
Abstract
Coercive control (CC) is a core facet of intimate partner violence (IPV) and involves asserting power, dominance, and control over another person. Although the adverse impacts of childhood exposure to interparental IPV have been well documented, the outcomes of childhood exposure to interparental CC have not been systematically examined. This study aimed to address this gap by reviewing available empirical evidence on interparental CC and child and family outcomes. Articles were identified by searching electronic databases using keywords relating to CC, children and parents, and child wellbeing outcomes. The final review included 51 studies that reported on adverse outcomes pertaining to parenting and family relationships (k = 29), child internalizing and externalizing problems (k = 7), social-emotional development (k = 5), and physical/health development (k = 17). Specifically, studies reported that CC was associated with increased parental psychopathology, poorer family functioning, harsher parenting and higher levels of child abuse, strained parent–child relationships, children used as tools and co-victims of CC, increased risk of child internalizing and externalizing problems, limited socializing opportunities, increased bullying, poorer perinatal outcomes, limited access to healthcare, and increased risk of child mortality. Evidence identified CC as a unique contributor to adverse child wellbeing outcomes, independent of exposure to IPV more broadly. Results indicated that the impacts of childhood exposure to CC are complex, far reaching, and, in some cases, devastating. The limitations of the findings, as well as implications for practice, policy, and research are discussed.
Keywords
Children exposed to familial violence are vulnerable to a plethora of long-term psychosocial issues. These can include behavioral and emotional adversities, higher rates of infant and child morbidity and mortality, and perpetration or victimization of violence in adolescence and adulthood (World Health Organisation [WHO], 2017). Family violence is gendered, with reports that more than 640 million women worldwide are subjected to intimate partner violence (IPV) (United Nations Office on Drugs and Crimes [UNODC], 2019). Globally, as many as 38% of female homicide victims (and 6% of male homicide victims) are murdered by an intimate partner (WHO, 2013). Critically, 95% of child family violence-related homicides occur at the hands of a parent or parent-like figure (i.e., step-parent) (DVDRT, 2019). Coercive control (CC) has been found to play a significant role in family violence and intimate partner homicides (DVDRT, 2019; Matias et al., 2020), yet little is known about its impact on children who are exposed to this dynamic between their parental figures.
CC is a core facet of IPV involving asserting power, dominance, and control over another person (Stark, 2007). Perpetrators enact CC using threatening and controlling tactics often including physical, sexual, and emotional violence, isolation, stalking, harassment, limiting access to financial resources (Christy et al., 2020), educational or occupational opportunity, and using systems (e.g., the legal system) against the target (Patafio et al., 2021). These strategies control and subordinate the target, ultimately stripping them of independence and autonomy (Stark, 2007).
While not all violent relationships are characterized by CC, and not all CC relationships include violence, CC is a strong predictor of severe and frequent instances of physical, psychological, and sexual IPV (Boxall & Morgan, 2021; DVDRT, 2019). Despite this significance of CC in IPV and the recent surge in attention paid to CC in the media, academic literature, and policy, the specific ways in which CC harms families, and particularly children, are poorly understood.
Children are “exposed to” as opposed to being “passive witnesses” of domestic abuse (Holden, 2003). They are often implicated, caught in, and required to manage and resist (i.e., survive) ongoing abuse (Tailor et al., 2014). Children exposed to IPV are at increased risk of experiencing emotional, sexual, and physical abuse; developing emotional and behavioral problems; experiencing life adversities (such as socio-economic, educational, and employment challenges); later life substance dependence; and subsequent victimization and perpetration of violence (Adejimi et al., 2021; Holt et al., 2008).
CC and Adverse Child Outcomes
Given the centrality of CC in IPV, and the well-documented impact of IPV on children, it is important to understand the impacts of interparental CC on child outcomes. Perpetrators of abuse often use children as a tool for asserting control and dominance over the adult victim (Beeble et al., 2007; Crossman et al., 2016). Research has begun investigating the specific associations, and the mechanisms through which CC may impact child-related outcomes, including parenting and parent–child attachment relationships, child internalizing and externalizing problems, and developmental health and wellbeing.
CC and parent–child relationship
Emotion security theory posits that children who are exposed to interparental conflict are at greater risk of developing psychopathology (Davies et al., 2016). This is likely due to children experiencing heightened fear and distress, along with limited access to emotionally available caregivers for psychological support. Secure attachment to caregivers is a protective factor for buffering the negative impacts of family adversity on child adjustment problems (Ding et al., 2014; Holt et al., 2008). However, security in the mother–child attachment relationship is compromised in the families of mothers exposed to IPV (McIntosh et al., 2021; Noonan & Pilkington, 2020). One explanation for this interaction is that mothers’ heightened risk of developing post-traumatic stress disorder (PTSD) symptoms in IPV environments reduces their capacity for maternal sensitivity toward their children (Suardi et al., 2020). Certainly, there are well-documented impacts of IPV on maternal emotional distress (Ellsberg et al., 2008), postnatal depression (Halim et al., 2018), parenting stress (Casanueva et al., 2008), and consequential parenting practices (Gustafsson & Cox, 2012; Sypher et al., 2022). Thus, parents’ psychological symptoms in the context of IPV merit important consideration for parenting and parent–child relationships.
While limited research has investigated the direct or indirect effect of CC on attachment, CC may impact parent’s ability to care for, engage with, and exhibit warmth toward children (Katz, 2019). Critically, children exposed to CC may be at increased risk of developing insecure attachment. Indeed, interparental CC dynamics are associated with strained and distant mother–child relationships (Katz, 2019).
CC tactics directly targeting parenting
CC abusers often undermine or interfere with the victim-parent–child relationship, in an attempt to purposely strain the parent–child relationship (Heward-Belle, 2017; Katz, 2019). The use of children to maintain control over victims tends to increase post-separation, where parenting, custody disputes, and contact pose opportunities to continue abuse (Feresin et al., 2019). This may have consequences for the child’s wellbeing as they are used as objects to enforce control, as well as for the parent’s “stay/leave” decisions when the risks for abuse remain post-separation.
CC and child internalizing problems
Family violence predicts victim stress and trauma as well as trauma symptoms in young people exposed to parental IPV (Tailor et al., 2014). Similarly, interparental CC extends beyond child-witnessing to child-victimization (Callaghan et al., 2018) and may render children vulnerable to stress, trauma, and maladaptive emotional coping. Child internalizing problems have been associated with exposure to CC even after controlling for physical IPV frequency and psychological abuse (Jouriles & McDonald, 2015). Consequently, to inform support and interventions for children, it is important to understand the unique contribution of CC on child adjustment and psychopathology, as well as the mediating and moderating factors of this interaction.
