies targeted the parents of infants or young children under 3 years of age. Most (n = 15, 83%) trials enrolled mothers or parents of newborns as their participants. Further information about the designs and characteristics of interventions, settings, and participants is presented in Supplemental Table S2.
Outcomes
This review examined the incidence of AHT in 5 out of 18 studies. Data were obtained from medical records with AHT-related diagnoses through regional/state-wide healthcare databases and/or child service records (Altman et al., 2011; Barr et al., 2018; Dias et al., 2005, 2017; Zolotor et al., 2015). The case definitions of AHT for the included five studies that measured the incidence of AHT are presented in Supplemental Table S3 (Appendix C). The parents’ self-report of knowledge and behaviors were explored in the remaining 13 studies. Two-thirds of studies (n = 9) measured the outcomes of self-report knowledge and behaviors once from a couple of weeks to months after the intervention. Four studies had more than one measure timepoint, including post-test data and follow-up data ranging from 2 to 5 months after intervention (Cala Cala et al., 2020; Kaya et al., 2022; Lopes et al., 2018; Morrill et al., 2015).
Risk of Bias
An overview of the methodological quality of the included studies is presented in Figures 2 and 3. All eight RCTs in this review were rated as having “some concerns” about the overall risk of bias (Figure 2). All ratings for the bias in the measurement of the outcomes included having “some concerns” due to the nature of participant-reported outcomes. The risk was rated as having “some concerns” for four out of the eight RCTs with regard to insufficient or unclear information for randomization methods and concealment (Barr, Barr, et al., 2009; Kaya et al., 2022; Lopes et al., 2018) and pseudo-randomization (Groisberg et al., 2020). The other four trials used random sequences generated by computer or coin toss (Barr, Rivara, et al., 2009; Cala Cala et al., 2020; Fujiwara, Isumi, Sampei, Miyazaki, et al., 2020; Fujiwara et al., 2012). In terms of the bias due to deviations from the intended intervention, four studies were rated as having “some concerns” because no information was provided to judge whether the participants’ non-adherence to intervention was related to the recruitment and implementation of the intervention (Fujiwara, Isumi, Sampei, Miyazaki, et al., 2020; Groisberg et al., 2020; Kaya et al., 2022; Lopes et al., 2018). Five studies were rated as having “some concerns” on the “bias due to missing outcome data” as the reasons for participants’ withdrawal, the management for missing data, or the differences between groups when the loss to follow-up was not reported (Cala Cala et al., 2020; Fujiwara et al., 2012; Groisberg et al., 2020; Kaya et al., 2022; Lopes et al., 2018).
Summary of risk of bias of randomized trials.
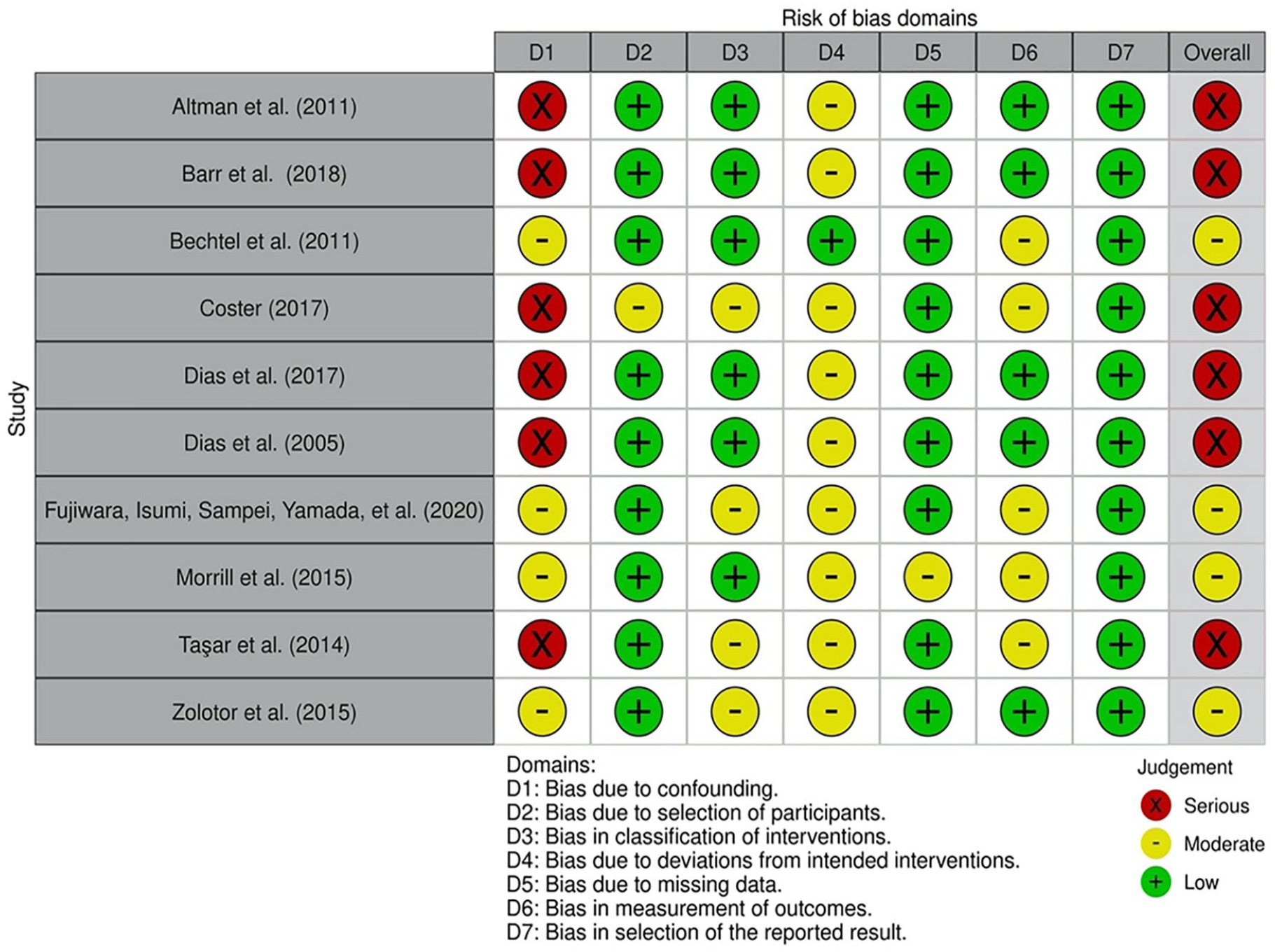
Summary of risk of bias of quasi-experimental trials.
