
Abstract
Autistic individuals are at an increased risk of experiencing victimisation. Previous reviews have focussed specific types of victimisation. Thus, a clearer picture considering the range of victimisation experiences autistic people face is required. This systematic review aims to identify the prevalence of victimisation in autistic individuals considering a variety of victimisation types (e.g., bulling, sexual victimisation, and crime) in both adults and children from clinical and community settings. Through systematic searches of relevant databases, 291 studies met the criteria for review. Of those, 34 studies met the inclusion criteria: a) quantitative studies, b) involving autistic individuals, c) reporting prevalence rates of victimisation. Meta-analysis found a pooled prevalence rate of victimisation of 44% in autistic individuals. Subgroup analysis examined moderating factors as high heterogeneity was present. This found the pooled prevalence rates for bullying to be 47%, 16% for child abuse, 40% for sexual victimisation, 13% for cyberbullying, and 84% for multiple forms of victimisation in autistic individuals, though heterogeneity remained. Correction for participants’ age, reporter used, and the population which the sample was recruited from did not reduce heterogeneity. Although heterogeneity impedes the definitive interpretation of the findings, this review illustrates the need for strategies and interventions to reduce the incidence of victimisation.
Introduction
Victimisation involves acts in which an individual is subject to cruel or unjust treatment, including bullying (intentional and repeated physical, verbal, and/or relational acts in situations wherein there is a difference in power; Olweus, 1993), maltreatment (including neglect and physical and emotional abuse), sexual victimisation (e.g. rape and sexual assault) and crime (e.g. robbery, theft and assault). There is a high prevalence of victimisation in individuals with Autism Spectrum Disorder (ASD), hereafter referred as autism (Paul et al., 2018; Sreckovic et al., 2014). Autism is a developmental condition characterised by difficulties with social communication and interaction, and restricted, repetitive behaviours or interests (World Health Organisation, 2018). Previously, there were subtypes within autism diagnosis, including Asperger’s Syndrome and Pervasive Developmental Disorder, Not Otherwise Specified. In the past decade, autism has been redefined as a single condition characterising a spectrum of functioning, to improve reliability and consistency in autism diagnosis.
Autistic individuals report higher rates of bullying, child abuse, sexual victimisation and crime victimisation than non-autistic individuals (Paul et al., 2018; Weiss & Fardella, 2018). Traits of autism, such as, misunderstanding non-verbal interactions or inappropriately responding in reciprocal conversations (Hellström, 2019), may increase the risk of victimisation. Restricted and repetitive behaviours may make individuals stand out from their peers, increasing vulnerability to bullying (Sreckovic et al., 2014). They may also experience high levels of social isolation (Liptak et al., 2011; Orsmond et al., 2013) and stigma (Neely & Hunter, 2014).
The impact of victimisation is well-documented. For autistic individuals, bullying is associated with anxiety and depression (Mayes et al., 2013), low self-esteem (Reid & Batten, 2006) and suicidal ideation or attempts (Carter, 2009). Physical and sexual abuse increase the risk of suicidal ideation or attempts in autistic people (Richa et al., 2014). Victimisation is associated with high levels of stress and symptoms of Post-Traumatic Stress Disorder (PTSD; Paul et al., 2018). Those who are victimised are at increased risk of being re-victimised (Pfeffer, 2016), perpetuating the cycle.
Given the increased risk of victimisation and clear detrimental outcomes, prevention is paramount. Several national and international acts and policies have been implemented. For example, in England, The Autism Act (2009) and the Fulfilling and Rewarding Lives strategy (HM Government, 2010, 2014) seek to increase the awareness and understanding of autism across public services and improve access to services and support in the community. However, measures are largely in response to victimisation, with less focusing on prevention. In 1998, Autism-Europe highlighted the need for prevention of violence and mistreatment against autistic individuals and outlined how educational programmes for autistic individuals and training for family and care professionals could help prevent victimisation.
Despite efforts, research suggests victimisation of autistic people is an ongoing problem. Hebron and Humphrey (2014) found 77% of over 800 autistic children in the UK were currently experiencing bullying. The Crime Survey for England and Wales found 9% of respondents with a ‘social or behaviour impairment’ (which included autism) experienced sexual assault in the three years prior to 2018, which was higher than rates for individuals with other conditions (Office for National Statistics, 2019). To inform prevention efforts, a clear understanding of the victimisation experiences of autistic individuals is required. Previous reviews have focussed on specific types of victimisations, such as bullying and cyberbullying (See: Beckman et al., 2020; Maïano et al., 2016; Sreckovic et al., 2014). However, focussing only on one specific victimisation type may prevent understanding of the multifaceted risk faced by this population. For instance, Pfeffer (2016) found autistic people who experienced victimisation are likely to be re-victimised in the same year, sometimes differently to their first victimisation. The traumatic impact of victimisation can be cumulative and in autistic individuals, increased exposure to traumatic events has been associated with greater severity of PTSD symptoms (Rumball et al., 2021). Thus, examining a single victimisation type could underestimate the impact of these experiences, overlooking the potential for multiple incidents across a variety of contexts. Establishing an estimate of overall victimisation rates for autistic individuals could highlight social problems and identify gaps in existing research relevant to directing prevention efforts.
Aims
This systematic review and meta-analysis considers a wide range of victimisation types (e.g. bullying, sexual victimisation, crime and child abuse), providing an overall prevalence rate of victimisation in autistic individuals. To the authors’ knowledge, this is the first time a diversity of victimisation experiences has been systematically reviewed in autistic people.
Method
Protocol and Registration
The protocol was designed in line with Preferred Reporting Items for Systematic Review and Meta-Analysis guidance (Shamseer et al., 2015) and was registered on PROSPERO (https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=151726)
Inclusion Criteria
Studies were selected according to the following criteria: 1. Participants: Adults and children were included. 2. Condition: Individuals diagnosed with autism, including Asperger’s Disorder and Pervasive Developmental Disorder Not Otherwise Specified (PDD-NOS), using all versions of the Diagnostic and Statistical Manual of Mental Disorders and the International Statistical Classification of Diseases and Related Health Problems, or those whereby the severity of symptoms reached the clinical threshold for autism assessed using validated instruments. For example, the Social Responsiveness Scale (Constantino & Gruber, 2005) measures autistic traits and has been shown to have predictive validity against the diagnostic criteria of autism (Chan et al., 2017). 3. Outcome: Studies reporting a prevalence rate of victimisation were included. 4. Study Design: Quantitative studies only. Case studies, book reviews and systematic reviews were excluded. 5. Other restrictions: There were no restrictions by setting type, publication date or language. Published and unpublished materials were included.