CC and externalizing problems
CC exposure has also been linked to child externalizing problems (Jouriles & McDonald, 2015). Social learning theory describes that direct experience or observation of others’ behavior influences one’s own learning and behavior (Bandura, 1978). This learning through observation includes aggression, whereby witnessing aggressive behavior begets vicarious learning of aggression. Supporting this, exposure to parental IPV has been associated with adolescent externalizing problems, including aggression, delinquency, peer relational challenges, and truancy (Fong et al., 2019). Individuals who were subjected to violence from their parents (directly victimized or witnessed violence) are more likely to experience or perpetrate violence in their adult relationships (Villafañe-Santiago et al., 2019). Maternal mental health, harsh parenting, and maternal warmth are found to be mediating factors between IPV exposure and externalizing problems (Fong et al., 2019). Given the impact of CC on parenting capabilities and on family violence, it is crucial to further understand the unique role of exposure to CC in children’s development of externalizing problems.
CC and developmental health and wellbeing
IPV poses risks to children’s developmental health and wellbeing across their lifespan (ANROWS, 2014; Tanimu et al., 2016). Children exposed to persistent, interparental conflict are at increased risk of poorer physical health, academic performance, and vocabulary skills compared to children not experiencing interparental conflict (ANROWS, 2017). Partner controlling behaviors increase the odds of pregnancy loss, above and beyond exposure to other forms of IPV (i.e., physical, sexual, and emotional abuse) (Tiruye et al., 2020a). These results substantiate that exposure to CC is a core facet to consider in accounting for children’s development and wellbeing.
Social-emotional development
Perpetrators of interparental CC often enact control by implicating the target’s children, such as preventing the children from spending time with others including family and peers, as well as restricting children from participating in extra-curricular activities (E. Katz, 2016). Thus, children’s social-emotional development and wellbeing may be negatively impacted through restricted opportunities to build meaningful relationships and develop individual interests and strengths. As with adult victim accounts on the impact of IPV contexts, the fear and constraint created from being exposed to interparental CC dynamics may be damaging to children in ways that are beyond physical violence alone.
Interactions underpinning interparental CC and child outcomes
Research has investigated the mediating and moderating variables linking IPV and adverse child and family outcomes. Evidence suggests that parenting capabilities and strategies such as emotion coaching buffer children exposed to IPV from internalizing and externalizing problems (L. F. Katz & Windecker-Nelson, 2006), as well as negative peer outcomes (L. F. Katz et al., 2008), and mothers’ depression has been found to mediate the link between IPV and child psychopathology (Miranda et al., 2013). Consequently, it is necessary to identify potential moderators of CC exposure and child relevant outcomes, as well as the mechanisms through which interparental CC relates to child outcomes.
Current Study
CC has become a focal point of family violence in policy and practice and while the general impacts of exposure to interparental IPV in childhood have been extensively researched, no prior studies have systematically reviewed the literature specifically examining exposure to interparental CC on children. This is a significant gap with serious implications for understanding how we can best support children exposed to CC. The aim of this study was to conduct a systematic review examining the child-relevant outcomes of interparental CC to build knowledge and inform clinical practice and policy.
The research questions addressed in the review were as follows
In what ways is CC associated with child wellbeing outcomes across the following domains?
(a) parenting and the parent–child relationship,
(b) internalizing and externalizing problems,
(c) developmental and social-emotional wellbeing
Exposure to interparental CC was predicted to result in adverse outcomes across the three domains.
2. Are there moderating or mediating factors explaining the relationship between parental CC and child outcomes?
Method
The review was conducted in compliance with the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines (PRISMA; Page et al., 2021). The study protocol was submitted to PROSPERO in February 2021 and published on the online international register for systematic reviews (Xyrakis & Pasalich, 2021).
Inclusion Criteria
Studies were included in the review if they: (1) measured or reported on interparental CC; (2) reported on the child-relevant outcomes of interparental CC regarding parenting factors and parent–child relationship dynamics, child mental health and wellbeing, and child development; (3) were written in English or a full English translation was available; (4) were an empirical, peer-reviewed study (e.g., not a book chapter, unpublished thesis, or editorial); and (5) were not a review or meta-analysis. We included papers with varying operationalizations of CC on the basis that they examined a pattern of partner controlling behavior between parents. Accordingly, studies were included if they examined partner controlling behavior only; controlling behavior in addition to physical, sexual, or emotional violence; or more specifically as a pattern of threatening, coercive, and controlling behavior irrespective of other forms of violence. Studies were excluded if children were only exposed to interparental CC in adulthood (i.e., after 18 years of age), or if exposure to CC was not clearly defined or differentiated from other forms of IPV (e.g., reports on physical violence only or does not clearly report the association between CC and child-relevant outcomes separate from other forms of abuse).
Search Strategy
Four electronic databases (Scopus, PsychInfo, PubMed, and Cochrane Library) were systematically searched for studies published up until the search date, July 26, 2021. A full search strategy is included in Supplemental Appendix A, outlining the keywords used relating to CC, children and parents, along with terms for parenting outcomes, internalizing and externalizing outcomes, and development. A grey literature search was not included, as research has indicated that the comparatively small proportion of unpublished studies included in systematic reviews rarely impact the results or conclusions (Hartling et al., 2017).
Study Selection and Data Collection
The study selection process is summarized in Figure 1. Search results from each database were imported to Covidence software system, which automatically removed study duplicates. Subsequent screening, reviewing, and data extraction was completed using the Covidence software. Two researchers independently screened the title and abstracts of the references, before checking full-text articles against the inclusion criteria. Disagreements were resolved through discussion and consensus.