The overall rating for six out of ten quasi-experimental studies was a serious risk of bias due to uncontrolled (Coster, 2017; Taşar et al., 2014) or uncontrollable (Altman et al., 2011; Barr et al., 2018; Dias et al., 2005; Dias et al., 2017) confounding of the effect of intervention in the studies (Figure 3). Nine studies were rated as a moderate risk of performance bias due to the lack of fidelity in the implementation of the intended intervention (i.e., not every parent of an infant received intervention during the state-wide or province-wide intervention periods, different doses of intervention for participants, without mention of the specific training for intervention practitioners across different institutions).
Effects of Interventions
The meta-analyses were performed using data from 16 studies. The studies by Altman et al. (2011) and Coster (2017) were excluded from the meta-analysis because their case definitions were incompatible with that of the other studies (Supplemental Table S2); nevertheless, the effectiveness of the interventions was still reported.
Incidence of AHT
The results showed that the incidences of AHT were rare events. Hence, newly diagnosed AHT cases per million same-aged population were used for the meta-analysis. The pooling result from four out of the five studies showed an insignificant difference between intervention and control groups (RR = 0.83, 95% CI [0.55, 1.26]; Figure 4). Considerable heterogeneity was noted (I2 = 95%). The subgroup analysis by the types of control (i.e., two historical controls and two regional controls) showed a reduction in the incident rate of AHT (RR = 0.55, 95% CI [0.48, 0.64]) in the subgroup of historical controls and a higher incident rate of AHT (RR = 1.13, 95% CI [1.01, 1.27]) in the subgroup of regional controls after implementing the intervention.
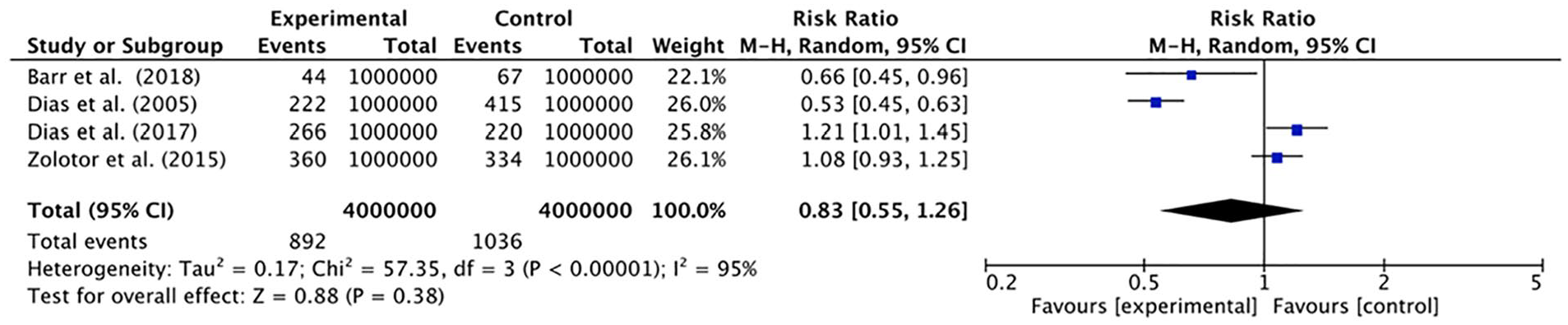
Forest plot of comparison of AHT preventive parenting programs versus regular care for the outcome of the AHT incident rate.