Information Sources and Search Strategy
Search Terms Included in the Systematic Search.
Selection Process
A total of 17,079 records were identified through literature searching. 6567 duplicate records were removed, and the title and abstract of the remaining 10,512 were screened against the eligibility criteria, resulting in a further 10,221 exclusions. In total, 291 titles met the inclusion criteria; full reports were sought. Nine papers could not be accessed, and one paper could not be translated. One additional paper was identified through reference searching. Available full text papers were reviewed by XX [blinded for peer review] to determine if they met the inclusion criteria. Two hundred and forty-five records were excluded.
Data Extraction
Information extracted included: publication type, country of origin, funding source, participant characteristics including diagnosis, age, and intellectual ability, study design, recruitment procedures, assessment tools, statistical techniques and prevalence rates of victimisation. Information relevant to risk of bias was documented during the data extraction process.
Quality Assessment
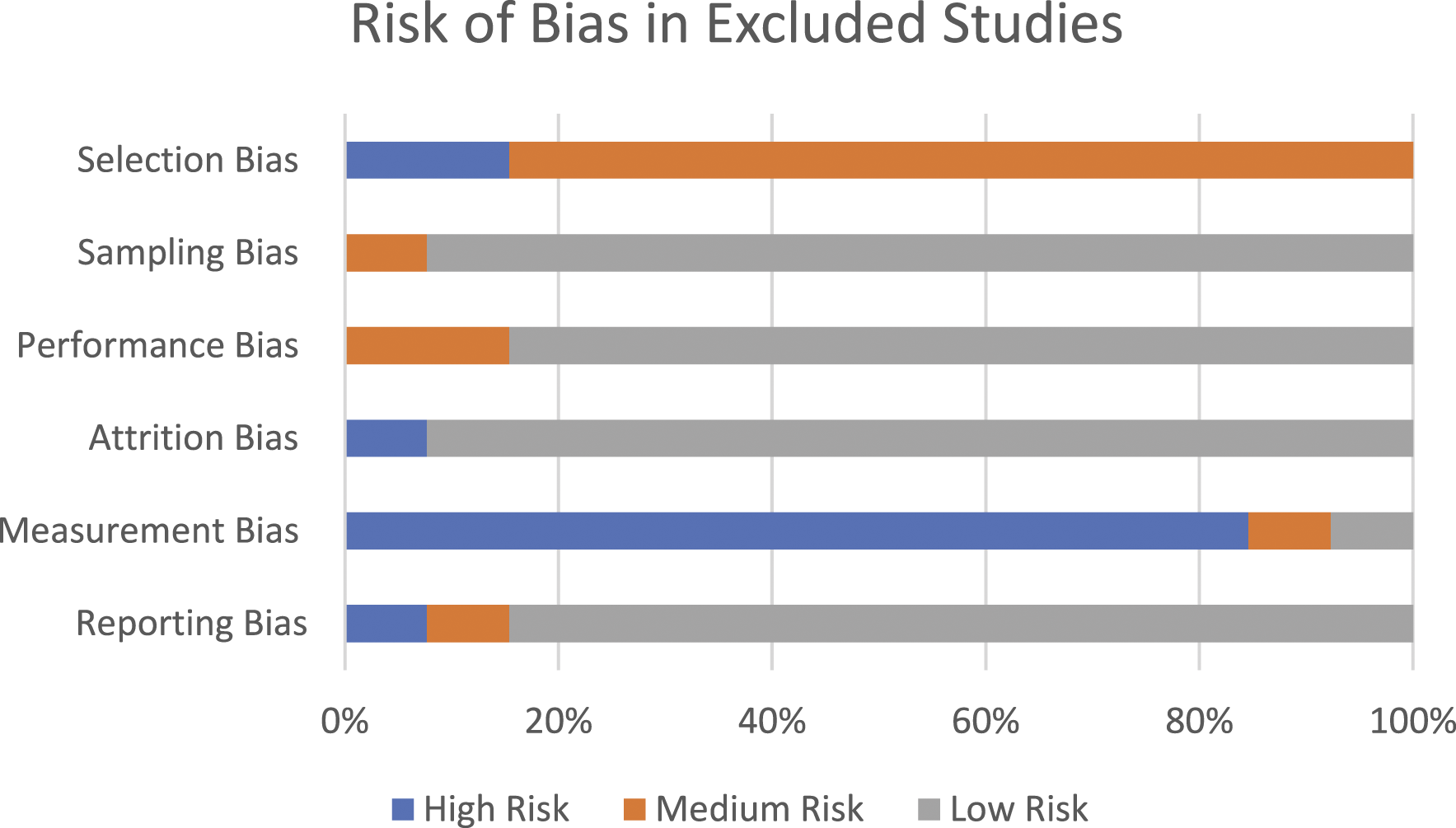
Quality assessment was conducted using Critical Appraisal Skills Programme Checklists (CASP, 2018). This considered the appropriateness of the study design, choice of outcome measure, statistical issues, reliability of measures used, recruitment processes and precision of the results. Risk of bias was separated into six types of bias: selection, sampling, performance, attrition, measurement and reporting bias. Judgement on the risk of bias was rated as ‘high’, ‘medium’ and ‘low’ as per the Centre for Reviews and Dissemination (2008) guidance. If a study obtained a high-risk rating for any of the categories, it was excluded from the review. Although stringent criterion, it ensured the included studies were of high quality. Quality assessment was completed by XX [blinded for peer review] and an independent party (XX) [blinded for peer review] for improved reliability: no discrepancy between reviewers was found. Forty-seven studies underwent quality assessment. Thirteen received at least one high-risk rating for bias and were excluded from the review. The selection process is detailed in Figure 1. Figure 2 depicts the risk of bias present in the thirteen excluded studies. Thirty-four studies did not present a high risk of bias and were included in this review. Prisma flow diagram showing Study Selection Process. Risk of bias graph for the 13 excluded studies.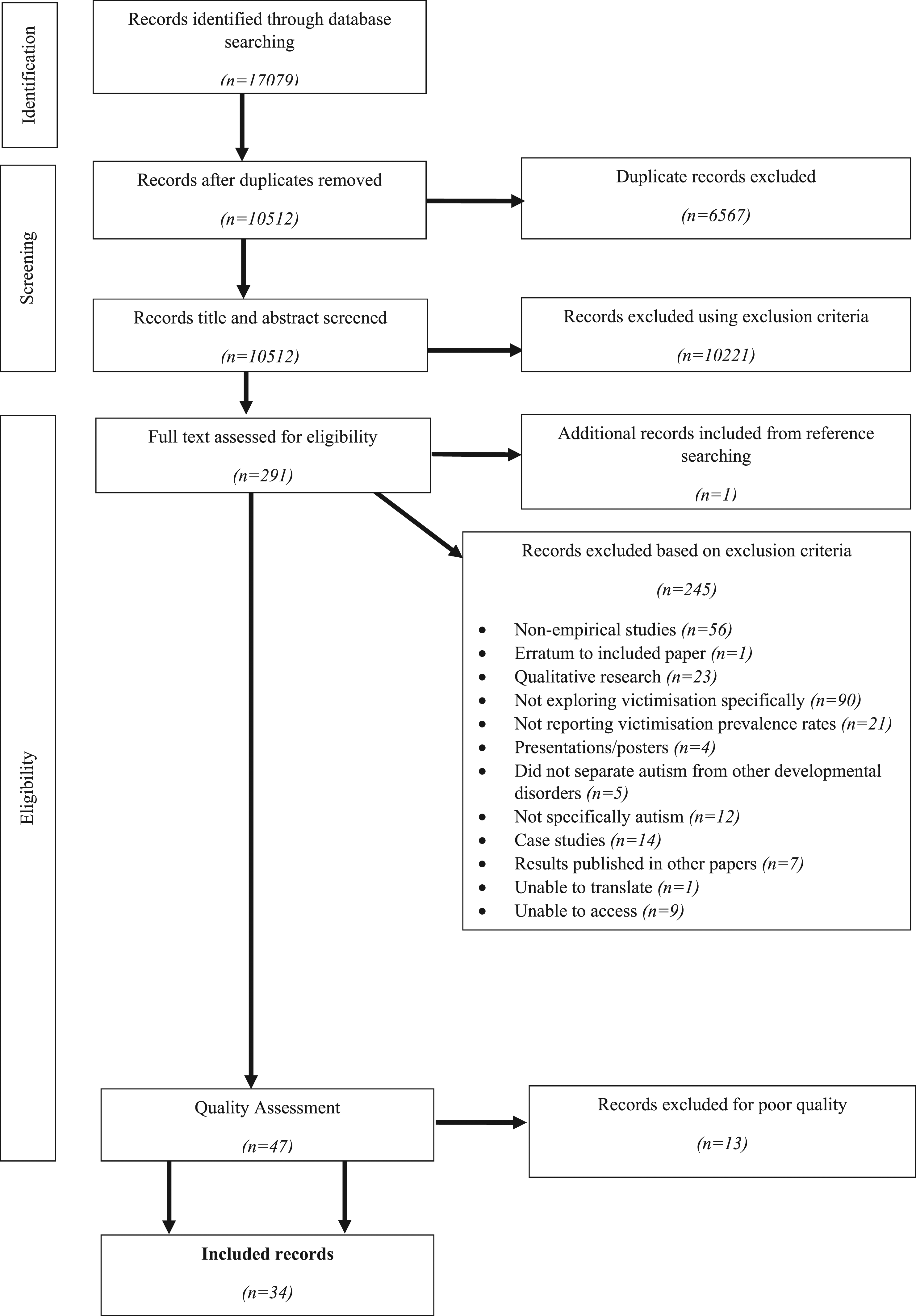
Meta-Analysis
The primary measure of interest, the prevalence rate of victimisation, was integrated across studies using meta-analytic methods. Prevalence rates across the studies were pooled using the inverse-variance heterogeneity model. This required the double arcsine square root transformation method to stabilise the variance (Barendregt et al., 2013). To simplify interpretation, the results were back transformed to natural proportions. A random effects model was used as study-level variability was anticipated. Homogeneity was assessed using I2. All analyses were performed using MetaXL version 5.3 (EpiGear International, 2016).