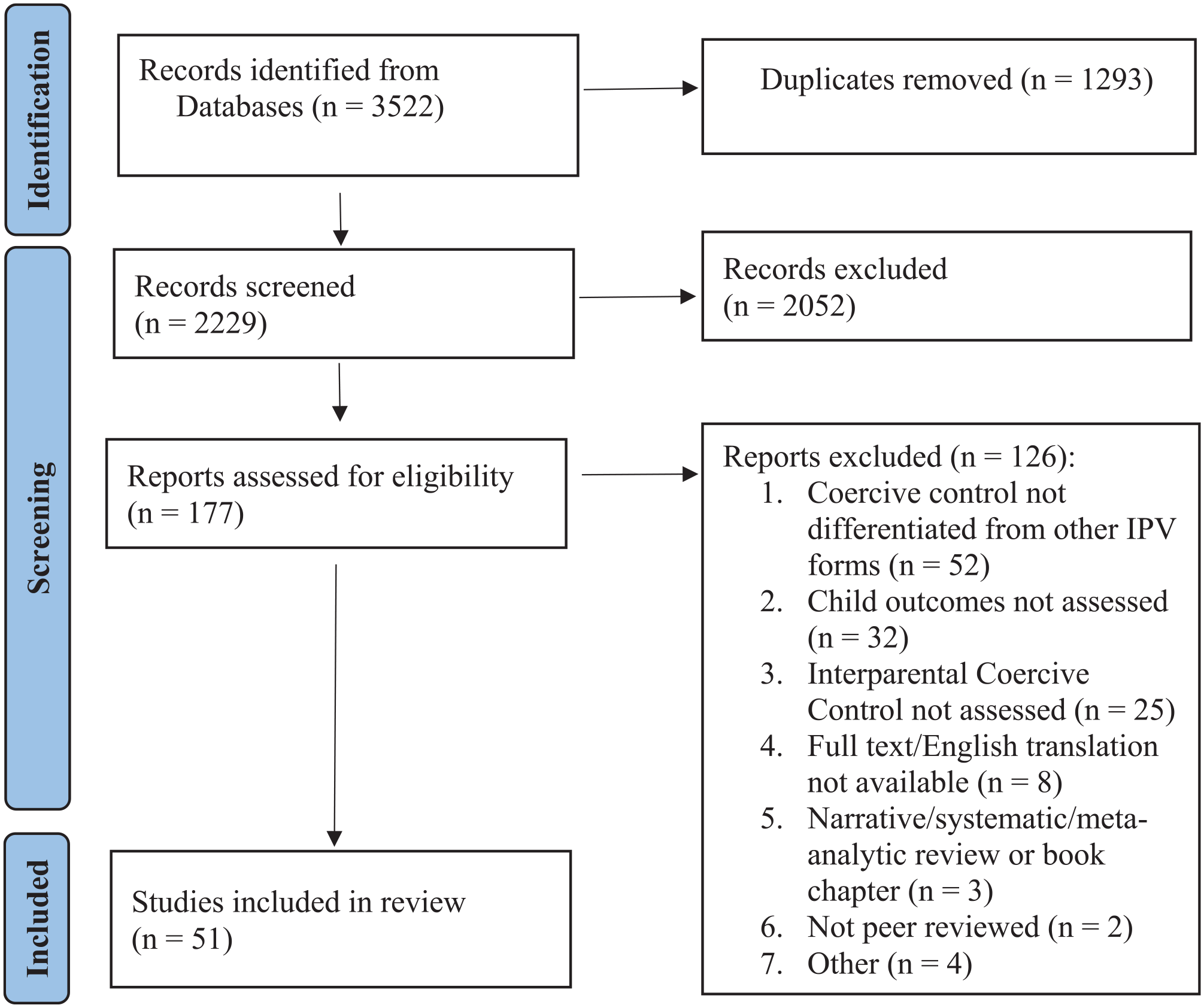
Study Selection Process.
Data extraction was conducted independently by the primary author and one other researcher, using the Covidence software. Information was extracted from included studies using a coding outline that was pre-developed by the authors and imputed into Covidence. The coding outline included publication details (e.g., author name, year, and country), sample characteristics (e.g., size, age, informant, and recruitment), measures used for interparental CC and child outcomes, study design, and main findings related to child outcomes. Discrepancies between coders were resolved through consensus.
Narrative synthesis of the findings from the included studies was conducted by grouping studies according to the type of outcome investigated. The current qualitative review summarizes the characteristics of each of the relevant studies; type of child outcomes measured; and the general findings of each study. Mediators and moderators are also discussed through narrative review.
Quality Assessment
Quality assessment was conducted using an Excel spreadsheet and was rated independently by the primary author and one other researcher. Study quality was assessed using the Standard Quality Assessment criteria for Evaluating Primary Research Papers from a Variety of Fields (Kmet et al., 2004). Separate checklists developed by Kmet et al., (2004) were used for qualitative and quantitative designs. Items were rated on a three-point scale (0 = No, 1 = Partial, 2 = Yes) assessing whether the study met certain quality criteria (e.g., clearly defined research question; relevant and appropriate study design; well defined and robust exposure/outcome measures; appropriate sample size). The final quality score was calculated by summing scores of each evaluation criteria, dividing by the total possible sum, and multiplying by 100 to produce a percentage score. This measure has produced good inter-rater reliability across a range of study designs (Kmet et al., 2004).
Results
The PRISMA flow diagram of the search results is shown in Figure 1. After duplicates were removed, 2,229 studies were included in the initial title and abstract screening phase. 163 full texts were reviewed for eligibility and a final 51 studies were ultimately included (Table 1). Studies were mostly excluded if CC was not clearly defined, identified, or separated from other forms of violence (k = 52), if child relevant outcomes were not assessed (k = 32), or if assessment of CC included relations other than the interparental dynamic (e.g., parent to child CC as a parenting strategy, or other family members such as in-laws included in measure of CC) (k = 25).
Included Studies Characteristics.
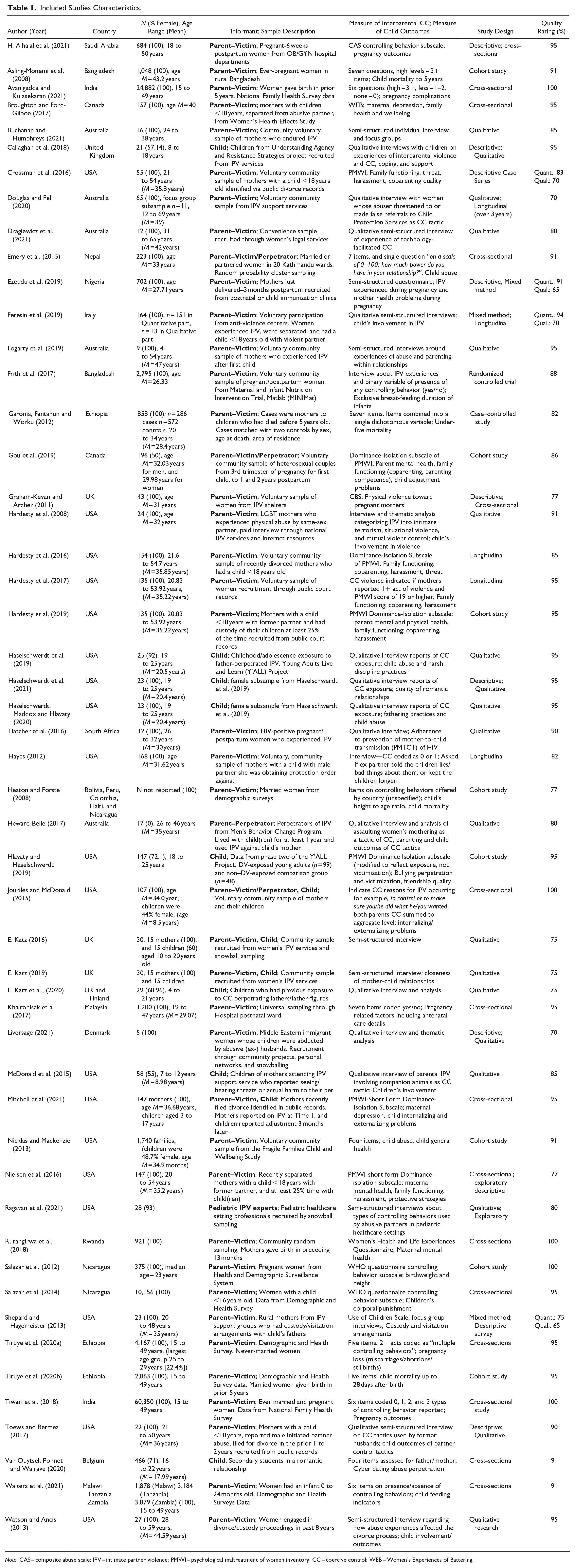
Note. CAS = composite abuse scale; IPV = intimate partner violence; PMWI = psychological maltreatment of women inventory; CC = coercive control; WEB = Women’s Experiences of Battering.