Altman et al. (2011) analyzed the incident rate of infants with AHT diagnosis to evaluate the effectiveness of a 3-year implementation of an AHT prevention program compared to a 5-year historical control. Two infants during the 3-year intervention period (0.7 injuries per year) and 14 infants during the 5-year historical control (2.8 injuries per year) were born and treated for AHT, showing a 75% reduction of the incidence (p = .03).
Knowledge of normal crying patterns
A total of 11 studies were used to evaluate the effects of the intervention on parents’ knowledge of normal crying patterns. Two meta-analyses were performed because of different levels of measurement (i.e., seven studies used the mean and SD of the scores, and four used the percentage of incorrect answer rate) to present the result of parents’ knowledge.
The result of the meta-analysis of seven studies using mean and SD showed that parenting programs improved the scores on parents’ knowledge of normal crying patterns at postintervention compared to control groups (SMD = 0.69, 95% CI [0.49, 0.89]; I2 = 95%; Figure 5(a)). The sensitivity analysis result showed that the intervention effects were maintained even when one quasi-experiment was excluded from the meta-analysis of the seven studies (SMD = 0.80, 95% CI [0.55, 1.05]; I2 = 95%). Subgroup analysis was performed based on the outcome measurements. Five studies used the same scale developed by Barr and his colleagues (Barr, Barr, et al., 2009; Barr, Rivara, et al., 2009; Fujiwara, Isumi, Sampei, Miyazaki, et al., 2020; Fujiwara, Isumi, Sampei, Yamada, et al., 2020; Fujiwara et al., 2012). The other two studies (Kaya et al., 2022; Lopes et al., 2018) used self-developed scales. A small reduction in heterogeneity and significant differences between intervention and control groups were found in subgroup analyses of five studies using Barr’s scale (SMD = 0.41, 95% CI [0.31, 0.51]; I2 = 81%) but not in the two studies using a self-report scale (SMD = 1.95, 95% CI [0.75, 3.16]; I2 = 93%).
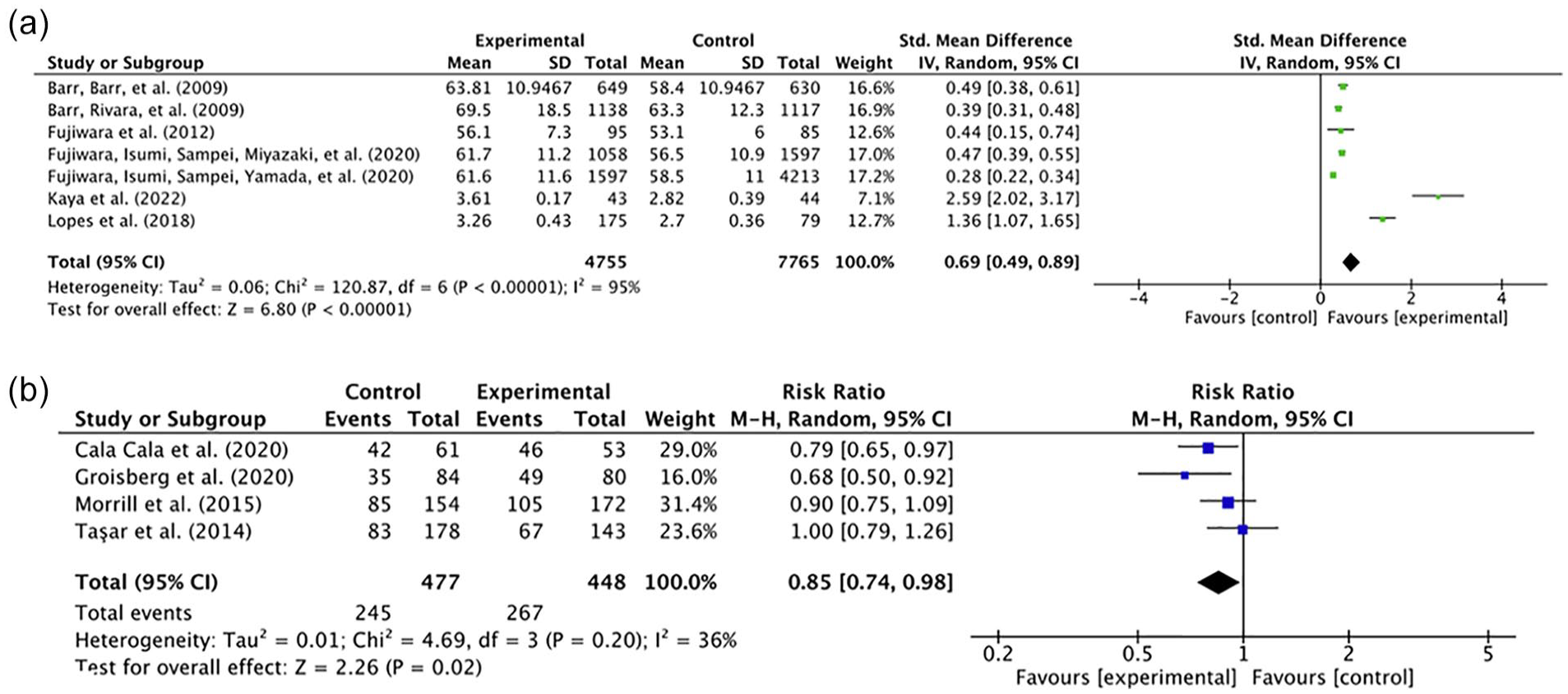
Forest plot of comparison of AHT preventive parenting programs versus controls for the outcome of parents’ knowledge of normal crying patterns. (a) Mean and SD of the scores were used in seven studies and (b) The percentage of incorrect answer rate was used in four studies to evaluate the effects of the intervention on parents’ knowledge of normal crying patterns.
