
Abstract
Adolescents are at an increased risk for experiencing dating and relationship violence (DRV) and gender-based violence (GBV). School-based interventions remain an important and frequently used method for DRV/GBV prevention. A clear understanding and description of the different components of school-based interventions specific to DRV/GBV is needed to organize and advance the array of prevention efforts being utilized in school settings. We conducted an intervention component analysis to create a taxonomy for school-based interventions addressing DRV and GBV. We searched 21 databases in July 2020 and updated searches in June 2021, alongside extensive supplementary search methods. We included randomized controlled trials (RCTs) in adolescents of compulsory school-age that were implemented within the school setting which partially or wholly focused on DRV and GBV topics. Our analysis included 68 studies describing 76 different school-based interventions. Through an iterative coding process we identified 40 intervention components organized within 13 activity categories, including both student-directed components and non-student-directed components such as activities for school personnel and family members of students. We also identified components addressing higher levels of the social-ecological model including structural-social and structural-environmental aspects of DRV/GBV which prior reviews have not considered. This taxonomy of components and synthesis of intervention efficacy for DRV/GBV school-based interventions provides a framework for comparing past intervention evaluations and constructing new interventions to address these issues at multiple levels within a community.
Keywords
Adolescents are at an increased risk compared to other age groups for experiencing interpersonal violence, especially dating and relationship violence (DRV) and gender-based violence (GBV) (David-Ferdon et al., 2016). DRV refers to physical, sexual, and emotional violence, including coercive control, between young people in relationships (Young et al., 2018). GBV refers to violence rooted in gender inequality and sexuality, for example, harassment or bullying on the basis of gender or sexuality such as sexual violence, coercion, and assault including rape, within or outside dating relationships (Jewkes et al., 2015). Despite evidence that DRV victimization in adolescence predicts later GBV victimization and that they may share common risk factors (Exner-Cortens et al., 2013, 2017), few previous reviews of interventions to address them among young people have meaningfully considered these constructs jointly (Taquette & Monteiro, 2019).
Such a combined consideration is important as interventions that nominally address GBV may impact DRV and vice versa, underpinned as they are by similar individual, social, and structural causes. For example, restrictive beliefs about gender roles, including beliefs about how men and women should typically act and not act, have been linked to increased DRV and GBV in multiple studies (e.g., Barter & Stanley, 2016; Crooks et al., 2019; Earnest & Brady, 2014; Taquette & Monteiro, 2019; Taylor et al., 2017; Young et al., 2018). Adolescents learn about and develop beliefs on topics like gender roles in unstructured ways, such as portrayals in popular media (Collins, 2011; Rasmussen & Densley, 2016), and structured ways, such as in workshops at school focused on discussing violence-related topics (Crooks et al., 2019; Meyer, 2015).
School-based programs are one of the primary avenues of DRV/GBV prevention undertaken with adolescents (Butchart et al., 2019). These interventions often draw on a range of activities and formats. Interventions can be simple, involving only a single activity for students, such as a film or video as in TakeCARE (Jouriles et al., 2019), or complex, operating across the socio-ecological model (Bronfenbrenner, 1977) and involving an array of different activities for students, staff, and parents over a period of several years as in the Good School Toolkit (Devries et al., 2017). A taxonomy for categorizing and describing the elements of school-based DRV/GBV interventions has not been developed, despite numerous reviews in the past decade. Despite having intervention reporting templates (e.g., Hoffmann et al., 2014) and generic intervention description taxonomies (e.g., Abraham & Michie, 2008) for more than a decade, these tools are often applied inconsistently by researchers when examining specific public health issues such as DRV/GBV. The lack of consistently applied criteria for describing interventions makes post hoc comparisons difficult to accomplish and obscures potential trends that might be found through meta-analysis, for example, which types of activities or other program components might be most effective. This need for consistent criteria has been noted by researchers in the DRV and GBV areas and in other areas of adolescent violence (Gaffney et al., 2021; Piolanti & Foran, 2022; Ttofi & Farrington, 2010).
Some progress has been achieved in the related field of adolescent bullying identifying different intervention components that may contribute to effectiveness. Components could include specific activities engaged in during the intervention or deliberate choices made by the designers on how the intervention is to be delivered. For example, Ttofi and Farrington (2010) conducted a systematic review and meta-analysis of anti-bullying school-based interventions and coded components ranging from activities for students such as whether they engaged in working with peers or watched videos, to school-wide activities such as conferences and policy review, and program material targeting adults such as parents or teachers. A decade later they updated their systematic review and meta-analysis with a closer examination of intervention components producing a taxonomy of 20 components organized within seven levels of the social ecological framework (Gaffney et al., 2021). That taxonomy, while useful, is situated heavily within the bullying literature. Coded components are closely linked to bullying-related content considerations, such as styles of classroom management and response to bullying, informal and formal peer involvement in bullying situations, discussions of how mental health links to bullying, or the inclusion of punitive versus non-punitive disciplinary methods in responding to bullying behaviors (Gaffney et al., 2021). Although this provides a useful comparison and reference for considering DRV/GBV school-based interventions, more specificity is needed.
Unfortunately, no prior reviews of DRV/GBV school-based programs have utilized a similar or comprehensive component coding schema as that of Gaffney et al. (2021) or even the earlier schema from Ttofi and Farrington (2010); only five components were coded, including whether interventions included a curriculum or not, who implemented the intervention, whether a community component was included or not, whether the intervention was implemented in single- or mixed-sex groups, and the pedagogical approach (participatory, didactic, or activity-based). Another systematic review and meta-analysis of relationship violence prevention interventions (Fellmeth et al., 2013) coded only the intervention setting (school, university, or community) and the duration of the intervention. A similar review of adolescent dating violence and sexual violence (Lundgren & Amin, 2015) coded interventions into one of five classifications, including parenting programs, targeted interventions, school-based programs, community-based programs, or economic empowerment programs. Examples of the different components typical for each type of classification were provided but there was no discussion or framework for examining those components presented. More recent meta-analyses of school-based DRV and physical/sexual violence prevention interventions report on specific components of interest, such as who presented the intervention (teacher, external staff, or graduate student) (De La Rue et al., 2017) or whether there was some type of parental involvement (Piolanti & Foran, 2022). One recent systematic review and meta-analysis of bystander intervention programs coded for a variety of components, including the format in which the program was typically delivered (in-person, video, web/computer delivered, or ad/poster campaign); the context of delivery (individual with facilitator, small groups, large groups, or alone); who delivered the program (teachers, school administrators, coaches, peers, medical professionals, external agency staff, or self-guided); and whether the program implementation was monitored or not (Kettrey et al., 2019). While these elements are no doubt important to consider, the rationale for why these elements and not others were coded for as intervention components is not clear.
A taxonomy of DRV/GBV intervention components will most directly help to simplify cross-intervention comparisons (Sutcliffe et al., 2015). Additionally, having a list of potential components would also enable designers to consider which “active” components—that is, those based on a clear understanding of past success—could be included in new interventions. Explicit consideration and description are especially needed for components that address target audiences beyond the adolescent students themselves. Although some review studies have looked at the involvement of parents or school staff (Huang et al., 2019; Rizzo, 2021), aspects of the physical and social school environment have been largely neglected. These structural components may be especially important considering research demonstrating school “hot spots” where DRV/GBV frequently occur (Bonell et al., 2013).
Current Study
Our goal in this study is to provide a systematic review and intervention component analysis of DRV/GBV school-based interventions with the goal of creating a taxonomy for program description.
Methods
We conducted this systematic review and intervention component analysis as part of a larger mixed-methods systematic review and evidence synthesis project (NIHR130144) examining evidence relating to school-based interventions for the prevention of DRV and GBV. The protocol for this study is registered on PROSPERO (Protocol CRD42020190463).
Inclusion and Exclusion Criteria
Full study inclusion and exclusion criteria are detailed in Supplemental Appendix A. Briefly, this included only randomized controlled trials (RCTs) or cluster RCTs that reported outcome evaluation data relating to DRV and/or GBV. Study designs could include comparators such as business as usual, waitlist control or another active intervention. We included studies with children in compulsory education (e.g., aged 5–18 years) attending school. We included evidence relating to interventions implemented in school contexts with students as separate from or part of relationships and sexual education classes that schools may provide. Interventions could be single-component or multi-component, or implement the same type of approach (e.g., group or classroom-based intervention) in a range of ways. Included interventions needed to focus in whole or in part on DRV and GBV, and could be universal, selective, or indicated. Included studies could be primary prevention (reducing incidence of DRV and GBV) or secondary prevention (improving responses to DRV and GBV). Included studies could include gender-specific groups (e.g., boys or girls only).