Sample Characteristics and Methodology
Study informants were parent survivors of CC (80%, k = 41), children of coercive controllers (24%, k = 12), and parent–perpetrators of CC (8%, k = 4). Six studies included two or three types of informants and one study used professional IPV expert informants from pediatric health settings. Three studies assessed both victimization and perpetration of CC, one of which included both members of the relationship as informants. Samples were from the USA and Canada (k = 21), Europe and the UK (k = 8), Africa (k = 7), Asia and the Middle East (k = 7), Australia (k = 5), and Latin America (k = 3). Majority of studies used a community representative sample (k = 29), other studies recruited from domestic violence services (e.g., shelters, support organizations, women’s services, and support groups) (k = 12), education settings (e.g., university or college) (k = 5), or healthcare settings (k = 5).
Most studies included purely quantitative data (k = 28), and 19 studies used qualitative analysis, and four used mixed methods. The sample characteristics, recruitment setting, design, and outcome measures are outlined in Table 1. Summary of main results pertaining to child relevant outcomes are outlined in Supplemental Appendix B. All included studies reported on female victim/survivors of CC and all bar one study examined CC in heterosexual relationships. Overall quality ratings can be found in Table 1. In general, study quality was high (70%−100%). However, quality ratings should be interpreted as a general indicator of overall study design and reporting, as outcomes of CC were not the primary aim of many studies.
Identification of Interparental CC
Interparental CC was assessed using validated measures (k = 16), self-constructed questionnaires (k = 13), single item questions (k = 2), or through thematic analysis defining CC or partner controlling behavior (k = 22). The most commonly used validated measure of CC was the Psychological Maltreatment of Women Inventory (PMWI; Tolman, 1999) Dominance-Isolation subscale (k = 8). Other measures used were: the partner controlling behavior measure from the WHO Multi-country Study on Women’s Health (García-Moreno et al., 2005) (k = 3), the Composite Abuse Scale (CAS; E. Alhalal et al., 2019) controlling behavior subscale (k = 1), Women’s Experiences of Battering (WEB; Smith et al., 1999) scale (k = 1), Controlling Behavior Scale (CBS; Graham-Kevan & Archer, 2003) (k = 1), Use of Children Scale (Beeble et al., 2007) (k = 1), and Johnson and Leone (2005) measure of intimate terrorism (k = 1). Eleven studies measured CC with their own set of questions (between 4 and 7 items) assessing presence of partner controlling behaviors, usually comprising themes relating to controlling contact with others (including excess jealousy of interactions with others), controlling engagement in daily activities (e.g., work/school), controlling access to resources (e.g., withholding money, access to health services), surveillance/monitoring, and (in some only) sexual coercion.
Identification of Child Outcomes
Child outcomes were categorized into three major groups: (1) parenting and family factors, included parent (usually the survivor) psychopathology (e.g., depression and PTSD), family functioning and dynamics (e.g., parenting stress, coparenting quality, and harassment), parent–child relationship dynamics (e.g., disciplinary strategies and relationship quality), and using children as pawns of CC (e.g., using children’s lives and circumstances to control the survivor); (2) child internalizing and externalizing problems; (3) developmental outcomes (e.g., social-emotional and physical health and mortality).
Parenting and Parent–Child Relationship
Twenty-nine studies reported on the impacts of CC on parenting factors.
Parent psychopathology (k = 5)
Quantitative studies (k = 4) found that parent survivors of CC experienced higher levels of anxiety, parenting stress, alcohol abuse, PTSD, suicidal ideation, and fear and depression than parents who did not report CC (Gou et al., 2019; Hardesty et al., 2019; Nielsen et al., 2016; Rurangirwa et al., 2018). In Rurangirwa et al. (2018), CC resulted in larger risk estimates of adverse mental health outcomes than exposure to physical, psychological, or sexual violence. Gou et al. (2019) found that after controlling for physical IPV perpetration by both partners, CC was longitudinally predictive of men’s depression and alcohol abuse, and women’s parenting stress. Additionally, Hardesty et al. (2019) reported that mothers exposed to CC experienced more chronic and high levels of depression compared to mothers who were not exposed to any form of partner violence. Comparatively, no difference was found in depressive symptoms for mothers who experienced other forms of IPV (i.e., situational couple violence) compared to those who experienced no partner violence. Nielsen et al. (2016) found no differences in parental psychopathology in recently separated mothers exposed to CC, situational couple violence, or no violence (note that all three groups met clinical cut-off for depression and PTSD). However, mothers exposed to CC experienced more fear during marriage and after separation compared to non-CC IPV-exposed and no-violence exposed mothers. In the only qualitative study relating to this outcome, CC was linked to emotional exhaustion, low self-esteem, low confidence, and stress, which inhibited parents meeting their children’s emotional needs due to managing their own mental health (Fogarty et al., 2019).
Family functioning (k = 10)
Regarding quantitative evidence under this outcome (k = 4), Broughton and Ford-Gilboe (2017) found CC along with difficulties with custody/access and maternal depression significantly predicted lower family health and wellbeing; however, maternal depression was the only unique predictor. Other quantitative studies reported that after controlling for other forms of IPV, CC was associated with lower coparenting quality (Gou et al., 2019; Hardesty et al., 2016, 2017), lower parenting competence (Gou et al., 2019), and fewer positive feelings toward former partner (abuser) as a father (Hardesty et al., 2016).
