
Abstract
Elder abuse is related to numerous adverse health and mental health conditions in older adults and some studies indicated higher rates of elder abuse in ethnic and racial minority populations than non-Hispanic Whites. This current study aims to summarize the risk and protective factors associated with elder abuse in community-dwelling racial minorities. A systematic review was conducted following Preferred reporting items for systematic review and meta-analysis (PRISMA) guidelines. AgeLine, Medline, PsycINFO, and CINAHL were searched without limitation on time periods of publication. Two authors independently screened the search results and assessed the eligibility and quality of the retrieved articles. A total of 718 articles were screened and 25 articles were included in the review. The 25 included studies’ publication dates range from 1989 to 2019. Five racial categories were generated: African Americans, Asian Americans, Native Americans, Hispanic Americans, and racial minorities in Canada. Risk and protective factors of elder abuse and its subtypes (e.g., physical and psychological abuse) for these racial groups were summarized. There are some common risk factors across racial minorities, such as dependence on caregivers and health issues. The review identified gaps and conflicting findings regarding culture and education that are worthy of further investigation. In particular, there is a lack of current research on elder abuse in racial minority older women, race minority subgroups, and protective factors of elder abuse. The results guide helping professionals to consider the role of traditional culture and identify warning signs of potential abuse among racial minority older adults.
Introduction
The population aged 60 or older is growing faster than any other age group worldwide and is expected to more than double by 2050 and more than triple by 2100 (United Nations, 2017). In the United States, it is predicted that one in five will be aged 65 or older by 2030, and the older population will be more ethnically and racially diverse (Colby & Ortman, 2015). However, no systematic review has summarized the risk factors and protective factors associated with elder abuse in racial minorities. Given the dramatic increase in the older population, elder abuse continues to be a growing public health and human issue in many countries. In the United States, Centers for Disease Control and Prevention reported that the direct medical costs of pain or injury associated with elder abuse are estimated to take up more than 5.3 billion dollars of the nation’s annual health expenditures, and financial exploitation alone costs older adults more than 2.6 billion dollars annually (Hall et al., 2016).
A widely accepted definition of elder abuse is “(a) actions that cause harm or create a serious risk of harm, whether or not intended, to a vulnerable elder by a caregiver or other person who stands in a trust relationship to the elder or (b) failure by a caregiver to satisfy the elder’s basic needs or to protect the elder from harm” (Wallace & Bonnie, 2003, p. 39). Elder abuse has various types including (a) physical abuse (i.e., acts that cause physical pain or injury); (b) psychological abuse, which includes acts that inflict emotional distress or psychological harm; (c) sexual assault; (d) financial exploitation; and (e) neglect (Bonnie & Robert, 2003). Perpetrators of elder abuse could be current spouses or partners, children and stepchildren, siblings or parents, other relatives, former family members, and nonkin perpetrators such as neighbors, friends, colleagues, and health-care providers (Wong et al., 2021).
Elder abuse is related to significant adverse health and mental health conditions, including elevated morbidity (Lachs et al., 1998; X. Dong et al., 2009; X. Q. Dong et al., 2011), increased likelihood of being disabled (Schofield et al., 2013), worst physical and functional health (Schofield et al., 2013; Wong & Waite, 2017), experiencing depression (Pillemer & Moore, 1989; Mouton et al., 2010; Roepke-Buehler et al., 2015) and anxiety (Wong & Waite, 2017), increased levels of psychological distress (Comijs et al., 1999), increased use of emergency medical services (Dong et al., 2012b), increased rates of hospitalization (Dong & Simon, 2013b; Dong et al., 2012a), and increased institutionalization (Dong & Simon, 2013a). Specifically, Lachs et al. (1998) found that victims of elder mistreatment had a threefold higher likelihood of mortality than nonvictims. The social consequences of elder abuse include elevated social isolation, declined social resources, and higher expenditures on services to make amends for resources lost through exploitation and to find and rehabilitate elder abuse victims (Anetzberger, 2004; Spencer, 1999).
At the global level, based on 52 studies from 28 countries, Yon et al. (2017) found the pooled prevalence rate to be 15.7% for overall elder abuse, 11.6% for psychological abuse, 6.8% for financial abuse, 4.2% for neglect, 2.6% for physical abuse, and 0.9% for sexual abuse. Population-based studies indicated that 1 in 10 older adults in the United States experienced at least a type of mistreatment in the past year (Acierno et al., 2010), and 1.7% of older adults experienced multiple types of mistreatment in the past year (Williams et al., 2017). However, the actual rates of victimization might be higher because of underreporting (Acierno et al., 2010; Williams et al., 2017). For example, the National Elder Abuse Incidence Study (Tatara et al., 1998), the first major investigation of elder abuse in the United States, did not collect data directly from older adults but assessed Adult Protective Service records and sentinel (e.g., community professionals) reports, which might greatly underestimate the scope of the problem. A much lower estimated overall prevalence of elder abuse (3.2%) was reported from a community-based sample (Pillemer & Finkelhor, 1988). In a more nationally representative study, Laumann et al. (2008) found that 9% of older people reported verbal abuse, 3.5% financial exploitation, and 0.2% physical mistreatment. Fisher & Regan (2006) found that approximately half of the women over 60 years experienced at least one type of maltreatment since age 55. A systematic review of 49 population studies demonstrated prevalent estimates of overall elder abuse that ranged between 3.2% and 27.5%. Such a wide range might indicate true variation in abuse rates across cultural settings and the inconsistency in defining and measuring abuse (Cooper et al., 2008).
Some studies indicated higher rates of elder abuse in ethnic and racial minority populations than non-Hispanic Whites. An integrative review based on nine studies reported rates of elder abuse ranging from 4.3% to 45.9% for American Indian elders (Crowder et al., 2019). For low-income Latino immigrants, 40.4% experienced any form of abuse within the past year (DeLiema et al., 2012). A study of 4,627 older adults called Chicago Health and Aging Project found that older African American men were three times more likely to experience self-neglect than older White men, and older African American women were twice more likely to experience self-neglect than older White women (Dong et al., 2012a). Other studies also found that being African American was associated with a higher risk of financial abuse (Beach et al., 2010; Laumann et al., 2008), and psychological mistreatment (Beach et al., 2010).
