
Abstract
The specific relationship between sexual coercion, intimate partner violence (IPV) during pregnancy, and intimate partner homicide (IPH) is poorly understood. Through a scoping literature review, we identified 101 studies on sexual coercion, IPV during pregnancy, and IPH and created a conceptual model suggesting unintended pregnancies may serve as both a risk factor for and a product of IPV that may escalate to IPH. We illustrate a healthcare systems intervention implication of this model in the context of the Colorado Family Planning Initiative (CFPI). Descriptive statistics suggest an inverse association between contraception access and IPH, which declined by 62% during the first 4 years of the CFPI. Interventions aimed at improving reproductive agency, including improving contraception access and reducing unintended pregnancy, may be a useful opportunity for clinician and health systems to contribute to reducing both lethal and nonlethal IPV.
Background
The Center for Disease Control and Prevention (CDC) reports that approximately one in four women have experienced a form of intimate partner violence (IPV) (Smith et al., 2018). IPV encompasses a variety of controlling behaviors including sexual coercion. Sexual coercion is an unwanted sexual contact that occurs as a result of pressure, intimidation, manipulation, or power imbalance (American College of Obstetricians and Gynecologists [ACOG], 2013). Some studies estimate that up to 59% of women have experienced sexual violence from an intimate partner (Mikton, 2010). In addition to sexual assault and rape, violent partners may use discreet strategies to sexually coerce their partners. Perpetrators of IPV may tamper with contraception or impair a woman’s ability to have protection during sex, ultimately resulting in an increased risk for unplanned pregnancy (Maxwell et al., 2018). Fear of violence frequently eliminates a woman’s autonomy over contraception use; rates of unplanned pregnancy are 30% higher among women experiencing IPV (Maxwell et al., 2018).
Becoming pregnant is a key risk factor for increased violence (Cliffe, 2018), including escalation of frequency and severity of abuse. The risk of violence during pregnancy is increased if the pregnancy is unintended (Shoffner, 2008). While many studies have reported homicide as one of the leading causes of death among pregnant women (Cliffe, 2018), it is unclear how sexual coercion influences the risk of lethal violence. Further unpacking of the relationship between sexual coercion, IPV, and intimate partner homicide (IPH) may lead to promising avenues for intervention. Because contraception, pregnancy, and childbirth are generally managed medically in the United States, we focus especially on opportunities for clinicians and health systems to intervene, while recognizing that these systems cannot be disentangled from others, such as legal and economic systems.
The purpose of this study is to use a scoping literature review to build a conceptual model to understand the interrelatedness of three key themes: (1) sexual coercion, (2) IPV during pregnancy, and (3) escalation of severity of IPV to lethal violence. This review also aims to identify potential avenues for intervention based on this model within the context of the United States healthcare system. Reproductive healthcare in the United States is highly politicized and access to contraception and abortion is impacted as a result of local and federal policies, creating a unique environment in which these factors interplay with IPV and sexual coercion. We illustrate this conceptual model by employing a secondary analysis of IPH data through the National Violent Death Reporting System (NVDRS) in Colorado during the timeline of the Colorado Family Planning Initiative (CFPI), which has previously been shown to have significantly reduced unintended pregnancy rates in Colorado (Colorado Department of Public Health and Environment, 2017).
Methods
Literature Search
This study used a scoping literature review following the methods described by Arksey and O’Malley (2005). PubMed, PsycINFO, and Cumulative Index of Nursing and Allied Health Literature were searched using a combination of keywords (and MeSH search terms in PubMed) that would encompass terms closely related to IPV, IPH, and sexual coercion. Search terms were developed to identify areas of overlap in these topics in the existing literature. For example, we used search terms including (“intimate partner violence” OR “domestic violence”) AND (“pregnancy” OR “pregnancy, unplanned” OR “pregnant”) AND (“homicide” OR “murder”). These database searches were performed in June to July 2020 with an additional search in December 2020 using terms including “sexual coercion,” “contraception,” and “intimate partner violence” to specifically gather additional literature on sexual coercion as the original search did not produce substantial results related to sexual coercion. Search terms were developed in consultation with a medical librarian.
Eligibility Criteria
All articles obtained through the search terms were reviewed by title and abstract by a single reviewer for eligibility using the systematic review web-tool, Rayyan. Studies were included if they met the following criteria: (1) the study took place in the United States, (2) the article was accessible in English, (3) the article was published in a peer-reviewed journal, (4) the article focused on any of the following topics: IPV during pregnancy, IPV and sexual coercion, or IPH (both pregnancy-associated and non-pregnancy-associated). Although our intent was to identify articles that discussed overlap of these themes, there were zero studies that addressed all three themes which required us to broaden our inclusion criteria to capture the existing overlap in the literature and further elucidate these themes. The consequence of this search and inclusion strategy is that we here review the literature on IPH that appeared in this pregnancy-related search (even if the article itself was about non-pregnancy-associated IPH), but we do not comprehensively review all the literature that exists on IPH outside of our search.
In order to develop a conceptual model related to these key themes, studies were not limited based on design or methodology. Literature reviews and systematic reviews were included in order to thoroughly explore all relevant models of peer-reviewed articles related to these themes, as supported by the Joanna Briggs Institute (Peters et al., 2015). Articles that discussed intervention strategies to reduce sexual coercion, IPV, and IPH were also included in this study to further elucidate the overlap of these forms of violence and comment on potential avenues for intervention within the development of the conceptual model. Studies were also not excluded based on date of publication.
Studies were excluded if their primary focus involved populations within countries outside of the United States. Studies were also excluded if they described infant or maternal obstetric outcomes from a pregnancy that involved IPV or were political or ethical commentary pieces.
Data Extraction
Data were extracted from all articles reviewed in full text for the following: population, study design, measures, and outcomes with descriptive findings. Additionally, articles were categorized by major theme(s): (1) sexual coercion, (2) IPV and pregnancy, and/or (3) IPH (both pregnancy-associated and non-pregnancy-associated).