We excluded interventions that did not seek to address DRV and GBV outcomes, for example, interventions focusing on another health promotion topic, such as healthy eating, that may have had an “opportunistic” effect on DRV or GBV outcomes, but that do not describe prevention of DRV or GBV in intervention descriptions. We also excluded interventions that were not delivered in compulsory education (e.g., university-based sexual violence prevention, or statutory/third sector youth services); or were not delivered at least in part in school contexts.
Search Methods
The search strategies were designed by an experienced Information Specialist and peer reviewed by a second Information Specialist. In July 2020, we searched the following bibliographic databases from inception and without limitation on date, language, or publication type: MEDLINE, Embase, PsycINFO, Social Policy and Practice (Ovid); CINAHL, ERIC, British Education Index, Education Research Complete, EconLit, Criminal Justice Abstracts (EBSCO); Cochrane Database of Systematic Reviews (CDSR) and the Cochrane Central Register of Controlled Trials (CENTRAL); NHS Economic Evaluation Database (NHS EED via the Centre for Reviews and Dissemination); Social Science Citation Index and Conference Proceedings Citation Index (Web of Science, Clarivate Analytics); Australian Education Index, ProQuest Dissertations & Theses Global, Sociological Abstracts including Social Services Abstracts, Applied Social Sciences Index and Abstracts (ProQuest); Trials Register of Promoting Health Interventions (TRoPHI) and Bibliomap (EPPI-Centre); and Campbell Systematic Reviews (Campbell Collaboration).
The search strategies included both free-text terms and subject headings for the school setting and DRV/GBV outcomes. We updated the bibliographic database searches in June 2021, with a revised strategy developed to improve precision, and added further search terms for named interventions. Full strategies for the original and update bibliographic database searches are available in the Supplemental Appendix B.
We completed forwards and backwards citation chasing on included studies in Scopus (Elsevier), Web of Science (Clarivate Analytics) and Google Scholar, and reviewed the reference lists of relevant systematic reviews and reports. To identify linked studies and further grey literature, we conducted targeted searches in Web of Science and Scopus using first and last author names, and searched Google Scholar for specific intervention names (e.g., Project Respect; Shifting Boundaries). We browsed publication lists on key websites (including USAID: www.usaid.gov; the National Criminal Justice Reference Service: www.ncjrs.gov; and UNGEI: www.ungei.org). We also searched clinical trial registries including ClinicalTrials.gov and WHO ICTRP. We downloaded search results into EndNote X9.2 (Clarivate Analytics) for deduplication. We conducted deduplication using EndNote deduplication functionality, plus manual checking. Subsequently, a single search file was uploaded to Covidence software (Covidence.org). Covidence provided further duplicate matching before screening.
Study Selection
We completed a pilot screen of a random sample of 100 records and discussed disagreements. Each record was then independently screened by two reviewers in Covidence. Records retained after this stage were accessed in full text and assessed against the inclusion criteria in duplicate and assigned to one or more evidence types (implementation/process, outcome, economic evaluation, and mediation/moderation). Only records that provided outcome evidence were included in this intervention component analysis and synthesis.
Data Extraction
Two reviewers undertook data extraction independently using standardized, piloted forms. Where disagreements occurred, a third reviewer was involved. If included studies were reported in languages that could be translated by the review team, a review author completed the data extraction form in conjunction with a translator.
Full extraction details for the larger project included information on study details; study design and methods; outcome measures; relevant mediation and moderation analyses; and economic data. Basic study details are listed by intervention in Supplemental Appendix C.
For the effectiveness synthesis, we considered four behavioral outcomes measured by either self-report or official records: DRV victimization, DRV perpetration, GBV victimization, and GBV perpetration. Our definition of DRV included emotional-verbal abuse, physical abuse, sexual violence, and cyber abuse which occurred within the context of a relationship. Our definition of GBV similarly included verbal harassment, physical violence, sexual violence, and cyber violence which occurred because of someone’s actual or perceived gender identity and expression or sexual orientation. We did not include outcomes related to “honour-based” violence, forced marriage, or genital mutilation. Additionally, we did not consider outcomes related to knowledge, attitudes, or social norms.
For the intervention component analysis, intervention descriptions were extracted as free text from: the body of the text, supplemental files cited in text, and when necessary, consultation with the authors. If authors were not traceable or information was unavailable from the authors within 2 months of contacting them, the study was not included in this synthesis.
Analysis Plan
We used intervention components analysis (Sutcliffe et al., 2015) to synthesize intervention descriptions into a descriptive taxonomy for DRV/GBV interventions paired with a basic synthesis of intervention efficacy to reduce DRV/GBV. Intervention components analysis is an inductive approach to comprehensively describing and categorizing intervention components in a target body of evidence. This is an appropriate method to describe intervention components when these components do not fit into pre-existing taxonomies of behavior change.
Two authors (AJR and GJMT) used open coding to independently generate comprehensive lists of possible intervention descriptors from five different intervention descriptions roughly selected to represent surface-level diversity, including length of program description, year of study publication, and type of publication (e.g., thesis, report, peer-reviewed article, etc.). The two lists were compared and combined. Using principles of axial coding, the two reviewers proceeded through the remaining intervention descriptions, collapsing codes, adding new codes as required, and meeting periodically to compare codes, determine if new axial codes were required and organized axial codes into categories. Findings were sense-checked with our advisory and stakeholder groups for face validity. The result was a comprehensive list of component descriptors to characterise included interventions, organized by relevant categories. Finally, we examined a co-occurrence matrix to identify if the identified components tended to combine with other components within interventions (frequencies in Supplemental Appendix D).
Intervention effectiveness was coded as whether an intervention was associated with a significant reduction in violence compared to control interventions. Interventions which reported a significant reduction in any type of DRV perpetration, DRV victimization, GBV perpetration, and/or GBV victimization for the intervention sample compared to the control sample were coded as “successful.” Interventions not showing significant reductions in any of those DRV/GBV outcomes for the intervention sample compared to the control sample were coded as “unsuccessful.”. Effectiveness coding by intervention is provided in Supplemental Appendix C.
Results
Searches yielded 40,160 records after de-duplication, of which 793 were screened in full text having not been excluded based on title/abstract review (see Figure 1). This combines the records from bibliographic database searches (n = 26,016) and additional searches (n = 14,144) after deduplication. In the intervention component analysis, we included 68 distinct studies reporting on 76 different DRV/GBV school-based programs.