Results regarding the prevalence of elder abuse across different racial groups were mixed. For example, Laumann et al. (2008) indicated that Hispanic older adults had a lower risk of verbal abuse and financial abuse than White older adults. Also, Hispanic older adults were less likely to experience neglect than other racial groups (Burnes et al., 2015). Nevertheless, the lower rates might reflect reporting bias because Hispanic older people tended to underreport elder abuse (DeLiema et al., 2012). A recent study by DeLiema et al. (2020) found that Hispanics were significantly less likely to report victimization by financial fraud (prize/lottery fraud and investment fraud). Joseph & Gonzalez (2018) pointed out that elder abuse might be especially hidden within the family and institutions in communities of racial minorities where beliefs, traditions, and cultural values significantly affect how elder abuse is perceived, defined, and reported. It is plausible that different racial groups might have different risk and protective factors in terms of elder abuse. The results of some studies discussed above, however, might not be accurate. For example, some studies (e.g., Acierno et al., 2010; Williams et al., 2017) used random digit dialing for sampling, which has been shown to be problematic (e.g., lower rates of response; Fowler, 2013).
Risk and Protective Factors
The risk factors related to elder abuse in the general older population were reported by researchers. Acierno et al. (2010) suggested that low social support is a risk factor for all types of elder abuse and triples the risk of victimization. A systematic review of 49 studies suggested 13 risk factors of elder abuse in community-dwelling elders (Johannesen & LoGiudice, 2013). They were categorized into four subgroups, including risk factors related to elder person (cognitive impairment, behavioral problems, psychiatric illness or psychological problems, functional dependency, poor physical health or frailty, low income or wealth, trauma or past abuse, and ethnicity), perpetrator (caregiver burden or stress, and psychiatric illness or psychological problems), relationship (family disharmony, poor or conflictual relationships), and environment (low social support, and living with others except for financial abuse).
Some studies also identified risk factors of elder abuse in racial minority older adults. Crowder et al. (2019) found a consensus for three risk factors for American Indian elders including substance abuse, mental health problems, and caregiving issues. For African Americans, there might be some historical attributes that provide context for elder abuse. For example, the legacies of racism and slavery have resulted in not only anger and hopelessness but also economic and health disparities (Mouton & Southerland, 2017). Transgenerational effects of the experience of slavery might also influence how African American older adults manifest the effects of mistreatment (Mouton & Southerland, 2017).
Very few studies have identified any protective factors related to reduced elder abuse in racial minority groups. Tuck (2009) suggested researchers to use desire-based research frameworks which emphasize understanding complexity, contraction, and the self-determination of individuals and communities. To study racial minorities, researchers should not only document the painful elements of social realities but also elements of hope and wisdom (Gingrich-Philbrook, 2005).
Current Study
The aforementioned studies suggested multiple racial differences regarding elder abuse. These racial differences suggest the possibility that social and cultural factors may play a role in elder abuse. It is of great significance to examine potential racial disparities in elder abuse, given the increasing public health focus on the reduction of racial disparities (Keppel et al., 2008). Further elucidation of racial differences for elder mistreatment is necessary to design more effective preventions or interventions, which requires an insightful understanding of racially and culturally specific elements of elder abuse. While several reviews have been done in the field of elder abuse (Cooper et al., 2008; Crowder et al., 2019; Johannesen & LoGiudice, 2013; Joseph & Gonzalez, 2018; Pillemer et al., 2016; Stodolska et al., 2020), to date, no review has done a comprehensive comparison and analysis regarding elder abuse across racial groups and examined risk and protective factors. Thus, this systematic review aims to synthesize the body of research on elder abuse specific to racial minorities in community-dwelling older adults to answer the following questions: (a) What are the risk and protective factors for elder abuse by race? (b) What uniquely leads to elder abuse in racial minority groups (e.g., culture)?
Methodology
Search strategy
This systematic review was conducted in compliance with the Preferred reporting items for systematic review and meta-analysis (PRISMA) statement (Moher et al., 2015). After consulting with university librarians, the following electronic bibliographic databases were searched: AgeLine, Medline, PsycINFO (American Psychological Association), and the Cumulative Index to Nursing and Allied Health Literature (CINAHL). The key phrases used in the search were: (“elder abuse” or “elder mistreatment” or “elder neglect” or “elder maltreatment”) AND (“racial differences” or “ethnic differences” or “racial inequality” or race or ethnicity or minority or “African American*” or “Hispanic American*” or “Latino American*” or “Asian American*” or “Native American*”).
Inclusion and Exclusion Criteria
The inclusion criteria were to: (1) study about elder abuse (physical abuse, emotional abuse, sexual abuse, financial exploitation, or neglect); (2) have at least 50% of the sample as racial or ethnic minorities in the country of publication (e.g., African American and Hispanic American); (3) focus on people aged 60 and above; and (4) consider risk and/or protective factors related to elder abuse. There was no limitation on time periods of publication, in consideration of the limited number of relevant articles about elder abuse among racial minority groups. Therefore, all relevant studies published before March 2021, when the current study started, were taken into consideration. The exclusion criteria were if: (1) the study is only about the definition/perception/measurement of elder abuse; (2) the publication type is systematic review/meta-analysis/case study/literature review/editorial/book chapter; (3) it is gray literature; (4) it is not in the English language; or (5) the full text of the article was not available. Attempts were made to access the full text through assistance from the university librarians and by contacting the author of the article. If the full text was not obtained, the study was then excluded.