Colorado National Violent Deaths Reporting System
We also performed a secondary analysis of IPHs in Colorado during the CFPI from 2009 to 2014 using the NVDRS Web-Based Injury Statistics Query and Reporting System. From 2009 to 2015, the CFPI program provided free and low-cost long-acting reversible contraceptives (LARCs) to low-income women. The program resulted in a cumulative total of 36,762 LARC insertions, alongside declining statewide fertility rates (48% decrease), abortion rates (47% decrease), and unintended pregnancy rates (40% decrease) for women aged 15 to 19 years old (CDPHE, 2017). Colorado was used as a model state due to the novel statewide approach of the CFPI and the lack of sizable data from other similar programs. The NVDRS reports data on the number of deaths, population size, crude death rate per 100,000, and age-adjusted death rate for select states. We collected data on homicides completed by a spouse or other intimate partner (current or ex) by any mechanism of injury or manner of death in Colorado between 2009 and 2014. We also used the NVDRS to obtain data on non-intimate partner violent deaths in Colorado over the same time period. These data were analyzed descriptively due to being available as aggregate information, and no inferential statistical analyses were performed.
Results
Study Selection
We identified 884 articles based on our initial search terms. After removing duplicates, 642 articles remained and were reviewed by title and abstract. Upon initial title and abstract review, 81 articles were included and reviewed in full text and 69 met eligibility criteria to be included in this study. Common reasons for exclusion included a focus on maternal and infant mortality unrelated to IPV and studies taking place outside the United States. Our search terms resulted in minimal identification of studies relating to sexual and reproductive coercion. Following an iterative scoping strategy, an additional search was completed with more precise terms related to sexual and reproductive coercion. From this search, an additional 38 articles were identified and reviewed by title and abstract. After full-text review, 32 met inclusion criteria. In total, our combined searches identified 922 articles and included 101 (Figure 1).
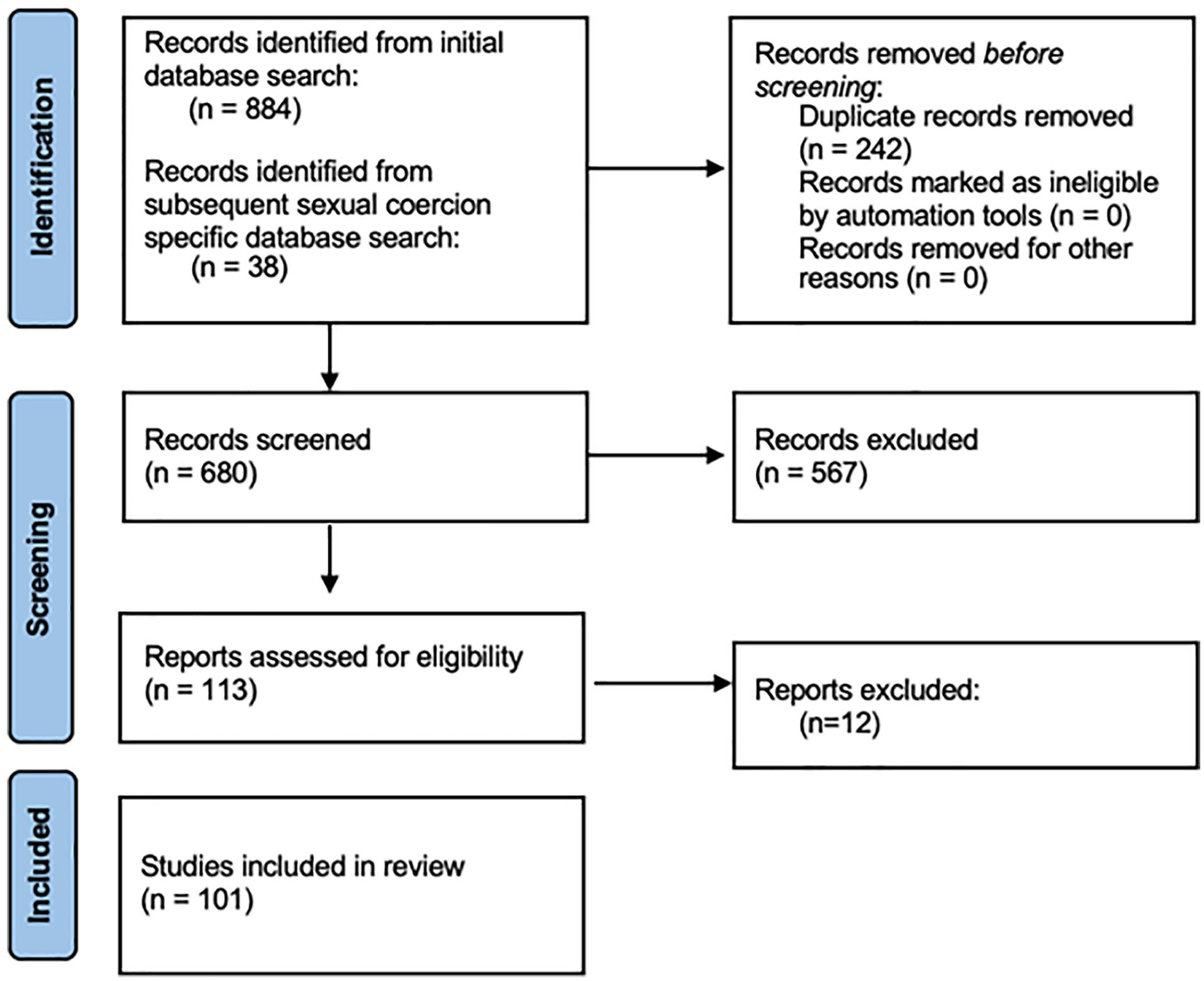
PRISMA flow chart for articles included in this study.
Study Designs and Characteristics
The included studies had a variety of focuses and study designs, most commonly literature reviews, retrospective analyses of IPH cases from a variety of U.S. states, and surveys or self-reports from IPV survivors (Table 1). Included studies were categorized based on main focus: IPV during pregnancy, IPH (both pregnancy-associated and non-pregnancy-associated), and/or sexual coercion. While IPV during pregnancy frequently overlapped with discussions on IPH, many articles had a single focus, and none of the identified articles connected all three themes together (Figure 2).
Study Design of Included Articles.
