
Abstract
Background: Interpersonal violence against children and adolescents can affect their mental health and functioning in the long term. To reduce mental health problems in children and adolescents, school-based mental health interventions have been shown to be beneficial. A review of school-based interventions designed to mitigate posttraumatic symptoms after interpersonal violence is lacking to date. Methods: We searched for original studies published in English or German until November 2019 in 6 electronic databases. Supplementary search strategies to reduce publication bias were implemented. Peer-reviewed original studies assessing school-based interventions for children and adolescents under the age of 21 after interpersonal violence were included. Relevant data was extracted, synthesised and assessed qualitatively. The methodological quality of included studies was assessed. Results: Of 5,021 unduplicated publications, 15 studies met eligibility criteria. The included studies were almost exclusively conducted in the USA; over half utilised a randomised-controlled design. Studies mainly focussed on Posttraumatic Stress Disorder (PTSD) or depression. In all studies, implemented interventions partially or fully mitigated posttraumatic symptoms. Nine school-based interventions, five of which were based on cognitive behavioural therapy (CBT), were identified. School staff were often involved in intervention implementation besides mental health professionals. Conclusions: School-based interventions can be beneficial to reduce mental health problems in children and adolescents after interpersonal violence. Trained school staff aided by mental health professionals can implement trauma-informed practices at school. While school-based interventions may be a feasible way to provide children and adolescents with accessible mental health care, further research on school-based trauma interventions outside the USA is necessary.
Introduction
During their lives, children and adolescents can be exposed to a myriad of adverse childhood experiences, including but not limited to interpersonal violence (i.e. physical and emotional abuse or neglect, sexual, domestic or community violence, or violent experiences during war and flight). These experiences can be summarised as interpersonal (Maercker & Hecker, 2016) or complex trauma (van der Kolk, 2005). Research has shown that refugee minors, in particular those unaccompanied by adults, are especially affected by interpersonal violence not only in their countries of origin, but also during flight and after arriving in host countries (e.g. Metzner et al., 2016). For example, children of asylum seekers in Germany reported having witnessed physical violence (41%) and having experienced violence at home against other family members (26%), physical attacks against the child (15%), physical child abuse at home (14%) or sexual violence (5%) (Ruf et al., 2010). A Dutch study revealed that compared to accompanied refugee and immigrant minors, unaccompanied refugee adolescents were more often exposed to physical abuse (63% vs. 23%) or sexual violence (20% vs. 8%) and had more often witnessed physical violence (72% vs. 47%) (Bean et al., 2007). Interpersonal violence against children and adolescents is however a problem independent of ethnic background, war or conflict. A global review of meta-analyses reported lifetime prevalence rates for sexual abuse (13%), physical abuse (23%), emotional abuse (36%), physical neglect (16%) and emotional neglect (18%) according to self-report (Stoltenborgh et al., 2015). For Europe, a systematic review reported median prevalence rates for sexual abuse (13%), physical abuse (12%), emotional or psychological abuse (22%), and neglect (27%) in childhood (Moody et al., 2018). As an example of a western industrialised country with no recent war exposure, an assessment of a representative German sample of 2510 participants aged 14 to 94 resulted in prevalence rates for moderate to extreme emotional abuse (7%), physical abuse (7%), sexual abuse (8%), emotional neglect (13%) and physical neglect (22%) during childhood (Witt et al., 2017).
Psychosocial Consequences of Interpersonal Trauma in Children and Adolescents
Experiencing complex interpersonal trauma can impact children and adolescents’ physical and mental health long-term into adulthood, putting them at higher risk, for example, for Posttraumatic Stress Disorder (PTSD), depressive disorders, anxiety disorders, behavioural or conduct disorders, substance abuse, risky sexual behaviour and sexually transmitted infections, chronic disease (e.g. obesity) as well as suicidal or self-harming behaviour, with a dose–response relationship (Hughes et al., 2017; Norman et al., 2012; Perez et al., 2018; Witt et al., 2019). Research has also shown that compared to other types of trauma, interpersonal long-term trauma can result in more (potentially chronic) impairment (Maercker, 2013). For example, higher one-year and lifetime prevalence of PTSD was reported for sexual violence in adulthood (37–50%), child sexual abuse (31–35%), war-related experiences (25–39%) or child neglect (22%) compared to other types of trauma (e.g. accidents: 8–13%, witnessing accidents or violence: 2–7%, fire or natural disasters: 0–5%) (Maercker, 2013; Maercker & Hecker, 2016). A meta-analytic review of 47 studies reported a high prevalence for PTSD (35%), emotional and behavioural problems (25%), depression (21%), anxiety disorders (15%) as well as suicidal ideation and behaviour (5%) in 24,786 refugee and asylum-seeking youths residing in European countries (Kien et al., 2018). In accordance to the ‘domains of impairment in children exposed to complex trauma’ described by Cook et al. (2005, p. 392), interpersonal trauma in childhood was also found to be a risk factor for aggressive, impulsive and problem behaviour, as well as delinquent or criminal behaviour (Hughes et al., 2017; Jimenez et al., 2016; Perez et al., 2018). Especially relevant from an educational point of view, childhood interpersonal trauma can impact children and adolescents’ academic functioning and outcomes, for example resulting in attention and concentration problems, educational underachievement or learning disabilities (e.g. language and literacy skills), discipline problems and conflicts (e.g. with peers or teachers), school changes, repeating forms 1 , absenteeism, or special education needs (Elklit et al., 2018; Holmes et al., 2018; Jimenez et al., 2016; Larson et al., 2017).
The Role of Schools in Providing Mental Health Care following Trauma
Children and adolescents spend a majority of their time at school and can be reached there independent of their ethnic, socioeconomic or familial backgrounds. Especially for children and adolescents who may suffer from a loss of trust in caregivers, a loss of a sense of self or low self-esteem following complex interpersonal trauma (Cook et al., 2005; van der Kolk, 2005), school staff (e.g. teachers), can serve as important attachment figures, provide support and help their pupils to re-learn trust in others. Therefore, schools can serve not only as practical locations to implement and provide interventions and mental health care services, but also as places of resilience (Gerke et al., 2019). For example, in a German survey of people who had suffered sexual violence and contacted a helpline for sexual abuse, participants reported that their well-being was positively affected by their teachers’ reactions and support following disclosure, and that an ongoing interest in their experience was perceived as helpful (Gerke et al., 2019).
In recent years, the benefit of school-based interventions or trauma-focussed practices for children and adolescents has been assessed in systematic reviews (Rolfsnes & Idsoe, 2011; Yohannan & Carlson, 2019; Zakszeski et al., 2017). Rolfsnes and Idsoe (2011) for example assessed the effectiveness of school-based interventions for children and adolescents suffering from PTSD after traumatic events in a meta-analysis of 19 international studies. Their results showed not only that school-based interventions were effective in reducing PTSD symptoms, but also that school staff (e.g. counsellors or teachers) were able to successfully implement the interventions, and that intervention access and completion rate was higher within the school setting compared for example to a clinical setting (Rolfsnes & Idsoe, 2011). Zakszeski et al. (2017) conducted a systematic review of 39 international studies and found that trauma-focussed practices within schools largely led to mitigation of posttraumatic symptoms and internalising problems following trauma exposure. Yohannan and Carlson (2019) assessed 41 international evaluation studies of school-based interventions, concluding that these interventions can help to mitigate posttraumatic outcomes in children after traumatic events. These systematic reviews however did not restrict the trauma exposure to specific events, instead including all types of trauma (e.g. natural disasters) and thus had very heterogenous samples.