Screening and Data Extraction
The data were extracted based on inclusion and exclusion criteria, study designs, primary and secondary outcome measures, and findings. The search outcomes were reported using the PRISMA flow diagram (Figure 1). The Mixed Methods Appraisal Tool (MMAT) version 2018 was applied to establish the quality of studies (Hong et al., 2018). We used summary tables to describe these elements, and we reported the results as a critical narrative synthesis. The range of publication dates of the screened studies is from 1981 to 2022. And the range of publication dates of the 25 included studies is from 1989 to 2019.
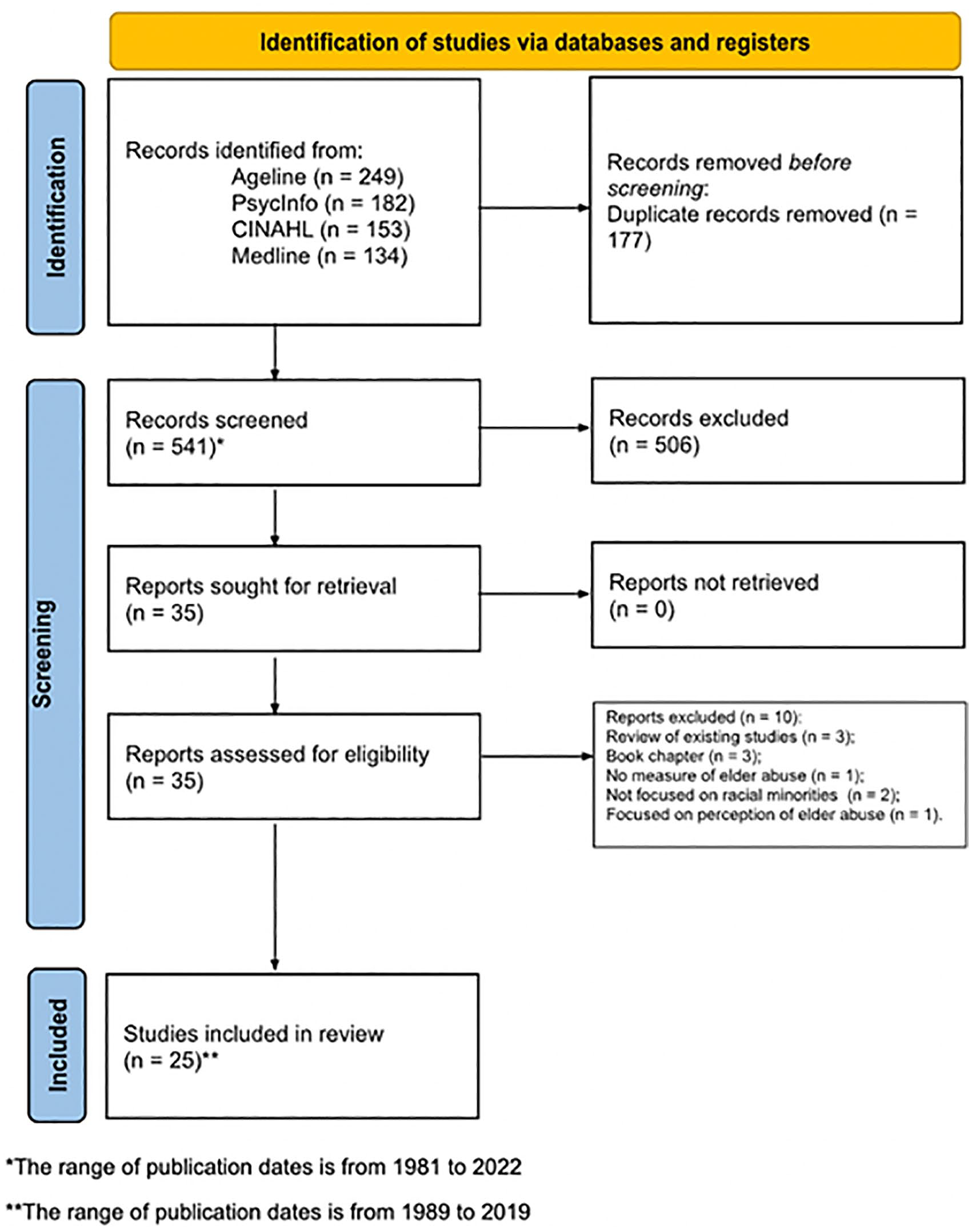
Flow diagram for systematic review.