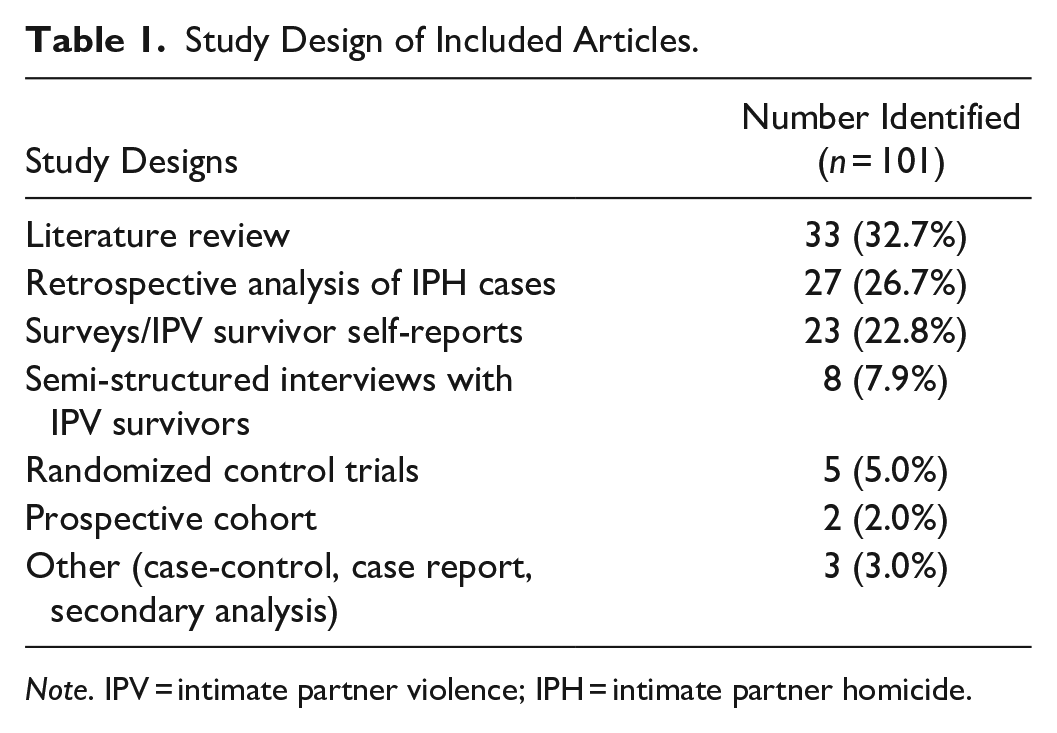
Note. IPV = intimate partner violence; IPH = intimate partner homicide.
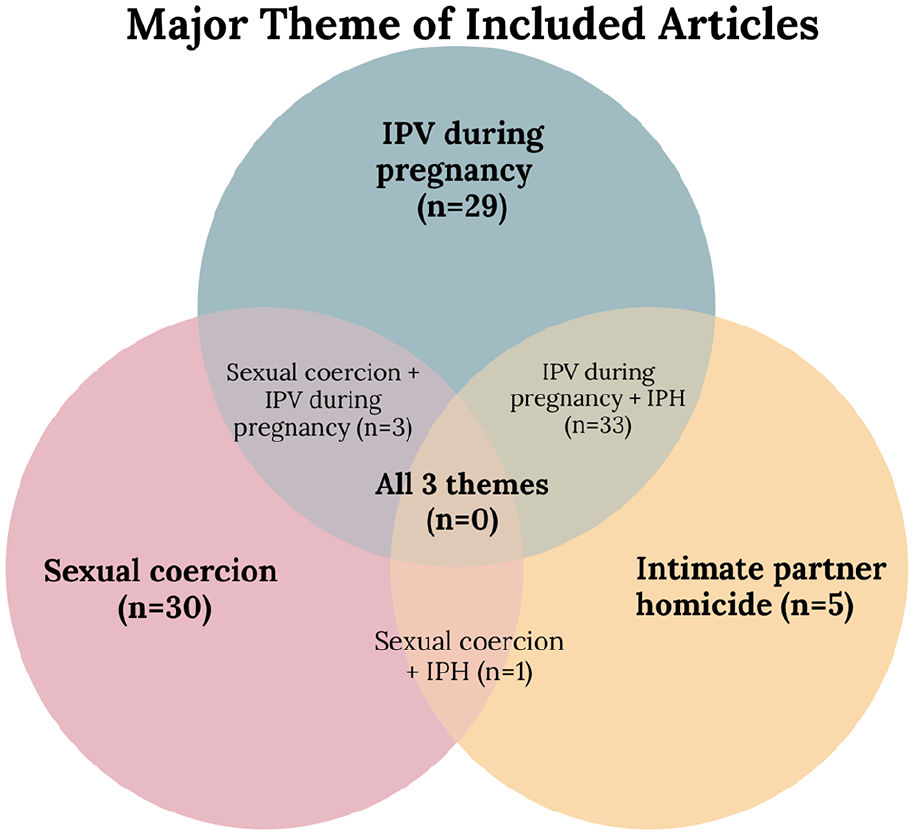
Major theme of included articles.
Sexual and Reproductive Coercion
The American College of Obstetricians and Gynecologists defines sexual coercion as unwanted sexual contact that occurs as a result of pressure, intimidation, manipulation, or power imbalance (ACOG, 2013). Reproductive coercion refers to “behavior that interferes with contraception use and pregnancy,” which may include tampering with contraception or interfering in abortion access (ACOG, 2013).
Sexual Coercion and Unintended Pregnancy Risk
Previous reviews concur that IPV impacts a woman’s sexual autonomy and contraception behaviors and increases the risk for unintended pregnancy (Coggins & Bullock, 2003; Espinosa & Osborne, 2002; Sarkar, 2008; Taylor, 2012), and find that women experiencing IPV were less likely to be on highly effective methods of contraception and were more likely to depend on less effective methods or no method at all (Maxwell et al., 2015). Interviews with women experiencing IPV found that violent partners would interfere in their partner’s reproductive autonomy by “controlling, forcing, or coercing” choices about their reproductive health (O’Connor-Terry et al., 2022). Women also reported that their partners have interfered in their ability to take birth control pills by attempting to destroy them or refusing to use condoms consistently (Katz & Sutherland, 2020). In a survey in Boston, 12% of 14 to 20 years old participants stated they have been afraid to request that their partner use a condom, most often for fear that they will be accused of cheating or that their partner will threaten to have sex with someone else (Silverman et al., 2011). The impact of IPV on reproductive autonomy is further elucidated by the experience of women in abusive relationships seeking abortion services. Some studies report that women in violent relationships are more likely to seek abortion services without consulting their partner (Hall et al., 2014). Furthermore, women seeking to terminate their pregnancy without partner knowledge were nearly three times more likely to be experiencing IPV according to one review (Maxwell et al., 2015).