Aims of This Systematic Review
Past research has shown the benefit of school-based services for children and adolescents following trauma exposure. However, a comprehensive systematic review on school-based interventions for children and adolescents targeting posttraumatic outcomes specifically after interpersonal violence is lacking to our knowledge. With view to the potentially severe and long-term mental health outcomes following complex interpersonal trauma, there appears to be a substantial gap in research. The current systematic review aims to close this gap by identifying and describing school-based interventions designed to mitigate psychosocial posttraumatic symptoms in children and adolescents after interpersonal violence.
Methods
The methods of this systematic review are based on guidelines for implementation and analysis of systematic literature reviews (e.g. Higgins et al., 2019; Moher et al., 2009).
Search Strategy
Terms Used in Systematic Database Literature Search.
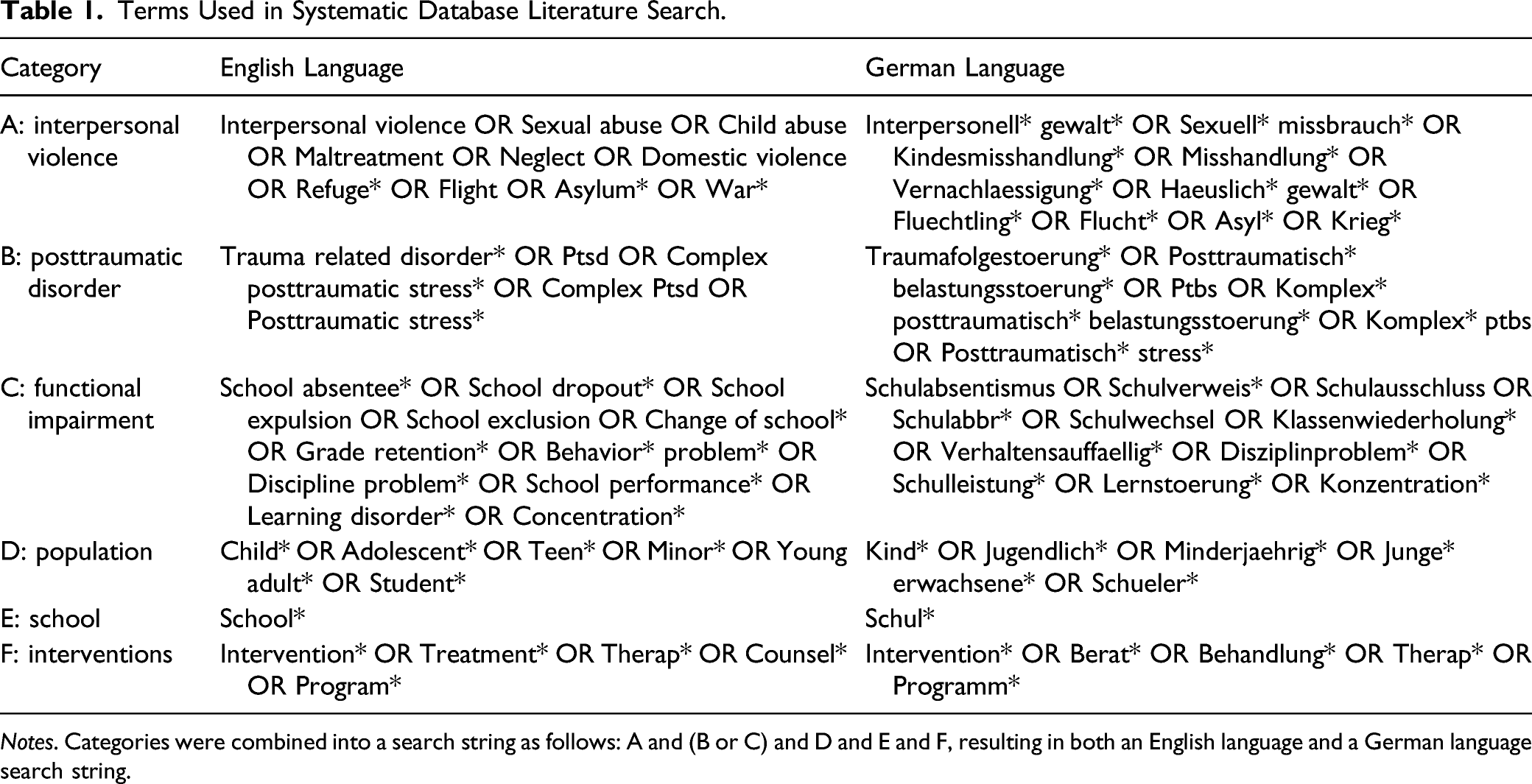
Notes. Categories were combined into a search string as follows: A and (B or C) and D and E and F, resulting in both an English language and a German language search string.