Results
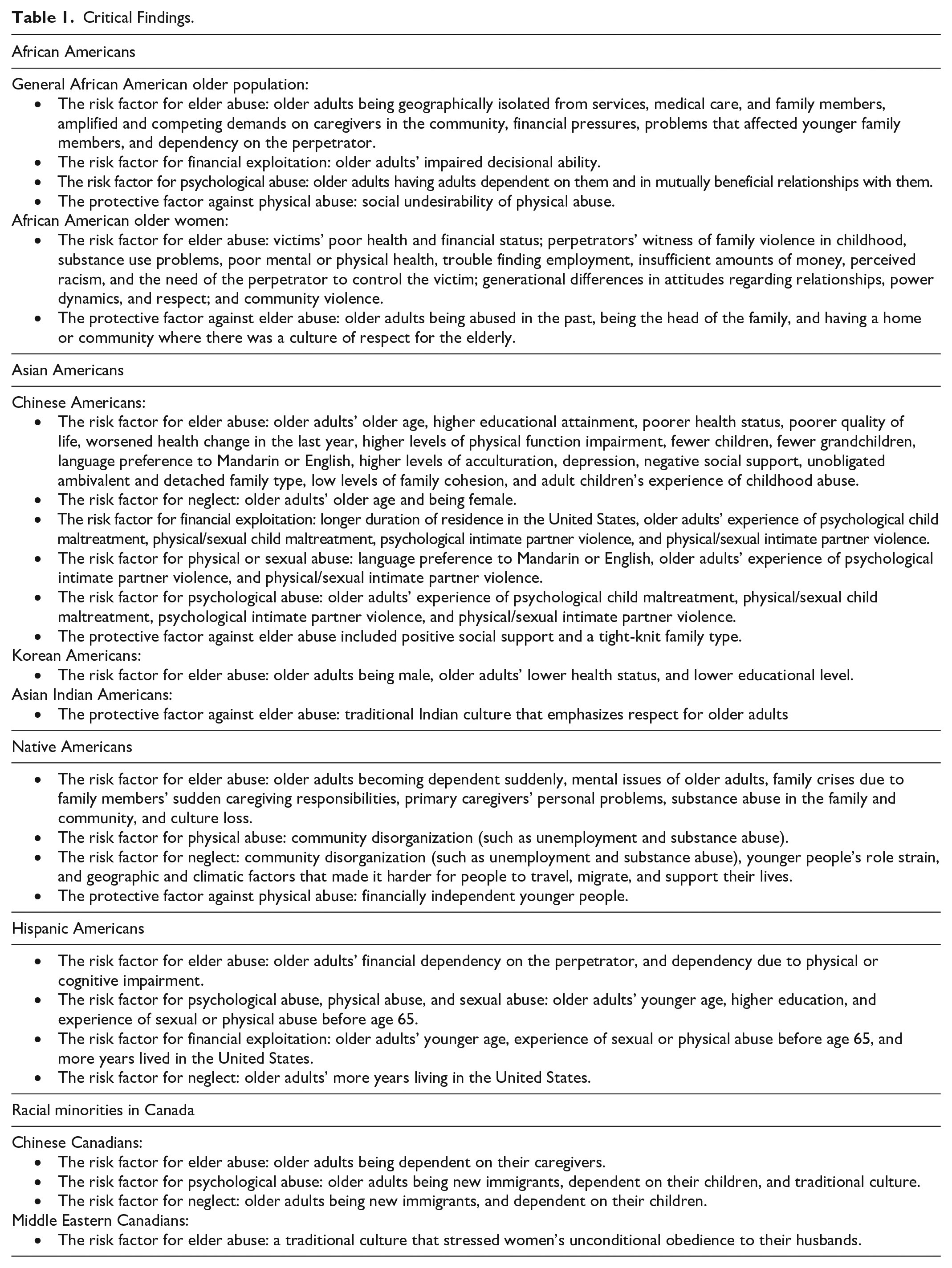
Using the key phrases, a total of 718 articles were found (249 from AgeLine, 182 from PsycINFO, 153 from CINAHL, and 134 from Medline). Deduplication resulted in 541 citations. Articles were then independently screened by two coders using the inclusion and exclusion criteria. The coding was reconciled by having coders 1 and 2 together to screen the articles that didn’t reach an agreement. After screening and reconciling by coders 1 and 2, 436 articles were excluded because they didn’t meet the inclusion criteria, and 105 articles were included. Then, coders 1 and 2 screened these 105 articles again to find those investigating risk and protective factors related to elder abuse. The number of articles retained for eligibility assessment was 35. After 10 were excluded for various reasons (see Figure 1), the final number of articles for review was 25, including 4 about African Americans, 11 about Chinese Americans, 2 about Korean Americans, 1 about Asian Indian Americans, 3 about Native American, 1 about Hispanic Americans, 1 about both African Americans and Hispanic Americans, and 2 about racial minority older adults in Canada. Three studies include a range of racial minority groups (Enguidanos et al., 2014; Tam & Neysmith, 2006; Walsh et al., 2007), while other studies specifically focus on a racial minority population (see Supplemental Table). All included studies are cross-sectional. Thirteen studies are quantitative (e.g., Lichtenberg et al., 2016; Wang & Dong, 2019), nine are qualitative (e.g., Enguidanos et al., 2014; Paranjape et al., 2009) and three are mixed method (e.g., Gao et al., 2019b; H. Y. Lee & Eaton, 2009). The majority of included studies were moderate to high in quality (92%). Two included studies had a 2* rating (on a rating scale of 1 to 5 with 5 being high quality) due to insufficient information or limitations in their study design (see Supplemental Table). See Table 1 for a summary of critical findings.
Critical Findings.
African Americans
For the African American population, five articles talked about possible risks or protective factors of elder abuse. The risk factors for elder abuse were older adults being geographically isolated from services, medical care, and family members (Griffin, 1994), amplified and competing demands on caregivers in the African American community (Njeri & Nerenberg, 1993), financial pressures (Njeri & Nerenberg, 1993), problems that affected younger family members (Njeri & Nerenberg, 1993), and dependency on the perpetrator including financial dependency, and dependency due to physical or cognitive impairment (Enguidanos et al., 2014). Regarding elder abuse subtypes, the risk factor for financial exploitation was older adults’ impaired decisional ability (Lichtenberg et al., 2016); the risk factor for psychological abuse was older adults having adults dependent on them and in mutually beneficial relationships with them (Griffin, 1994); the protective factor against physical abuse was social undesirability of physical abuse (Griffin, 1994).
A study focused on African American older women waiting to be seen in the ambulatory medicine clinics of a city hospital (Paranjape et al., 2009) identified that the risk factor for elder abuse included victims’ poor health and financial status; perpetrators’ witness of family violence in childhood, substance use problem, poor mental or physical health, troubles finding employment, insufficient amounts of money, perceived racism, and the need of the perpetrator to control the victim; generational differences in attitudes regarding relationships, power dynamics, and respect; and community violence. Regarding the protective factor against elder abuse, the study suggested that older women were less likely to be in an abusive relationship if they were abused in the past, the head of the family, and had a home or community where there was a culture of respect for the older generation.