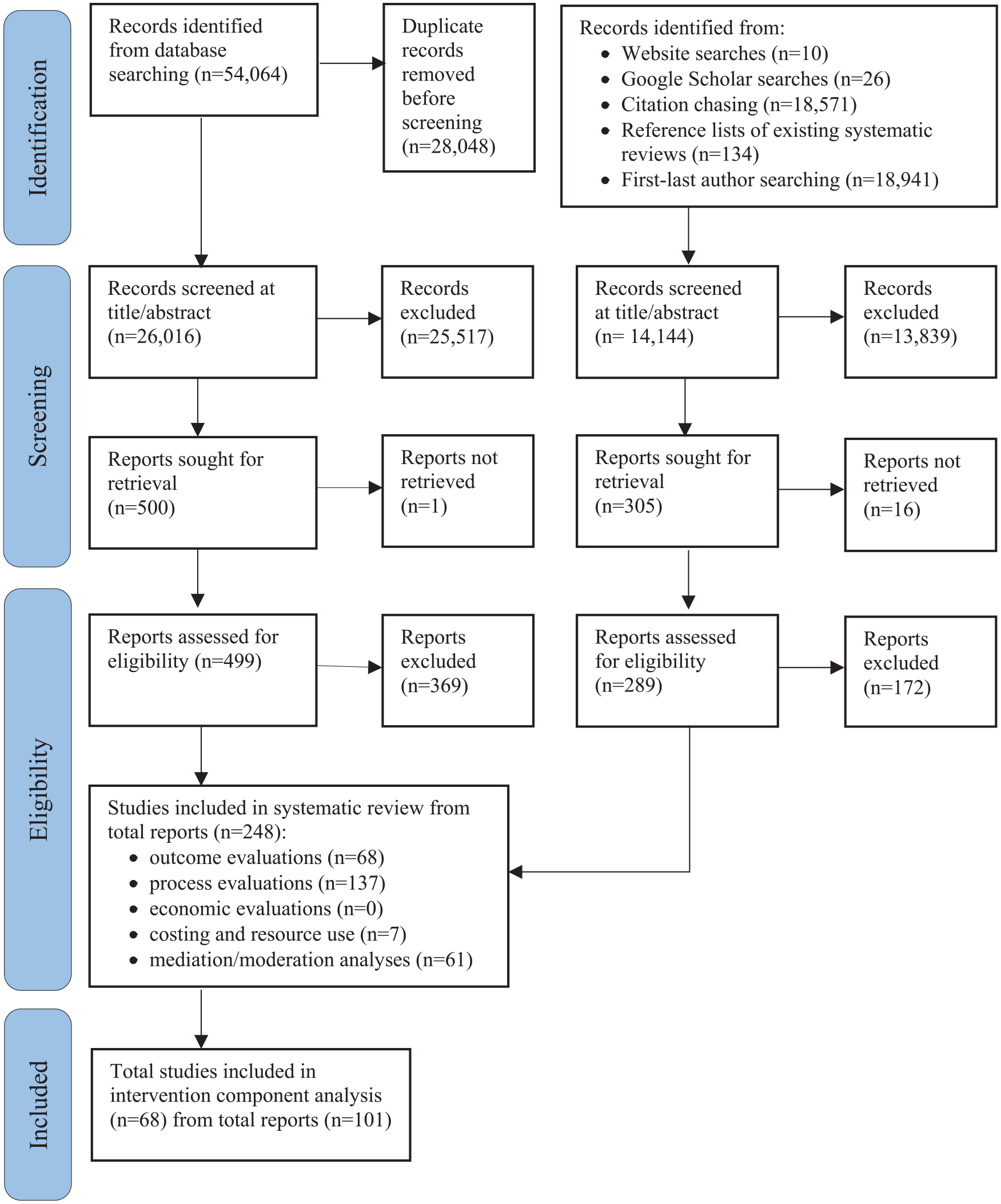
PRISMA flowchart.
Characteristics of Included Interventions
The majority of the interventions (63%) were conducted in North America, with the remaining split across Europe (13%), Asia (11%), Africa (9%), and South America (4%); across this, 50 interventions were undertaken in high-income country contexts. Sample size of the studies ranged from 47 to 89,707 participants (median 839). The interventions were mostly delivered in middle or high school settings (i.e., ages 11–18 years); only four (5.9%) also or solely included students within primary/junior school settings. Students’ age ranged from 9 to 19 years. The majority of interventions were conducted with students of both sexes, while four and six interventions were conducted exclusively with male and female students, respectively. Only 2 studies permitted students to record their gender beyond the binary, and only 5 studies reported students’ self-reported sexuality. No studies were conducted solely with LGBTQ+ students. Half of included studies (52.9%) reported race or ethnicity of students; of these more than 50% of students identified as White/Caucasian (37.8%), Hispanic or Latino (18.9%), and Black or African American (10.8%). School and/or students’ socioeconomic status (SES) was reported for 35 studies, of which 11 were identified as including more than 50% of students from lower SES backgrounds (e.g., free or subsidized school lunches, etc.).
Intervention Component Analysis Results
The intervention component analysis examined 76 different programs. All the programs were school-based interventions to prevent DRV and/or GBV but with diverse goals and program components. Program descriptions varied in length, ranging from a single paragraph to full curriculum syllabi to individual daily lesson plans and scripts. The range of topics addressed as part of the program description also varied considerably, including topics such as: specialized technology or activities used; general and specific content covered; intended goals and objectives of the program; physical space; settings, and timing where the program took place; and who delivered the program as well as their training and preparation prior to program delivery.
The initial open coding generated a list of 143 different codes roughly organized around 11 preliminary groups of codes relating to: topics addressed in the program content; skills discussed or practiced during the program; activities students engage in during the program; intended result of those activities at the end of the program; aspects describing the individuals and technology delivering the program; details about the location in which the program took place; the presence of others during the program; how students are guided through the program; the medium(s) through which program material is communicated; details of how school staff were involved with the student portions of the program and/or received their own material; and details of how the extended community (parents, families, local groups, etc.) were involved with the student portions of the program and/or received their own materials. Through discussions and consultation with both our advisory panel of practitioners, scholars, and researchers in the field of school-based program implementation and our youth advisory panel several elements of the initial coding list were eliminated as not part of a salient frame for describing and comparing the activities in which participants engage in during an intervention. This resulted in removing from the final codebook several practical element codes, such as the different definitions of different types of violence presented in each intervention, and also several more abstract element codes, for example, the wide array of intended moral, psychological, or social, mechanisms of an intervention as described by the creator. The remaining codes were re-organized into a final codebook of 40 intervention components organized into 13 different program activity types. These describe the activities in which students, school staff, and the extended local community may participate in as part of an intervention.
Nine of those program activity types (and their 25 intervention components) targeted student-level change mechanisms while four program activity types (and their 15 intervention components) targeted non-student-level change mechanisms, including school personnel, family/parents of students, structural environmental and structural social aspects. Frequency of components and descriptions are presented in Table 1.
Taxonomy of DRV/GBV Intervention Components: Frequency, Description, and Intervention Success.
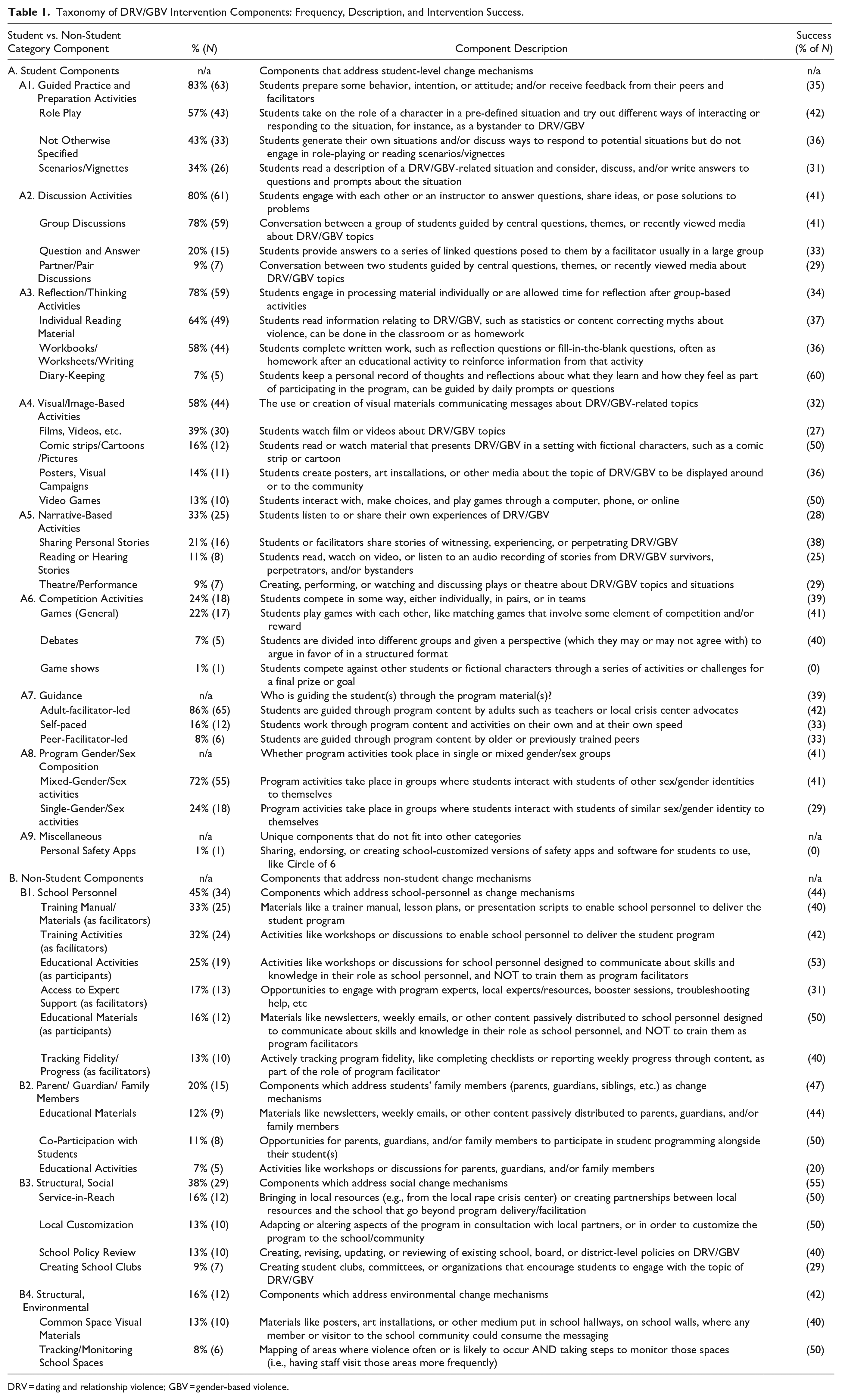
DRV = dating and relationship violence; GBV = gender-based violence.