Selection Process
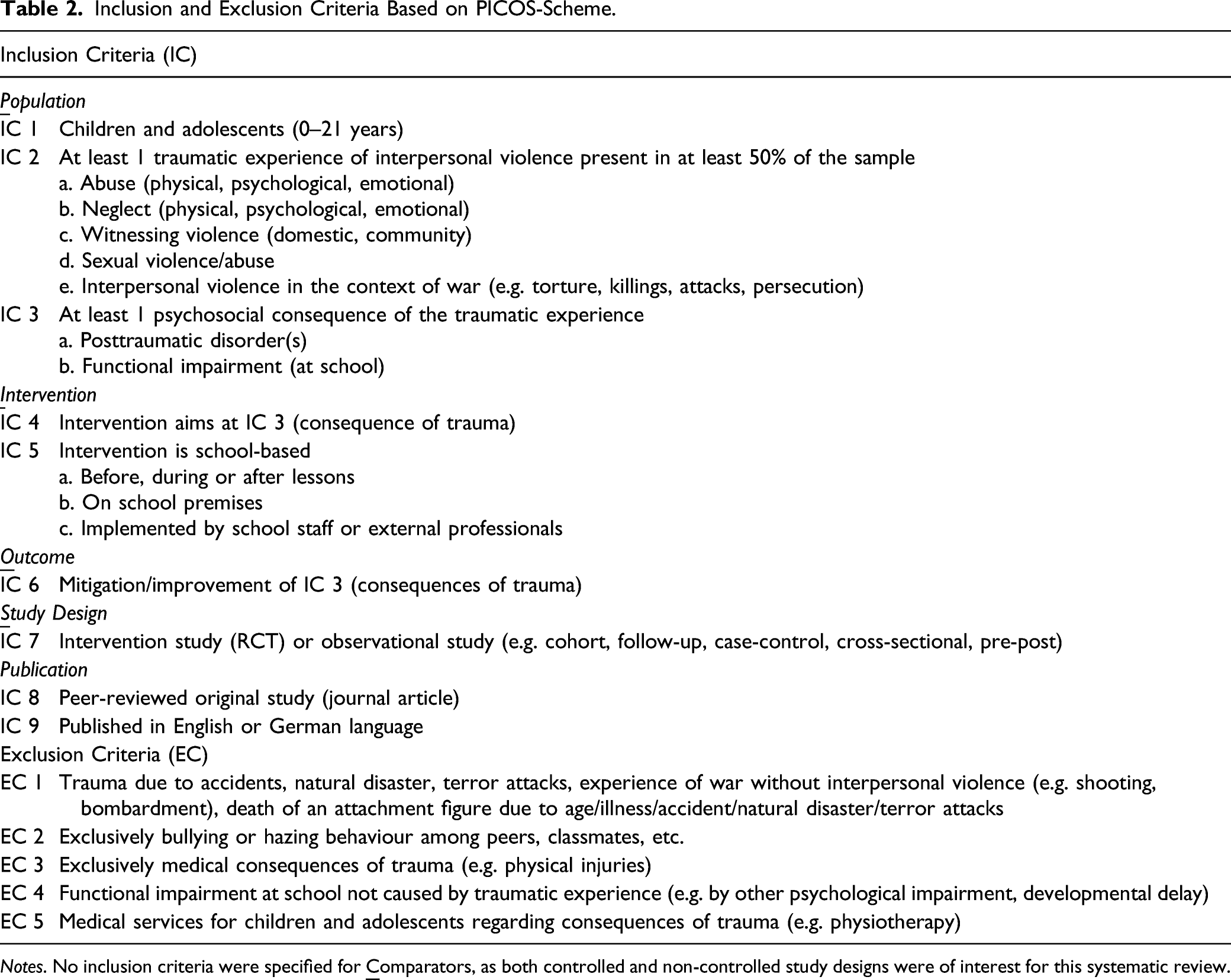
The systematic database search yielded 6,237 results, with an additional 50 publications identified via supplementary search. After removal of duplicates, 5,021 publications remained (see Figure 1). Two independent reviewers (graduated psychologists) screened the remaining publications for conformity with inclusion criteria using title, abstract and keywords (see Table 2). PRISMA-flow-diagram for the presentation of study selection process (Moher et al., 2009). Inclusion and Exclusion Criteria Based on PICOS-Scheme. Notes. No inclusion criteria were specified for 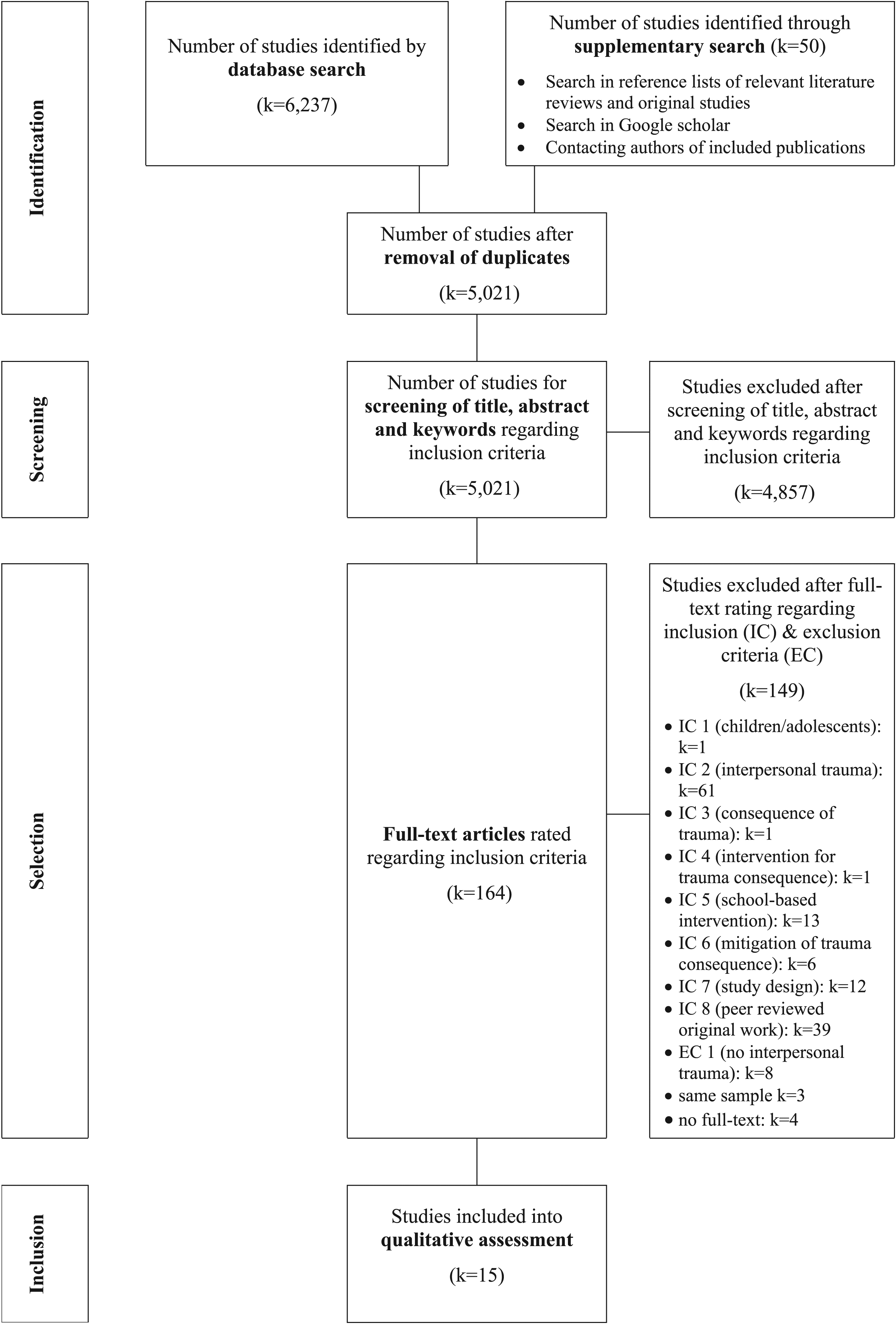
After screening, the full-texts of 164 publications were considered eligible for inclusion into the systematic review and assessed by the independent reviewers regarding their conformity with inclusion criteria (see Figure 1). The reviewer assessments matched in 80% of publications, resulting in a moderate inter-rater reliability (κ = .56; Altman, 1999). The independent reviewers were not blind to authors and journal of the assessed publications in either step. In cases of differing assessments, the publication in question was discussed until consensus was reached. In cases of publications examining the same sample, only the publication with most relevant data for the current systematic review was included into data synthesis.