Asian Americans
For the Asian American population, 14 articles were found, including 12 about Chinese Americans, two about Korean Americans, and one about Asian Indian Americans. For Chinese Americans, the risk factor for elder abuse included older adults’ older age (Dong, 2014), higher educational attainment (Dong, 2014; Dong et al., 2014, 2016), poorer health status (Dong, 2014; Dong et al., 2016), poorer quality of life (Dong, 2014; Dong et al., 2014), worsened health change in the last year (Dong, 2014; Dong & Wang, 2017; Dong et al., 2014, 2016), higher levels of physical function impairment (Dong, 2017), fewer children (Dong et al., 2014, 2016), fewer grandchildren (Dong et al., 2016), language preference to Mandarin or English (Dong & Wang, 2017), higher levels of acculturation (Gao et al., 2019a), depression (Gao et al., 2019a, 2019b), negative social support (overall, from spouse, from families, and from friends) (Zheng et al., 2019), unobligated ambivalent family type (Li et al., 2019), detached family type (Li et al., 2019), low levels of family cohesion (Gao et al., 2019b), and adult children’s experience of childhood abuse (Dong et al., 2017).
Regarding elder abuse subtypes, the risk factor for neglect was older adults’ older age (Dong & Wang, 2017) and being female (Dong & Wang, 2017); the risk factor for financial exploitation was a longer duration of residence in the U.S. (Dong & Wang, 2017), older adults’ experience of psychological child maltreatment, physical/sexual child maltreatment, psychological intimate partner violence, and physical/sexual intimate partner violence (Wang & Dong, 2019); the risk factor for physical or sexual abuse was language preference to Mandarin or English (Dong & Wang, 2017), older adults’ experience of psychological intimate partner violence, and physical/sexual intimate partner violence (Wang & Dong, 2019); the risk factor for psychological abuse was older adults’ experience of psychological child maltreatment, physical/sexual child maltreatment, psychological intimate partner violence, and physical/sexual intimate partner violence (Wang & Dong, 2019). The protective factor against elder abuse included positive social support (overall, from a spouse and family) (Zheng et al., 2019), and tight-knit family type (Li et al., 2019). For Korean Americans, the risk factor for elder abuse includes older adults being male (H. Y. Lee & Eaton, 2009), older adults’ lower health status (Chang, 2016), and lower educational level (Chang, 2016; H. Y. Lee & Eaton, 2009). According to Nagpaul’s (1997) study, traditional Indian culture that emphasizes respect for older adults might be a protective factor against elder abuse for Asian Indian Americans.
Native Americans
Three studies focused on elder abuse in Native American older adults. Brown’s (1989) study suggested that possible risk factors for elder abuse might include older adults becoming dependent suddenly, mental issues of older adults, family crises due to family members’ sudden caregiving responsibilities, and primary caregivers’ personal problems. According to Maxwell & Maxwell (1992), community disorganization (such as unemployment and substance abuse) was a possible risk factor for physical abuse, while financially independent younger people might protect older adults from being physically abused; the risk factor for neglect included community disorganization (such as unemployment and substance abuse), younger people’s role strain, and geographic and climatic factors that made it harder for people to travel, migrate, and support their lives. Jervis et al. (2017) interviewed 100 urban and rural older Native Americans about what it meant to be treated well and poorly. They found that when alcohol is a major problem in a reservation, somebody gets abused (e.g., little children and elders). And there is an intergenerational transmission of both abusive drinking and mistreatment in families affected by alcohol abuse. In addition, with a decline in “traditional” values, people now tend to mind their own business and are afraid to get involved if mistreatment happens to others. Therefore, substance abuse and culture loss are possible risk factors for elder mistreatment occurring in contemporary native communities.
Hispanic Americans
Only one study was identified specifically for Hispanic Americans (DeLiema et al., 2012). Focusing on low-income Latino immigrants in the U.S., the study inferred that the risk factor for psychological abuse, physical abuse, and sexual abuse was the same, including older adults’ younger age, higher education, and experience of sexual or physical abuse before age 65; the risk factor for financial exploitation included older adults’ younger age, experience of sexual or physical abuse before age 65, and more years lived in the U.S.; the risk factor for neglect included more years living in the U.S. Enguidanos et al.s’ (2014) study included both Hispanic Americans and African Americans. Through focus groups, it was found that older adults’ financial dependency on the perpetrator, and dependency due to physical or cognitive impairment, might contribute to elder abuse.
Racial Minorities in Canada
Two studies talked about factors related to elder abuse in Canadian racial minority groups. For Chinese Canadians, the possible risk factor for elder abuse included older adults being dependent on their caregivers (Tam & Neysmith, 2006); the risk factor for psychological abuse might include older adults being new immigrants (Walsh et al., 2007), being dependent on their children (Walsh et al., 2007), and traditional culture (Tam & Neysmith, 2006); the risk factor for neglect included older adults being new immigrants (Walsh et al., 2007) and being dependent on their children (Walsh et al., 2007). For Middle Eastern Canadians, the possible risk factor for elder abuse included traditional culture which stressed women’s unconditional obedience to husbands (Walsh et al., 2007).
Discussion
This study is the first review to summarize the existing literature on the risk and protective factors of elder abuse in community-dwelling racial minorities. Different racial groups may have distinct characteristics in terms of elder abuse. Therefore, this study is helpful to guide programs and policies to serve this population. The current study reviewed studies not only conducted with a quantitative method but also with a qualitative and mixed method. This is meaningful because elder abuse might be a sensitive and complicated topic and qualitative research is known for its strength in understanding human affairs in general and subjective experiences (Thyer, 2012). This systematic review summarized the body of research on elder abuse specific to racial differences. The results of current research identified several common risk factors of elder abuse across racial minorities, such as dependence on caregivers and health issues. It also acknowledged some discrepancies in the literature. For example, culture could have both risk and protective effects. To better serve racial minority older adults, it is important to understand what might put them at higher risk or protect them from elder abuse. This review also discovers gaps in the existing literature that future research could work on.