Sexual Coercion and Other Forms of IPV
When reproductive coercion is present in a relationship, 75% of women reported other types of IPV (Chisholm et al., 2017). In a study of women seeking care at obstetric and gynecologic clinics, 8.6% reported that reproductive coercion was involved in their most recent pregnancy; women reporting reproductive coercion were nearly three times more likely to report additional forms of IPV—including physical and sexual violence and threats of violence—than women who did not report reproductive coercion (Fay & Yee, 2020). Sexually coercive behaviors may increase the risk of unintended pregnancy and further increase the risk of IPV as abuse may escalate in frequency and severity during pregnancy (Taylor, 2012), and particularly during unintended pregnancies (Aretakis, 2008). Unintended pregnancy may increase the risk of IPV up to fourfold (Gazmararian et al., 1995; Shoffner, 2008). Sexual coercion may also predict the frequency and severity of abuse; sexual coercion is associated with an increased risk of completed strangulation among women experiencing IPV, and experiencing multiple strangulation attempts significantly increased the risk of homicide (Messing et al., 2018).
Intimate Partner Violence During Pregnancy
Prevalence
The prevalence of IPV during pregnancy in the United States may be as high as 20% of all pregnancies (Chisholm et al., 2017; Morrison et al., 2022). However, the proportion of IPV during pregnancy that is detected varies widely depending on screening tools used and the population demographics. Some studies report rates of IPV during pregnancy to be between 3% and 8% of all pregnancies (Chisholm et al., 2017; Cox et al., 2004; Poole et al., 1996). Due to overall low rates of universal IPV assessment in medical settings, it is likely that the incidence of IPV during pregnancy is underreported.
Demographics and risk factors
Rates of IPV among pregnant women are particularly high among women who are young, unmarried, have lower education levels, and women of color. Both individual studies and reviews have repeatedly found that pregnant teens and young adults are at a significantly increased risk of experiencing IPV during pregnancy compared to older adults (Chambliss, 2008; Lipsky et al., 2003; Mackey, 1993; Stadtlander, 2018). Additionally, younger women of color are more likely to experience IPV during pregnancy than young White women (Bullock et al., 2006; Deshpande et al., 2017), and women with less than 12 years of education are at a four times increased risk of experiencing IPV during pregnancy (Chisholm et al., 2017; Lipsky et al., 2004). However, increasing educational attainment alone may not be a protective factor; women who have a higher education than their male partners are nearly 10 times more likely to be killed by their partner than women with equal education as their partner (Taylor & Nabors, 2009).
Forms of IPV during pregnancy
IPV may begin or escalate in frequency and severity during pregnancy. Many studies identified pregnancy as a high-risk time for increased severity of IPV (Bronson & Reviere, 2017; Chang et al., 2005; Geller, 2017; Hawkins, 2002; Kavanaugh & Miller, 2012; Koch & Campbell et al., 2007; Matias et al., 2020).
A study of assaults during pregnancy in emergency departments throughout Pennsylvania found that the prevalence of assault was nearly twice as high for pregnant women than nonpregnant women (Deshpande et al., 2017). In a sample of pregnant Hispanic women, over 20% reported forced or coerced sex, 33% reported having been kicked, 40% had been punched, and 30% reported that their partner threatened to kill them (Wiist & McFarlane, 1998). Other studies have identified differences in the locations of physical assaults among pregnant and nonpregnant women. Specifically, studies have identified that physical assaults during pregnancy were more often directed toward the breast, abdomen, and torso, rather than the head and neck as are most common among nonpregnant women (Bohn, 1990; Chambliss, 2008; Nannini et al., 2008; Taylor, 2012). Taylor (2012) proposed that assaults to the abdomen may indicate the “sense of ownership” abusive partners feel over their victims, and that these controlling and jealous behaviors may lead to feeling threatened by a pregnancy and induce escalation of severity to lethal violence. Regarding access to lethal means, a sample of 199 pregnant IPV survivors found that 41% of their abusers had access to a firearm, and survivors whose partner had access to a gun were more likely to report experiencing physical and non-physical violence and threats of violence (McFarlane et al., 1998).
Additionally, abuse during pregnancy is associated with an increased risk of IPH (Campbell et al., 2007; Matias et al., 2020). IPV during pregnancy is one of the strongest predictors of IPH; victims who are abused during pregnancy are over three times as likely to be murdered by their partner (Matias et al., 2020), and women killed or nearly killed by their intimate partner are more likely to have been abused during pregnancy (Campbell et al., 2007; McFarlane, 2002). For these reasons, abuse during pregnancy is frequently reported as an independent risk factor for IPH (Campbell, 1999; McFarlane, 1995).
Pregnancy-Associated IPH
Prevalence
Pregnancy-associated deaths are defined as maternal death during pregnancy or within 1 year postpartum due to any cause (Creanga et al., 2014). The studies included in our search frequently identified IPH as a leading cause of death among pregnant and postpartum women (Bronson & Reviere, 2017; Chang et al., 2005; Hawkins, 2002; Kavanaugh & Miller, 2012; Koch & Geller, 2017). While a minority of studies and reviews reported similar rates of IPH among nonpregnant and pregnant women (Decker et al., 2004; Samandari et al., 2010, 2011), other research has found a sizeable difference in IPH risk among pregnant women. Generally, studies report between 11% (Wallace et al., 2016) and 900% (Koch et al., 2016) increased risk of IPH during pregnancy and in the postpartum period, with greater risks identified in women aged 10 to 29 years (200% increased risk) and Black women (900% increased risk) (Koch et al., 2016). Some scholars (Shadigian & Brauer, 2005) raise the concern that underreporting of pregnancies on death certificates due to lack of examinations of the uterus or blood pregnancy tests may obscure true rates of pregnancy-associated deaths (Dannenberg et al., 1995; Krulewitch et al., 2001 Shadigian & Brauer, 2005), further suggesting rates of IPH may not be similar between pregnant and nonpregnant women.