Data Extraction and Synthesis
After reviewing the full-texts against the inclusion criteria, 15 studies were included into the systematic review. Using a structured table for data synthesis, two independent reviewers first extracted and coded relevant information for describing the studies included: country where the study was conducted, methodology (e.g. study design, data collection, control group, posttraumatic outcomes assessed), sample characteristics (e.g. size, age and gender distribution, trauma exposure), and intervention outcome. Next, the independent reviewers extracted and coded information about the school-based interventions described in the studies included: name and acronym, studies utilising the intervention (or a modification thereof), and intervention characteristics (e.g. primary goal, target population, type of intervention, implementation at school, duration, contents or components). In case of mixed-methods studies, only quantitative methods and data were extracted. If the information extracted from the studies differed between the first and second reviewer, a third reviewer was consulted. No authors of studies included were contacted for further information or data.
Methodological Quality Assessment
The methodological quality of the studies included was assessed by two independent reviewers using the Mixed Methods Appraisal Tool (MMAT; Hong et al., 2018).
The Mixed Methods Appraisal Tool
The MMAT (Hong et al., 2018) was developed for methodological quality assessment of empirical studies included in systematic reviews comprising different study designs. Overall, five types of study designs can be assessed using the MMAT: qualitative, quantitative randomised controlled trials (RCTs), quantitative non-randomised, quantitative descriptive and mixed methods. Methodological quality is assessed first using two screening questions (applicable to all study designs). If one or both screening questions are not met, further assessment ‘may not be feasible or appropriate’ (Hong et al., 2018, p. 2). Second, methodological quality is assessed with five quality criteria particular to each study design. Due to the current systematic review’s focus on intervention studies, quality criteria for only two relevant study designs (quantitative RCTs and quantitative non-randomised) were applied. For quantitative RCTs, following quality criteria were assessed: (1) ‘Is randomi[s]ation appropriately performed?’, (2) ‘Are the groups comparable at baseline?’, (3) ‘Are there complete outcome data?’, (4) ‘Are outcome assessors blinded to the intervention provided?’, and (5) ‘Did the participants adhere to the assigned intervention?’ (Hong et al., 2018, p. 2). For quantitative non-randomised studies, following quality criteria were assessed: (1) ‘Are the participants representative of the target population?’, (2) ‘Are measurements appropriate regarding both the outcome and intervention (or exposure)?’, (3) ‘Are there complete outcome data?’, (4) ‘Are the confounders accounted for in the design and analysis?’, and (5) ‘During the study period, is the intervention administered (or exposure occurred) as intended?’ (Hong et al., 2018, p. 2).
Methodological quality assessment procedure
The independent reviewers assessed the quality of included studies using first the screening questions for all study categories, and second the five quality criteria particular to each study design. In case of mixed-methods studies, only the quality of quantitative methodology was assessed. Disagreements in assessment were resolved through discussion. The screening questions and quality criteria were assessed as ‘met’, ‘not met’ or ‘not enough information available’, resulting in a global assessment of methodological quality (high, medium, low). Both screening questions had to be met; if one or more screening questions were assessed as ‘not met’ or ‘not enough information available’, the study quality was immediately judged as ‘low’, regardless of quality criteria assessment. After screening, the included studies’ methodological quality was further assessed using the five quality criteria, resulting in overall ratings of high (all quality criteria met), medium (3–4 quality criteria met) or low (0–2 quality criteria met) methodological quality.
Results
Methodological Quality Assessment of Studies Included in the Systematic Review Based on MMAT Criteria (k = 15).
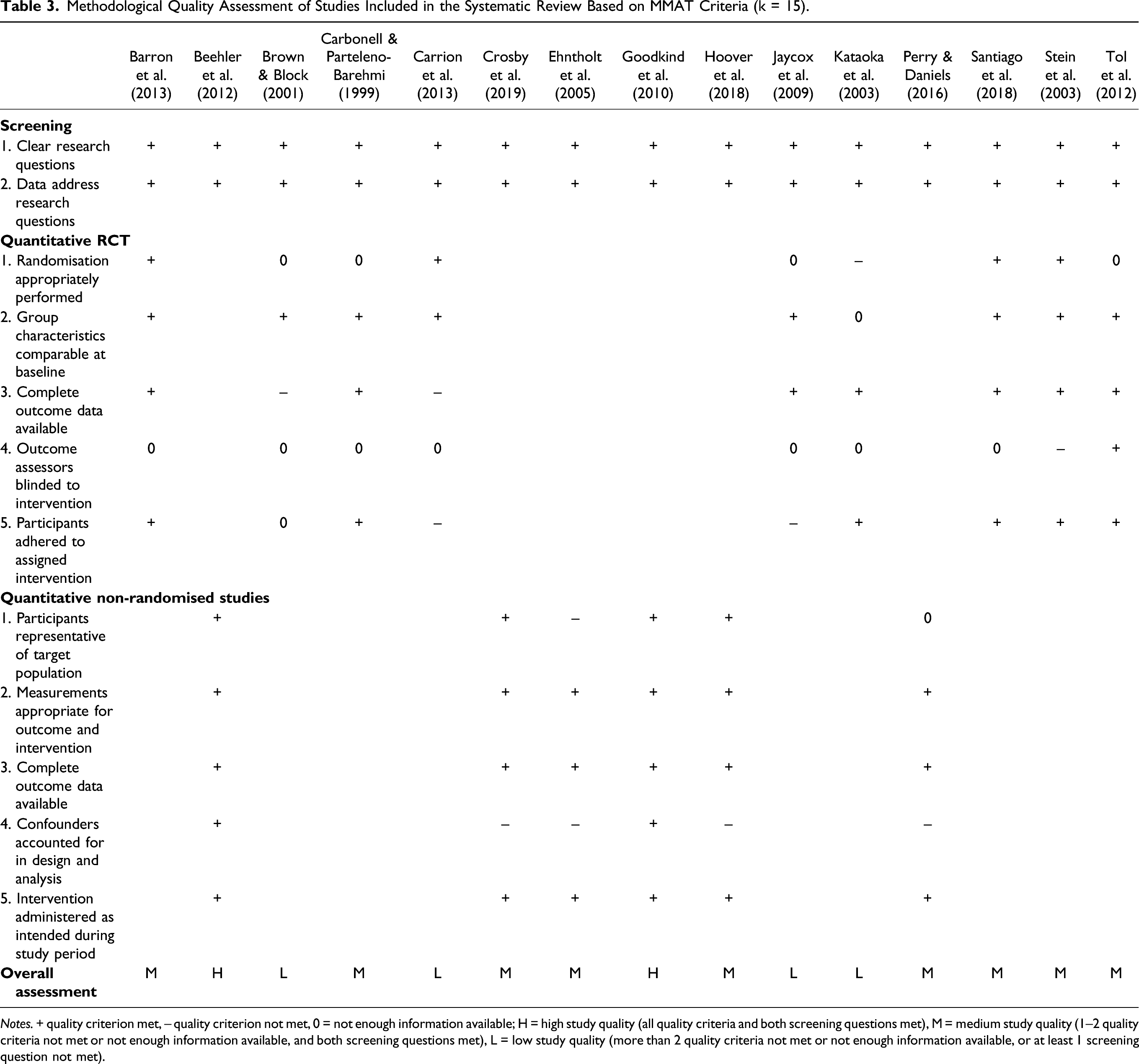
Notes. + quality criterion met, – quality criterion not met, 0 = not enough information available; H = high study quality (all quality criteria and both screening questions met), M = medium study quality (1–2 quality criteria not met or not enough information available, and both screening questions met), L = low study quality (more than 2 quality criteria not met or not enough information available, or at least 1 screening question not met).