A lower risk for incorrect answers among parents was found in the intervention groups than in the controls among four studies using the percentage of incorrect answer rate (RR = 0.85, 95% CI [0.74, 0.98]; I2 = 36%; Figure 5(b)). The result of sensitivity analysis showed that the intervention effects were maintained when one study (Taşar et al., 2014) with a high risk of bias was excluded from the meta-analysis of the four studies (RR = 0.81, 95% CI [0.70, 0.94]; I2 = 24%). Four studies were divided into two subgroup analyses according to study design. The results of the subgroup analyses showed a significant reduction of heterogeneity (I2 = 0%). An intervention effect was found (RR = 0.76, 95% CI [0.64, 0.90]) in the subgroup of two randomized trials (Cala Cala et al., 2020; Groisberg et al., 2020), while no significant difference was found between intervention and control groups (RR = 0.94, 95% CI [0.81, 1.09]; I2 = 0%) in the subgroup of two quasi-experiments (Morrill et al., 2015; Taşar et al., 2014).
Knowledge of the dangers of shaking
Two meta-analyses (one of seven studies used the mean and SD of the scores; the other three used the percentage of incorrect answer rate) were performed to evaluate the effects of the intervention on parents’ knowledge of the dangers of shaking. The result of the meta-analysis of seven studies using mean and SD showed that parenting programs significantly improved the scores on knowledge of the dangers of shaking at post-intervention compared to control groups (SMD = 0.51, 95% CI [0.28, 0.73]; I2 = 96%; Figure 6(a)). The sensitivity analysis result revealed that the intervention effects were maintained when one quasi-experiment was removed from the meta-analysis of the seven studies (SMD = 0.66, 95% CI [0.34, 0.97]; I2 = 97%). Subgroup analysis was performed based on different outcome measures (i.e., five studies used the scale developed by Barr and his colleagues, and two used self-developed scales) for seven studies using the mean and SD of the scores. A small reduction in heterogeneity and significant differences between intervention and control groups were found in the subgroup analysis of five studies (SMD = 0.19, 95% CI [0.07, 0.31]; I2 = 87%). There were no significant differences and heterogeneity reduction in the meta-analysis of the remaining two studies (SMD = 2.42, 95% CI [−0.59, 5.42]; I2 = 98%).
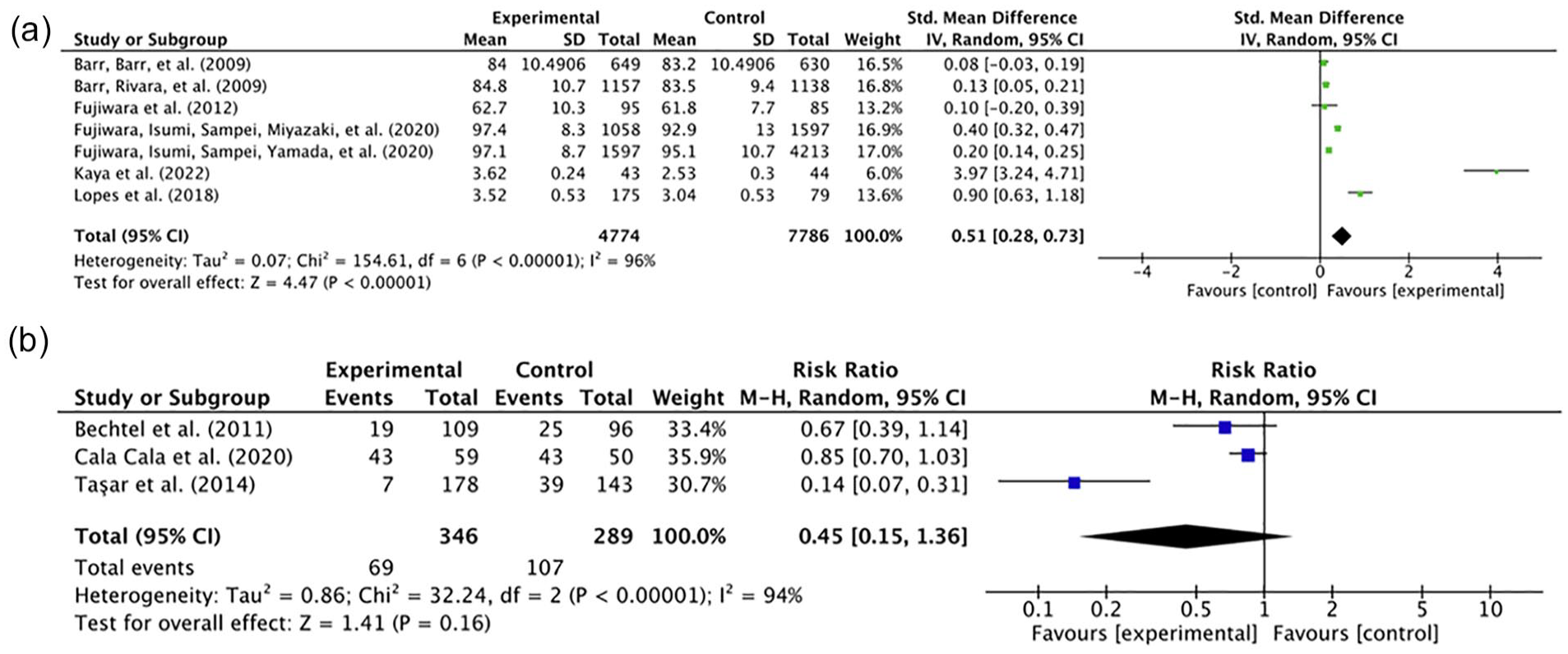
Forest plot of comparison of AHT preventive parenting programs versus controls for the outcome of parents’ knowledge of the dangers of shaking. (a) Mean and SD of the scores were used in seven studies and (b) The percentage of incorrect answer rate was used in three studies to evaluate the effects of the intervention on parents’ knowledge of the dangers of shaking.