Risk factors
Risk factors for IPH—irrespective of pregnancy status—are well documented. These risk factors include a prior history of IPV, young age (Krulewitch et al., 2001; Shadigian & Brauer, 2005; Wallace et al., 2016), unmarried status (Austin et al., 2016; Campbell et al., 2003; Krulewitch, 2009), separation from the abuser (Campbell et al., 2003), perpetrator access to firearms (Matias et al., 2020), unemployment (Campbell et al., 2003), and low socioeconomic status (Aretakis, 2008; Campbell et al., 2003; O’Reilly, 2007; Sharps et al., 2001). Separation from an abusive partner is associated with over a three times increased risk of IPH and the combination of an excessively controlling partner and separation after having lived together accounted for a ninefold increased risk of IPH (Campbell et al., 2003).
Risk factors identified for pregnancy-associated IPH are often similar to those of non-pregnancy-associated IPH, including younger age (Krulewitch et al., 2001; Shadigian & Brauer, 2005; Wallace et al., 2016), unmarried status (Austin et al., 2016; Krulewitch, 2009), non-white (Bronson & Reviere, 2017; Chang et al., 2005), estrangement from the father of the child (Bronson & Reviere, 2017). Controlling, jealous traits in an abusive partner increases the risk for pregnancy-associated IPH and attempting to leave the abuser may exacerbate this risk (Adhia et al., 2019; Cliffe et al., 2019; Decker et al., 2004).
Risk throughout pregnancy
Hospital visits for IPV during pregnancy tend to be highest during the first trimester and the first year postpartum (Nannini et al., 2011). Over half of pregnancy-associated homicides in the United States between 1991 and 1999 happened after a live birth (Chang et al., 2005). Recent reviews of statewide pregnancy-associated homicides in Illinois (Koch & Geller, 2017), Massachusetts (Martin et al., 2007), and North Carolina (Austin et al., 2016) indicated these homicides predominantly took place in the postpartum period, and often more than 1 (Koch & Geller, 2017) to 6 months (Austin et al., 2016) postpartum.
Timing of prenatal care
Prenatal care emerges as a notable theme in the study of IPH. Although studies consistently report that prenatal care represents a crucial opportunity for intervention of violence and lower acquisition of prenatal care is associated with higher risks of violence and IPH (Chang et al., 2005; Cheng & Horon, 2010), multiple studies also made note that between 49% (Chang et al., 2005) and 70% (Cheng & Horon, 2010) of victims of pregnancy-associated homicide had secured prenatal care in their first trimester. In a review of pregnancy-associated deaths in the United States between 1991 and 1999, nearly half of pregnancy-associated homicide victims had secured prenatal care in their first trimester of pregnancy, however, women who had no prenatal care were at a two to three times increased risk of homicide (Chang et al., 2005). A review of pregnancy-associated homicides in Maryland between 1993 and 2008 found over 70% of homicide victims had begun care during the first trimester, yet IPH was still most prevalent during this time (Cheng & Horon, 2010). Other studies found that women experiencing IPV were twice as likely to begin prenatal care in the last trimester of pregnancy, and that IPV was the highest at 3 months postpartum (McFarlane et al., 1992; Shadigian & Bauer, 2004). Women who received early prenatal care had the lowest mortality rate (Chang et al., 2005).
Intervention strategies
Research has considered the ability for healthcare provider intervention to prevent IPH. Reviews suggest that commonly used strategies have included universal screening for IPV throughout a pregnancy and referrals to local resources (Parker & McFarlane, 1991). However, a more recent review of 10 randomized control trials for interventions to reduce IPV during and after pregnancy found that none resulted in a significant reduction of abuse (Jahanfar et al., 2014).
Women experiencing IPV have increased barriers to accessing confidential and affordable healthcare and may fear retaliation if they disclose the abuse. In a study of survivors of strangulation by an intimate partner, 7% of victims lied to medical providers when questioned about the assault to protect the abuser, for fear of ongoing or increasing abuse (Shields et al., 2010). A review (Shoffner, 2008) found that women preferred self-completed written IPV screenings, rather than face-to-face screenings completed with healthcare providers, indicating preferences of delivery of the screening questions could impact willingness to disclose. Although not the majority preference, face-to-face interactions with healthcare providers do play a role. In Philadelphia, more than half of IPH victims had sought medical care within 1 month prior to the homicide (Mehta et al., 2016), and in a review of IPH in North Carolina between 1992 and 1994, in one-third of IPHs the obstetric provider was suspicious or knew the patient was experiencing IPV (Parsons & Harper, 1999).
Discussion: A Conceptual Model of IPH in Pregnancy
Our study aimed to provide a scoping review of the interrelatedness of sexual coercion, IPV during pregnancy, and risk of IPH. We identified 101 articles that discussed these themes through varying perspectives, including literature reviews, surveys, autopsy reports, and semi-structured interviews. Many articles connected themes of IPV during pregnancy and IPH, or IPV and sexual coercion. Although the connection between the three may seem self-evident, none of the articles we reviewed addressed all three together. The conjunction of these themes may provide crucial insight to further address IPV and the risk of IPH.
Our review suggest that sexual coercion is highly associated with other forms of IPV (Chisholm et al., 2017) and increases the risk of unintended pregnancy (Espinosa & Osborne, 2002; Sarkar, 2008; Taylor, 2012). Moreover, sexual coercion may indirectly increase the risk of future victimization through the increased probability of pregnancy, which is widely regarded as a high-risk time for onset or increased severity and frequency of abuse (Bianchi et al, 2014; Koch et al., 2016; McFarlane et al., 2014). Women who are younger, unmarried, and nonwhite are at increased risk for experiencing IPV during pregnancy (Chambliss, 2008; Lipsky et al., 2003; Mackey, 1993). Importantly, unintended and mistimed pregnancies significantly increase the risk of danger and progression to lethal abuse (Shoffner, 2008). Programs like the CFPI that have aimed to provide access to reproductive healthcare to low-income women have previously demonstrated efficacy at reducing unintended pregnancy and abortions (CDPHE, 2017).
Our review suggests that violence may escalate in IPV relationships at least in part related to loss of reproductive autonomy associated with sexual and reproductive coercion, suggesting that interventions like the CFPI may confer benefits to women in IPV relationships by increasing access to reproductive healthcare.