There were several considerations when determining data to be included in the meta-analysis. First, for cases wherein the study measured victimisation in the past year and lifetime (Paul et al., 2018; Pfeffer, 2016), prevalence of lifetime victimisation was included in the meta-analysis, as this incorporated past-year victimisation. Secondly, for studies wherein multiple prevalence rates were provided via multiple reporters, decisions were made with consideration of empirical literature.
Ashburner et al. (2019) found no significant difference between adolescent self- and parent-reports of bullying and cyberbullying victimisation. As autistic self-reports have been found to have validity (Keith et al., 2019; Van Roekel et al., 2010), self-reported bullying and cyberbullying was therefore included in the meta-analysis, as two separate prevalence rates (A = bullying, B = cyberbullying). Hebron and Humphrey (2014) found a positive correlation between parent- and teacher-reports of bullying. Sensitivity analysis identified that neither had a substantial effect on heterogeneity. As parents may witness bullying that occurs outside the classroom, parent-reported data were included in the meta-analysis. Hu et al. (2019), Van Schalkwyk et al. (2018) and Chou et al. (2019) found low agreement between parent- and self-reported victimisation. Similarly, Van Roekel et al. (2010) found low agreement between teacher-reported bullying victimisation and peer- and self-reported victimisation. As participants were older children, it is possible that parents and teachers are unaware of victimisation experiences (Van Schalkwyk et al., 2018), especially for cyberbullying (Hu et al., 2019). Thus, self-reported victimisation was favoured for inclusion in the meta-analysis for these studies.
Thirdly, Toseeb et al. (2019) provided prevalence rates for current experiences of bullying at two time points for the same sample. The most recently captured prevalence rate was used in the meta-analysis. Finally, two studies were not included in the meta-analysis but were qualitatively synthesised due to the nature of the data presented. Doyle (2016) provided prevalence rates for specific bullying behaviours rather than an overall prevalence rate for bullying. For example, ‘a teen left them out of an activity they really wanted to be included in’ (Doyle, 2016, Table 1, p. 48). It was not possible to synthesise this data into an overall prevalence rate. Hall-Lande et al. (2015) provided prevalence rates for types of maltreatment experienced by a sample of children, all of whom had been maltreated. These results would influence the meta-analysis as the sample would be biased to victimised children alone.