Study Characteristics
Description of Studies Included in the Systematic Review (k = 15).
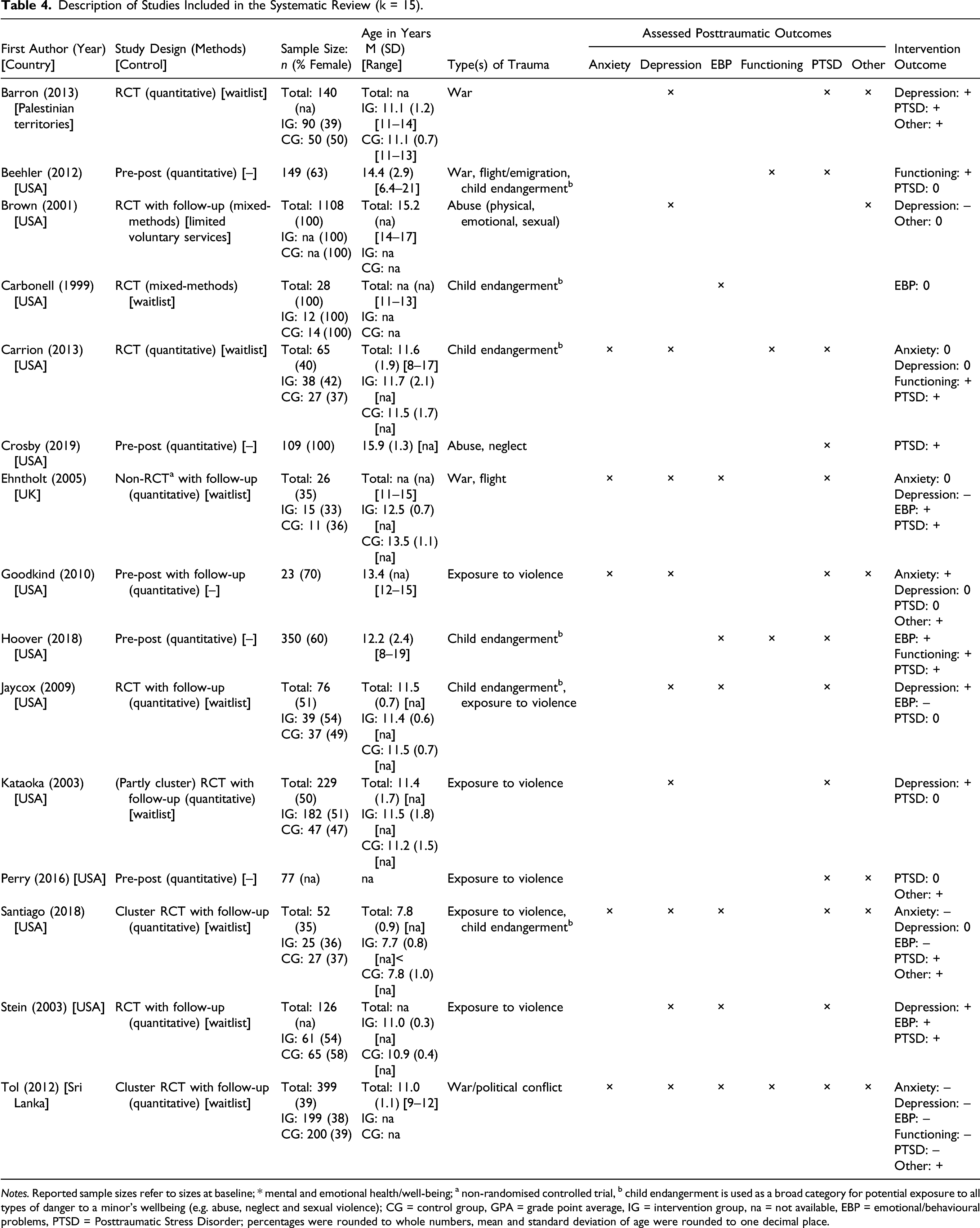
Notes. Reported sample sizes refer to sizes at baseline; * mental and emotional health/well-being; a non-randomised controlled trial, b child endangerment is used as a broad category for potential exposure to all types of danger to a minor’s wellbeing (e.g. abuse, neglect and sexual violence); CG = control group, GPA = grade point average, IG = intervention group, na = not available, EBP = emotional/behavioural problems, PTSD = Posttraumatic Stress Disorder; percentages were rounded to whole numbers, mean and standard deviation of age were rounded to one decimal place.
Sample Characteristics
Only counting intervention groups, sample sizes ranged from n = 12 to n = 350, with a total of n = 1369 children and adolescents receiving treatment interventions included across all studies (information available for k = 14 studies). The percentage of female intervention group participants ranged from 33% to 100% and was unknown for k = 1 study. Intervention group participants were on average 12.1 years old (information available for k = 11 studies). Only k = 4 studies reported age ranges for their intervention groups, resulting in an overall range of 6–21 years (see Table 4). The study samples included were generally exposed to violence (k = 6 studies) or child endangerment (k = 6 studies). Samples in k = 4 studies had experienced war and conflict in their countries of origin (Palestinian Territories, Barron et al., 2013; Sri Lanka, Tol et al., 2012) or were forced to flee or emigrate from their countries of origin (Beehler et al., 2012; Ehntholt et al., 2005) (see Table 4). The refugee samples were ethnically diverse, originating from five (Ehntholt et al., 2005) to nine (Beehler et al., 2012) different regions.
Assessed Posttraumatic Outcomes
Almost all studies assessed PTSD (k = 13) or depression (k = 10) as posttraumatic outcomes. Emotional or behavioural problems were assessed in k =7, anxiety in k = 5 and global functioning in k = 4 studies. In k = 6 studies, other posttraumatic outcomes (e.g. coping behaviour, substance use, grief, global mental health) were assessed. Furthermore, one study (Barron et al., 2013) assessed school performance as outcome (see Table 4). Instruments most frequently used to measure PTSD symptoms were the Childhood PTSD Symptom Scale (Foa, Treadwell, Johnson & Feeny, 2001) (k = 6) and the UCLA PTSD Reaction Index (Pynoos et al., 1998) (k = 4). Depression was mainly measured using the Children’s Depression Inventory (Kovacs, 1992) (k = 6) and the Depression Self-Rating Scale (Birleson, 1981) (k = 3). Self- and third-party-report versions of the Strengths and Difficulties Questionnaire (Goodman, 1997) were most frequently used to measure emotional and behavioural problems (k = 4).