There was no significant difference in parents’ knowledge of the dangers of shaking between the intervention and control groups among three studies using the percentage of incorrect answer rate (RR = 0.45, 95% CI [0.15, 1.36]; I2 = 94%; Figure 6(b)). The intervention effect emerged when one study (Taşar et al., 2014) with a high risk of bias was excluded from the meta-analysis in the sensitivity analysis (RR = 0.82, 95% CI [0.69, 0.99]; I2 = 0%). Subgroup analysis was not performed on only three studies in this meta-analysis.
Safe coping strategies in response to inconsolable crying
The intervention effect on parents’ safe coping strategies in response to inconsolable crying was assessed by asking parents to indicate how often (frequency) they have used the listed behaviors. Six studies using the mean and SD of the scores were analyzed. The result of the meta-analysis showed a low level of heterogeneity and marginally significant increased use of safe coping strategies among parents in the intervention groups compared to those in the control groups (SMD = 0.05, 95% CI [0.00, 0.10]; I2 = 26%; Figure 7). The sensitivity analysis result showed that the intervention effect did not exist when two quasi-experiments were excluded from the meta-analysis (SMD = 0.04, 95% CI [−0.01, 0.09]; I2 = 0%). The findings of the subgroup analyses by study design showed insignificant effects of the interventions on the parents’ behaviors in response to inconsolable crying among RCTs and quasi-experiments (SMD = −0.01, 95% CI [−0.27, 0.24]; I2 = 81%).

Forest plot of comparison of AHT preventive parenting programs versus controls for the outcome of parents’ safe coping strategies in response to inconsolable crying among six studies using mean and SD of the scores.
Coster (2017) recruited and divided parents into three intervention groups with different time points of film watching on AHT prevention (i.e., antenatal, immediate postnatal, and 6-week postnatal) and one matched control. The findings of the survey for infants aged 6–9 months revealed that parents in the intervention groups were more likely to use the strategy of “putting infants down in a safe place and walking away” in response to inconsolable crying than the control groups (interventions vs. control = 48%–61% vs. 42%, p < .05).
Emotional self-regulation in response to inconsolable crying
Five studies evaluated the effects of the intervention on parents’ emotional self-regulation in response to inconsolable crying by asking parents about the frequency of using the listed behaviors. There was no intervention effect on the use of emotional self-regulation after the intervention compared to the control groups (SMD = 0.07, 95% CI [−0.03, 0.18]; I2 = 63%; Figure 8). The sensitivity analysis result showed an insignificant intervention effect after removing one quasi-experiment from the meta-analysis (SMD = 0.04, 95% CI [−0.06, 0.14]; I2 = 66%). The findings of subgroup analyses based on different types of controls showed insignificant effects of the interventions on the parents’ emotional self-regulation in response to inconsolable crying compared to either placebo controls (SMD = 0.08, 95% CI [−0.02, 0.17]; I2 = 34%) or usual-care controls/cross-over design (SMD = 0.01, 95% CI [−0.12, 0.13]; I2 = 85%).

Forest plot of comparison of AHT preventive parenting programs versus controls for the outcome of parents’ emotional self-regulation in response to inconsolable crying.
Discussion
This review synthesized evidence from eight RCTs and 10 quasi-experiments to evaluate the effectiveness of parenting programs in preventing AHT, reducing AHT incidence, and improving parents’ knowledge, coping strategies, and self-regulation. There was no pooling effect on decreasing the incidence of AHT after the intervention. Notably, an intervention effect on the reduction of AHT incidence appeared in the subgroup analysis compared with historical controls. The pooling effects of parenting programs demonstrated significant effects on improving parents’ knowledge about normal crying patterns and the dangers of shaking and using safe coping strategies in response to inconsolable crying. However, no intervention effect on emotional self-regulation in response to inconsolable crying was found between the intervention and control groups (Table 1, a summary table of the critical findings of the present review).