Results
Study Characteristics
In total, 633,051 participants were involved in 34 included studies, which included individuals with autism, Asperger’s Syndrome, and PDD-NOS, and comparison groups of individuals with intellectual disabilities, physical disabilities and those without disabilities. Participant age ranged from one to 57 years. Seventeen studies originated in the United States, three in the United Kingdom,1,14,26,27 three in Taiwan,9,15,17 three in Canada6,7,32 and two in Australia.2,18 One study was conducted in each of the following: Sweden,3 China, 1 South Korea,16 South America,19 the Netherlands30 and France.23
Most studies were cross-sectional (n = 27). Three utilised a case-control design,3,23,25 three used cohort design,12,13,17 and one was a prospective longitudinal study.27 Seven studies recruited participants from the general population.12,13,17,18,25,26,27 Eight utilised clinical samples from psychiatric units or inpatient/outpatient services.1,3,4,9,15,20,21,29 Eighteen studies recruited participants from the community through local schools, support groups and autism services. One study used a community and clinical sample.23 Six studies involved adult participants,3,5,6,11,25,33 and twenty-eight studies involved children and adolescents.
Descriptive Information for Included Studies.
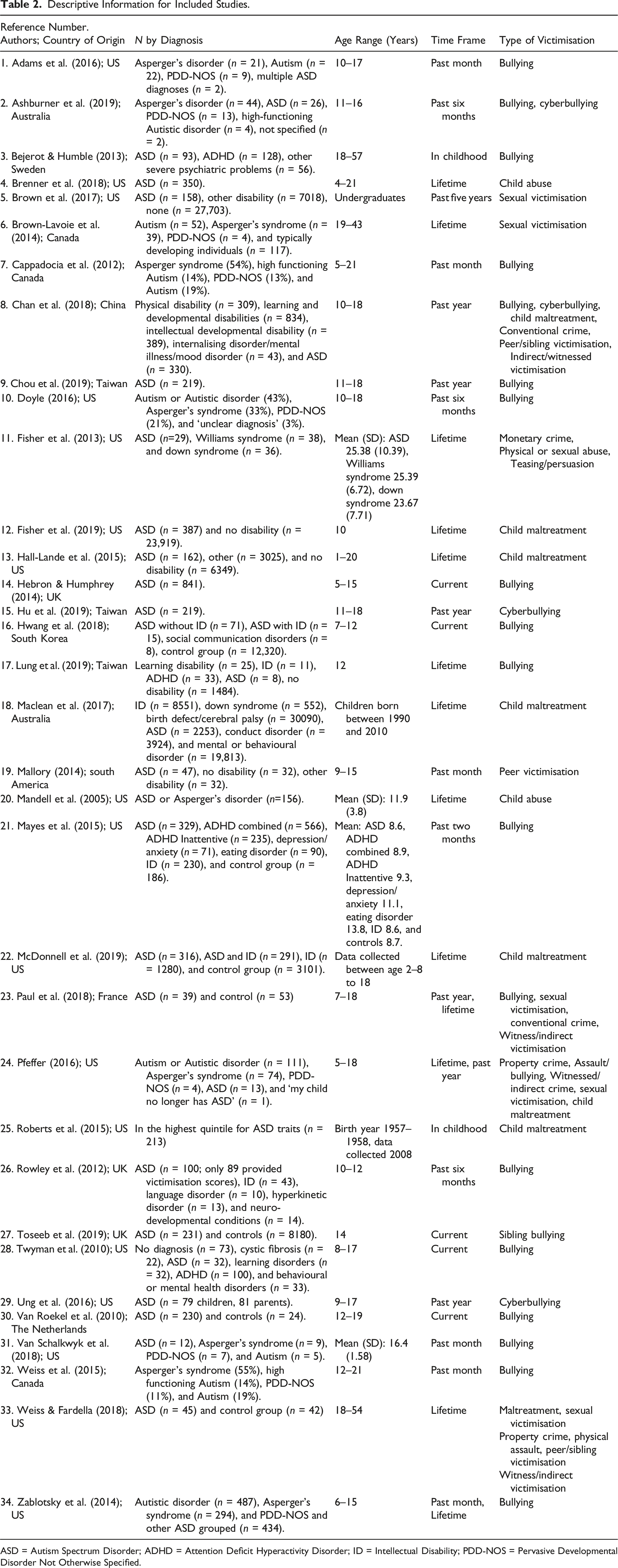
ASD = Autism Spectrum Disorder; ADHD = Attention Deficit Hyperactivity Disorder; ID = Intellectual Disability; PDD-NOS = Pervasive Developmental Disorder Not Otherwise Specified.