Common Risk Factors
There are some common risk factors across racial minorities. Older adults’ dependence or increased demand on caregivers was found to increase the risk of elder abuse for African Americans (Enguidanos et al., 2014; Griffin, 1994), Hispanic Americans (Enguidanos et al., 2014), and Native Americans (Brown, 1989), as well as the risk of elder abuse, psychological abuse, and neglect for Chinese Canadians (Tam & Neysmith, 2006; Walsh et al., 2007). This finding is in concordance with the caregiver stress and burden theory (Steinmetz, 1978, 1988), which posited that overwhelmed caregivers may harm or fail to take care of older people. Johannesen & LoGiudice’s (2013) systematic review also indicated that caregiver burden or stress was associated with a higher risk of elder abuse in the general population. It is noticeable that older adults’ increased dependence on family members is an important issue to be taken care of when dealing with elder abuse across all racial groups. However, Griffin (1994) suggested that older adults having adults dependent on them could also increase the likelihood of physical elder abuse, which is not mentioned either by caregiver stress burden theory or Johannesen & LoGiudice’s (2013) systematic review. Older adults’ burden of taking care of other family members might be an overlooked area in current elder abuse literature.
Isolation is also a common factor likely leading to elder abuse. Older adults being isolated from services, medical care, and family members were related to a higher risk of elder abuse in the African American community (Griffin, 1994). For Chinese Americans, negative social support (Zheng et al., 2019) and low levels of family cohesion elder abuse (Gao et al., 2019b) might result in elder abuse. Higher levels of physical function impairment, which might make older adults isolated from others, were also associated with a higher risk of elder abuse (Dong, 2017). For Native Americans, geographic factors that made it harder for people to travel or visit their families might cause elder neglect (Maxwell & Maxwell, 1992). In light of Bronfenbrenner’s (1979) Ecological Model, the environment individuals live in, shapes their lives. Being isolated from the microsystem (e.g., family) and the macrosystem (e.g., community and culture) might be challenging and make older adults more vulnerable to being abused.
Many studies identified health and mental health-related variables as risk factors for elder abuse. In terms of physical health, older adults’ health problems were associated with higher odds of elder abuse in the Chinese American community (Dong, 2014; Dong et al., 2016). The same relationship was also confirmed in the Korean American community (Chang, 2016). In terms of cognitive health, it is suggested that older adults’ impaired decisional ability (Lichtenberg et al., 2016) was related to elder abuse encountered by African American older adults. In terms of mental health, depression was related to elder abuse for Chinese American older adults (Gao et al., 2019a, 2019b), and mental issues were related to elder abuse for Native American older adults (Brown, 1989). Substance abuse is a risk factor identified by several included studies. Paranjape et al. (2009) suggested that perpetrators’ substance use problems might put African American older women at higher risk of elder abuse. For Native Americans, Maxwell & Maxwell (1992) and Jervis et al. (2017) demonstrated that substance abuse in the family and community is a possible risk factor for elder abuse. These findings imply that helping professionals should pay more attention to older adults with physical, cognitive, or mental health issues when handling elder abuse in racial minorities.
Culture
There are mixed findings regarding culture and traditions’ impact on elder abuse. Gao et al. (2019a) found no relationship between traditionalism and elder abuse or elder neglect among Chinese Americans. Nevertheless, for African American older women, living in a home or community with a culture of respect for the older generation could protect them from being abused (Paranjape et al., 2009). Traditional Indian culture that emphasizes respect for the elderly had a protective effect on Asian Indian American older adults (Nagpaul, 1997). Jervis et al. (2017) also pointed out that as the traditional culture in Native American communities declines, people tend to ignore the incidence of mistreatment of others. Sometimes culture can have a negative effect. For Middle Eastern Canadians, a possible risk factor for elder abuse could be a traditional culture that emphasizes women’s unconditional obedience to their husbands (Walsh et al., 2007). Traditional culture was also found to be related to an increased likelihood of elder abuse for Chinese Canadian older adults (Tam & Neysmith, 2006). Therefore, it is important to see traditional culture in a whole picture context, rather than in a solely negative or positive lens, and assume tradition has the same effect on all racial minorities.
For racial minorities and immigrants, their traditional culture might not be widely accepted by society and their younger generations, and the attempts to acculturate might put them at higher risk of elder abuse. For example, generational differences in attitudes regarding relationships, power dynamics, and respect probably put African American older generations at a higher risk of elder abuse (Paranjape et al., 2009). For Chinese Americans, older adults’ higher levels of acculturation were related to a higher risk of elder abuse (Gao et al., 2019a), and their longer duration of residence in the U.S. (Dong & Wang, 2017) was related to a higher risk of financial exploitation. This finding to some extent echoes S. A. Black et al. (1998) and Wilmoth & Chen’s (2003) research which suggested that stress associated with immigration and acculturation may place immigrants at increased risk for depressive symptoms than their Native-born counterparts. Angel et al. (2001) also suggested that later-life immigration could be particularly stressful as the pressure of coming to a new and unfamiliar environment might increase the risk of depression and isolation. Helping professionals should give special attention to older adults who experience a different culture than the majority population, and alternative interventions may be required to connect them to social support and resources.
Trauma
Both victims’ and perpetrators’ previous exposure to violence has been associated with elder abuse. For African American older women, their perpetrators’ witness of family violence and experience of family violence in childhood was related to an increased likelihood of use of elder abuse (Paranjape et al., 2009). Dong et al. (2017) found that adult children’s experience of childhood abuse was a possible risk factor for use of elder abuse. Social learning theory might be able to explain this finding, which postulated that aggressive behaviors were modeled by adults, such as parents, and then adopted by children (Bandura & Barab, 1971). However, much remains unknown regarding how violent behavior is adopted and lasts for such a long time, and if any other factors have an impact. For example, M. C. Black et al. (2011) theorized that children’s exposure to domestic violence that resulted in a positive outcome for the perpetrator would lead them to be more likely to adopt aggressive behaviors in adulthood. More research is needed to fully understand this process. Chinese American older adults’ experience of childhood abuse and intimate partner violence were both related to increased risk for elder abuse (Wang & Dong, 2019). DeLiema et al. (2012) found that low-income Hispanic American immigrants’ experience of sexual or physical abuse before age 65 could lead to an elevated likelihood of elder abuse. Therefore, incorporating trauma informed care principles and trauma interventions into programming for elder abuse victims and perpetrators might be helpful. To be trauma-informed is to understand the involvement and impact of violence and victimization in individuals (Elliot et al., 2005), which would be beneficial for victims and perpetrators to recover from not only previous trauma but also current abusive relationships.