Summary Table of Critical Findings.

Note. AHT = abusive head trauma.
Effectiveness on AHT Incidence
The pooled effect of parenting programs from four quasi-experiment studies showed no reduction of the AHT incidence rate with considerable heterogeneity; however, the subgroup analyses suggested a substantial reduction of heterogeneity and an intervention effect of decreased incidence of AHT in programs with historical controls compared to those with concurrent regional controls. This result could be interpreted as different extents of bias deriving from different control groups (Pandis, 2012; Papageorgiou et al., 2017; Thomas, 2014). The use of historical controls could overestimate (Pandis, 2012) or underestimate (Papageorgiou et al., 2017) the intervention effects than concurrent controls in clinical trials. Chronological bias or time trend bias occurs when historical controls are used (Ghadessi et al., 2020; Pannucci & Wilkins, 2010), in which outcomes vary over time and confound the intervention effects (Pandis, 2012). Even in RCTs, a large block size for randomization is related to an increased extent of chronological bias with highly inflated type 1 error, leading to an overestimation of the intervention effect (Tamm & Hilgers, 2014). Nevertheless, AHT is a rare and life-threatening condition, in which the design with historical controls is necessary to achieve a sufficient power analysis (Hatswell et al., 2020) and make trials feasible. Among the four included studies with the outcome of AHT incidence, only one study (Zolotor et al., 2015) controlled the bias from confounders via statistical analysis. Whatever kinds of control arms would be used, it is suggested that observational trials be required to reduce the effects of bias and confounders, such as adjustment for the bias using mixed treatment comparison for summary data or propensity score method for individual data (Ghadessi et al., 2020), to better estimate the effectiveness of AHT preventive interventions in future research.
Another potential explanation for the different results between the two subgroup analyses on AHT incidence was that a global great economic recession (December 2007–June 2009) coincided with the implementation of AHT preventive programs in the two trials with concurrent regional controls (Dias et al., 2017; Zolotor et al., 2015). On the other hand, programs whose implementation periods for trials and historical controls were before (Altman et al., 2011; Dias et al., 2005) or after (Barr et al., 2018) the economic recession with little overlapping time showed significant intervention effects on reducing AHT incidents. Literature has shown that the great economic recession was associated with a rise in the AHT rate (Berger et al., 2011; Huang et al., 2011; Wood et al., 2016). Further, the intervention effect on reducing the occurrence of AHT could be weakened by the consequences of the economic recession. The results of this review echo the findings from previous studies that an increased rate of AHT in the subgroup analysis with current regional controls would be reflected in the economic stress during the economic recession.
Effectiveness on Knowledge
The results of this review revealed an intervention effect on knowledge improvement on normal crying patterns and dangers of shaking after both sensitivity and subgroup analyses. In addition, the findings from subgroup analyses showed that trials using the same measurement tools or with an RCT design had significant intervention effects. The use of the same measurement tools or RCT research design can reduce heterogeneity and diminish potential biases or confounders, making the results more robust.
Knowledge about infant crying, the dangers of shaking, strategies to soothe infants, or other AHT-prevention-related information was involved in all the parenting programs in this review. Parents’ knowledge related to parenting practice and behavior is a vital parenting competence to support parenting and child outcomes (National Academies of Sciences, Engineering, and Medicine, 2016). The improved knowledge can empower the parents’ capacity to understand and use health information to modify their risk behaviors (Nutbeam, 2000). Literature has shown that the increase in parental knowledge about infant sleep health and behavior is associated with using a safe and healthy sleep environment for infants (Middlemiss et al., 2015). Accordingly, improving parental knowledge has been regarded as a mandatory approach to parent training interventions.
Effectiveness on Safe Coping Strategies and Emotional Self-Regulation
The findings of this review showed that parenting programs had marginal effects on the use of safe coping strategies but no intervention effect on emotional self-regulation in response to inconsolable crying. Only two out of the seven included studies with the outcome of using safe coping strategies have found that parents in the intervention groups reported significantly increased use of safe behavioral responses to infant crying compared with the control groups (Coster, 2017; Fujiwara, Isumi, Sampei, Yamada, et al., 2020). In contrast, parents’ self-reported risky behaviors of shaking were found to be an effective indicator to detect the intervention effect to evaluate the effect of parenting programs on preventing AHT (Fujiwara, Isumi, Sampei, Miyazaki, et al., 2020; Fujiwara, Isumi, Sampei, Yamada, et al., 2020). Behavioral change can be regarded as an outcome indicator to evaluate the effect of interventions on improving health outcomes and preventing child maltreatment (van IJzendoorn et al., 2020). Both safe coping strategies and risky behaviors of shaking can be adopted to assess the effect of parenting programs on preventing AHT.