Risk of Bias
There was some evidence of bias in the included studies which is presented in Figure 3. The most common types of bias present were measurement and selection bias. Risk of bias graph for the 34 included studies.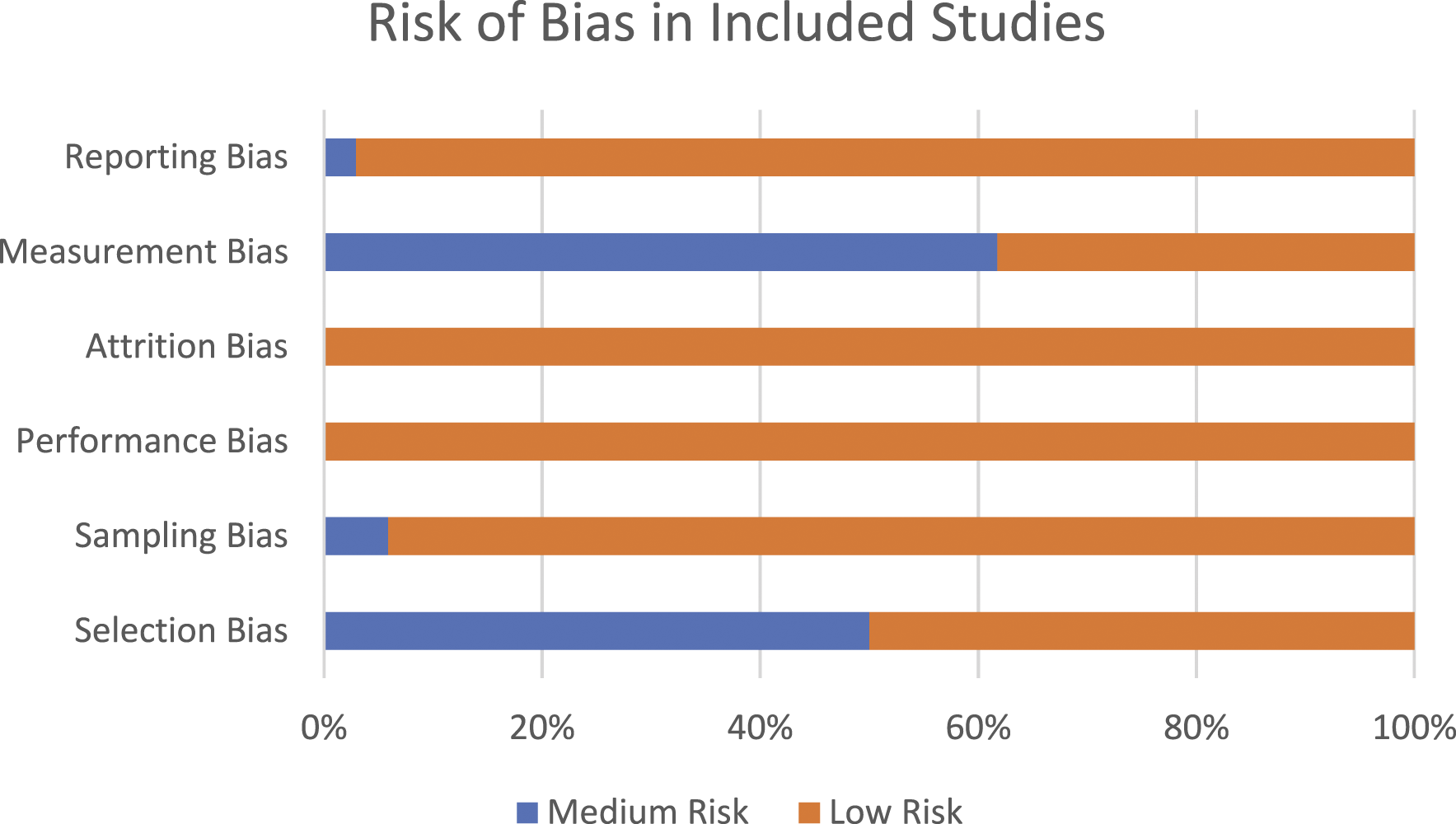
Prevalence of Victimisation
The pooled prevalence of victimisation in autistic individuals was 44% (See Figure 4). There was substantial heterogeneity between the studies (I
2
= 99%). Sensitivity analysis indicated that no single study had a substantial impact on heterogeneity. Pooled Prevalence rates for reported victimisation.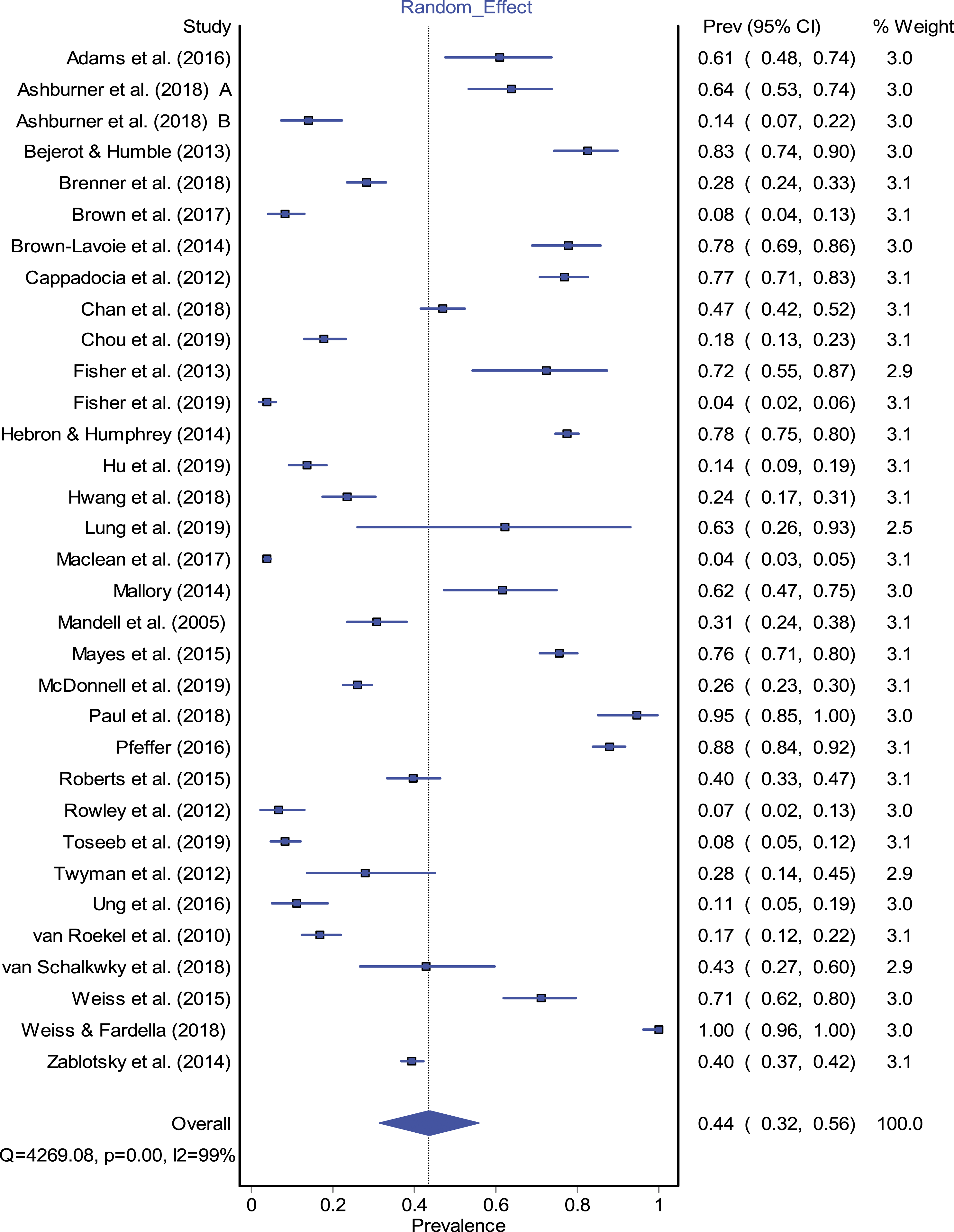
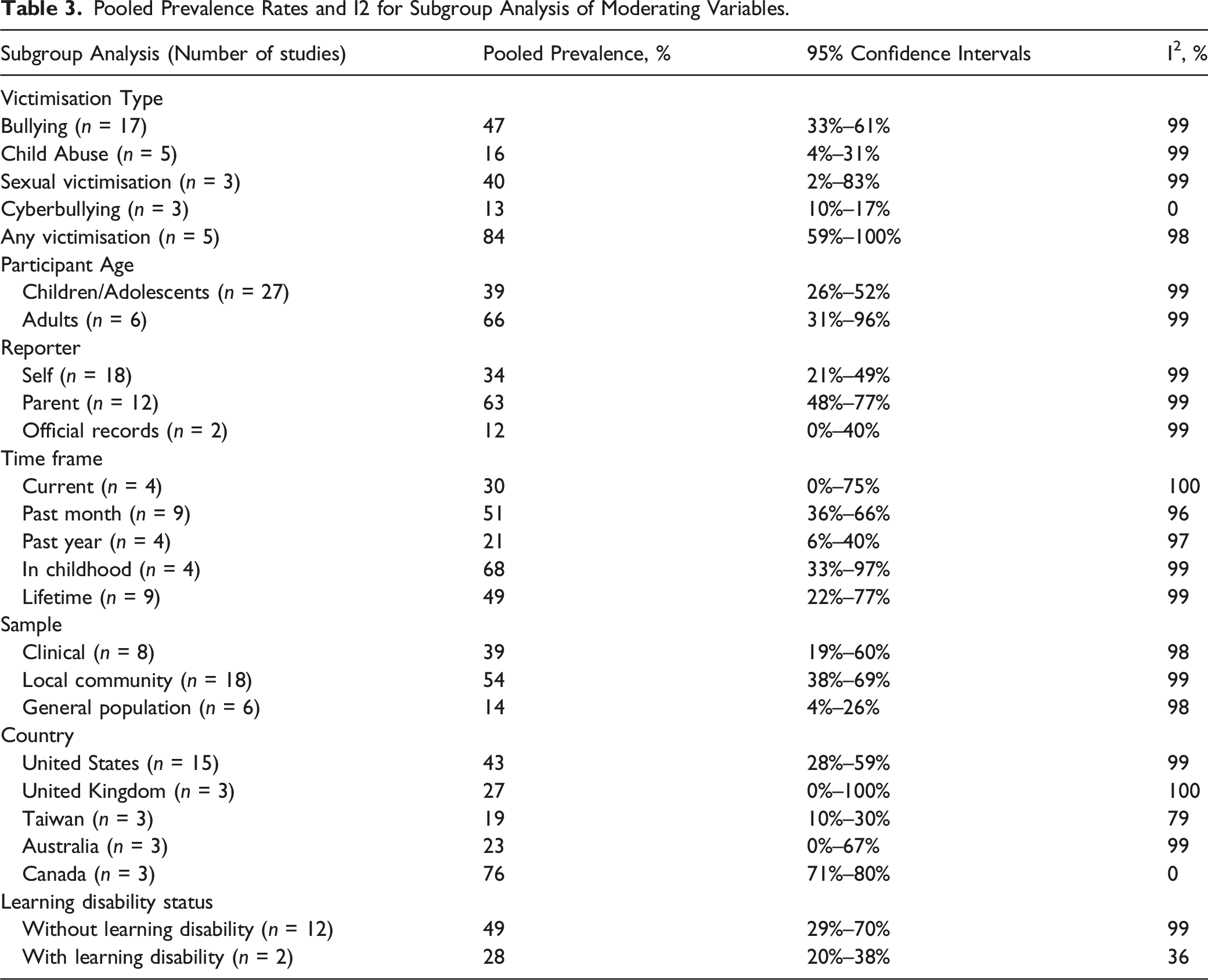
Subgroup Analysis
Pooled Prevalence Rates and I2 for Subgroup Analysis of Moderating Variables.
Sample Characteristics
Subgroup analysis identified a pooled prevalence rate of 39% for studies utilising child or adolescent participants (age<18 years), and 66% in studies using adult autistic participants (age>18 years). For clinical samples, the pooled prevalence rate for victimisation was 39%. In the local community samples (e.g. samples recruited from one local area), pooled prevalence rate for victimisation was 54%. In general population samples, the pooled prevalence rate of victimisation was 14%. Substantial heterogeneity was present across all subgroups.
Of the included studies, 13 did not report on the cognitive abilities of the participants and several studies used a sample with a wide range of intellectual abilities (e.g. Brenner et al. (2018) report verbal IQ scores to range from 30 to 125). Nevertheless, 10 studies reported their samples to be ‘high functioning’ or that the sample scored greater than 70 on a validated