Qualitative studies (k = 3) reported that interparental CC was linked to less amicable separation (Hardesty et al., 2008) and limiting access to financial resources and child support required to provide for children (Fogarty et al., 2019; Toews & Bermea, 2017). Five studies (three quantitative, one qualitative, and one mixed-method) found that interparental CC was associated with increased post-separation hostility, harassment (Dragiewicz et al., 2021; Nielsen et al., 2016), fear, and perceived threat of future harm compared to other forms of IPV (Crossman et al., 2016; Hardesty et al., 2016, 2017). Crossman et al. (2016) descriptive case series found that compared to mothers exposed to physically violent CC, nonviolent CC exposed mothers reported similar levels of fear and control during marriage, and more fear post-separation, as well as more coping strategies.
Harsh discipline and child abuse (k = 7)
Quantitative (k = 4) analysis reported interparental CC to be associated with neglectful parenting by the mother/survivor (through CC impacting mothers’ ability to meet children’s needs) (Nicklas & Mackenzie, 2013), father/perpetrators use of more frequent and severe child abuse, and both mothers’ and fathers’ use of harsh or over-reactive parenting behaviors (Emery et al., 2015; Gou et al., 2019; Salazar et al., 2014). The effects on child abuse remained after controlling for physical violence severity (Emery et al., 2015). Qualitative analysis (k = 3) found that compared to those exposed to non-CC IPV, interparental CC was associated with frequent and severe child abuse, and disengaged, harsh, restrictive, and volatile paternal behaviors (Haselschwerdt et al., 2019, 2020). Intervening and being directly victimized during father-perpetrated violence toward mothers was more common among the CC-exposed compared to non-CC IPV exposed (Haselschwerdt et al., 2019). Similarly, McDonald et al. (2015) qualitative study reported that children of parents who threatened to harm pets as a tactic of CC would often intervene in violence to protect the pets.
Parent–child relationship quality (k = 11)
Qualitative studies (note no quantitative evidence for this outcome) showed that father-perpetrated CC was associated with strained and distant mother–child relationships through perpetrators isolating mothers from their children; discrediting or degrading mothers to their children; controlling mother–child activities; making mothers feel guilty or incompetent; dominating and undermining mothering; pressuring mothers to use “tough love” approaches to mothering; and impoverishing mothers in a way that impedes their child’s daily lives (Buchanan & Humphreys, 2021; Dragiewicz et al., 2021; Feresin et al., 2019; Fogarty et al., 2019; Heward-Belle, 2017; E. Katz, 2016, 2019; Toews & Bermea, 2017). E. Katz et al. (2020) found that post-separation, CC-perpetrating fathers used dangerous fathering tactics (intrusive, threatening and/or punishing behaviors), and “admirable” fathering tactics (overt caring, indulgent, concerned and/or “playing the vulnerable-victim father”). The interaction of the opposing fathering tactics was associated with restricted liberty in children.
Using children as pawns (k = 9)
Qualitative studies (k = 8) showed that CC perpetrating parents used their children as tools for ongoing abuse post-separation through filing for custody; denying the children or neglecting the children’s needs; withholding child support; threatening to kidnap the children or actually abducting children (Liversage, 2021); using children and visitation to gain access to the mother and maintain abuse and CC; making false reports to child protection services against the mother; or discrediting the mother in court to manipulate custody arrangements (Callaghan et al., 2018; Douglas & Fell, 2020; Haselschwerdt et al., 2019; Shepard & Hagemeister, 2013; Toews & Bermea, 2017; Watson & Ancis, 2013). Dragiewicz et al. (2021) found fathers used children to enable technology-facilitated CC by coercing children to provide their mother’s digital information (i.e., passwords).
One quantitative study found that the majority (75%) of mothers who reported that their abuser (ex-partner and child’s father) kept children longer than supposed to during visitation and told lies to the children, experienced CC during their relationship (Hayes, 2012). Keeping the children longer and telling them lies were understood as manipulation and control tactics; however, these behaviors were not significantly associated with CC (note this study had a small sample size which may have impacted the nonsignificant results). In Crossman et al. (2016), for 75% of mothers who experienced nonviolent CC, post-separation contact, visitation, and child support exchanges were opportunities for ongoing stalking, harassing, or threatening behaviors by former partners.
The culminated evidence highlights patterns of associations between interparental CC and parenting or parent–child relationship factors; however, the cross-sectional nature of these studies means that causation cannot be assumed.
Child Internalizing and Externalizing Problems
Six studies reported on the links between CC and child psychological outcomes. Regarding qualitative analysis (k = 2), E. Katz et al. (2020) reported that post-separation CC fathering was associated with fear and symptoms of anxiety in children. Moreover, in Shepard and Hagemeister (2013), mothers reported that custody arrangements with CC-perpetrating fathers impacted children’s sense of safety, wellbeing, sadness, confusion, attitudes, and behaviors.
Four quantitative studies reported on child psychological outcomes. Interparental CC was predictive of children’s externalizing (Gou et al., 2019) and internalizing problems after controlling for physical violence, psychological abuse, and mothers’ education (Jouriles & McDonald, 2015). Mitchell et al. (2021) reported a three-way interaction whereby boys aged 6 to 10 years old whose mothers experienced CC violence had higher hyperactivity scores than mothers who reported no violence. Comparatively, adolescent males aged 11 to 17 years whose mothers experienced CC violence had less hyperactivity than those whose mothers reported no exposure to IPV. Van Ouytsel et al. (2020) found that observing father perpetrated CC was significantly associated with adolescent’s subsequent perpetration of digital monitoring behaviors in romantic relationships. The association was nonsignificant for exposure to mother-perpetrated CC.
Developmental Outcomes
Twenty-two studies reported on the effects of interparental CC on child development.
Social-emotional development (k = 5)
Qualitative studies (k = 4) showed CC exposure hindered social, educational, and extra-curricular participation, and fostered situations where children had to self-monitor to avoid violence (e.g., self-manage behaviors and speech to appease the abuser), abandon their home, school, friends, and routine at a moment’s notice (Callaghan et al., 2018; E. Katz, 2016; E. Katz et al., 2020). Haselschwerdt et al. (2021) qualitative study found that participants who reported exposure to interparental IPV, including CC in childhood, experienced abusive relationships in high school, but not in college. Some participants who were exposed to CC violence (and not other forms of IPV) in childhood reported having non-abusing, healthy, and supportive relationships in high school. Haselschwerdt et al. (2021) reported that IPV exposure influenced participants’ beliefs of what was acceptable/unacceptable and the ability to recognize red flags of unhealthy relationships.