Using positive self-talk as one of the cognitive reappraisal strategies for emotional self-regulation can help downregulate parents’ negative emotions, reducing the use of negative parenting behaviors (Zimmer-Gembeck et al., 2022). Only one study showed increased use of emotional self-regulation when confronting inconsolable infant crying among parents in the intervention arm than the control arm, but the intervention effect was not significant after adjusting covariates (Fujiwara, Isumi, Sampei, Yamada, et al., 2020). Infants’ inconsolable and unsoothable crying is a stressful situation for parents. The reviewed trial of parenting programs on preventing AHT focuses on the use of an emotional self-regulated strategy (i.e., self-talk) to cope with inconsolable crying. Meanwhile, literature has shown that programs using a professional-guided approach to emotional regulation reduce parents’ stress or emotional difficulties (Lopes & Williams, 2018). Unlike a self-guided approach, the professional-guided approach of emotional regulation with more doses or times for parents’ training showed an effective result on parents’ emotional regulation to alleviate their stress (Lopes & Williams, 2018). Nevertheless, the use of a self-regulated strategy to train parents can be a time-saving option for professionals and researchers. Future research may want to compare and examine the underlying pathways for these two approaches to parents’ emotional regulation in response to inconsolable crying.
Delivery Components
Most included trials applied a one-on-one session (17 out of 18 studies) and delivered once (16 out of 18 studies) for participating parents, except for two state-wide/province-wide programs. The previous review by Lopes and Williams (2018) indicated that parenting programs on the awareness of AHT were simpler and cost lower than the other two types of initiatives of AHT prevention, including the reduction of the quantity of infant crying and the parental stress and emotional difficulties. In order to increase the accessibility, state-wide or province-wide parenting programs aimed to reduce the AHT incidence rate provided standardized training for healthcare providers who delivered the program and used individualized sessions for the parents (Altman et al., 2011; Barr et al., 2018; Dias et al., 2005, 2017; Zolotor et al., 2015). The two state-wide/province-wide programs administrated a three-dose parenting program for public education through a media campaign with paid radio commercials (Zolotor et al., 2015) or a volunteering campaign with a purple knit cap for preventing AHT (Barr et al., 2018). In view of the remaining parenting programs that focused on the outcomes of knowledge and behavior (i.e., safe coping strategies and emotional self-regulation), all of them were delivered once; the intervention effects on knowledge were better than that on behavior. Literature has shown that more dosages of parenting programs to prevent child abuse are related to fewer children’s behavioral problems (Fang et al., 2022). Future parenting programs on preventing AHT can apply more doses of intervention and examine its effects on parents’ behavioral change through the use of safe coping strategies and emotional self-regulation.
Strengths and Limitations
This review is the first attempt to quantitatively synthesize evidence of the effectiveness of parenting programs on AHT prevention. Randomized trials and quasi-experiments were selected, and critical appraisals were conducted to ensure the quality of the included studies. However, a few limitations of this review warrant discussion. First, a high level of heterogeneity and a limited number of included studies in this review might reduce the precision and statistical power of the meta-analyses. Although the sensitivity and subgroup analyses were applied whenever possible to ensure the results were robust, these results should be carefully interpreted. Second, only studies written in English and Mandarin were included and analyzed, which might have limited the comprehensiveness of this review along with language bias. Further, only four studies related to AHT preventive intervention written in Japanese, Spanish, and Germany were found but excluded because of their study design (i.e., only a single group, post-test or pre-post design). Another limitation is that the analysis for publication bias was not performed due to the small number of studies. Lastly, unrecognized or uncontrollable confounding factors in included quasi-experiments can also affect the results. Therefore, the findings of the meta-analyses should be interpreted with caution.
Implications for Practice and Research
This review supports the use of parenting programs on preventing AHT as routine health education for expectant parents and parents of newborns at maternity, child, and/or family health care units and primary care clinics, as well as the community health and social care services for families with infant and young children. However, preventing AHT might need to go beyond improving parental knowledge and teaching them to use safe strategies in response to infants’ inconsolable crying. Due to the insignificant impact of parenting programs on the reduction of AHT incidence rates or parental emotional distress, they are suggested to support parental emotional distress and address the issues of the social and economic context of the family. AHT prevention strategies should focus on the “context” of the family (economic, basic needs, social support, and social capital) apart from parents’ knowledge.
Further research can focus on the effect of parenting programs in reducing the incidence rate of AHT by adjusting covariates to mitigate the potential bias in using controls from patient registries or medical charts. In order to resolve the power reduction problem caused by small sample sizes for AHT cases (Zolotor et al., 2015), future studies may use Trial Sequential Analysis to enhance the precision and power of the estimation of intervention effect (Wetterslev et al., 2017). The required sample size for further trials can also be determined by Trial Sequential Analysis to get a firm conclusion regarding the effectiveness of the AHT preventive interventions (Claire et al., 2020). In addition, because none of the included RCTs and quasi-experiments were rated as low risk of bias in this review, rigorous and well-designed research to mitigate the bias is required in the future. Development and validation of a gold standard measure or a core outcome set will be useful to assess the parents’ knowledge of AHT and safe coping strategies and emotional self-regulation in response to inconsolable crying. Accurate information about program performance can be obtained and compared across studies from different countries. Further investigations about the effects of preventive interventions on improving parents’ competence to handle inconsolable crying and the mechanism among knowledge, soothing strategies, emotional self-regulation, and the reduction of the occurrence of AHT are warranted. Table 2 summarizes the implications of this review for practice, policy, and research.