measure of intellectual ability3,6,9,15,21,23,29,30,31,33 and two studies provided separate prevalence rates for those with and without learning disabilities (Hwang et al., 2018; McDonnell et al., 2019). Thus, using 14 sets of data, pooled prevalence rates of victimisation for those without a learning disability was 49%, even higher than the 28% for those with a learning disability.
Subgroup analysis including 27 studies from 5 countries was conducted. The pooled prevalence of victimisation was 43% for the US, 27% for the UK, 19% for Taiwan, 23% for Australia and 76% for Canada. Substantial heterogeneity was present across all subgroups, except the Canada subgroup (I 2 = 0).
Measurement Characteristics
Subgroup analysis of victimisation type identified a bullying victimisation pooled prevalence rate of 47%. Doyle (2016) found the most frequent bullying behaviours experienced by autistic children were being left out of activities (72%), being teased (50%) and being threatened or beaten up (43%). Pooled prevalence of child abuse was 16%. Hall-Lande et al. (2015) found that in children who had experienced abuse, 5.8% had experienced neglect, 35% physical abuse, 8.3% sexual abuse, 1.3% mental injury and emotional harm and 0.6% medical neglect. Pooled prevalence rates in the current data were 40% for sexual victimisation (not classified as child abuse by the included studies), 13% for cyberbullying and 84% for multiple forms of victimisation measured altogether. There was substantial heterogeneity in all these subgroups, except for cyberbullying. Subgroup analysis by reporter used found a pooled prevalence of 34% for self-reporters, 63% for parent-reporters and 12% for official records.