Reported Intervention Outcomes
While not all implemented interventions significantly improved all posttraumatic outcomes, positive intervention effects (fully or partially significant, or approaching significance) were reported in the majority of included studies. For PTSD symptoms, 92% of relevant studies reported full (k = 7) or partial (k = 5) mitigation, while depressive symptoms were mitigated fully (k = 4) or partially (k = 3) in 70% of relevant studies. Emotional and behavioural problems and anxiety fully or partially improved in about 60% of relevant studies (k = 4 and k = 3, respectively). Functioning fully improved as a result of the implemented intervention in three of k = 4 relevant studies (see Table 4).
Description of Implemented Interventions
Description of Interventions Implemented in the Studies Included in the Systematic Review (k = 15).
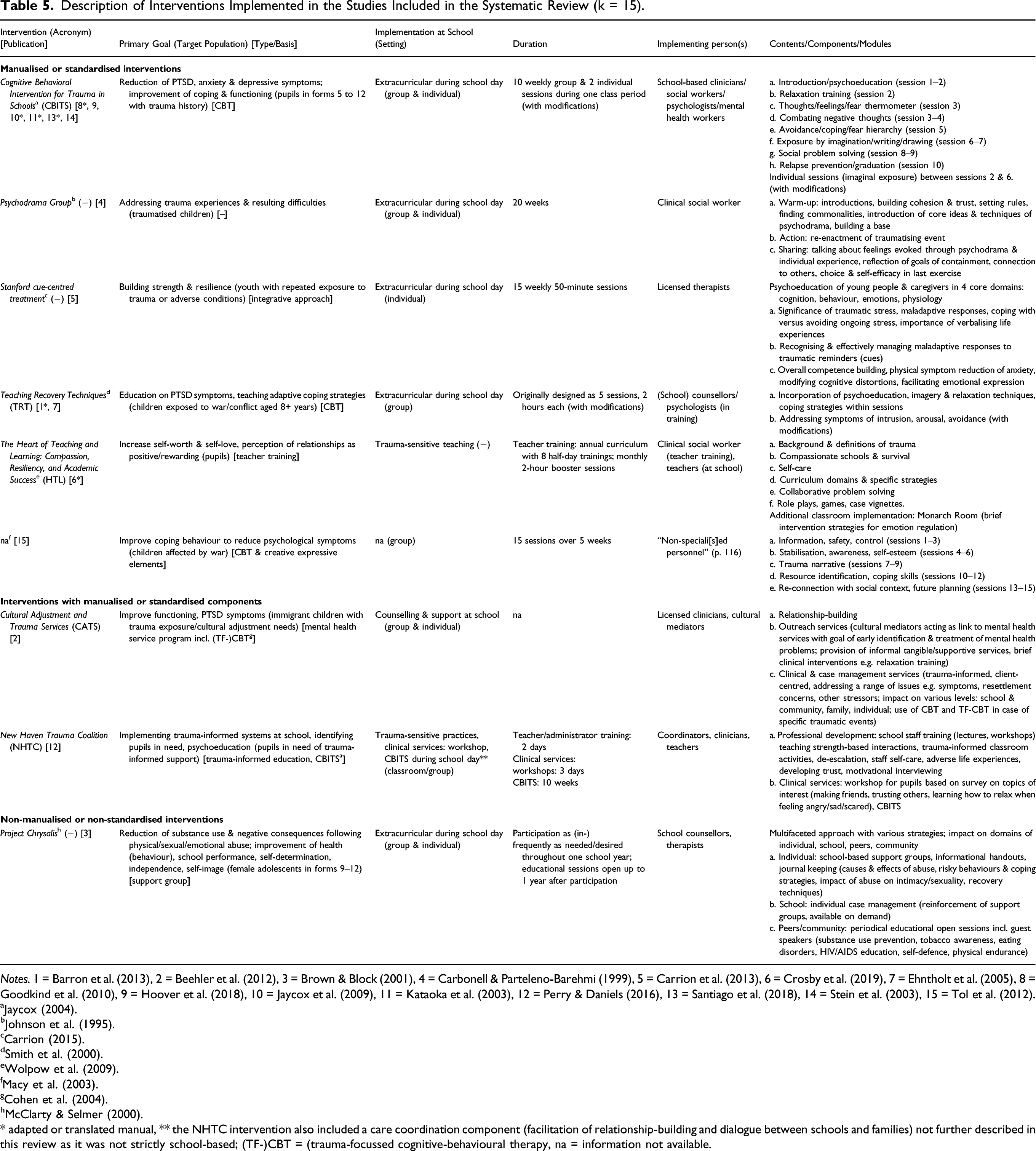
Notes. 1 = Barron et al. (2013), 2 = Beehler et al. (2012), 3 = Brown & Block (2001), 4 = Carbonell & Parteleno-Barehmi (1999), 5 = Carrion et al. (2013), 6 = Crosby et al. (2019), 7 = Ehntholt et al. (2005), 8 = Goodkind et al. (2010), 9 = Hoover et al. (2018), 10 = Jaycox et al. (2009), 11 = Kataoka et al. (2003), 12 = Perry & Daniels (2016), 13 = Santiago et al. (2018), 14 = Stein et al. (2003), 15 = Tol et al. (2012).
* adapted or translated manual, ** the NHTC intervention also included a care coordination component (facilitation of relationship-building and dialogue between schools and families) not further described in this review as it was not strictly school-based; (TF-)CBT = (trauma-focussed cognitive-behavioural therapy, na = information not available.
Overall, nine different interventions were implemented across all k = 15 studies. Almost all interventions had no gender restrictions, the only exception being Project Chrysalis (Brown & Block, 2001) which solely addressed females who had experienced physical, emotional or sexual abuse. Two further interventions however were implemented in all-female samples (Psychodrama Groups, Carbonell & Parteleno-Barehmi, 1999; HTL, Crosby et al., 2019). Of the k = 4 studies assessing war- and flight-related trauma, all implemented interventions specifically addressed war-related trauma or culture-sensitive needs, and k = 2 studies (Beehler et al., 2012; Ehntholt et al., 2005) implemented their interventions in ethnically diverse refugee or immigrant samples.