Summary Table of Implications for Practice, Policy, and Research.
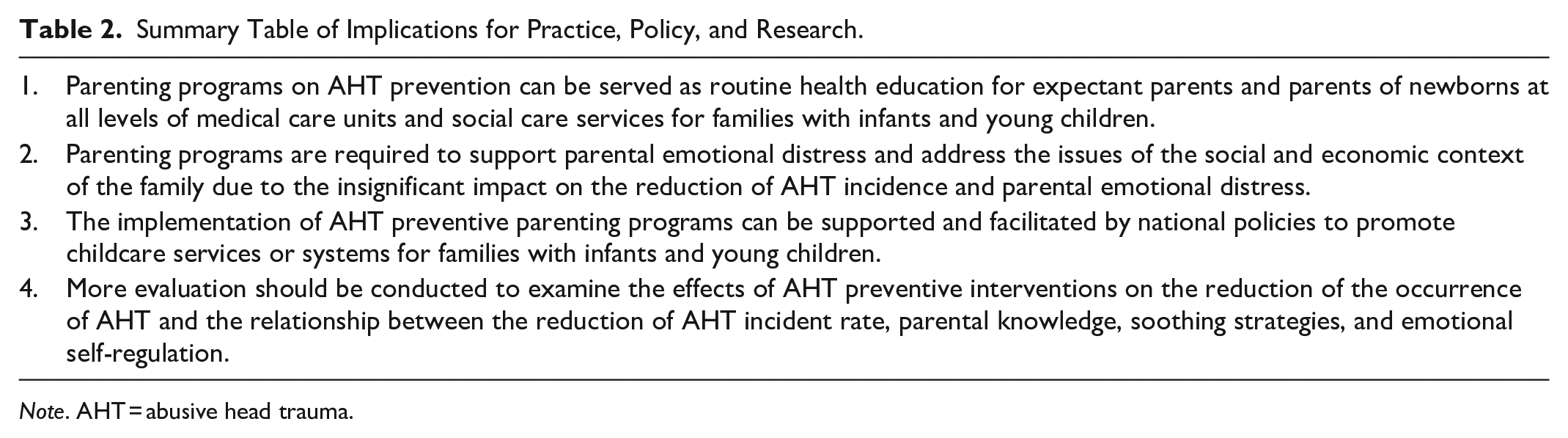
Note. AHT = abusive head trauma.
Conclusion
Parenting programs on preventing AHT can improve parental knowledge of infant crying, the dangers of shaking, and the use of safe coping strategies in response to infant crying. The effect of parenting programs on reducing AHT incidence varies across research designs and appears to be undetermined. This review contributes to drawing a generalizable conclusion to strengthen the evidence base for the effects of AHT preventive parenting programs on increasing parenting competence to provide safe care for infants. Moreover, losing lives and health due to AHT is not inevitable. It is important to incorporate AHT prevention concepts into public health and child welfare policies to create a safe and protective net for children.
Supplemental Material
sj-pdf-1-tva-10.1177_15248380231151690 – Supplemental material for The Effectiveness of Parenting Programs in Preventing Abusive Head Trauma: A Systematic Review and Meta-Analysis
Supplemental material, sj-pdf-1-tva-10.1177_15248380231151690 for The Effectiveness of Parenting Programs in Preventing Abusive Head Trauma: A Systematic Review and Meta-Analysis by Hsin-Yi Chang, Yu-Chun Chang, Yi-Ting Chang, Yi-Wen Chen, Pei-Yu Wu and Jui-Ying Feng in Trauma, Violence, & Abuse
Supplemental Material
sj-pdf-2-tva-10.1177_15248380231151690 – Supplemental material for The Effectiveness of Parenting Programs in Preventing Abusive Head Trauma: A Systematic Review and Meta-Analysis
Supplemental material, sj-pdf-2-tva-10.1177_15248380231151690 for The Effectiveness of Parenting Programs in Preventing Abusive Head Trauma: A Systematic Review and Meta-Analysis by Hsin-Yi Chang, Yu-Chun Chang, Yi-Ting Chang, Yi-Wen Chen, Pei-Yu Wu and Jui-Ying Feng in Trauma, Violence, & Abuse
Supplemental Material
sj-pdf-3-tva-10.1177_15248380231151690 – Supplemental material for The Effectiveness of Parenting Programs in Preventing Abusive Head Trauma: A Systematic Review and Meta-Analysis
Supplemental material, sj-pdf-3-tva-10.1177_15248380231151690 for The Effectiveness of Parenting Programs in Preventing Abusive Head Trauma: A Systematic Review and Meta-Analysis by Hsin-Yi Chang, Yu-Chun Chang, Yi-Ting Chang, Yi-Wen Chen, Pei-Yu Wu and Jui-Ying Feng in Trauma, Violence, & Abuse
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Science and Technology [Grant number: 108-2813-C-006-138-B]
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.