Subgroup analysis of time frame for reporting victimisation was conducted on 30 studies. Three studies were not included as they reported other timeframes than the identified time frames (e.g. past two months). The pooled prevalence of current victimisation was 30%. For victimisation in the past month, pooled prevalence was 51%. For victimisation in the past year, pooled prevalence was 21%. For victimisation in childhood, pooled prevalence was 68%. Pooled prevalence of lifetime victimisation was 49%. Substantial heterogeneity was present across all subgroups.
Additional Subgroup Analysis
Additional analysis was conducted within subgroups (e.g. adults only and bullying only) to examine the remaining heterogeneity. Two analyses indicated reduced heterogeneity. In studies using adult participants, prevalence rates of victimisation in childhood were 79% (I 2 = 0%). Similarly, when examining child abuse, 28% of individuals within a clinical sample reported experiencing child abuse (I 2 = 0%). Thus, heterogeneity may be explained by a combination of moderating factors rather than single influences.
Discussion
Critical Findings.
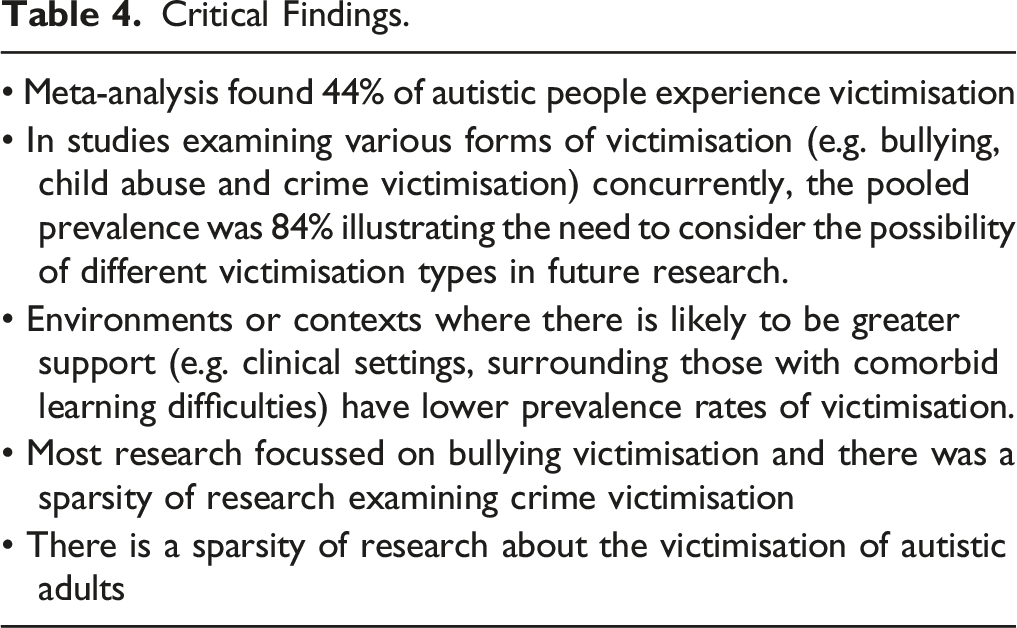
Five studies examined multiple types of concurrent victimisation (Chan et al., 2018; Fisher et al., 2013; Paul et al., 2018; Pfeffer, 2016; Weiss & Fardella, 2018), finding a pooled prevalence rate of 84%, illustrating the importance of measuring various forms of co-existing victimisation. Pfeffer (2016) found that autistic young people who experienced victimisation were likely to be re-victimised in the same year, sometimes differently to their first victimisation. The prevalence of victimisation may be higher than recorded, as studies examining discrete forms of victimisation (e.g. bullying or sexual victimisation) do not measure other victimisation experiences. Future research examining the prevalence or impact of victimisation should account for the possibility of multiple victimisation experiences, for example, by using the Juvenile Victimization Questionnaire (Hamby et al., 2005) which assesses five categories of victimisation.
Subgroup analysis illustrated a higher prevalence of victimisation in community compared to clinical groups (54% and 39%, respectively). Those in the clinical groups may have more severe difficulties (due to autism or co-occurring conditions), so receive more support and access to intervention. This may also explain the greater prevalence rates of victimisation in individuals without learning disabilities. Additionally, participants were recruited from different community settings, including mainstream schools and special education schools. School settings is an important factor in victimisation as mainstream settings may offer less social protection to autistic students (Zablotsky et al., 2014), leading to greater victimisation in these settings. These factors may influence prevalence rates and heterogeneity within these subgroups.
Another important study-level factor is informant type. In autistic people, self-report has been considered to lack reliability (Mazefsky et al., 2011). Difficulty understanding social situations may affect autistic children’s ability to answer questions on victimisation (Loveland et al., 2001). Nonetheless, autistic adolescents provide more comprehensive assessment of internal experiences than their parents (Keith et al., 2019). Further, Van Roekel et al. (2010) found autistic adolescents had similar perceptions of bullying to adolescents from the general population. There are also challenges in informant-reports of victimisation; parents may underreport bullying (Holt et al., 2008), peers may not witness victimisation (Van Roekel et al., 2010), and teachers may interpret autistic behaviour as bullying (Chou et al., 2019). Subgroup analysis demonstrated higher prevalence rates when parents reported victimisation than self-reporters. However, heterogeneity remained, indicating that choice of reporter alone does not influence prevalence. Future research should utilise multiple reporters to build a comprehensive understanding of victimisation experiences (Rubin et al., 2006): each reporter has their own predictive validity since each observes behaviour in different contexts (Achenbach et al., 1987)
Overall, this review shows a large proportion of autistic people experience victimisation in various forms. At a societal level, greater understanding and acceptance of autism could reduce the risk of victimisation. Education, health and social services should be set up to better understand and support autistic people. This review provides preliminary insights into the development, structure or implementation of prevention programmes. This may include educational interventions to improve knowledge about and attitudes towards autistic individuals (See, Campbell et al., 2019; Staniland & Byrne, 2013). This could reduce stigma and discrimination. Skills training may help autistic individuals to identify when they are being victimised and know how to seek support.