We therefore propose a single conceptual model elucidating the link between sexual coercion and IPH, and the mechanism by which LARC may reduce IPH risk by interrupting the pregnancy consequences of sexual coercion, a common component of IPV (Figure 3). This model integrates these themes and suggests that unintended and mistimed pregnancies may serve as both a risk factor and product of IPV, and that IPV may begin or escalate in frequency and severity during pregnancy further increasing the risk for escalation to IPH. Through this model, reducing unintended pregnancy may be used as an approach for intervention to reduce both lethal and nonlethal IPV.
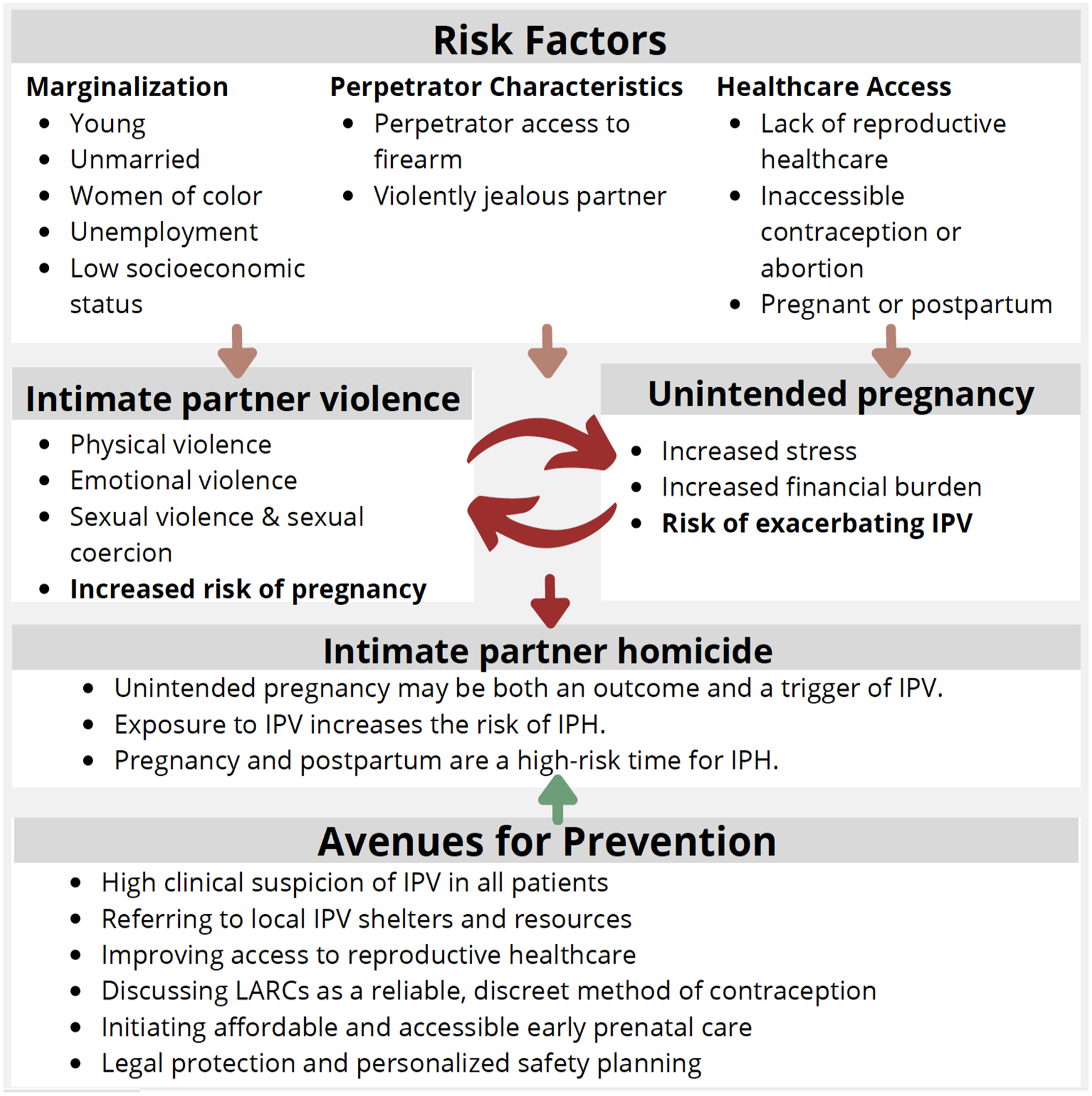
Unintended pregnancy can be thought of as both an outcome and a trigger for intimate partner violence (IPV). Exposure to IPV significantly increases the risk of intimate partner homicide (IPH). Using this model, both IPV and unintended pregnancy can be used as a point for advocacy to reduce mortality.
Our review supports that the standard methods for intervention (i.e., universal screening) frequently yields low results due to a variety of barriers including the provider’s lack of time or knowledge on the subject, lack of privacy, unfamiliarity with local IPV resources, or the victim’s fear of increased violence if their partner finds out (Clements et al., 2011; Stonard & Whapples, 2016). Additionally, even when IPV is detected and a referral to resources are completed, risk of violence may prevent victims from accessing services, and the increased risk of abuse when a victim attempts to leave a violent relationship could cause further damage and potentially increase the risk of homicide (Adhia et al., 2019; Campbell et al., 2003; Cliffe et al., 2019; Decker et al., 2004). Moreover, some studies found that the single strongest sociodemographic factor of IPH perpetration is unemployment, suggesting that income inequality may contribute to violence, and that a pregnancy may exacerbate these financial concerns, increasing the likelihood of homicide (Aretakis, 2008; Campbell et al., 2003; O’Reilly, 2007; Sharps et al., 2001). Our review suggests that additional avenues for intervention are necessary to more holistically address the diverse needs of IPV victims. Some of these avenues could include advocating for increased access to confidential and discreet contraception and reproductive healthcare, increasing job opportunities and financial stability, and educating healthcare providers to create unique safety plans for patients experiencing IPV, as encouraging victims to leave the relationship may actually serve to increase risk of homicide.
In particular, our findings highlight that addressing unintended pregnancies may serve as a potential route for intervention to reduce IPV and IPH. Although research related to this connection is limited, we investigated this relationship by evaluating the rate of IPH in Colorado during the CFPI, a novel statewide approach that provided low- and no-cost LARCs to low-income women.