A. Student Intervention Components
A1. Guided Practice and Preparation Activities
The majority of evaluated programs (83%, n = 63) included activities where students received guidance and feedback on practiced behaviors, hypothetical intentions, or general attitudes related to how they might respond to DRV/GBV in some way in the future . Such activities provide adolescents with an opportunity to test out ideas for behavior/intentions with their peers and/or a facilitator to provide feedback, as well as observe the ideas of their peers. This most frequently took the form of active role-playing (57%) where students act out how they would respond in a situation where they are the target or a bystander to DRV/GBV. For example, in the JOVEN intervention students engaged in role-playing activities “to act out healthy bystander behaviors with friends who were in risky situations and at risk for physical or sexual harm” (Gonzalez-Guarda et al., 2015, p. 412). Another method of guided practice and preparation included providing written vignettes (34%) describing DRV/GBV to which students would write their hypothetical reaction. For example, in the RITDVPP intervention, students considered a range of teen dating violence (TDV) vignettes and “brainstormed healthy behaviors to solve real life relationship dilemmas.” (Silverman, 2000, p. 75). About half of the programs engaged in guided practice and preparation not otherwise specified in the program descriptions (43%). This included programs that provided no detail beyond stating “skill building” or “skill practice” happened during the program sessions.
A2. Discussion Activities
Most programs (80%, n = 61) included discussion-based activities where students would engage with each other in groups (78%), in pairs (9%) or through question-and-answer formats with their instructor (20%). Most studies simply mentioned that discussions (or questions, etc.) took place without further elaboration.
A3. Reflection/Thinking Activities
A majority of evaluated programs (78%, n = 59) included activities in which students engaged in individual processing of material. This was most often through providing individual reading material (64%) or completing workbooks/worksheets/writing assignments (58%). A smaller number of programs included diary-keeping (7%) as part of the program sessions. For example, the It’s Your Game intervention required students to complete “individualized journaling activities. . .to help students personalize information” (Peskin et al., 2014, p. 1472).
A4. Visual/Image-Based Activities
More than half of evaluated programs (58%, n = 44) included activities centered around visual materials such as posters, films, video games, or cartoons. The most common visual program element was the use of a film or video (39%), which often served as the basis for a discussion or series of discussions among the students (e.g., Pacifici et al., 2001). Graphic novels or cartoon strips were used by some programs (16%), for example in Let Us Protect Our Future (Jemmott et al., 2018) a comic workbook was distributed to students to provide characters and a storyline they could follow along with throughout the intervention. Some programs included posters and other visuals (14%) which were put up around the school and classrooms. For example, Safe Dates (Foshee, 1998; Foshee et al., 1998, 2000, 2004, 2005) not only provided visual materials with key program messages but engaged students in creating more visual materials such as posters as a summative or concluding activity so students showed what they learned during the intervention. Video games, either via the internet, on a local personal computer or a CD-ROM, were also used in some programs (13%). In a few cases, the entire program consisted of playing the video game (e.g., PR:EPARe, Arnab et al., 2012) whereas, in other programs, playing the video was to supplemental other activities (e.g., Me & You, Peskin et al., 2019)
A5. Narrative-Based Activities
A third of evaluated programs (33%, n = 25) included activities that revolved around listening to the stories of others’ experiences with DRV/GBV or sharing one’s own stories of experiencing DRV/GBV. Often this included asking students to share personal stories (21%), for example in IMPower adolescent women were encouraged to share assault experiences as part of self-defense training and also to inform resource dissemination to survivors of prior DRV/GBV in the class (Baiocchi et al., 2017). Other interventions involved reading or listening to personal stories (11%). This frequently involved bringing in guest speakers to talk with students, or students reading stories from survivors, perpetrators, or bystanders to violence. In Expect Respect, the entire third session involved students listening to and talking with a survivor of relationship abuse from the local area, to show what violence could look like in their own community (Roberts, 2009). A small number of programs (9%) incorporated theatre shows, skits, or plays into the activities for students (such as in Benzies & Batchies, de Lijster et al., 2016). Some programs that used theatre incorporated students into the creation process of the performance. For example, in Youth in Action Bystander Theatre (Gale, 2011), students “present an unsolved problem to the audience. The problem posed was a scene that comes from a real-life story of one of the participants, who then, drawing upon her real-life experiences, plays the protagonist in the scene.” (p. 17). Most programs provided a script for students to learn and perform for their peers (e.g., de Lijster et al., 2016; Merrell, 2004).
A6. Competition Activities
A quarter of evaluated programs (24%, n = 18) included activities with a competitive component where two or more players or teams compete in giving answers, finishing a story or game. Although program descriptions often referred to these activities as games of some sort (22%), the content of these could be more serious than a typical child’s game. For example, in Katie Brown Educational Program (Joppa et al., 2016), the gameplay involved students practicing assertive communication skills when confronted with DRV-related behaviors. The game could also be a contest, as in the You-Me-Us program (Coyle et al., 2019), where students competed to design a healthy relationship message, with the winner’s idea being used in the actual prevention campaign materials in their school community. In other programs, the games had little relevance to violence but instead were meant to lighten the mood or break up the more serious content, as in the Gender Equity Movement in Schools (GEMS) program, where the school-based campaign included “games and races” (ICRW, 2017, p. 9) alongside essay writing, speeches, and pledges for equality and nonviolence. A few programs mentioned debate (7%) as a form of competition among students during program sessions, although none of those programs provided examples or elaborated upon the nature of the debates or the topics that students debated. One program utilized a game show concept (PR:EPARe; Arnab et al., 2012) within a video game so that students could engage in competition virtually with the computer rather than against each other.
A7. Guidance
The relationship between the student in the program and the person facilitating or guiding the program was coded to be inclusive rather than discrete. Portions of a program could be facilitated by an adult, a peer, or by the students themselves. The majority of evaluated programs were adult-facilitator-led (86%, n = 65). Adult facilitators could include external facilitators from a national or local agency, a trained team of presenters or performers from a local university, a single presenter (usually the creator of the program), or school personnel who had received training or other materials to help them present lesson plans or other program elements. Some evaluated programs were peer-facilitator-led (8%, n = 6). These students usually attended additional meetings and trainings prior to the program implementation to learn how to facilitate the program. In some programs peer facilitators volunteered (e.g., Coyle et al., 2019) and in other programs peer facilitators were nominated by students or school staff because they were seen as leaders or influential in school (e.g., Miller et al., 2015). Finally, some evaluated programs were self-paced (16%, n = 12) meaning that the students usually worked through material individually and only came together as a group for a few topics. This could allow students to work at a pace that best suited them and allowed them to fully comprehend material through re-reading or re-viewing work material additional times, etc., until they were ready to move to the next topic.
A8. Program Gender/Sex Composition
The nature of whether classes were single or mixed sex/gender or a combination of these was coded to be inclusive rather than discrete. Some programs included sessions that were single sex/gender early on in the program, but later sessions were mixed (e.g., Filho, 2017). Programs that were entirely self-paced (i.e., only involve individual work) were excluded from this coding as this was meant to capture the potential for interaction between students of the same or different sexes/genders, and no interaction at all took place in these programs. The majority of evaluated programs used mixed sex/gender groups (72%, n = 55) for at least one session or activity. Only a quarter of evaluated programs used single sex/gender groups (24%, n = 18) for at least one session or activity.
A9. Miscellaneous
A single program utilized a component that did not fit into another other category nor was anything similar used in any other program. Project Respect in the United Kingdom (Meiksin et al., 2020) encouraged students to download and use the freely available personal safety app “Circle of 6” (www.circleof6app.com). The app was used on mobile devices and “helps individuals discreetly request help from their pre-identified contacts for support if threatened by/experiencing dating and relationship violence” (Meiksin et al., 2020, p. 4).
B. Non-Student Intervention Components
B1. School Personnel
About half of evaluated programs (45%, n = 34) included activities or materials designed specifically for school personnel. Programs which utilized school personnel as facilitators often provided trainings and workshops to prepare them to deliver the program (32%). These trainings could not only cover the specific program content of DRV/GBV information but also skills for facilitating discussion about sensitive issues with adolescents or positive classroom management strategies (e.g., Achyut et al., 2016; Jewkes et al., 2019).
Some programs had manualized lesson plans or scripts (33%) which school personnel received so as to make the program delivery as consistent across schools as possible (e.g., Safe Dates, Foshee et al., 1998). Program materials for school personnel sometimes included progress tracking checklists or other methods of charting fidelity (13%) concerning how the program was delivered, the pace of the program delivery, and whether content was or was not included for any reason (e.g., Macgowan, 1997). A few programs included specific access to expert support as a resource for school personnel (17%). For example, coaches responsible for delivering the Coaching Boys Into Men program received biweekly technical assistance from local advocates for the duration of the sports season, in order to review how content was progressing and address any challenging situations that might arise (Jaime et al., 2018).
A few programs targeted school personnel as the recipients of the program directly, rather than as agents delivering the student program. This could include specific trainings for school personnel (25%), such as in the Expect Respect program where teachers received training “to raise awareness of bullying and sexual harassment and to prepare school personnel to respond effectively to witnessed or reported incidents” (Rosenbluth et al., 2004, p. 214). This could also include materials shared with school personnel (16%), such as in the Me & You program in which a newsletter was emailed to all school staff with content that included “DV types, unhealthy relationship behaviors, importance of addressing DV in schools, and the ‘recognize-respond-refer’ model” (Peskin et al., 2019, p. 1421). This type of passive material could be reviewed by school staff at their own time and saved as reference material for responding to situations in the future.
B2. Parent/Guardian/Family Member
A fifth of evaluated programs (20%, n = 15) included components designed for family members of students participating in the program. Some programs involved family members as co-participants (11%) with the students during some of the student programming. For example, the JOVEN curriculum invited family members to attend the final session where students practiced their newly learned healthy communication skills in negotiating topics such as curfews and dating (Gonzalez-Guarda et al., 2015). Similar to school personnel, family members could also be the recipients of the program directly. A few programs held special activities for family members (7%), such as an orientation held with the local parent–teacher association to explain the program to parents, encourage them to ask their students about the program topics, and provide community resources if they needed additional support (Macgowan, 1997). Other programs simply sent materials for family members (12%), such as pamphlets, booklets, brochures, or weekly newsletters, home with students for their family members to read if they chose (e.g., Ekhtiari et al., 2014; Wolfe et al., 2009)
B3. Structural-Environmental
A small number of evaluated programs (16%, n = 12) included specific activities and tasks that aimed to address structural-environmental elements of the school setting. These activities were concerned with improving the physical features of the school building and/or spaces to address DRV/GBV. Programs addressed structural environmental features in two ways. Several programs included visual materials in common spaces (13%), such as posters or other artwork that could be placed in hallways, on bulletin boards, as screensavers in the computer labs, etc. Often students were involved in creating these visual materials so that they resonated more strongly with the specific school context. These materials helped to alter the school climate by communicating the values of the school (anti-violence, pro-helping, etc.) to anyone who walked through school common spaces. A few programs also included efforts to track and monitor school spaces (8%). Spaces with low or no adult supervision were often rated as the most violence-prone and riskiest areas of a school campus (Astor et al., 2001). To address this issue, programs asked students to identify areas and then planned staffing changes to better monitor those areas (e.g., Taylor et al., 2013).
B4. Structural-Social
Just over a third of evaluated programs (38%, n = 29) included specific activities and tasks that sought to change the structural-social climate of the school setting. This could include a number of different efforts. Some programs sought to improve the school climate by facilitating service-in-reach from local resources (16%) who could speak about the anti-violence work going on in their own community and promote local support services for survivors (e.g., Mathews et al., 2016; Muck, Schiller, & Kartner, 2018; Muck, Schiller, Zimmermann, et al., 2018). Other programs required the school board or school staff to review or create policies (13%) for how they would respond to DRV/GBV. The goal of this policy review in the Project Respect program was to strengthen or create policies that would hold perpetrators accountable and support survivors in seeking help after violence (Meiksin et al., 2020). A few programs started by having local staff and community members review the existing program content and work together to make changes to customize the program material (13%) to the specific school, community, region, or country context where it was being implemented. For example, prior to the implementation of the Jesse prosocial video game, a diverse group of school and community stakeholders reviewed the content to ensure it was culturally relevant and appropriate for their Caribbean context (Boduszek et al., 2019). Finally, a few programs included the creation of school clubs or after-school activity groups (9%). These groups of students could sometimes be part of delivering program materials, such as with the high school-aged “brand ambassadors” in the Dating Matters program (Niolon et al., 2019). Additionally, such clubs could help ensure that the program would persist beyond the timeframe of the study by incorporating the program aims into a more stable organizational structure at the school (i.e., special interest clubs and organizations for students).
C. Combinations of Components
Although many interventions evaluated here were very complex or lasted several semesters, no intervention included every different component. Individual interventions utilized an average of 8.70 different components (SD = 4.17, range: 2–23). All interventions except one utilized one or more student component, with an average of 5.32 different student components (SD = 2.53, range: 0–13). Only two-thirds of interventions (62%, n = 47) utilized at least one non-student component, with an average of 3.83 different non-student components (SD = 2.85, range: 0–10).
Several pairs of components occurred frequently (i.e., were observed in more than half of the interventions). These pairs tended to be student components with other student components. The most frequently observed combinations were of adult-facilitator-led activities paired with group discussions (n = 56), mixed-gender activities (n = 47), individual reading material (n = 42), workbooks (n = 40), or role-play (n = 39). Also frequently paired was group discussions with mixed-gender activities (n = 44), individual reading material (n = 40), role-play (n = 40), and worksheets (n = 38). Mixed-gender activities also paired often with individual reading material (n = 37), workbooks (n = 36), and role-play (n = 35). Considering non-student components, training activities paired often with training manuals/materials for school personnel as intervention facilitators (n = 24), and both paired equally often the intervention being adult-facilitator-led (n = 25) and with leading group discussions (n = 21). Collapsing activities within categories, we note that about a third to a half of interventions that used a guided practice/preparation activity were also likely to use any reflection/thinking activity except diary-keeping (n = 17–28), be adult-facilitator-led (n = 21–39), include group discussions (n = 21–40), and/or to include some mixed-gender activities (n = 21–35). No other pair combination trends between categories emerged.
Intervention Efficacy Synthesis Results
Only a third of the included interventions (38%, n = 29) were coded as successful in reducing DRV/GBV victimization or perpetration when compared to control interventions. Considering proportions of successful interventions across study characteristics, successful interventions were somewhat more likely to be set in high-income countries, though some few successful interventions did take place in middle- and low-income countries. No other trends emerged regarding other characteristics associated with intervention success, including country of implementation, mean age of students, percentage of male or female student participants, school/grade setting of implementation, or intervention duration. Student sexuality, ethnicity, and SES were not consistently reported in enough studies to allow for even this basic examination.
Efficacy for Individual Components
We next examined intervention success in relation to the identified intervention components. The highest success rates were 61% (11 of 18) for interventions with single gender activities and 60% (3 of 5) for interventions with diary-keeping. The lowest success rate was 20% (1 of 5) for interventions with educational activities for parents/guardians/family members. All individual component and category success rates are provided in Table 1.
Efficacy for Component Pairs
The reviewed interventions demonstrated 86% of the 780 total possible pairings that our 40 components could have formed; about 16% of those pairs were only in a single intervention. For parsimony, we restrict our observations below of component-pair efficacy trends to only pairs which were in two or more interventions, and which were likely to be in successful interventions (see Supplemental Appendix D for all individual pair incidences and percentage success rates).
Interventions with comics and cartoons were almost always successful regardless of pairings, with the exception of comics paired with scenarios and comics paired with films. Interventions that paired films and included activities/materials for school personnel as participants were mostly successful. Question-and-answer activities paired well with parent/family co-participation and diary-keeping. Debates were successful when paired with group discussions or individual reading material. Guided practice/preparation activities were mostly successful when in interventions that also included some single-gender activities. Scenarios/vignettes were mostly successful when paired with educational materials for parents/family members.