The majority of interventions was manualised or standardised (6/9) or integrated a manualised or standardised component (2/9); for a short description of the interventions see Table 5. In k = 6 studies, the authors implemented an adapted (e.g. according to local needs and resources) or translated version of a manualised intervention. Five interventions in k = 11 studies were based on (trauma-focussed) cognitive behavioural therapy (CBT) or used CBT-based components (see Table 5), of which k = 5 studies achieved complete mitigation of posttraumatic outcomes (see Table 4). The primary goals of the interventions implemented were largely building resilience and coping strategies (6/9), mitigation of posttraumatic symptoms and problems (e.g. PTSD, depression, anxiety, psychological distress) (5/9) and improving functioning (2/9). About half (i.e. five) of the interventions were implemented as extracurricular sessions during the school day (k = 11 studies), while one intervention consisted of counselling and support at school (Beehler et al., 2012) and another implemented trauma-sensitive teaching at school using teacher trainings (Crosby et al., 2019). One intervention described by Perry and Daniels (2016) implemented both trauma-sensitive practices within the school and extracurricular clinical services. Overall, four interventions (k = 9 studies) utilised group settings with individual components, three interventions (k = 4 studies) utilised pure group settings, and one intervention (k = 1 study; Carrion et al., 2013) offered purely individual treatment (see Table 5). The implemented interventions’ duration varied, with the number of sessions necessary ranging between 5 and 20. One intervention (Project Chrysalis; Brown & Block, 2001) allowed for pupils to participate as (in-)frequently as per their needs throughout one school year. The persons implementing the interventions across the included studies mainly comprised mental health professionals (e.g. clinicians, psychologists, counsellors, therapists). Five interventions described in k = 11 studies included school personnel in implementation, two of which utilising trauma-sensitive teaching and practices (Crosby et al., 2019; Perry & Daniels, 2016) were implemented by teachers within the school or had teachers participating in the implementation process (see Table 5).
Two interventions were implemented in more than one study: Teaching Recovery Techniques (TRT; Smith et al., 2000) (k = 2 studies) and Cognitive Behavioral Intervention for Trauma in Schools (CBITS; Jaycox, 2004) (k = 6 studies, with k = 1 further study utilising CBITS as an intervention component). One study implementing TRT each achieved full (Barron et al., 2013) or partial (Ehntholt et al., 2005) mitigation of posttraumatic outcomes (see Table 4). Three studies (Hoover et al., 2018; Kataoka et al., 2003; Perry & Daniels, 2016) implementing CBITS or using CBITS as an intervention component achieved complete mitigation of posttraumatic outcomes, while four studies achieved partial mitigation (Goodkind et al., 2010; L. H. Jaycox et al., 2009; Santiago et al., 2018; Stein et al., 2003) (see Table 4).
Discussion
The current systematic review aimed at identifying and describing school-based interventions designed to mitigate posttraumatic outcomes in children and adolescents after interpersonal violence. The results show that school-based interventions can be a beneficial approach in improving posttraumatic symptoms, especially PTSD, after complex interpersonal trauma, with all intervention studies described in this review achieving partial or full symptom mitigation for at least one posttraumatic outcome.
Discussion of Current Findings
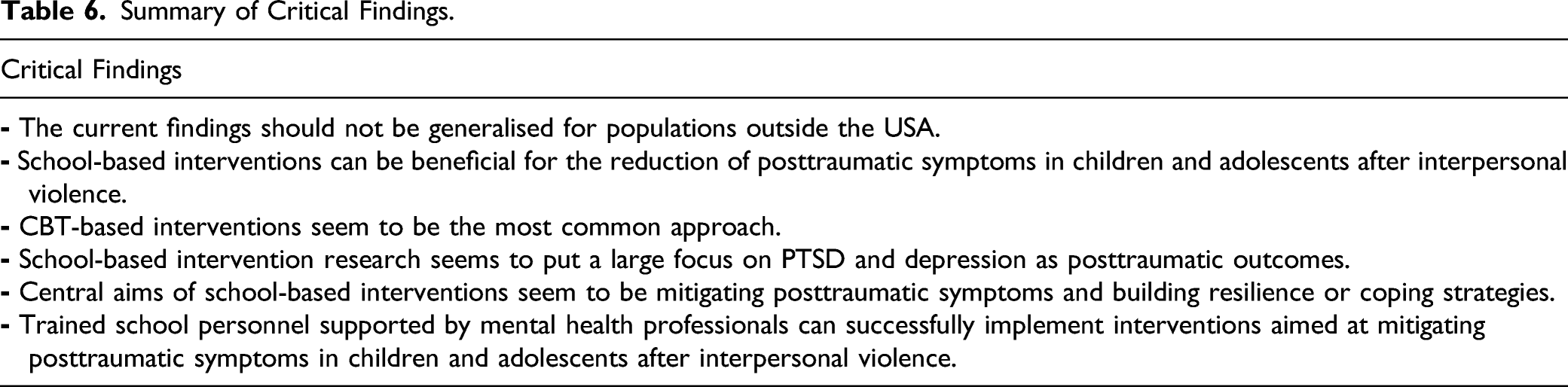
Summary of Critical Findings.
Diversity and generalisability
The current findings indicate that the interventions described in the included studies are gender-inclusive and able to address samples with diverse needs. As mentioned above, with the exception of Project Chrysalis (Brown & Block, 2001), no intervention had gender restrictions. Furthermore, there was a broad range of interpersonal trauma experiences in the samples assessed, with only two studies (Brown & Block, 2001; Crosby et al., 2019) focussing on specific types of interpersonal violence. Interventions addressing war- and flight-related trauma generally had culture- or war-sensitive content and were in part implemented in ethnically diverse samples (e.g. Beehler et al., 2012; Ehntholt et al., 2005). While these findings might seem to point to a broad applicability of the interventions described in the included studies, one factor limiting a generalisation of the current findings needs to be considered: consistent with previous findings (e.g. Yohannan & Carlson, 2019; Zakszeski et al., 2017) the overwhelming majority of research was based in the USA. Given the US-based Trauma and Learning Policy Initiative (TLPI), first introduced in 2005 and further developed into a framework for action in 2013 (Massachusetts Advocates for Children, MAC, 2009, 2013), this finding is not surprising. The TLPI is in its core a research-based project to reform and develop schools, introducing trauma-informed practices and teaching (MAC, 2009, 2013) and consequently impacting US-American policy, practice and research. While the USA has effectively become a pioneer in school-based trauma-informed practices and research, there is a dearth of school-based intervention research targeting consequences of complex interpersonal trauma in other parts of the world. As such, taking global differences in populations, mental health care services and school systems into account, the findings of the current review cannot be generalised for populations outside the USA.
Excluded studies
Overview of Retroactively Excluded Studies.