The relationship between previous abuse and elder abuse could be partly explained by the cumulative advantage/disadvantage theory, which posited that early life adversity could lead to further adversity in adulthood (e.g., poor education and lack of social support) (Dannefer, 2003). Some studies did support the relationship between poor education and elder abuse (Chang, 2016; H. Y. Lee & Eaton, 2009) and the relationship between lack of social support and elder abuse (Zheng et al., 2019). A conflicting finding is that Paranjape et al. (2009) demonstrated that African American older women’s risk of being abused would decrease if they were abused in the past. Future research should work on the discrepancy to find out the reason behind it.
Education and Age
Findings regarding education and age are mixed. Some studies suggested that higher education was related to a higher risk of elder abuse for Hispanic Americans (DeLiema et al., 2012) and Chinese Americans (Dong, 2014; Dong et al., 2014, 2016) while one study found that there was no relationship for Chinese American (Dong & Wang, 2017) and another two found lower levels of education associated with a higher risk of elder abuse for Korean Americans (Chang, 2016; H. Y. Lee & Eaton, 2009). This is counterintuitive because education is often considered a protective factor. For example, J. Lee et al., (2018) demonstrated that education in early life had protective effects against memory impairment related to late-life depression; in households with a member with a mental disorder, a parent’s education level was positively associated with family adaptability (Greeffet al., 2006). In addition, some studies found that older age was related to a higher risk for elder abuse (Dong, 2014; Dong & Wang, 2017) while another study found that younger age was a risk factor (DeLiema et al., 2012). These are areas that require further investigation.
Gender
More research is needed on racial minority older women since they possess multiple socially marginalized identities which might make them especially susceptible to abuse. Dong & Wang (2017) found that being female was related to an increased risk of elder neglect for Chinese American older adults. According to intersectionality theory, racial minority women have two socially marginalized identities. For example, African American women were both African American and female. Intersectionality theory argues that their lived experiences, specifically researchers’ experiences of discrimination and oppression, are essentially different from African American men and White women (Bowleg, 2012; Crenshaw, 1990). African American older women even have one more socially marginal identity: old age. This review did find that African American older women had a larger number of risk factors related to elder abuse, especially perpetrator-related factors (Paranjape et al., 2009). Further investigation is needed to find out how discrimination and oppression put racial minority older women in a vulnerable position to face abuse.
Race minority subgroups
Compared to Asian Americans, risk and protective factors related to elder abuse in subgroups of African Americans, Hispanic Americans, and Native Americans were not discussed. There might be numerous differences between these subgroups which could provide insight into the degree of within-group variability. For example, a Hispanic subgroup might include Latin Americans, Mexican Americans, and Puerto Ricans. Each of these subgroups reflects some unique and varying distinctions, such as culture, history, and levels of assimilation (Whitfield et al., 2008). More research should be conducted to fill this gap.
Protective Factors
Only a few studies identified protective factors related to elder abuse, including social undesirability of physical abuse (Griffin, 1994); victims being abused in the past, being the head of the family, and living in a home or community with a culture of respect for older adults (Paranjape et al., 2009); positive social support and tight-knit family type (Li et al., 2019); and traditional Indian culture that emphasizes respect for older adults (Nagpaul, 1997). It can be seen from these studies that the culture of respect is a common protective factor for older adults. Researchers’ and practitioners’ strength-based perspectives would be significant to help older adults who experienced elder abuse. According to Gable & Haidt (2005), we should not only look at distress or suffering but also discover the other side of the coin, such as positive experiences and healthy families, to address the “full spectrum of human experience” (p. 105). Gingrich-Philbrook (2005) also suggested that, based on desire-based frameworks, individuals’ wisdom and hope when confronted with painful experiences should not be overlooked.
Limitations and Quality of Evidence
The current study has a couple of limitations. Gray literature was not included in this study. This would be a limitation because published literature might be biased toward positive over null results. What’s more, it is noticeable that null results are not often published. Also, the current study is limited to studies available in English and databases searched.
The included studies also have some limitations. All findings were based on cross-sectional analysis. The downside is that it is hard to fully understand if the risk and protective factors influence elder abuse or the other way around. In the future, more longitudinal data would be needed to better understand the relationship between elder abuse and the risk and protective factor identified in this paper. These studies were also based on a nonexperimental survey research design. Inherent in survey data are threats to both internal validity (i.e., causal inferences) and external validity (i.e., generalizability) of results. The sample size varies across studies. Some had thousands of participants (e.g., Dong, 2014; Dong & Wang, 2017), while others only had about a dozen participants (e.g., Brown, 1989; Tam & Neysmith, 2006) and some didn’t even report the number (e.g., Maxwell & Maxwell, 1992; Nagpaul, 1997). In terms of sampling, many studies involve a procedure of availability sampling and purposive sampling, which would undermine the generalizability of the findings. For example, Lichtenberg et al. (2016) recruited volunteers from a senior center to participate in their study. In addition, studies didn’t use consistent measurements and methods, which might influence the quality of evidence. Several studies are old (e.g., Brown, 1989; Maxwell & Maxwell, 1992; Nagpaul, 1997). Attitudes and opinions about elder abuse may have changed since the 1980s. We include them because there are limited studies available regarding elder abuse among racial minorities. For example, Brown’s (1989) and Maxwell & Maxwell’s (1992) research are two of the three studies we found about risk and protective factors for Native Americans.