Between 2009 and 2015, the CFPI offered low- and no-cost LARC, including intrauterine devices and contraceptive implants, to low-income women seeking reproductive healthcare services (CDPHE, 2017). These forms of contraception are discrete, tamper-resistant, and do not require coordinated efforts between sexual partners in order to be effective. Given this, LARCs are a method of contraception that may have particular utility for individuals experiencing IPV or sexual coercion. The Colorado Department of Public Health and Environment has previously reported that the rate of unintended pregnancy declined by 40% during the time period of this program (CDPHE, 2017). We collected data of IPH in Colorado reported to the NVDRS over the same time period, which indicated that the crude rate of IPH declined from 0.66 per 100,000 at the start of CFPI in 2009 to 0.25 per 100,000 in 2012 (Figure 4). From 2012 to 2015, the IPH rates increased, following a larger trend of increasing non-IPH and violent crime in Colorado, although remaining below the average level reported in the 5 years prior to the start of CFPI.
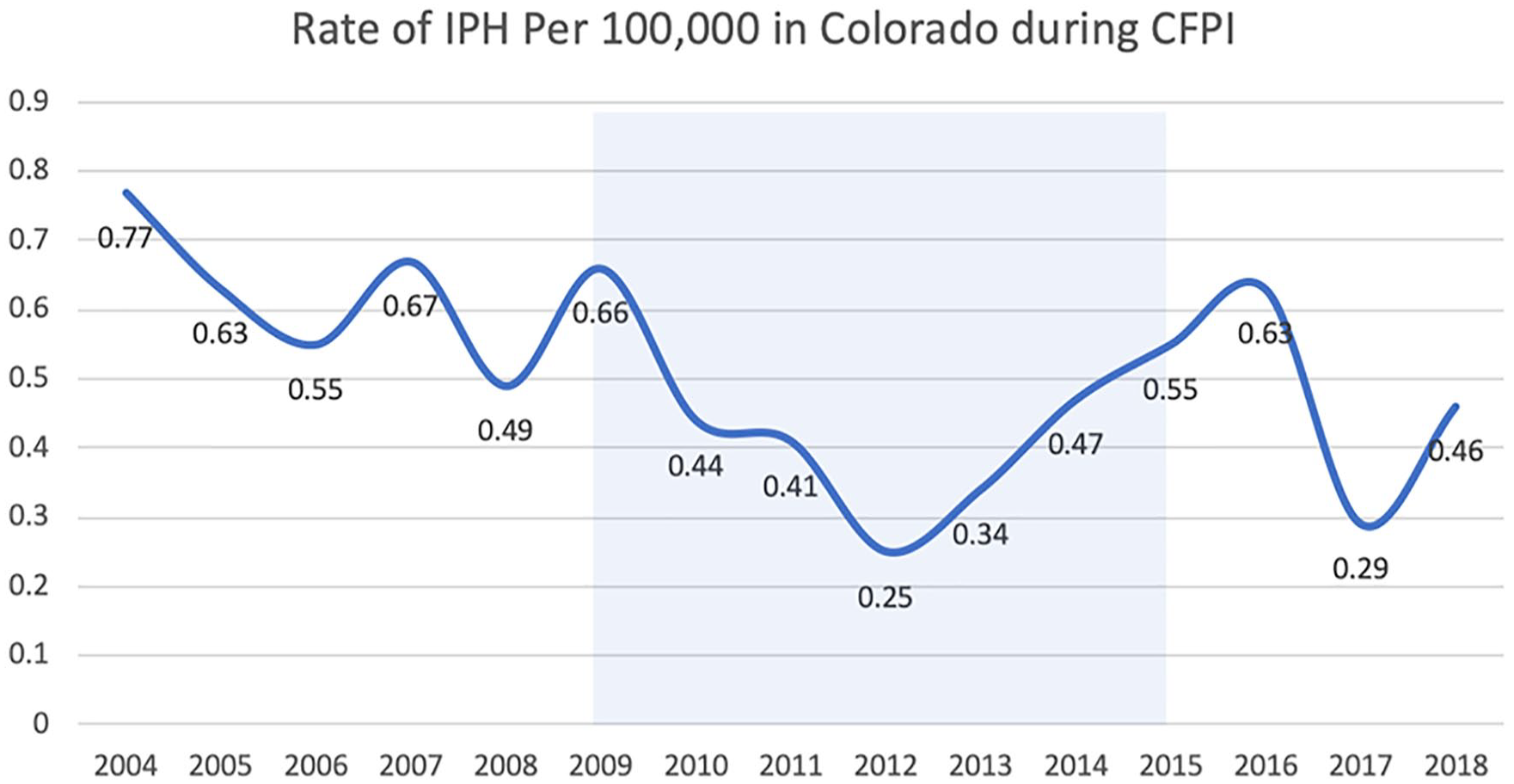
Crude rate of intimate partner homicide (IPH) per 100,000 in Colorado before, during (shaded box), and after the Colorado Family Planning Initiative (CFPI).
Prior to the CFPI program, IPH rates in Colorado were slowly declining, from 0.77 per 100,000 in 2004 to 0.67 per 100,000 in 2008. However, in the 4 years following the start of the program, Colorado saw a 62% drop in IPH, alongside a 26% drop in unintended pregnancy among women aged 15 to 19 years old. Although IPH in Colorado rose again from 2012 to 2015, this was associated with an increase in overall violent crime. Additionally, non-intimate-partner-related homicides in Colorado throughout the course of the CFPI increased, suggesting the reduction of IPH from 2009 to 2012 cannot be attributed to any generalized decrease in overall levels of homicide in Colorado.
Moreover, the CFPI specifically addressed the needs of reproductive healthcare for young low-income women, who would be most at risk for IPV involving sexual coercion, unintended pregnancy, and the possibility of escalation to lethal abuse. Given the CFPI program provided LARCs, which are a more discrete and effective method of birth control that are less prone to tampering as used in sexual coercion, it is possible that women who were experiencing or at risk for IPV were able to avoid unintended pregnancy, as the overall Colorado unintended pregnancy rate dropped by 40% throughout the program. Following our proposed framework for understanding the interconnection between these themes, it is possible that increasing reproductive autonomy and control over reproductive health care behaviors by increasing access to contraception both reduced unintended pregnancy and conferred some protection against severe or lethal IPV. This may serve as one avenue for intervention to address a complex issue that necessitates coordinated efforts between community and national social and healthcare agencies, policy changes, and wider recognition and screening for IPV and sexual coercion to effectively manage on a broad scale. Specifically, our conceptual model supports that prevention efforts must include a variety of strategies, including healthcare providers maintaining a high clinical suspicion of IPV, knowledge and access to local IPV resources, access to comprehensive reproductive healthcare and counseling, affordable and accessible prenatal care, and legal support. Access to discreet contraception may be considered as one facet of a concerted effort to simultaneously reduce risk of unintended pregnancy and reduce risk of IPV victimization.