Hlavaty & Haselschwerdt (2019) quantitative study found that after controlling for interparental physical violence exposure, exposure to CC was associated with higher levels of bullying victimization, and higher friendship quality. Furthermore, the positive association between exposure to interparental physical violence and bullying victimization was rendered nonsignificant after controlling for CC exposure.
Physical health development (k = 17)
During pregnancy and postpartum (k = 12)
Two qualitative studies examined the impact of CC on perinatal outcomes. Buchanan and Humphreys (2021) reported that CC during pregnancy included reproductive coercion, controlling prenatal visits and decisions, and preventing prenatal care. Hatcher et al. (2016) found that men’s perpetrated CC resulted in difficulty adhering to prevention of mother-to-child transmission (PMTCT) of HIV through increased isolation and being barred access to clinics or medication by their partner perpetrator.
Ten quantitative studies reported on perinatal outcomes. Tiwari et al. (2018) found that after adjusting for sexual/physical violence, CC was associated with significantly higher odds of poor access to prenatal care and skilled delivery care compared to women who did not experience CC. Three studies reported that partner CC was associated with violence against pregnant women, which was in turn associated with higher levels of physical injury during pregnancy and pregnancy complications (Ezeudu et al., 2019; Graham-Kevan & Archer, 2011; Khaironisak et al., 2017). Other studies found a direct association between CC and increased odds of pregnancy complications (after accounting for other forms of IPV) (Avanigadda & Kulasekaran, 2021), intrauterine growth retardation (H. Alhalal et al., 2021), and negative outcomes for breastfeeding practices (Frith et al., 2017; Walters et al., 2021). Tiruye et al. (2020a) found CC-exposure increased the odds of pregnancy loss by 1.72 times compared to mothers who did not experience CC. These odds were slightly higher than exposure to other forms of IPV. Tiruye et al. (2020b) found that experiencing CC increased the odds of neonatal mortality at a comparative magnitude to other forms of IPV exposure.
Early years of life (k = 4)
Two quantitative studies found that interparental CC was associated with increased risk of mortality before the age of five (Asling-Monemi et al., 2008; Garoma et al., 2012). CC produced higher risk estimates than other forms of IPV (Garoma et al., 2012). Specific partner controlling behaviors that increased risk included restricted contact with family and friends, and husbands’ jealousy and anger toward other men (Asling-Monemi et al., 2008). Other quantitative studies showed that maternal exposure to CC was associated with children having lower height-for-age z-scores (no significant association for maternal exposure to other forms of IPV) (Salazar et al., 2012), and lower nutrition status (Heaton & Forste, 2008). Ragavan et al. (2021) qualitative study found that parent CC impacted pediatric healthcare access and quality of care, including: limiting access through insurance, transport, controlling scheduling/cancellations, demanding care at specific locations; dominating healthcare visits through decision making, limiting access to prescriptions, medication, therapy, or subspeciality referrals; using the healthcare system for abuse which decreased healthcare team engagement; and manipulating perceptions of the healthcare team against the survivor.
Mediating/Moderating Factors
Ten studies reported on interactions, buffers, or protective factors of CC and child and family outcomes. However, no empirical data reported on mediating factors explaining the underlying mechanisms through which interparental CC is linked to child outcomes. Regarding protective factors, health and support services were only considered helpful for child and family outcomes when the provider understood the complexities of CC and a lack of understanding reportedly increased survivors’ isolation (Buchanan & Humphreys, 2021; Dragiewicz et al., 2021; Shepard & Hagemeister, 2013). Barriers to support and safety included rural location and limited access to affordable resources (Shepard & Hagemeister, 2013). For parent survivors of CC, protective factors against poor outcomes included higher socio-economic status, education, linguistic ability, strategies for understanding and coping with IPV experiences, ability to use and understand service systems (e.g., the law and community services), focusing on the children, career development, and help-seeking behaviors (Fogarty et al., 2019; Liversage, 2021). In Salazar et al. (2014), mothers’ education level was a protective factor against IPV leading to children’s corporal punishment. However, exposure to CC significantly decreased the protective effect of women’s education level on children’s corporal punishment.
Hardesty et al. (2016; 2017) found that better coparenting quality among CC-exposed mothers and their former partner (CC perpetrator) buffered mothers against post-separation harassment, fear, and perceived threat of future harm, and improved frequency of parental communication and positive feelings toward the former partner as a father. Conversely, Hardesty et al., (2019) reported that for CC-exposed mothers, higher post-separation coparenting conflict was associated with less depression and PTSD. These interactions were in the opposite direction for mothers not exposed to any IPV. Hardesty et al. (2017) reported that CC survivors had more variability in coparenting trajectories compared to survivors of situational couple violence or no exposure to violence.
Child protective factors included working with the parent-survivor to find ways to resist control and restrictions imposed by the perpetrator-parent, maximizing time spent with the parent-survivor, and recognizing the perpetrator-parent’s actions as manipulative (E. Katz, 2016; E. Katz et al., 2020). These protective factors reportedly reduced the impact of CC on limited emotional support, isolation, and quality of parent–child relationships.
Discussion
This study conducted the first comprehensive systematic review of the evidence on consequences of interparental CC on child and family outcomes. Fifty-one studies were identified that collectively provide evidence that interparental CC has significant implications for child and family wellbeing across the domains of: (1) parenting and parent–child relations (including parental psychopathology, adverse family functioning, harsh parenting and child abuse, strained parent–child relationships, and children being used as pawns for abuse); (2) child internalizing and externalizing problems, and (3) child development (social-emotional and physical health development).
Regarding parent psychopathology, multiple studies concluded that parent-survivors of CC were susceptible to adverse mental health outcomes (e.g., Gou et al., 2019; Hardesty et al., 2019; Rurangirwa et al., 2018). Furthermore, in several studies, the adverse impacts of CC on parents’ mental health were more substantial compared to other forms of IPV (e.g., Gou et al., 2019; Rurangirwa et al., 2018). These findings are in line with past research linking IPV more broadly to psychological symptoms in survivors (Tanimu et al., 2016). Limited evidence commented on how parental psychopathology in the context of CC minimized parents’ capacity to manage their children’s emotions due to managing their own distress (Fogarty et al., 2019). As past research has found IPV-related psychopathology to be associated with maternal sensitivity and parent–child attachment (Suardi et al., 2020), additional research is needed to assess the unique impact of CC on these outcomes.