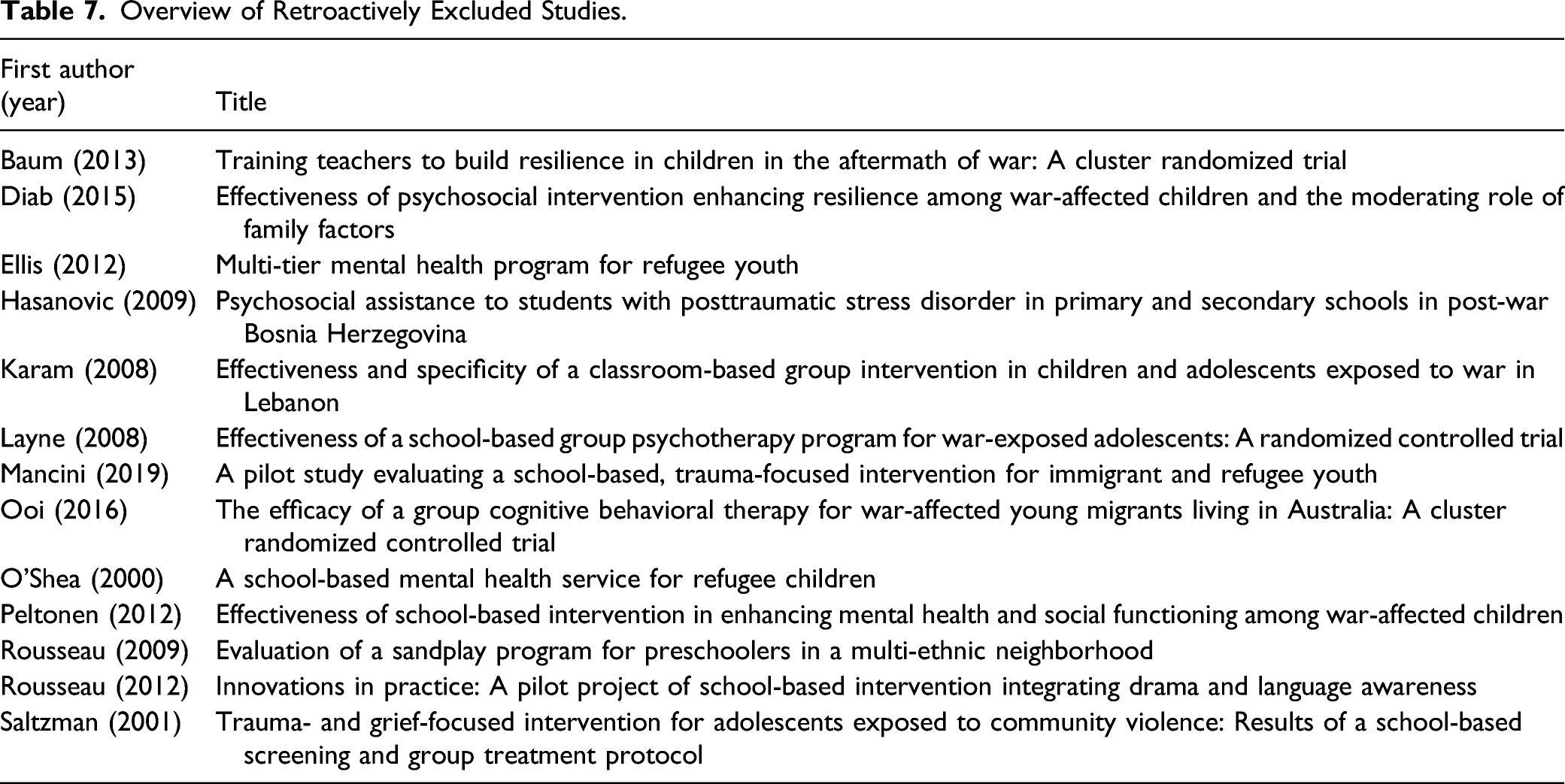
Unfortunately, although the strict selection criterion regarding trauma exposure provided clearer decisions and certainty that at least 50% of the assessed sample had experienced at least one type of interpersonal violence, the exclusion of these otherwise relevant studies also meant an omission of some important findings and a restriction of regional diversity in the current systematic review. More specifically, the excluded studies largely assessed war- and flight-related trauma (12/13) and were conducted in a range of different countries, that is, USA (3/13), Canada, Palestinian Territories and Bosnia and Herzegovina (2/13 each), as well as the UK, Australia, Israel and Lebanon (1/13 each), with English-speaking countries again dominating research (8/13). While, similar to the included studies, most excluded studies assessed PTSD (9/13) and depression (7/13) as posttraumatic outcomes, there were also a number focussing on emotional and behavioural problems (5/13). Regrettably, a large number of interventions implemented by teachers (7/13) had to be excluded, as well as all interventions incorporated into the school day (5/13) as opposed to extracurricular sessions. Furthermore, all studies achieving no mitigation of posttraumatic symptoms (4/13) were excluded.
Future research
Due to the current systematic review’s objective and resulting heterogeneity of studies as well as samples included into data extraction and synthesis, a meta-analysis was not feasible. As a result, no conclusions can be drawn regarding the actual effectiveness of school-based interventions for posttraumatic symptoms following interpersonal violence. As shown by the current systematic review, a strict criterion regarding (interpersonal) trauma exposure can moreover lead to the exclusion of a range of relevant intervention studies – in fact, trauma exposure was the criterion most studies were excluded by (see Figure 1). In situations where children and adolescents are exposed to war or community violence, however, interpersonal violence is rarely a singular event but rather goes hand in hand with a myriad of other potentially traumatic experiences. Additionally, in a heterogenous school or classroom setting, diverse experiences of the pupils targeted by the intervention are to be expected. As such, necessary meta-analyses on comparable school-based trauma interventions (e.g. manualised, CBT-based interventions or teacher trainings) could examine populations of children and adolescents who have experienced trauma globally related to war or flight (including e.g. bombings or shelling) or adverse childhood experiences as a whole (including e.g. incarceration or mental health problems of a parent, drug abuse at home), potentially creating more homogenous and comparable samples rather than including the samples based on experiences of interpersonal violence only.
Limitations
In addition to the aforementioned lack of generalisability of the current findings outside the USA, following limitations have to be considered when interpreting the results of this systematic review. First, the database search and selection process were limited to German and English language publications, quite possibly excluding relevant intervention studies in other languages from the current systematic review. Second, despite efforts to minimise publication bias and despite some intervention studies achieving no significant mitigation of posttraumatic outcomes being present in the retroactively excluded studies, a tendency to publish only ‘positive’ and significant results cannot be ruled out. While the current findings indicate benefits of school-based interventions for children and adolescents after complex interpersonal trauma, one should be careful not to overestimate this benefit. Third, while a majority of included studies implemented manualised or standardised interventions, modifications to the interventions were made in some cases according to the needs and local conditions in participating schools, making statements about the benefit of these manualised interventions in their intended form difficult or even impossible. Fourth, 40% of included studies used a single sample pre-post or non-randomised controlled study design, and about one third of RCT-studies did not include a follow-up assessment. Fifth, the comparability of included studies may be limited by the sample compositions themselves (e.g. age range very large or not reported, in part small sample sizes, varying gender proportions). Sixth, the tool used for assessment of methodological quality (MMAT, Hong et al., 2018) was developed with a clinical or medical focus. However, as none of the included studies were medical trials, their methods were not reported with the necessary detail, resulting in many assessments of ‘not enough information available’ especially with regards to RCTs. Consequently, study quality was rated as medium or low for most studies. We nonetheless chose to use the MMAT due to its capacity to assess methodological quality of different study types within the same systematic review. Last, as mentioned above, no meta-analysis was conducted in view of the current review’s objectives and resulting heterogeneity of included studies. However, a systematic review without meta-analysis can neither provide insight about the actual effectiveness of intervention studies nor compare the effectiveness of school-based interventions.
Strengths
Taking into account the limitations, the current systematic review also shows a number of strengths. