
Abstract
Intimate partner violence (IPV) is a public health problem that has devastating physical, psychological, and economic consequences. The emergency department (ED) is an important point of contact for individuals experiencing IPV. However, there are few studies synthesizing interactions between patients experiencing IPV and providers. We aimed to summarize the existing evidence regarding (1) ED care experiences of patients with a history of IPV and (2) experiences of ED providers interacting with them. The secondary aim of this review was to evaluate high-quality care barriers and facilitators and to elucidate common causes of care avoidance. A literature search of peer-reviewed electronic databases was undertaken. Inclusion criteria consisted of studies detailing IPV-related patient or provider experiences surrounding ED visits. Articles published before 2000 or unavailable in English/French were excluded. A total of 772 studies were screened, yielding a final number of 41 studies. Negative patient experiences arose from individual-, institutional-, and system-level issues, commonly including adverse provider behavior. Negative provider experiences stemmed from individual-, institutional-, and system-level issues, such as a lack of knowledge and lack of infrastructure. Facilitators to positive patient experiences included interacting with empathetic providers, having privacy, and receiving timely specialized care. Facilitators to positive provider experiences included feeling well-equipped to manage IPV and having policies leading to appropriate care. Negative ED care experiences reveal inadequate care quality, ultimately leading to secondary victimization of individuals experiencing IPV. This review also uncovered important literature gaps regarding experiences of those who identify as equity-deserving.
Keywords
Introduction
One in three women and one in four men have experienced intimate partner violence (IPV) in their lifetime (Black et al., 2011) and, in the United States, one out of five homicide victims were killed by an intimate partner (Smith & Cooper, 2011). IPV is defined as any behavior that causes physical, psychological, or sexual harm to those within an intimate relationship and continues to be an ongoing human’s rights issue (World Health Organization, 2012). Fifty percent of women seen in emergency departments (EDs) report a history of IPV, and approximately 44% of those killed by their abuser were seen in the ED in the 2 years before their murder (Huecker et al., 2021). The ED thus represents a unique clinical environment to reduce IPV-related morbidity and mortality.
Emergency providers commonly experience frustration, limited time, and powerlessness when caring for individuals who have experienced IPV (Williston & Lafreniere, 2013). Furthermore, many patients describe ED providers as rushed and lacking compassion. This often results in negative care experiences (Yam, 2000).
Patient care experiences relate to the contact patients have with the healthcare system such as effective communication with clinicians or interactions with professional providers (Agency for Healthcare Research and Quality, 2020; Agency for Healthcare Research and Quality, 2022). Provider care experiences relate to clinician engagement in their day-to-day work, for example workflow efficiency or experiences regarding effective scheduling (Healthbox, 2019).
Patient care avoidance is described as turning away from threat-related cues, which results in not being able or willing to be involved in necessary care (Klop et al., 2018), negatively influencing an individuals’ well-being (Ye et al., 2012). Negative patient care experiences have been linked to patient care avoidance and generate negative patient outcomes (Schwei et al., 2017). Conversely, positive patient care experiences create better clinical outcomes, improved patient adherence to medical advice, better disease prevention, improved patient safety practices, and lower utilization of unnecessary healthcare services (Agency for Healthcare Research and Quality, 2022; Kelley et al., 2014).
There are few systematic reviews (SRs) delineating negative experiences from both patient and provider perspectives related to IPV care within the ED. We, therefore, conducted an SR with a primary aim of summarizing the existing evidence regarding (1) ED care experiences of patients with a history of IPV and (2) experiences of ED providers interacting with them. The secondary aim was to evaluate contributors to positive and negative care experiences, as well as uncover reasons behind patient care avoidance.
Contributors to positive and negative care were organized into three levels: individual (related to the person such as interpersonal interactions or individual practices), institutional (related to the ED such as departmental practices, norms, and infrastructure) and systemic (related to the system, including inter-institutional, historical, economic and cultural policies or norms) issues.
Methods
We conducted a systematic literature review of health services responses to IPV, following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Moher et al., 2009). We assessed patient and provider perspectives of emergency care surrounding IPV to uncover common themes relating to both positive and negative experiences. To evaluate common contributors to positive and negative care experiences, we aimed to be as inclusive as possible in our search strategy regarding social identities, demographic factors, provider types, and diversity of experiences.
Search Strategy
During September 2021, we searched Embase, PsychInfo, Medline, CINAHL, and Cochrane for peer-reviewed primary studies published between January 2000 and March 2021. Furthermore, snowballing of landmark studies and grey literature searches including conference proceeding searches were completed sequentially through Google Scholar, ProQuest Dissertations, and Theses Global. We conducted exhaustive searches across these databases using a variety of MeSH terms and keywords including but not limited to: Intimate Partner Violence, attitudes, experiences, and Emergency Department, details of which are found in Appendices A and B.
Inclusion and Exclusion Criteria
Inclusion criteria comprised any study detailing first-person perspectives, experiences, attitudes, or stories on interactions between individuals identifying as having experienced IPV (current or past) and any professional involved in medical care or paramedical care during or surrounding ED visits for any reason. These providers could include physicians, emergency medical services, nurses, nurse practitioners, social workers, physiotherapists, occupational therapists, emergency medical technicians (EMTs), police workers, or administrative workers. All study designs and all participant demographics were included, without restriction by age, gender, sexual orientation, race, language, or disability status. Studies without available full texts or not in English/French were excluded. We limited inclusion to the year 2000 and later in an attempt to reflect the current socio-cultural context of ED care.
Assessment of Methodological Quality
Two independent reviewers (ED and AN) completed title/abstract screening and, subsequently, full-text screenings for eligibility using Covidence (Veritas Health Innovation, 2021). Disagreements between reviewers were resolved through team adjudication after independent review. Inter-rater agreement of study inclusion was confirmed following screening.
Quality assessment of included studies was conducted using the Critical Appraisal Skills Program (Critical Appraisal Skills Program, 2021). One reviewer (ED) completed the critical appraisal on all studies with 30% reviewed in duplicate by a second independent reviewer (AN) for quality assurance. Discrepancies were resolved by consensus or by an independent third-party review. Each study’s risk of bias was evaluated as low, medium, or high by combining ethical considerations and critical appraisal findings, as well as specific limitations including lack of saturation, lack of independent recruiters or analysis, and presence of selection or misclassification bias. Studies meeting all 10 CASP criteria were considered highest quality. Due to the small number of studies meeting inclusion criteria, no study was excluded based on lower methodological quality or CASP scores.
Results
Study Inclusion
A total of 802 studies were imported into Covidence, including 196 duplicates. In title and abstract screening, 426 studies did not meet study inclusion/exclusion criteria. Full-text screening was completed on 180 studies and yielded 41 final studies meeting all inclusion criteria. Cohen’s Kappa measuring inter-rater reliability for title/abstract and full-text screening were 69% and 65%, respectively. Reasons for exclusion are provided in Figure 1 PRISMA diagram and individual details surrounding included studies are shown in Table 1.
PRISMA diagram.
Included Studies.
Note. I denotes in-person, virtual or telephone interview or focus-group-based data collection; Q denotes questionnaire or survey-based data collection; pts denotes patient participants; pvs denotes provider participants; Med denotes medium bias risk. ED = emergency department; EMTs = emergency medical technicians; IPV = intimate partner violence; RCT = randomized controlled trial.
Characteristics of Included Studies
Of the 41 included studies, 17 focused on patient experiences, 22 focused on provider experiences, and two included both patient and provider ED care experiences. There were 15 studies completed in North America, 10 in Central and Eastern Europe, nine in Australasia, three in East and South-East Asia, two in the Middle East, and one in Africa. While study designs varied, qualitative methodology was predominant, followed by mixed-methods studies. Personal and focus-group interviews were the most frequent data collection method (34/41, 83%) followed by cross-sectional surveys or questionnaires (7/41, 17%). Other study designs included one publication featuring a personal narrative, one featuring a literature review, and one secondary qualitative analysis of audiotapes between patients and providers from a randomized controlled trial evaluating a health risk assessment tool.
Patient Study Demographics and Characteristics
While inclusion and exclusion criteria varied, studies on patient experiences almost always recruited women, with only a single study (Du Mont et al., 2014) featuring perspectives from men and/or transgender individuals. Two studies (Koziol-McLain et al., 2008; Leppäkoski et al., 2011) excluded participants based on their inability to speak English or experiencing substance use or mental illness. In all, 13 studies featured data from participants experiencing ongoing IPV at the time of data collection, while six did not explicitly detail whether IPV was ongoing. Seven studies collected information on education and dependents, with most participants having at least secondary education and one or more children.
Commonly collected patient demographics were gender and age, while sexual orientation was not reported in any study. Only two studies (Du Mont et al., 2013, 2014) collected experiences from people identifying as having a disability. Three studies reported the mean ages of participants (30.7, 34 and 30 years) (Catallo et al., 2012; Koziol-McLain et al., 2008; Rhodes et al., 2007) and three reported the median ages of participants (28.5, 39 and 28 years) (Bacchus et al., 2003; Leppäkoski et al., 2011; Pratt-Eriksson et al., 2014). In all, 11 studies collected details on race or ethnicity. Of these, few featured experiences from participants identifying as Black, Indigenous and People of Color (BIPOC).
Provider Study Demographics and Characteristics
Studies mostly featured the perspectives of nurses (21/22, 95%) and physicians (11/22, 50%) caring for IPV-affected patients. Seven studies collected data solely from nurses (Efe & Taşkın, 2012; Fay-Hillier, 2016; Goldblatt, 2009; Inoue & Armitage, 2006; Robinson, 2010; Tower et al., 2012; van der Wath et al., 2013). Social workers were included in three studies (Colombini et al., 2013; D’Avolio, 2011; Dawson et al., 2019); EMTs in two studies (Broissoie & Roberto, 2015; Leppäkoski & Paavilainen, 2013); administrative professionals in three studies; spiritual care professionals in two studies (Broissoie & Roberto, 2015; McGarry, 2017); and justice system professionals in one study (Broissoie & Roberto, 2015).
Gender was not collected in approximately one-third of the studies. Among those that reported gender, male provider perspectives were often missing; 10 studies only successfully recruited female providers and two directly excluded male participants (Goldblatt, 2009; Inoue & Armitage, 2006). No studies featured trans or gender diverse providers. Only one study collected sexual orientation demographics, where 1/21 participants identified as gay (Fay-Hillier, 2016).
Provider race or ethnicity was explicitly collected in four studies (D’Avolio, 2011; Fay-Hillier, 2016; Rhodes et al., 2007; van der Wath et al., 2013). Seventy-five percent of these mainly featured participants identifying as European, Caucasian, or white. No provider study collected information regarding disability.
Methodological Quality of Included Studies
All 10 criteria of the CASP checklist were met in eight studies: one patient-centered study (Koziol-McLain et al., 2008), five provider-centered studies (Dawson et al., 2019; Fay-Hillier, 2016; O’Malley, 2011; Ritchie et al., 2009; Zijlstra et al., 2017), and both of the patient–provider studies (Dowd et al., 2002; Rhodes et al., 2007).
Validated or piloted data collection tools were used in 11 studies: four patient-centered studies (Du Mont et al., 2013, 2014; Loke et al., 2012; Olive, 2017), six provider-centered studies (Broissoie & Roberto, 2015; Colombini et al., 2013; Efe & Taşkın, 2012; Leppäkoski and Paavilainen, 2013; O’Malley, 2011), and one patient–provider study (Dowd et al., 2002).
In all, 14 studies reached saturation: five patient-centered studies (Bacchus et al., 2013; Catallo et al., 2012, 2013; Reisenhofer & Seibold, 2013; Yam, 2000) and nine provider-centered studies (D’Avolio, 2011; Dawson et al., 2019; Fay-Hillier, 2016; Goldblatt, 2009; Inoue & Armitage, 2006; Loughlin et al., 2000; Ritchie et al., 2009; van der Wath et al., 2013; Zijlstra et al., 2017).
In total, 14 studies used independent analysts: five patient-focused studies (Catallo et al., 2012, 2013; Koziol-McLain et al., 2008; Loke et al., 2012; Pratt-Eriksson et al., 2014), seven provider-focused studies (Broissoie & Roberto, 2015; Goldblatt, 2009; Loughlin et al., 2000; O’Malley, 2011; Ritchie et al., 2009; Sormanti & Smith, 2009; Zijlstra et al., 2017), and both patient–provider studies (Dowd et al., 2002; Rhodes et al., 2007).
Findings of the Review—Patient Perspectives
Contributors to positive and negative care experiences were identified at the individual, institutional, and systemic levels. Sample quotes and principal findings are provided in Table 2.
Critical Findings—Patient and Provider Care Experiences.
Note. pts denotes patients; pvs denotes providers. EDs = emergency departments; IPV = intimate partner violence; TIC = trauma-informed care.
Positive Experiences
In general, patients perceived opportunities for open discussions on IPV as positive (Koziol-McLain et al., 2008) and long overdue (Koziol-McLain et al., 2008). Two studies in this review described the psychological processes behind the decision to seek care and establishing readiness to discuss IPV or to leave a violent relationship. Using the Transtheoretical Model of Change, the first study (Catallo et al., 2012) found that individuals often disclose IPV after weighing the benefits against the risks of disclosing, the latter including examples such as fear for their safety, fear of child apprehension, and/or fear of judgment from healthcare providers. The second study (Catallo et al., 2013) described disclosure and care seeking as a four-phase process, with minimizing the risk of intrusion by healthcare professionals and evaluating the level of trust with these professionals at the center. Patients felt that disclosing violence to an ED provider could cause intrusion, defined as involvement of healthcare professionals resulting in further chaos and trauma. Risk of intrusion was weighed against the ability of the provider to offer services or interventions perceived as useful and positive. In a third study, healthcare interactions were found to have important effects on individual identity, helping victims acknowledge IPV and begin to re-construct their sense of self (O’Doherty et al., 2016).
On an individual level, patients commonly described interactions with non-judgmental, empathetic and caring providers as contributors to positive ED experiences (Catallo et al., 2012; Leppäkoski et al., 2011; Reisenhofer & Seibold, 2013; Olive, 2017). Patients appreciated having a provider validate their experience as consisting of IPV and pausing in their busy shift to acknowledge IPV as wrong or unjustified (Bacchus et al., 2003; Koziol-McLain et al., 2008; Reisenhofer & Seibold, 2013; Yam, 2000). Many patients perceived experiences positively when their providers cared for them holistically, seeing them as a whole person and not just as their injuries. This included having access to objective and thorough medical care (Leppäkoski et al., 2011) and comprehensive psychological and social support to meet their needs (Du Mont et al., 2013; Koziol-McLain et al., 2008; Mayer, 2000; Olive, 2017; Tower et al., 2006; Yam, 2000).
On institutional and systemic levels, many patients positively described experiences with providers who were knowledgeable on IPV (Du Mont et al., 2013; Leppäkoski et al., 2011). This included positive interactions with dedicated and kind law enforcement workers offering support before, during, and after ED care (Mayer, 2000; Olive, 2017). It was important for patients to have the ability to be seen quickly (Leppäkoski et al., 2011), and to have providers who took the time to listen to them (Olive, 2017). Patients also appreciated access to private spaces helping them feel safe (Leppäkoski et al., 2011). Readily available local resources (Du Mont et al., 2013; Leppäkoski et al., 2011), access to timely specialized IPV care around-the-clock (Leppäkoski et al., 2011), and an option for close follow-up with timely community referrals (Yam, 2000) all played significant roles in ensuring positive care experiences.
Negative Experiences
A concerning number of negative patient experiences were uncovered, commonly arising from perceived adverse provider behavior, as well as institutional and system-level issues encountered when navigating the health system.
On an individual level, negative provider behaviors commonly perceived by patients included providers minimizing violence (Leppäkoski et al., 2011; Rhodes et al., 2007; Yam, 2000), appearing unconcerned (Mayer, 2000; Reisenhofer & Seibold, 2013; Yam, 2000), displaying blame (Bateman & Whitehead, 2004; Leppäkoski et al., 2011; Mayer, 2000; Reisenhofer & Seibold, 2013; Yam, 2000), expressing pity (Du Mont et al., 2013; Mayer, 2000), or exhibiting judgment (Du Mont et al., 2013; Mayer, 2000; Pratt-Eriksson et al., 2014; Reisenhofer & Seibold, 2013; Rhodes et al., 2007; Roush, 2009; Tower et al., 2006; Yam, 2000). Patients also cited having negative experiences when providers appeared cold (Mayer, 2000; Pratt-Eriksson et al., 2014; Reisenhofer & Seibold, 2013) or lacked compassion (Pratt-Eriksson et al., 2014; Yam, 2000).
Patients also commented on providers seeming uncomfortable or lacking knowledge, education, and experience with the subject of IPV (Bateman & Whitehead, 2004; Mayer, 2000; Pratt-Eriksson et al., 2014; Rhodes et al., 2007; Yam, 2000), with many providers only focusing on physical injuries (Leppäkoski et al., 2011; Loke et al., 2012; Reisenhofer & Seibold, 2013; Yam, 2000). Patients found it particularly harmful when providers ignored violence or failed to address it as the reason for their ED visit (O’Doherty et al., 2016; Leppäkoski et al., 2011; Mayer, 2000; Yam, 2000). While these provider behaviors were mostly recorded from nurses and physicians, one study also outlined EMS as exhibiting similar behavior (Bateman & Whitehead, 2004). Patients also described providers displaying controlling or “pushy” behavior (O’Doherty et al., 2016; Olive, 2017; Pratt-Eriksson et al., 2014; Yam, 2000), with some providers becoming frustrated or uncaring when patients declined police involvement (Mayer, 2000l; Tower et al., 2006; Yam, 2000).
On the institutional level, lack of privacy was a predominant problem, including instances such as sitting in a busy waiting room and perceiving stares from others seeing their injuries, or having to recount violence knowing others could overhear the conversation (Bacchus et al., 2003; Du Mont et al., 2013, 2014; Leppäkoski et al., 2011; Olive, 2017; Yam, 2000). This was also reflected in providers often failing to separate abusive partners from patients during medical examinations (Bacchus et al., 2003; Mayer, 2000; Rhodes et al., 2007; Yam, 2000). Long wait times commonly led to negative experiences (Du Mont et al., 2013, 2014; Leppäkoski et al., 2011; Mayer, 2000), as did interacting with providers who appeared rushed (Du Mont et al., 2014; Mayer, 2000; Yam, 2000). Patients described feeling burdensome and being treated as less important than other patients (Reisenhofer & Seibold, 2013; Tower et al., 2006; Yam, 2000).
On the systemic level, patients reported a lack of effective inter-agency communication and the absence of referral systems for follow-up (D’Avolio, 2011; Du Mont et al., 2014; Leppäkoski et al., 2011; Olive, 2017). Interacting with professionals or services that could not meet their needs further contributed to negative experiences, often leading to feelings of hopelessness (Leppäkoski et al., 2011; Loke et al., 2012; Mayer, 2000; Olive, 2017; Pratt-Eriksson et al., 2014). Negative experiences discouraged individuals from seeking future care (Loke et al., 2012; Tower et al., 2006), with some even resolving to never return to a hospital again (O’Doherty et al., 2016).
Finally, patients described feeling failed by the system (Loke et al., 2012; Mayer, 2000; Olive, 2017) within both the healthcare and justice systems (Catallo et al., 2012; Leppäkoski et al., 2011; Loke et al., 2012; Pratt-Eriksson et al., 2014; Mayer, 2000). For example, some patients felt that both police and ED providers belittled their feelings (Leppäkoski et al., 2011; Loke et al., 2012; Mayer, 2000; Pratt-Eriksson et al., 2014; Reisenhofer & Seibold, 2013), normalized violence (Loke et al., 2012; Rhodes et al., 2007), or vindicated the abuser (Reisenhofer & Seibold, 2013). Patients also experienced stereotyping during ED care, for instance commonly feeling labeled as mentally ill or unintelligent by providers (Mayer, 2000; O’Doherty et al., 2016; Reisenhofer & Seibold, 2013; Yam, 2000). These adverse interactions were compounded, leading to a sense of futility (Leppäkoski et al., 2011; Loke et al., 2012; Mayer, 2000), as well as fear of police involvement within ED care (Catallo et al., 2012, 2013; Mayer, 2000).
Findings of the Review: Provider Perspectives
We identified contributors to both positive and negative care experiences at the individual, institutional, and systemic levels. Sample quotes and principal findings are shown in Table 2.
Positive Experiences
On the individual level, nurses and physicians noted positive experiences when able to support patients’ autonomy and offer useful services to patients (Fay-Hillier, 2016; Loughlin et al., 2000; Ritchie et al., 2009; Tower et al., 2012). Providers felt that making a difference even for one person (Loughlin et al., 2000; Ritchie et al., 2009; Tower et al., 2012) and helping to make people feel safe were important to them (Tower et al., 2012). Additional contributors to positive experiences included feeling knowledgeable and well-equipped to manage IPV in the ED (Loughlin et al., 2000; McGarry & Nairn, 2015).
On the institutional level, this was often achieved through education and practice increasing providers’ comfort in asking about and managing IPV (Loughlin et al., 2000; Maina, 2009; McGarry, 2017; Ritchie et al., 2009). Nurses and physicians also described policies and protocols as crucial contributors to positive experiences helping them provide effective and high-quality care (Loughlin et al., 2000; Ritchie et al., 2009). Providers described having adequate time and easy assessment tools (O’Malley, 2011), as well as cooperation (Broissoie & Roberto, 2015; Dawson et al., 2019; Fay-Hillier, 2016; O’Malley, 2011) as key contributors, including ED clinicians placing value on social workers within the interdisciplinary team (Dawson et al., 2019). Positive experiences also transpired when medical personnel, clerical staff, and security personnel successfully collaborated to keep patients safe (Dawson et al., 2019; Tower et al., 2012). Providers also cited having access to on-site, around-the-clock specialized IPV care as contributing to positive experiences (Dawson et al., 2019; Maina, 2009; McGarry & Nairn, 2015; O’Malley, 2011) as did the ability to arrange referrals to community resources (O’Malley, 2011).
Negative Experiences
On the individual level, providers described asking patients about IPV as opening “pandora’s box” (Dowd et al., 2002; Loughlin et al., 2000; Sormanti & Smith, 2009), “a can of worms” (Sormanti & Smith, 2009), and “a cesspool unable to be solved in the ED” (Zijlstra et al., 2017). Some physicians and nurses believed that IPV was a private, family affair (Efe & Taşkın 2012; Inoue & Armitage, 2006; Sormanti & Smith, 2009; Tower et al., 2012) and viewed it as a social problem rather than a health concern (Robinson, 2010). These providers sometimes held the opined that managing IPV was not their job (Colombini et al., 2013; Dawson et al., 2019; Efe & Taşkın, 2012; Inoue & Armitage, 2006; Sormanti & Smith, 2009; Tower et al., 2012). These attitudes were described by many physicians and nurses as a deterrent to discussing IPV, with many delegating this task to social workers (Dawson et al., 2019; Inoue & Armitage 2006; Maina, 2009).
Nurses, physicians, and social workers noted feelings of frustration and powerlessness when patients declined police involvement (Fay-Hillier, 2016; Robinson, 2010; Zijlstra et al. 2017) or returned to a violent situation (Colombini et al, 2013; Dawson et al., 2019; Fay-Hillier, 2016; Inoue & Armitage, 2006; O’Malley, 2011; Robinson, 2010; Sormanti & Smith, 2009).
Difficulty reconciliating personal experiences with IPV was another individual factor leading to negative provider experiences (Dawson et al., 2019; Leppäkoski & Paavilainen, 2013). Four provider studies collected information on personal history of IPV (Dawson et al., 2019; Fay-Hillier, 2016; Leppäkoski & Paavilainen, 2013; O’Malley, 2011). These found that at least one-fifth of nurses, practical nurses and EMTs had experienced IPV themselves (Leppäkoski & Paavilainen, 2013) and that 21% of male and 27% of female nurses and physicians had personally experienced family violence. Furthermore, over 60% knew someone who had experienced family violence (O’Malley, 2011).
On the institutional level, there was a lack of training and education on IPV which was mentioned in many studies examining experiences of nurses, practical nurses, EMTs, residents, and staff physicians (Dowd et al., 2002; Fay-Hillier, 2016; Inoue & Armitage, 2006; Leppäkoski & Paavilainen, 2013; Loughlin et al., 2000; Maina, 2009; Ritchie et al., 2009; Sormanti & Smith, 2009; Zijlstra et al., 2017). This was reflected in negative physician and nursing provider experiences stemming from lack of knowledge and comfort surrounding IPV (Colombini et al, 2013; Dawson et al., 2019; Dowd et al., 2002; Loughlin et al., 2000; Maina, 2009; McGarry, 2017; Rhodes et al., 2007; Robinson, 2010; Roush, 2009; Sormanti & Smith, 2009; Zijlstra et al., 2017).
Additionally, a lack of guidelines, policies, and infrastructural support often led to negative experiences for nurses and physicians (D’Avolio, 2011; Dowd et al., 2002; Loughlin et al., 2000; Maina, 2009; Zijlstra et al., 2017), as did insufficient standardized protocols for EMT providers. (Broissoie & Roberto, 2015) Physicians, nurses, social workers, and clinical officers cited lack of awareness of existing resources and protocols as negative contributors (Dawson et al., 2019; Loughlin et al., 2000; Maina, 2009). While inter-agency collaboration was usually described as positive, one detective mentioned that the competing missions of law, health, and advocacy professionals could create tension (Broissoie & Roberto, 2015).
Lack of on-site, around-the-clock IPV-care specialists (D’Avolio, 2011; Loughlin et al., 2000; Maina, 2009; Sormanti & Smith, 2009) was particularly frustrating for ED providers, as was the absence of reliable follow-up through effective and timely referral systems (Dowd et al., 2002; Loughlin et al., 2000; Maina, 2009). In this context, physician and nurses frequently invested many hours to find appropriate services for their patients (McGarry & Nairn, 2015; Robinson, 2010; Zijlstra et al., 2017), sometimes remarking that no good local resources existed (D’Avolio, 2011; Dawson et al., 2019; Efe & Taşkın, 2012; Fay-Hillier, 2016; Loughlin et al., 2000; Sormanti & Smith, 2009). Some nurses, doctors, and clinical officers also described dissatisfaction when seeking assistance from police and legal professionals, only for their patients to not be taken seriously or to be declined legal counsel (Maina & Majeke, 2008). These issues compounded intense feelings of frustration and powerlessness in care delivery (Efe & Taşkın, 2012; Fay-Hillier, 2016; Maina, 2009; Robinson, 2010; Sormanti & Smith, 2009; Zijlstra et al., 2017).
On the systemic level, providers described working in chronically under-resourced environments, with significant time constraints as a major barrier to positive experiences (Colombini et al., 2013; D’Avolio, 2011; Dawson et al., 2019; Dowd et al., 2002; Efe & Taşkın, 2012; Fay-Hillier, 2016; Loughlin et al., 2000; McGarry & Nairn, 2015; Ritchie et al., 2009; Robinson, 2010; Sormanti & Smith, 2009; Zijlstra et al., 2017). While this was mostly felt by nurses and physicians, administrative personnel also reported similar experiences (D’Avolio, 2011; Zijlstra et al., 2017). Nurses and physicians also noted they were forced to prioritize unstable patients, challenging their ability to holistically manage IPV (Fay-Hillier, 2016; Ritchie et al., 2009). Limited ED infrastructure with a lack of private spaces also contributed to negative experiences (Efe & Taşkın, 2012; Loughlin et al., 2000; Zijlstra et al., 2017).
Finally, providers held stereotypes and perpetuated bias related to IPV, such as thoughts that patients experiencing IPV were not reliable (Fay-Hillier, 2016; Maina, 2009; O’Doherty et al., 2016; Robinson, 2010; Sormanti & Smith, 2009; Tower et al., 2012; Zijlstra et al., 2017), were embellishing their stories or lying for their own benefit (Fay-Hillier, 2016; Loke et al., 2012; Pratt-Eriksson et al., 2014; Tower et al., 2012), were responsible for their experiences of violence (Inoue & Armitage, 2006; Robinson, 2010; Sormanti & Smith, 2009), were drug (Mayer, 2000) or attention-seeking (Fay-Hillier, 2016), were unkept or impoverished (Inoue & Armitage, 2006; Tower et al., 2012), were intoxicated (Fay-Hillier, 2016; Inoue & Armitage, 2006; Tower et al., 2012), and/or were mentally ill (Fay-Hillier, 2016).
Discussion
Patient Perspectives
Patients experiencing IPV reported highly variable ED care. These ranged from positive, when interacting with empathetic providers who effectively meet their needs, to negative, when interacting with judgmental providers who lacked education surrounding IPV and failed to provide necessary services.
Patients commonly described negative experiences such as feeling blamed, judged or rushed, having violence minimized, or lacking access to specialized care in the ED. Negative experiences discouraged individuals from seeking future care (Loke et al., 2012; Tower et al., 2006), likely contributing to secondary victimization and adverse health and legal outcomes (Ahrens, 2006; Campbell & Raja, 1999).
Trauma-informed care (TIC) is an approach to providing care that recognizes the widespread impact of trauma, promotes cultural safety, empowerment, and healing, and actively resists re-traumatization (ONSADVTC, 2019). Ultimately, this review demonstrated a lack of TIC contributing to decreased care-seeking behaviors. This may lead to increased morbidity and mortality, as highlighted by studies demonstrating a link between social isolation and IPV-related injury and death (Goodman & Epstein, 2008). This risk is punctuated in the context of the COVID-19 pandemic (Usher et al., 2020).
To address this, we recommend system-level change to foster TIC at the individual and institutional levels. This should include advocacy for appropriate infrastructural and financial resources within the ED, specifically focused on ensuring access to private spaces, IPV-care specialists and effective community-based programs. Of note, while universal IPV screening may provide important opportunities for intervention, it is our recommendation that appropriate resources be in place prior to universal screening implementation to avoid the harmful practice of seeing patients screen positively for IPV but not be offered appropriate support by ED providers following disclosure.
In this regard, to optimize clinical care and avoid frustration from both patients and providers, institutions require better referral systems and more highly trained teams available for around-the-clock evidence-based IPV care. While it remains an extremely complex and challenging issue, institutions also need to consider large-scale and small-scale changes to improve time constraints faced by providers. ED environments should also be adapted such that patients experiencing IPV can receive care within a space that is physically and emotionally safe.
Increased provider education is also required for TIC and we recommend providers receive training on a regular basis regarding TIC with specific applications for the ED context.
Recognizing that individual, institutional, and system issues are intertwined, initiatives such as ED-based policies and educational programs should be created in consultation with individuals holding expertise in IPV care and TIC and, whenever possible, individuals with a lived experience of IPV. These policies and programs should reflect an intersectional approach based on the unique issues providers and patients face in their specific context and should be guided by the concepts of Equity, Diversity, Inclusion, Indigeneity, and Accessibility. More details on this study’s implications for practice, policy, and research are shown in Table 3.
Implications of the Review for Practice, Policy, and Research.
EDs = emergency departments; IPV = intimate partner violence; TIC = trauma-informed care.
Patient Care Avoidance
As a secondary objective, this review aimed to evaluate common causes of health avoidance, including why some patients decline further resources after disclosing IPV. While some patients described leaving the ED early because of fear that their partner would find them or harm them (Catallo et al., 2012; Mayer, 2000) or because of long wait times (Du Mont et al., 2013), no included studies specifically addressed this question within their primary objective. Collectively, findings suggest that patients’ perceived ability to create a better life for themselves outside of their current abusive relationship may impact decisions around accepting further intervention. Patients who felt that the healthcare system was unable to help them were less likely to invest on engaging in open discussions with providers, focusing instead on protecting themselves from re-victimization (Catallo et al., 2012, 2013; Loke et al., 2012).
When patients visited the ED, they evaluated how much they could trust a provider to avoid intrusion, which was affected by past experiences with providers and whether the present ED provider displayed a non-judgmental and supportive approach. Interacting with a trustworthy provider supported IPV disclosure. Subsequent positive interactions helped patients re-establish their self-efficacy and identity, attributes that facilitate ending violent relationships (Hosey, 2012). Conversely, when interacting with judgmental providers, patients withdrew from care.
Provider Perspectives
The perspectives of ED providers interacting with patients who have experienced IPV were also variable. In general, positive experiences occurred when providers had appropriate knowledge and comfort levels surrounding IPV and worked within efficient systems that were well-suited to meet patients’ needs. Conversely, negative experiences occurred when providers operated within a system that did not have adequate TIC, or when they carried personal experiences of IPV or prejudice toward their patients. Providers also reported a lack of knowledge surrounding IPV, as well as frustration and time pressures limiting their ability to appropriately manage IPV in the ED.
This SR also revealed that between one-fifth and one-third of providers have personally experienced IPV (Leppäkoski & Paavilainen, 2013; O’Malley, 2011). Many providers described the difficulty of navigating the intersection between personal and professional identities in this context, particularly when strong emotions resurfaced and made it difficult to remain professional. Recognizing how commonly IPV is experienced among providers, it is important to offer more opportunities and better tools to help providers reflect on their own trauma when caring for patients experiencing IPV.
Provider Stereotyping and Discrimination
Providers commonly held stereotypical beliefs toward IPV-affected patients, which led to discrimination. For example, this resulted in providers doubting the veracity of patients’ experiences of violence (Fay-Hillier, 2016; Loke et al., 2012; Maina, 2009; O’Doherty et al., 2016; Pratt-Eriksson et al., 2014; Robinson 2010; Sormanti & Smith, 2009; Tower et al., 2012; Zijlstra et al. 2017). As a result, many providers mentioned fear of liability after documenting an incident as IPV, worrying that IPV may be falsely reported by patients (Fay-Hillier, 2016; Sormanti & Smith, 2009; Zijlstra et al., 2017). The idea that individuals lie about violence or sexual assault is a myth that has repeatedly been shown to be false (Lonsway et al., 2009; Rollero, 2020). While being stereotyped certainly contributed to negative patient experiences on the individual level, these were often repetitive instances throughout patients’ lives, reflecting a pervasive systemic problem within the healthcare system.
Similarly, providers often mistrusted patients’ ability to think for themselves, perceiving them as incapable because of mental illness (Fay-Hillier, 2016), substance use (Fay-Hillier, 2016; Inoue & Armitage, 2006; Reisenhofer & Seibold, 2013; Tower et al., 2012; Yam, 2000) or because of low socio-economic status (Fay-Hillier, 2016; Inoue & Armitage, 2006; Tower et al., 2012). This likely represents a common “othering” technique used by providers as a defense mechanism to reassure oneself that they are immune to experiencing IPV (Montoya & Agustín, 2013).
In addition, patients experiencing IPV, most commonly women, were sometimes explicitly labeled by providers as “crazy” (Reisenhofer & Seibold, 2013) or “stupid” (Mayer, 2000). This reflects the “crazy woman” trope which labels woman as irrational or incompetent (Mahdawi, 2016) and often leads to victim-blaming attitudes. The gender discrimination by providers highlighted in this SR has been emphasized in previous literature (Govender & Penn-Kekana, 2008).
Many providers believed that IPV-affected patients were responsible for their experiences of violence (Inoue & Armitage, 2006; Robinson, 2010; Sormanti & Smith, 2009), an attitude known to diminish empathy toward IPV-affected individuals which has been underscored in previous studies (Garcia, 2014). In this context, providers’ duty to offer empathetic, high-quality care conflicted with negative biases held toward patients. In turn, providers adopted a paternalistic approach, lacking TIC principles and decreasing patient autonomy.
To address this, we recommend provider education initiatives focusing on information to improve provider comfort-level, debunk common myths, clarify the challenges of ending a violent relationship, and provide data regarding legal outcomes in their region. In addition, helping providers understand the impact of patients’ many intersecting social identities affecting their experiences of violence and decreasing providers’ implicit biases regarding their patients are crucial factors in improving IPV care.
Provider Perspective Cycle
Many providers experienced moral distress when supporting patients experiencing IPV was impossible within their imperfect system. Moral distress is defined as a phenomenon in which institutional constraints make it nearly impossible to pursue the right course of action (Widianti et al., 2019). Emergency providers were frequently disheartened when faced with the reality of inadequate services and follow-up for IPV.
Providers described a variety of emotions, from relief when a severely injured patient showed signs of improvement, to crying when managing distressing cases (van der Wath et al., 2013). They cited seeing victims who were disfigured as being particularly traumatic (Goldblatt, 2009; van der Wath et al., 2013) and explained that this affected them when they went home to their families (Goldblatt 2009; van der Wath et al., 2013), sometimes causing intrusive memories (Maina, 2009; van der Wath et al., 2013). Vicarious trauma subsequently occurred when providers were exposed to other people's trauma repeatedly (Dawson et al., 2019), a phenomenon commonly described by ED providers (Greinacher et al., 2019).
The emotional labor and burn-out associated with caring for IPV victims was discussed in a recent Cochrane SR (Rivas et al., 2019), which examined the effectiveness of advocacy interventions for women experiencing IPV. Emotional labor refers to providers being expected to regulate and suppress their emotions. Consistent with our review, emotional labor allowed for maintenance of professionalism but lent itself to provider burn-out and patients feelings dismissed.
An American study found that women experiencing IPV can make up to five attempts to leave their abuser before ending the relationship permanently (Yamawaki et al., 2012). Providers will thus often have the experience of caring multiple times for the same individuals experiencing IPV. In the face of caring for individuals who repeatedly present after a violent assault, providers described feelings of frustration and powerlessness (Colombini et al., 2013; Dawson et al., 2019; Inoue & Armitage, 2006). Specifically, providers felt frustrated when patients experiencing IPV returned to the same environment (Colombini et al., 2013; Dawson et al., 2019; Fay-Hillier, 2016; Inoue & Armitage, 2006; O’Malley, 2011; Robinson, 2010; Sormanti & Smith, 2009) or did not wish for police involvement (Fay-Hillier, 2016; Robinson, 2010; Zijlstra et al., 2017). These experiences resulted in a sense of futility and eventually resulted in many providers avoiding IPV-related discussions (Efe & Taşkın, 2012; Inoue & Armitage, 2006; Loughlin et al., 2000; Robinson, 2010; Sormanti & Smith, 2009). Some felt that this forced them to develop an impersonal approach (Sormanti & Smith, 2009; Tower et al., 2012; van der Wath et al., 2013).
These feelings of frustration and helplessness in conjunction with realization of systemic problems ultimately predispose providers to burn-out (Williston & Lafreniere, 2013). Not only does provider burn-out decrease care quality (Salyers et al., 2017), but it can also lead providers slip from understanding to blame toward their patients (Ferencik & Ramirez-Hammond, 2019).
In the context of ED care-seeking for IPV, patients report negative interactions when providers display harmful behaviors. This contributes to patients’ secondary victimization. Patients may approach care in a more guarded manner, potentially declining additional resources. They may also avoid ED care unless severe violence makes it absolutely necessary. These intersecting factors drawn from the literature contribute to a cycle as illustrated in Figure 2.
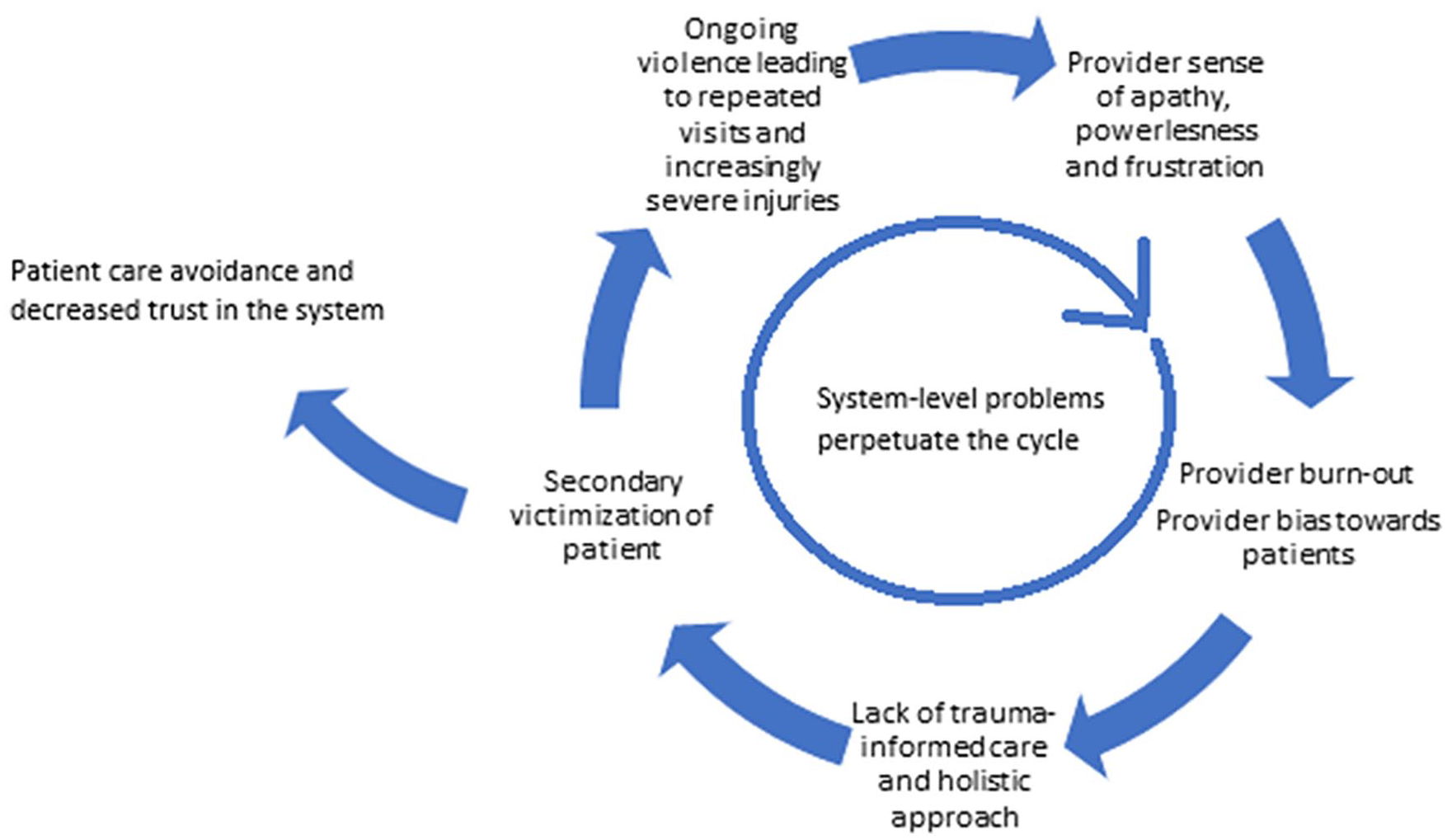
Provider perspective cycle resulting in negative patient care experiences.
It is our recommendation that institutions use evidence-based interventions focused on minimizing moral distress and burn-out for ED care providers. This includes implementing comprehensive wellness initiatives, providing leadership and infrastructure that supports workers’ health and building a safe work-place culture. Finally, we recommend addressing systemic and institutional issues producing burnout such as short staffing (Mazurek, 2019).
Limitations
Limitations of Current Evidence
In general, the predominance of retrospective and qualitative studies using convenience sampling make this review’s results prone to bias. In addition, many studies failed to capture detailed socio-demographic data on study participants. Of the studies reporting demographic data, there was a marked lack of inclusivity of participants diverse in gender, race, ethnicity, sexual orientation, and disability in most studies leading to potential selection bias.
Limitations of SR
The PRISMA 2009 Checklist (Moher et al., 2009) was used to reflect high-quality SR methodology. We reduced language limitation using extensive and diverse search methods, avoided outcome reporting limitations by using each author’s wording for results and independently screened, reviewed, and appraised studies to improve study rigor (Higgins & Green, 2011). However, our study does have inherent limitations. First, we may have missed some studies not published in English/French or published in other grey literature sources. Second, the World Health Organization’s IPV definition used for most studies, including ours, is incomplete because it excludes financial violence, stalking, and cyber-violence (World Health Organization, 2012) which may have under-detected participants. In addition, as is a common limitation for many studies related to IPV, patients experiencing IPV but not disclosing this would not see their experiences included in the data reviewed. Third, rigor varied within the included studies with only eight satisfying all CASP criteria and only 14 explicitly using two independent reviewers, increasing the risk of confirmation bias and decreasing validity. In addition, many studies had small sample sizes with 81% of studies having less than 50 participants. While an appropriate sample size in qualitative research is still debated (Vasileiou et al., 2018), saturation was only reported in 14 studies. While we included studies regardless of quality to ensure no data were missed, this introduces challenges in interpreting results from the studies with limited internal validity.
Strengths
This SR adds to the current body of knowledge and extends beyond previous reviews since it is the first to synthesize study findings associated with negative and positive care experiences from both patient and provider perspectives. It also uniquely undertook a detailed analysis of demographic and social identity data recorded in each study and specifically used search strategies aiming to include perspectives from a diverse range of patients and providers.
This review holistically summarizes ED-specific contributors to positive and negative care experiences. There are few existing SRs exploring ED IPV-care experiences, with most focus on IPV-screening efficacy. While perspectives from nurses and physicians continue to have the strongest presence in the literature, our SR successfully included evidence from a wider variety of provider backgrounds.
Recommendations for Future Research
More studies evaluating the impact of negative ED experiences on overall access to care and ability to stop, avoid, or escape violence are needed. Further studies focusing on ED care experiences after a remote experience of IPV and on follow-up care offered through EDs would be of benefit. Several studies captured the provider burden of caring for IPV-affected patients—another area requiring further research.
This review revealed large gaps in the literature surrounding patients and providers who identify as male or as members of equity-deserving groups such as Two-Spirit, lesbian, gay, bisexual, transgender, queer or questioning, BIPOC or experiencing a disability. Pointed efforts are necessary to include a diverse range of ED patient and provider perspectives. Detailed participant demographic data surrounding age, gender, sexual orientation, race, ethnicity, language, and disability should be prioritized.
Conclusion
This SR of ED care experiences for patients with lived experience of IPV and their providers identified contributors to positive experiences including access to private and timely care, knowledgeable providers, and accessible specialized care teams with efficient referral systems. Primary contributors to negative care experiences included provider lack of knowledge and prejudice, lack of trauma-informed and patient-centered care, lack of time and privacy in the ED, and lack of accessible IPV-care teams. This review also indicated that both parties experience frustration and hopelessness associated with the limitations of the healthcare system, stemming from complex interactions at the individual, institutional, and systemic levels. Findings underscore the need for increased attention toward more inclusive population recruitment in future studies. Correcting the systemic, institutional, and individual problems outlined in this review should be guided by intersectional, equity-based policy creation, as well as promotion of provider education and burn-out prevention. The findings of this SR are a step toward elucidating research needs and interventions to provide high-quality, TIC that will contribute to reduced morbidity and mortality related to IPV.
Supplemental Material
sj-docx-1-tva-10.1177_15248380221118962 – Supplemental material for Patient and Provider Emergency Care Experiences Related to Intimate Partner Violence: A Systematic Review of the Existing Evidence
Supplemental material, sj-docx-1-tva-10.1177_15248380221118962 for Patient and Provider Emergency Care Experiences Related to Intimate Partner Violence: A Systematic Review of the Existing Evidence by Emma Duchesne, Aisha Nathoo, Melanie Walker and Susan A. Bartels in Trauma, Violence, & Abuse
Footnotes
Acknowledgements
We would like to thank Alison Ross, B.Sc. (Queen’s University), Lorenzo Robiso, B.Sc. (Queen’s University), Daniel Duchesne, M. Eng., P. Eng. (Université Laval), and Sandra Halliday, M.Sc. MLIS. (Queen’s University) for their support.
Declaration of Conflicting Interests
The author declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research and/or authorship of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.