Tailored prevention could be developed based on victimisation type and informed by targeted systematic reviews. For instance, subgroup analysis found higher rates of bullying and sexual victimisation than cyberbullying and child abuse for autistic individuals (potentially due to differences in the risk factors for each type of victimisation). However, the highest prevalence rate for victimisation was found for studies measuring ‘any’ victimisation, reiterating the importance of conducting this review. Collaboration across multiple settings (e.g. schools, social services and community support groups) is crucial for victimisation prevention.
Implications for Practice, Policy and Research.
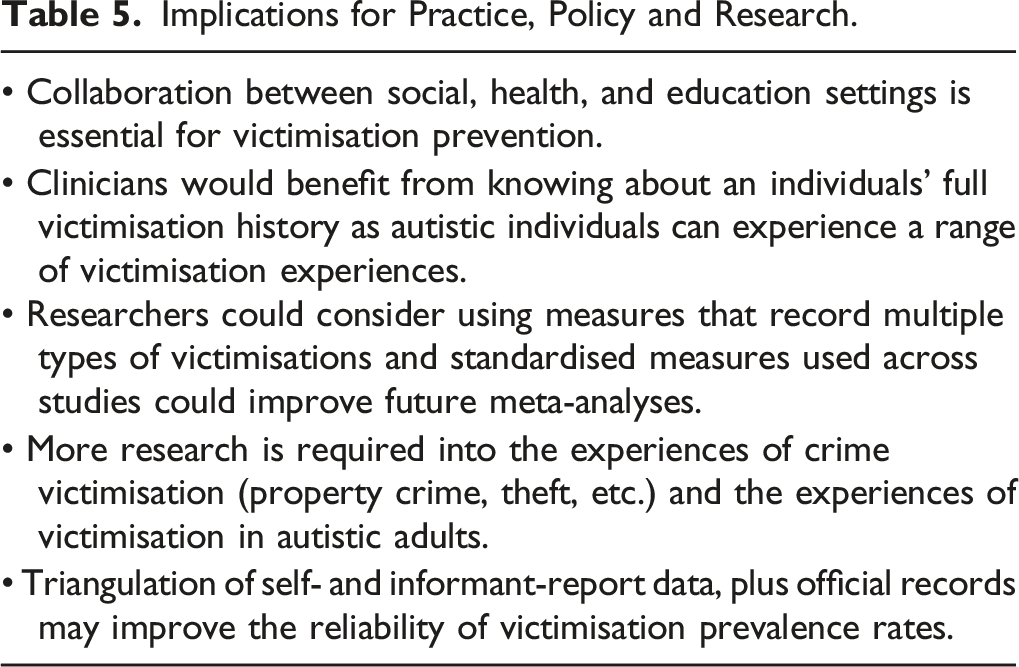
Three main limitations of studies included in this review include the following: (1) lack of validation of autism diagnoses (reliance of informant reports), (2) not accounting for co-occurring conditions and (3) inconsistency across studies in definition of victimisation type. Although parental reports have been used to estimate autism prevalence with good sensitivity and specificity (Russell et al., 2015), validated diagnoses would improve the validity of the results. Additionally, many studies did not report on the presence of learning disabilities. Learning disabilities have been found to increase the risk of maltreatment allegations in autistic children (Maclean et al., 2017). However, this review found greater rates of victimisation in those without a learning disability. Greater consideration of learning disabilities could reduce heterogeneity in prevalence rates of victimisation. Finally, definitions of victimisation were provided to participants in some studies, but not documented in others. As such, constructs may have been interpreted differently between participants (Sreckovic et al., 2014). For example, the term ‘peer victimisation’ has been used interchangeably with bullying within victimisation literature but may be interpreted differently by participants.
Disclosure is an important consideration for future victimisation research, as fear of reporting victimisation may influence the findings (Pfeffer, 2016). For example, survivors of sexual abuse may feel unable to disclose their experiences (Sable et al., 2006), and stigma associated with revealing abuse may influence caregiver-reports (Mandell et al., 2005). Researchers should be conscious of potential recruitment bias: most studies do not report how their study aims were presented to potential participants. The exception was Weiss and Fardella (2018) who stated their study was a project about interpersonal violence.
Strengths and Limitations
Strengths of this review include more than 17,000 records identified though the initial search procedures, the use of validated scales in many studies, a large number of participants, and stringent quality assessment procedures. However, there was a still a low to moderate risk of bias present in the included studies. The main limitation is substantial heterogeneity in the pooled prevalence rates. Explanations include differences in victimisation measures and variations in timeframes used, co-occurring psychiatric conditions, or a range of participant-level differences such as socioeconomic status, age of diagnosis and ethnicity. The results of this study should therefore be interpreted with caution and replicated considering new evidence. An additional limitation relates to search strategy, as ‘PDD-NOS’ and ‘prevalence’ were not included as search terms in the review, an oversight which may have influenced the number of studies identified. Study selection was conducted by one researcher, which could have introduced bias into the selection process. Finally, several papers could not be accessed or translated. It is unclear whether the inclusion of these studies would have produced more homogenous results.
Conclusions
This review found a pooled prevalence rate of victimisation of 44% in autistic individuals. The available literature exploring child abuse, sexual victimisation and conventional crime in autistic individuals was smaller than studies about bullying. More research is required in these areas to clarify the experiences of autistic individuals and identify suitable interventions to reduce the risk of victimisation. Future research should explore co-occurring conditions and protective factors in victimisation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Notes
Author Biographies
Dr. Grace Trundle, Forensic Psychologist from the University of Nottingham. Her doctoral thesis focussed on victimisation and offending in individuals with Autism and Pathological Demand Avoidance.
Dr. Katy Jones, PhD, is an Assistant Professor of Applied Psychology for the Faculty of Medicine and Health Sciences at the University of Nottingham. She is interested in areas of forensic psychology, and understanding addictive behaviour, impulse control, and decision-making.
Professor Danielle Ropar, PhD, is a Professor for the Faculty of Science at the University of Nottingham who explores individual and group differences in clinical (e.g. autism) and non-clinical populations within the areas of social understanding and sensory processing. She established the Autism Research Team at the University of Nottingham.
Dr. Vincent Egan is a Chartered Clinical and Forensic Psychologist. He was also an Associate Professor for the School of Medicine at the University of Nottingham. His interests include personality and mental disorder in relation to offending, extremism, and sexual and violent offending.