Some factors might have a mediating or moderating effect on the relationship between elder abuse and other factors, rather than directly influencing elder abuse. For example, Dong & Wang (2017) suggested that older adults’ experience of childhood abuse could predispose older people to elder abuse. Some studies also found that worst health status (Chang, 2016; Dong, 2014; Dong et al., 2016) and financial pressures (Njeri & Nerenberg, 1993; Paranjape et al., 2009) would increase the likelihood of elder abuse. It might be the case that health status and financial strain mediate or moderate the relationship between childhood abuse and elder abuse. More research is required to illustrate how in detail these identified risk and protective factors affect elder abuse. Ten out of 12 studies about American Chinese elder abuse used the same dataset which was collected from the greater Chicago area. This would be a methodological limitation and impact the generalizability of these studies. Future research should increase diversity geographically so that we could know if these findings could be applied to people from other regions. In addition, all included studies focus on community-dwelling elders, therefore findings of the current study are not generalizable to institutionalized elders.
Implications
See Table 2 for a summary of these implications. For practitioners, traditional culture should be understood in a whole picture, because it could be multifaceted and impose different impacts across racial minorities; trauma informed care should be incorporated into prevention and interventions for elder abuse; more attention should be paid to racial minority elderly with caregivers of potential personal issues, such as substance use and mental health issues. To be trauma-informed involves understanding individuals and their symptoms in the context of their life experiences and cultures, acknowledging that some symptoms may represent efforts at coping (Butler et al., 2011). Racial minority older adults may be different in many ways compared to their White counterparts, and these differences might be associated with adversities (e.g., elder abuse) over their life course. Practitioners should understand and respect it so that more appropriate and effective services could be provided accordingly.
Review Implications.
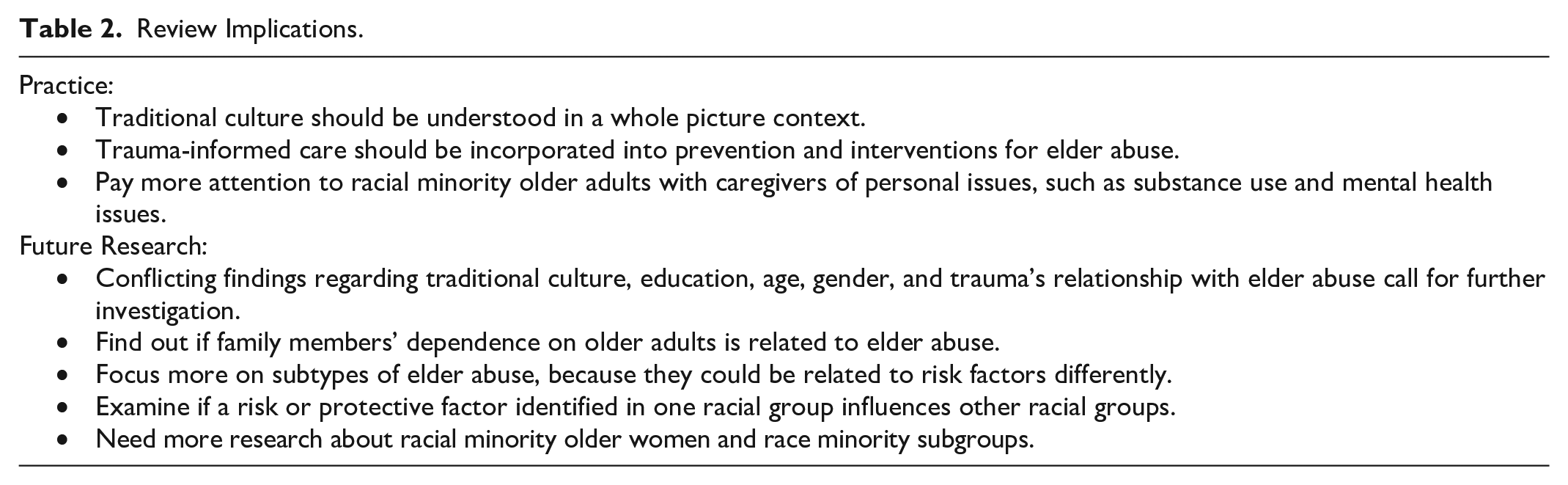
In the future, researchers should focus more on which component of the traditional culture is beneficial or harmful, because some studies suggested cultural risk factors for elder abuse and others did not. Other conflicting findings included education, age, gender, and trauma, which require further investigation. Further research is needed in some specific areas. For example, studies suggested that older adults’ dependence on caregivers would increase the risk of elder abuse (Brown, 1989; Griffin, 1994; Tam & Neysmith, 2006; Walsh et al., 2007). However, less is known about whether family members’ dependence on older adults would be related to elder abuse (Griffin, 1994). In addition, further investigation should be focused on subtypes of elder abuse, because they could be related to risk factors differently. We realized some gaps between racial groups regarding health and mental health that future research could work on. For example, the influence of cognitive impairment on elder abuse was only investigated for African Americans (Lichtenberg et al., 2016). And the influence of mental health issues on elder abuse was only investigated for Chinese Americans (Gao et al., 2019a, 2019b) and Native Americans (Brown, 1989). Elder abuse research about racial minority older women, race minority subgroups, and protective factors is scarce. Racial minority women could have multiple socially marginalized identities, racial subgroups could have huge differences, and recognizing protective factors could inform practice to a great extent. To work on these unknown areas would be of great significance to both research and practice.
Supplemental Material
sj-docx-1-tva-10.1177_15248380221140123 – Supplemental material for A Systematic Review: Risk and Protective Factors of Elder Abuse for Community-Dwelling Racial Minorities
Supplemental material, sj-docx-1-tva-10.1177_15248380221140123 for A Systematic Review: Risk and Protective Factors of Elder Abuse for Community-Dwelling Racial Minorities by Wenxing Wei and Sarah Balser in Trauma, Violence, & Abuse
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.