In terms of family functioning, compared to other forms of IPV or no family violence, CC was associated with more acrimonious separations, coparenting difficulties, challenges accessing essential parenting resources, less perceived parenting competence, and more post-separation fear and hostility (e.g., Crossman et al., 2016; Gou et al., 2019; Hardesty et al., 2016, 2017). There were mixed results regarding the interaction of coparenting quality among CC survivors and family outcomes (i.e., Hardesty et al., 2016; 2019). Evidence also indicated that the trajectories of coparenting factors varied substantially among CC survivors (Hardesty et al., 2017). It may be that the variability within the existing (and limited) evidence reflects the variability of survivor experiences post-separation. More research is required to understand the mechanisms by which coparenting factors may influence the impact of CC on family outcomes.
Included studies consistently reported negative correlational outcomes regarding interparental CC and child disciplinary strategies, child abuse, the parent–child relationship, and children’s level of involvement in IPV (e.g., Callaghan et al., 2018; Crossman et al., 2016; Dragiewicz et al., 2021; E. Katz 2016, 2019; Nicklas & Mackenzie, 2013; Salazar et al., 2014). Previous research has documented the link between childhood exposure to interparental violence and child abuse (Holt et al., 2008). The current review reveals that CC is an important driving force for this association (e.g., Emery et al., 2015; Haselschwerdt et al., 2019, 2020). Additionally, as with past research on childhood exposure to other forms of violence (see Holden, 2003), children exposed to interparental CC were co-victims, used as pawns for abuse (e.g., Callaghan et al., 2018; Crossman et al., 2016; Dragiewicz et al., 2021; Liversage, 2021). The evidence concluded that children’s lives, environment, living situations, and their health and wellbeing were often used as leverage to impose CC over the survivor-parent.
The evidence of CC on child psychological outcomes was relatively scarce. Nonetheless, all studies examining this domain found an association between CC and child internalizing and/or externalizing symptoms (e.g., Gou et al., 2019; Jouriles & McDonald, 2015; Mitchell et al., 2021; Van Ouytsel et al., 2020). However, among the four quantitative studies, the methodology and findings were varied. Notably, some evidence indicated that the impact of CC on child psychological symptoms remained after controlling for other forms of family violence (Jouriles & McDonald, 2015). As previous research has recorded the impact of childhood exposure to family violence more broadly and subsequent emotional or behavioral problems (Fong et al., 2019; Holt et al., 2008), additional research is needed to examine the unique impact of CC on this association, as well as relevant mediating and moderating factors. Particularly, no studies in the current review examined exposure to CC and symptoms of trauma, despite links between IPV exposure more broadly and trauma in children (Tailor et al., 2014).
Regarding child development outcomes, the findings indicated that CC exposed children experienced more bullying and less social opportunities (e.g., restricted from engaging in extracurricular activities and spending time with friends) (e.g., Callaghan et al., 2018; Haselschwerdt et al., 2021; E. Katz, 2016; E. Katz et al., 2020). Furthermore, accounting for CC exposure negated the impact of other forms of IPV on bullying victimization (Hlavaty & Haselschwerdt, 2019), indicating that CC is an important mechanism in the link between IPV and child social development. Contrastingly, some studies reported that exposure to interparental CC was associated with better friendship and relationship quality. Haselschwerdt et al. (2021) explained that this may be due to young people’s exposure to, and awareness of parental CC influencing their ability to recognize the signs of unhealthy relationships and subsequently act protectively. No studies in this review examined the impact of CC on children’s education and academic achievement, despite past research finding that interparental conflict impacts these domains (ANROWS, 2017). More research is needed to understand the mechanisms and mediating factors by which CC influences children’s social-emotional and educational development.
The included studies provided converging evidence about the association of exposure to interparental CC and adverse physical development outcomes including: perinatal outcomes; poorer nutrition, growth, and general health; mortality before the age of five; and difficulties accessing quality pediatric care (e.g., Asling-Monemi et al., 2008; Ezeudu et al., 2019; Garoma et al., 2012; Graham-Kevan & Archer, 2011; Khaironisak et al., 2017; Salazar et al., 2012). Importantly, CC was associated with increased risk of early life mortality at comparable, if not slightly higher odds to other forms of IPV (e.g., Tiruye et al., 2020a, 2020b). These results expand on past research linking IPV with increased risks of miscarriage (Tanimu et al., 2016) and highlight the significance of CC as a unique contributor to the adverse impacts of IPV. Furthermore, future research should examine the specific mechanisms through which CC contributes to adverse developmental outcomes and mortality.
Several studies (e.g., Buchanan & Humphreys, 2021; Fogarty et al., 2019; E. Katz 2016; E. Katz et al., 2020; Liversage, 2021; Salazar et al., 2014; Shepard & Hagemeister, 2013) shed light on potential protective factors for the adverse impacts of interparental CC in the following domains: health and support services (e.g., access to affordable services with specialist understanding of CC); parental qualities (e.g., education, employment, help seeking behaviors); caregiving dynamics (e.g., attention on caring for and connecting with children, working with children to resist CC); and child dynamics (e.g., awareness of patterns of abuse). Importantly, evidence found that the protective impact of maternal education was minimized by exposure to CC as opposed to other forms of IPV (Salazar et al., 2014). This finding suggests that CC, compared to other forms of IPV, may more severely undermine mother’s psychological capacity to support children, further emphasizing the importance of parent-survivor support and intervention. More research is needed to understand these interactions and to explore the efficacy of tailored interventions. Furthermore, evidence that children’s awareness of their parents’ CC tactics protects them from psychological symptoms (E. Katz et al., 2020) and later in life partner abuse (Haselschwerdt et al., 2021) highlights the importance for education and population health messaging to increase awareness and help seeking. Evidence of child specific protective strategies was scarce, and future research should endeavor to examine this. Furthermore, no evidence examined specific mediating factors examining the underlying mechanisms through which interparental CC leads to adverse child outcomes. Future research is needed to examine mediators of this association.
Limitations and Implications for Future Research
In addition to the research limitations and recommendations outlined above, the current review highlights existing discrepancies in the definition and measurement of CC (implications for research summarized in Table 2). First, of the included research, some conceptualized CC as partner controlling behaviors only, controlling behaviors in addition to physical violence, or as a specific relationship dynamic involving a pattern of threatening, coercive, and controlling behaviors irrespective of physical violence. The latter most closely reflects fundamental and theoretical definitions of CC (e.g., Stark, 2007). Previous research has reviewed existing operationalizations of CC in adult populations (Hamberger et al., 2017) which should be considered in determining the appropriate use of CC measurement. Future research should use consistent, theoretically sound measures of CC in examining child and family outcomes. Second, majority of included studies were cross-sectional, and therefore correlational in nature. Future research is needed to clarify the causal implications of interparental CC on child and family outcomes. Third, the current review included mostly single informants of child outcomes. Future studies using multiple informants (especially children, service professionals, and LGBTQI+ families) and consistent methodology are required. Fourth, only one study gathered information from both parents, providing limited insight into dyadic dynamics of CC and child and family outcomes. Future research should address this gap.