Workbooks were somewhat likely to be successful when paired with comics/cartoons, video games, diary-keeping, single-gender activities, and self-paced interventions. Diary-keeping was mostly successful in various pairings, including with most of the discussion and reflection/thinking categories, and also with comics/cartoons, role-play, mixed-gender activities, and in adult-facilitator-led interventions. Individual reading materials were mostly successful when paired with debates, diary-keeping, service-in-reach, and comics/cartoons.
Interventions in which students shared personal stories showed some success when done with question-and-answer activities, theatre activities, service-in-reach, single-gender activities, or school personnel educational activities. Interventions with both single and mixed gender activities were very likely to be successful. Single-gender activities were also generally successful when paired with local customization, service-in-reach, any activities in the guided practice/preparation category, or with any activities for school personnel.
Interventions that included parent/family co-participation alongside students were very successful when paired with question-and-answer activities, self-paced guidance, local customization, and nearly any visual/image-based activity except for posters/visual campaigns. Interventions that included educational materials for parents/family members were also highly successful when paired with any visual/image-based activities, alongside scenarios/vignettes, or with self-paced interventions. Local customization was likely to be successful in interventions when paired with single-gender activities, parent/family member co-participation alongside students, and guided practice/preparation not-otherwise-specified.
Discussion
Our intervention component analysis generated a taxonomy of 40 components organized within 13 categories describing not only program activities for students but also other target audiences (parents, teachers, and the larger community) as well as structurally targeted program efforts. See Table 2 for a summary of the critical findings we identified through our analyses, which confirm prior findings (e.g., Gaffney et al., 2021; Kettrey et al., 2019) and also suggest new ways in which DRV/GBV school-based prevention programs could be re-examined, improved or created in the future. See Table 3 for a summary of the major implications for policy, practice, and research based on our findings.
Summary of Critical Findings.
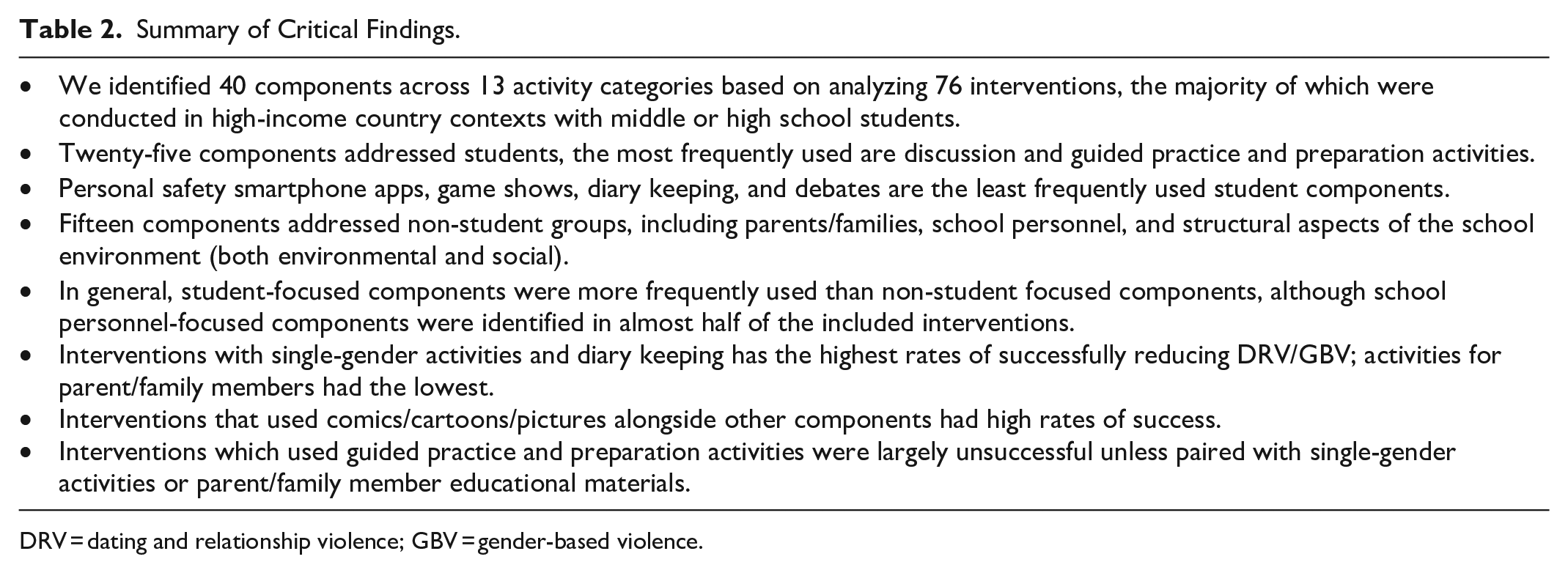
DRV = dating and relationship violence; GBV = gender-based violence.
Implications for Policy, Practice, and Research.
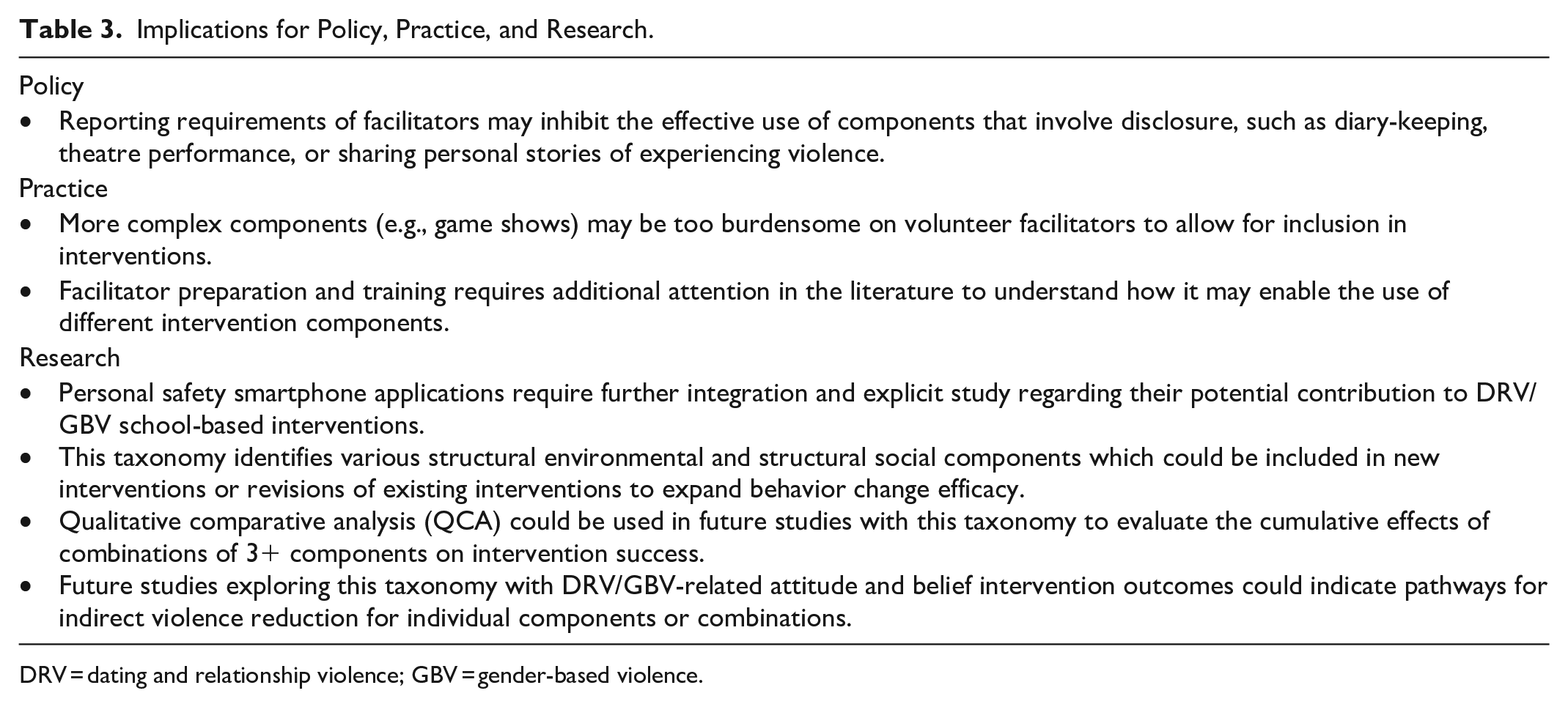
DRV = dating and relationship violence; GBV = gender-based violence.