These results are only correlational, and our data did not allow causality to be assessed. Therefore, it is necessary that future research address the connection of unintended pregnancy as a route for intervention to assess for statistical significance. Additionally, to our knowledge, the CFPI is the only program of this nature and scale in the United States to provide free and low-cost LARCs to low-income women statewide. However, similar smaller-scale programs, including the Contraceptive CHOICE Project in St. Louis, have also shown success in reducing unintended pregnancies and abortion rates, and suggest that when barriers such as access, cost, and knowledge were controlled for, women opted for highly effective and discreet contraception (McNicholas et al., 2014). Future research of similar programs may provide further insight into the connection between unintended pregnancy and impact on IPH.
The results of this scoping literature review provide a framework for connecting the impact of sexual coercion, IPV during pregnancy, and IPH on health outcomes and mortality for women experiencing or at risk for IPV. Sexual coercion is highly associated with IPV and unintended pregnancy which may further increase the risk of severe abuse that may escalate to IPH. Through our proposed theoretical model, we highlight unintended pregnancy as an opportunity for intervention that may reduce further IPV victimization or IPH. Future research should continue to explore the relationship of these themes and gather more concrete data to assess the impact of reducing unintended pregnancy on outcomes of IPV and IPH.
This study has multiple limitations. Firstly, the quality of data we collected from the NVDRS is only correlational and we are unable to infer any causality about the impact of reducing unintended pregnancy on IPH. However, we hope that this conceptual model created through the literature and secondary data analysis can provide a novel lens for viewing IPV victimization and avenues for intervention. We also experienced limitations in our search terms and required an additional search with more specific terms, indicating that we may have missed some literature relating to sexual coercion and the relationship with IPV and IPH. Additionally, because of the lack of literature connecting the themes of sexual coercion, IPV during pregnancy, and IPH together, we did not find any literature relating all of these topics together, and we were not able to perform a systematic review or meta-analysis that would have further supported the conclusions of this study. Future research should evaluate this conceptual model by directly investigating this relationship.
Conclusion
This scoping literature review indicates that sexual coercion is associated with both an increased risk of unintended pregnancy and increased severity of IPV. Moreover, pregnancy is associated with an increased risk of onset or increasing severity of IPV which contributes to higher pregnancy-associated homicide rates among this population, and this risk increases when the pregnancy is unintended or mistimed. We propose a conceptual model that interrelates these themes and highlights unintended pregnancy as a potential avenue for intervention in reducing both IPV victimization and IPH. Improving access to discrete and effective contraceptive methods and increased agency of reproductive health may interrupt the cycle in which IPV removes reproductive autonomy, increases the risk of unintended pregnancy, and further exacerbates the risk of severe and lethal violence. Implications for practice, policy, and research are summarized in Table 2.
Summary Table of Implications for Practice, Policy, and Research.
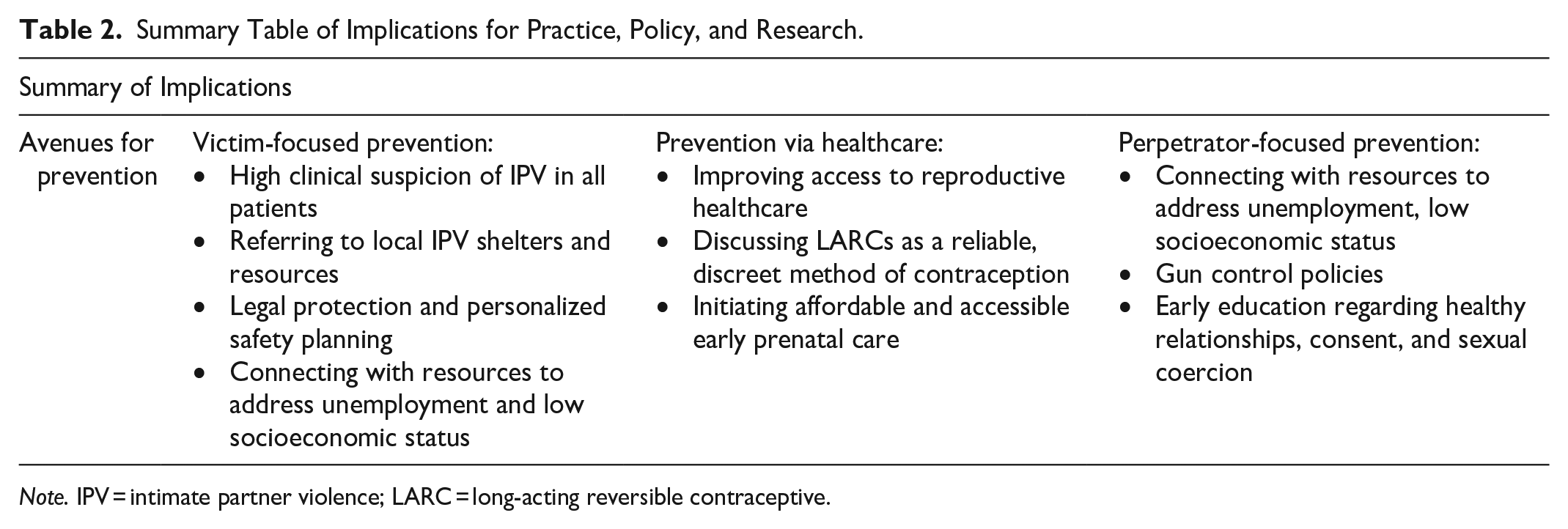
Note. IPV = intimate partner violence; LARC = long-acting reversible contraceptive.
Footnotes
Acknowledgements
Emily Joan Smith received stipend support for this work as a Central Michigan University College of Medicine Summer Research Scholar. We would like to thank the Summer Research Scholar Program for supporting this research. We would also like to thank biomedical librarian, Rebecca Renirie, for her expertise in creating search terms.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Emily Joan Smith received stipend support for this work as a Central Michigan University College of Medicine Summer Research Scholar.