Implications for Practice, Policy, and Research.
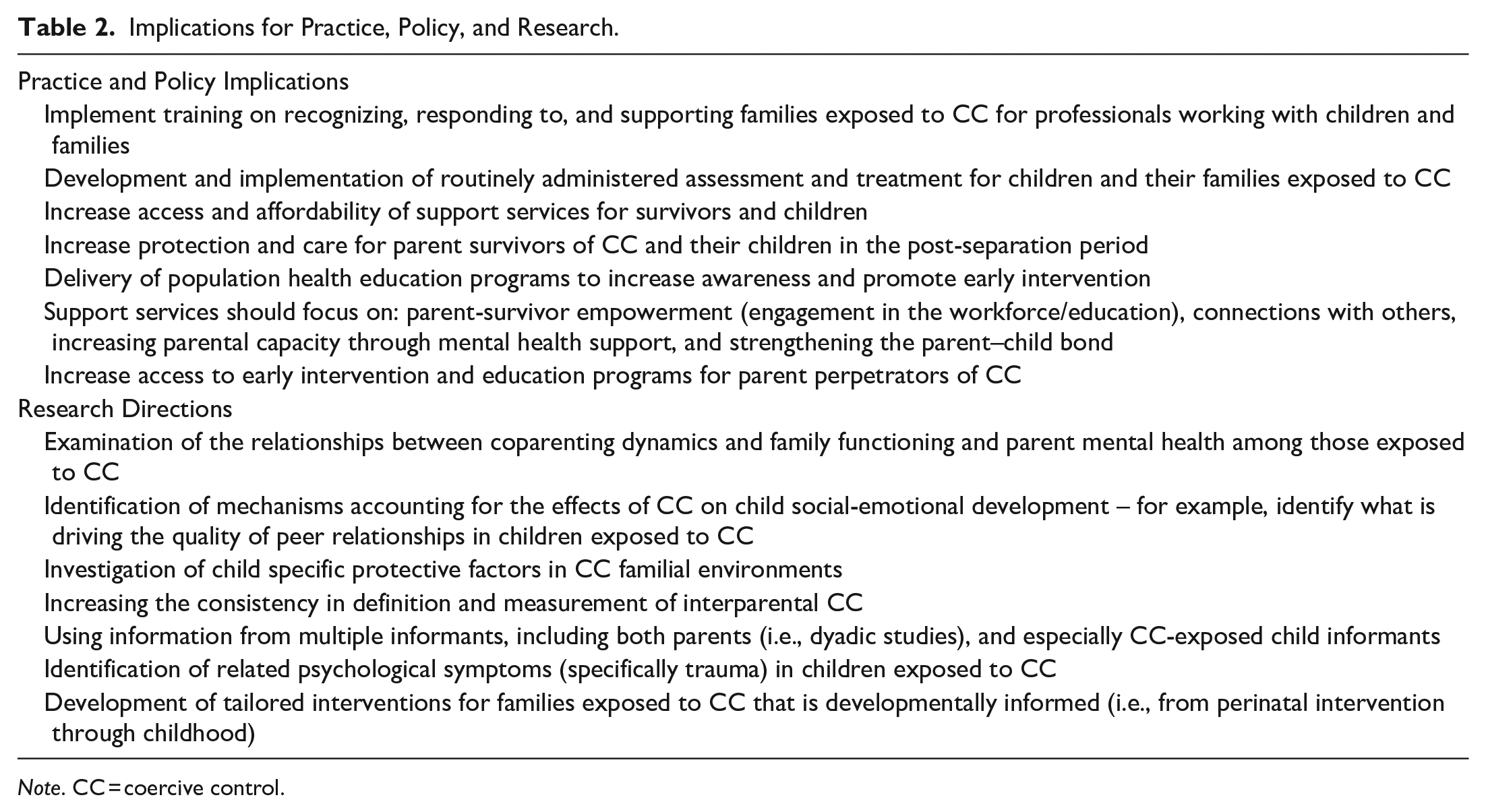
Note. CC = coercive control.
Finally, findings from this review indicate that more research is needed to understand the psychological impacts of exposure to CC in children. Despite thorough evidence that children are co-victims of CC, and adult survivors of CC experience substantial psychological (specifically trauma) symptoms, no studies in the current review examined symptoms of trauma in children exposed to CC. Large-scale quantitative data is required on the wide range of CC impacts in children, and to examine where interventions would be most effective.
Implications for Practice and Policy
Table 2 outlines recommendations for ongoing practice and policy. As there are broad and devastating impacts of interparental CC on children across multiple domains, there is substantial need for consistent approaches of the assessment and intervention of children exposed to CC. Such approaches should address the impacts of CC across the domains of family, psychological, and developmental outcomes and provide evidence-based support specifically for parent survivors of CC. Given evidence that service professionals’ level of sensitivity to and understanding of CC impacts the helpfulness of services, it is crucial that helping professionals have access to training and education on recognizing and supporting families exposed to CC. Furthermore, as affordability and accessibility have been identified as barriers to help seeking, it is important that parent-survivors of CC and their children are given accurate, accessible information about available support services and resources. This effort may be assisted with public health messaging and education to increase the awareness of child and family impacts of CC and encourage parent-survivors to seek help. Support services for survivors and children should focus on increasing safety (particularly in the post-separation period) and identified protective factors including enhanced mental health support, parent-survivor empowerment in education and employment, strengthening supportive connection with others, and strengthening the parent–child relationship. Support and rehabilitation services for perpetrators should focus on awareness and education of the impacts of their actions and behavior change intervention.
In conclusion, this was the first systematic review to examine the broad impacts of exposure to interparental CC on child and family outcomes. The findings provide comprehensive evidence of adverse impacts of CC on child and family dynamics, child psychopathology, and physical and social-emotional development. This research has the potential to inform targeted and tailored interventions for children and their families exposed to interparental CC and provide evidence-based information to inform policy around CC and children.
Supplemental Material
sj-docx-1-tva-10.1177_15248380221139243 – Supplemental material for Interparental Coercive Control and Child and Family Outcomes: A Systematic Review
Supplemental material, sj-docx-1-tva-10.1177_15248380221139243 for Interparental Coercive Control and Child and Family Outcomes: A Systematic Review by Nakiya Xyrakis, Benjamin Aquilina, Ella McNiece, Thomas Tran, Connor Waddell, Aino Suomi and Dave Pasalich in Trauma, Violence, & Abuse
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.