Most and Least Used Components
Given that the focus of this analysis was on school-based programs, it is perhaps unsurprising that group discussions and the use of individual reading materials for students were the components most frequently identified. Discussions are an interactive activity where students are required to think and apply knowledge as well as have the opportunity to ask questions about topics about which they are unsure. Most discussion formats allow for students to hear the ideas, reasons, and explanations of their peers. These two activities, discussions and reading material, are ubiquitous across most types of school curricula. They are also activities that can be deployed with minimal preparation and cost. The format complexity of a given activity may well be a driving force behind whether an intervention incorporates that type of activity. This idea gains more traction if we look at the least frequently used components with students, which were game shows, diary-keeping and debates. Game shows and debates have complex formats to design, requiring interconnected structures and some type of guidance, whether programmed ahead of time or “in the moment” from a facilitator. They may also require continuous oversight and skill to facilitate, which puts a heavy burden on program facilitators in terms of successfully guiding those activities. These more complex and structured activities may also be difficult to do meaningfully with large groups of students. Although game shows and debates can be done in teams, much time is still focused on individual competition rather than the entire team participating in every moment. DRV/GBV program creators may deliberately not use these components if they want to maximize intervention impact on all students in a short time period.
Nuances of Disclosure, Storytelling, and Prior Skills
Diary-based activities, while on the surface may appear to be less complex, invite other nuances that may make DRV/GBV program creators lean away from them. For example, if teachers or other adults are regularly reviewing these diary entries (if only to ensure that the activity is being completed), disclosures of experiences perpetrating or experiencing DRV/GBV may legally need to be reported to an authority. This could situate facilitators in a potentially difficult position where they may need to violate a student’s privacy or face legal repercussions themselves (for failing to report violence). Even without reporting requirement issues, students may feel their privacy is being violated if facilitators reviewed entries for any reason, which would undermine how genuinely students engaged with the diary-keeping activity. The very act of disclosing victimization in an activity could also carry with it negative consequences. Survivors of DRV/GBV often say they do not tell anyone about their experience of violence due to fear of not being believed, stigma toward victims, and general taboos around talking about sex-related things in public (Adeosun, 2015; Zinzow et al., 2021). In order for these types of activities to be done in a trauma-informed manner, programs would likely need counselors or other staff that could respond to support students if a public disclosure did not go well. Although it is likely many programs did provide information to students about support resource or how to speak with a counselor if they wanted to privately disclose violence, we did not assess this element directly. While we did note a dozen programs included service-in-reach components from local crisis and support centers, there are many passive ways this information could be provided (emails, pamphlets, calling cards, etc.). Future examination of how best to inform students about survivor support resources could help programs decide which methods to use.
Individualized activities, such as diary-keeping but also including video games or workbooks, rely on students’ capabilities and underlying skills to be successful. This dependence on prior skills may be why these activities tended to be in fewer successful interventions and had inconsistently high and low rates of success when paired with other activities. If students have not developed or been taught critical thinking and reflection skills necessary for an activity, reading a story or keeping a diary may be stressful rather than helpful (Merisuo-Storm, 2006). Even with the use of guiding prompts or suggestions to begin diary entries, students with lower emotional awareness, weaker writing skills, or who feel more discomfort thinking about DRV/GBV topics likely benefit less from diary-keeping activities. This high individual variability in engaging in the activity could also create confounding factors that are difficult to control for in program evaluation efforts that seek to examine the impact of prior-skill-dependent activities like diary-keeping, completing workbooks, or performing in theatrical plays.
Promising Cartoons, Comic Books, and Safety Apps
Our general findings on intervention success offer few simple conclusions. There is no single component which seems to determine if an intervention will succeed or fail. Several different individual and pairs of components showed promise in consistently being present in successful interventions versus unsuccessful interventions. The use of comics, cartoons, and pictures in particular, appears to be promising both individually and in combination with other activities. These types of visual materials may provide a way for adolescents to engage with an intense topic like DRV/GBV but at a safe “distance” (Brecht, 1964). For example, a comic book character can experience DRV in vivid detail with realistic emotions so that adolescents understand what violence really looks like; and yet when reading that story students must still turn the page, look at the next panel, and in general be reminded that it is a story about a fictional character. This deliberate distancing can allow audiences to feel empathy for a fictional character. Disrupting the narrative brings the story details from the subconscious mind to the conscious mind; so the audience is forced to consider what just happened instead of merely watching it happen (Wijers, 2018). The mechanisms through which fictional characters can evoke strong emotions is explored in the performing arts (e.g., Eriksson, 2011) and video game (e.g., Dunne, 2014) literatures, but has not yet been studied in a violence prevention context. This approach could help adolescents learn about scary topics, like violence, in ways that are less personal compared to typical activities, such as hearing a classmate share their story of victimization.
The student component utilized least was personal safety apps. Only one program utilized a smartphone app or described a deliberate integration of anti-violence resources with mobile devices. This low representation is very likely due to the technologies that underlie smartphone usage generally. Widespread and affordable access to smartphones and improvements in wireless internet technologies that enable the use of smartphone apps only converged in the last 16 years, and only became widely used by a majority of adolescents (in higher-income countries) in the last decade (Lenhart, 2015). Recent national surveys suggest almost 95% of teenagers in the United States have a smartphone or have access to one, with nearly half of those teens reporting they are online on a near-constant basis (Anderson & Jiang, 2018). The only smartphone app used by a DRV/GBV intervention we found in our review focuses on personal safety and planning. However, as smartphone device access continues to grow and software development methods improve, it is likely that more DRV/GBV programs will explore the use of smartphone apps. Beyond safety and planning, apps could be used to deliver educational content and engage students in online activities, stories, and games that have relevant bystander, safety, or relationship messages embedded within them. The versatility of smartphone apps provides a wide range of possibilities for intervention developers to consider. For example, eHealth interventions to address sexual health, mental health, and substance use have shown some success (Meiksin et al., 2021). Translating effective strategies from those individual health domains for application into the domain of interpersonal and community health (i.e., interpersonal violence) will be a key endeavor for researchers in the coming years.
Expanding Non-Student Components
Similar to Gaffney et al. (2021) coding schema for anti-bullying programs, we identified over a dozen components focused on aspects of social-ecological impact beyond the individual student as a change mechanism. Although the associated intervention success rates for these non-student components were similar to student components, we believe they are critical to a comprehensive understanding of DRV/GBV as not just individual acts of violence but as expressions of deeply ingrained and chronic community inequities and problems. The normalization of violence, approval of perpetrators, and apathy toward victims are all community-level attitudes and beliefs that adolescents absorb (Leone et al., 2020; MacLean, 2017; Plourde et al., 2020). Efforts to address violence that meaningfully address higher levels of the social-ecological model can often become highly tailored to a specific local circumstance and resist broader comparison. This taxonomy provides a way to consider structural-social and structural-environmental components, which can serve as a useful guide in comparing different interventions’ efficacy. We noted several promising combinations of activities for students that were highly successful in interventions that also included school personnel activities, materials for parents/family members, and structural efforts of various types. Existing interventions which do not utilize these higher-level approaches can use this taxonomy to consider which components might best pair with the student-focused activities they already employ.
Unfortunately, the level of detail provided by included studies about their non-student program components was not sufficient to create a taxonomy with the same level of detail as that for student-facing components. Components relating to parents, guardians, and family members specifically need additional exploration, a point raised by prior reviewers as well (e.g., Huang et al., 2019). Although in our findings we noted that interventions with activities for parents/ guardians/family members had the lowest success rate, we believe these components still merit further inclusion and evaluation. Measures of parent/family participation may be an important first step to more effective parent activities. Parent components frequently occur outside the school itself and thus may be difficult to verify as having happened, let alone more in-depth considerations such as how engaged parents were during their workshop. Alternately, if material is sent home for parents/family to read, it is not always clear whether the parents/family of those students have read the material. We can be certain that students had the opportunity to share materials with their parents and family, but no interventions include indicators of whether parents received material, read to the end, understood the material, had questions about the material, etc. Thus, evaluations of these kinds of family-based components are being influenced by an array of confounding variables which may have nothing to do with whether the materials were effective. Interventions should look for ways to better track fidelity across the different audiences and contexts of program activities, so that measured outcomes can be clearly linked to intervention components.
Limitations and Future Directions
Although our systematic review was exhaustive and comprehensive with regard to DRV/GBV school-based prevention interventions, the intervention component analysis was only carried out on studies which used an RCT design. Many additional DRV/GBV school-based prevention interventions have been developed/delivered and many of those have been evaluated and reported upon in the scientific literature. Our goal in focusing on RCT designs was to provide a taxonomy with evaluation in mind, so that future intervention impact analyses and meta-analyses can more easily and more consistently be conducted across interventions. Additionally, limiting our scope to studies with randomization and control groups reduces the possibility that the intervention success we coded was due to confounds or unexpected influences.
We cannot rule out the influence of publication bias, although our multiple and comprehensive search strategies did locate more RCTs than prior reviews and several that were not published. We also recognize that there may be very specialized program components that are newly developed or so rarely used that our search did not collect them, and they may therefore not be part of our taxonomy. While we did examine pairs of components, we did not examine groups of three or more components in relation to their relative likelihood of being included in a successful or unsuccessful intervention. We believe that our taxonomy can serve as a template for future research teams to conduct qualitative comparative analyses (QCA) which may be able to identify more complex patterns of three or more components utilized in successful DRV/GBV interventions.
Our evaluation of intervention success at reducing DRV/GBV victimization and perpetration should also be interpreted with caution. There are many reasons beyond what we coded which could impact the success of an intervention, including program fidelity or local cultures which hamper program goals. Additionally it is possible that certain components are more likely to have an effect on DRV/GBV-related attitudes and beliefs which may then over time decrease violence in the community. We hope that future reviewers can use the taxonomy we have identified to explore complex and indirect pathways along these components to intervention success.
Additionally, our stated goal was to focus on only DRV/GBV prevention interventions, which may limit the generalizability of these findings when considering preventative school-based interventions for other types of violence (e.g., race-related violence, disability stigma and violence, identity-based violence). As we note, we did find similar categories to other prior reviews (e.g., Gaffney et al., 2021) but also unique aspects in this literature. Other prevention programs among adolescents might have similar program components or they may have different salient elements that need to be addressed/captured. For example, programs designed to reduce racial microaggressions or prejudice may keep track of the race of facilitators, the racial dynamics and groups in the student body, and the demographic makeup of visuals and images in the program. While these factors are also potentially relevant for DRV and GBV programs, study program descriptions did not contain a level of detail that enabled us to consider this as a salient component for DRV/GBV interventions. The closest approximations could be considered the component of local customization of content to reflect and incorporate local values, attitudes, and realities. Future studies that consider intervention components of other types of violence should focus intentionally on how unique dynamics and common dynamics of different types of violence are reflected in program activities.
We only examined school-based or primarily school-based interventions in this review and excluded community-based and family-based interventions. This likely contributed to the lower degree of detail in program descriptions when describing components that went beyond students to teachers, parents, families, and the community. Future research and expansion of this taxonomy could look to include interventions regardless of primary location or avenue of delivery. This could illuminate potential synergies between family-based program and school-based programs: for example, activities in one setting could be paired with guided homework or parent-based work in the other setting. The embedded nature of DRV/GBV as behaviors supported by cultural norms means that approaches which address all aspects of normative messages are more likely to be successful at reaching adolescents and creating lasting change.
We did not consider prevention programs conducted with older adolescents; specifically, we excluded programs delivered on college or university campuses. The differences between middle/high school students and college student are stark in many domains. Current knowledge on pedagogical approaches best suited for different age groups is also clear in the ways that high school versus college students receive and process information. While our taxonomy of intervention components can serve as an initial guide to evaluating the different components of college-campus focused DRV/GBV prevention programs, more and specific work exploring relevant programs’ components is needed. For example, college students are likely to have more sophisticated reading, writing, and comprehension skills compared to middle school students. However, the use of individualized work in the college setting may encounter other problems as the living situation and social situation of college students can vary considerably across individuals and between institutions. The very structure of a “school day” likewise changes from highly regimented and continuous in high school to a more fluid schedule where a student may have several hours between classes and has to use, engage, and interact with the college campus space and schedule entirely differently than when they were in high school (Conley, 2010; Venezia & Jaeger, 2013). Alternatively, some aspects may translate well across age groups. For example, the importance of positive student—teacher relationships has been shown to be generally related to beneficial outcomes for both high school and college students (Li, 2022; Wang et al., 2013). This suggests that examining the role of school personnel in programming is an important category to consider and further develop in studies of college campus-based interventions.
Conclusion
Although previous systematic reviews have been conducted on DRV and GBV components, the present study is the first to consider DRV/GBV jointly with the goal of creating a taxonomy of intervention components reflecting the types of activities and target audiences of DRV/GBV school-based prevention interventions. In addition to a variety of student-focused categories of intervention and related activities, we identified components that address higher levels of the social-ecological model as mechanisms to change adolescent DRV/GBV, including teacher components, parent/family components and structural-social/environmental components. This taxonomy provides guidance for both future meta-synthesis evaluations and for future DRV/GBV program creators. As efforts to address violence among adolescents continue to evolve and expand, the common language provided in this study helps to organize what we already know so that we can continue to deliver what is effective and improve what is not.
Supplemental Material
sj-docx-1-tva-10.1177_15248380221134294 – Supplemental material for Exploring the Activities and Target Audiences of School-Based Violence Prevention Programs: Systematic Review and Intervention Component Analysis
Supplemental material, sj-docx-1-tva-10.1177_15248380221134294 for Exploring the Activities and Target Audiences of School-Based Violence Prevention Programs: Systematic Review and Intervention Component Analysis by Andrew J. Rizzo, Noreen Orr, Naomi Shaw, Caroline Farmer, Annah Chollet, Honor Young, Vashti Berry, Emma Rigby, Ann Hagell, Chris Bonell and G. J. Melendez-Torres in Trauma, Violence, & Abuse
Supplemental Material
sj-docx-2-tva-10.1177_15248380221134294 – Supplemental material for Exploring the Activities and Target Audiences of School-Based Violence Prevention Programs: Systematic Review and Intervention Component Analysis
Supplemental material, sj-docx-2-tva-10.1177_15248380221134294 for Exploring the Activities and Target Audiences of School-Based Violence Prevention Programs: Systematic Review and Intervention Component Analysis by Andrew J. Rizzo, Noreen Orr, Naomi Shaw, Caroline Farmer, Annah Chollet, Honor Young, Vashti Berry, Emma Rigby, Ann Hagell, Chris Bonell and G. J. Melendez-Torres in Trauma, Violence, & Abuse
Supplemental Material
sj-xlsx-3-tva-10.1177_15248380221134294 – Supplemental material for Exploring the Activities and Target Audiences of School-Based Violence Prevention Programs: Systematic Review and Intervention Component Analysis
Supplemental material, sj-xlsx-3-tva-10.1177_15248380221134294 for Exploring the Activities and Target Audiences of School-Based Violence Prevention Programs: Systematic Review and Intervention Component Analysis by Andrew J. Rizzo, Noreen Orr, Naomi Shaw, Caroline Farmer, Annah Chollet, Honor Young, Vashti Berry, Emma Rigby, Ann Hagell, Chris Bonell and G. J. Melendez-Torres in Trauma, Violence, & Abuse
Supplemental Material
sj-xlsx-4-tva-10.1177_15248380221134294 – Supplemental material for Exploring the Activities and Target Audiences of School-Based Violence Prevention Programs: Systematic Review and Intervention Component Analysis
Supplemental material, sj-xlsx-4-tva-10.1177_15248380221134294 for Exploring the Activities and Target Audiences of School-Based Violence Prevention Programs: Systematic Review and Intervention Component Analysis by Andrew J. Rizzo, Noreen Orr, Naomi Shaw, Caroline Farmer, Annah Chollet, Honor Young, Vashti Berry, Emma Rigby, Ann Hagell, Chris Bonell and G. J. Melendez-Torres in Trauma, Violence, & Abuse
Footnotes
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Chris Bonell was principal investigator, and Honor Young and G.J. Melendez-Torres co-investigators, of one of the trials included in this systematic review.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is funded by the NIHR Public Health Research Programme (NIHR130144). In addition, Vashti Berry and G.J. Melendez-Torres are part-supported by the NIHR Applied Research Collaboration South West Peninsula (NIHR PenARC). The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care. The funders had no role in the design and conduct of the study.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References

Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.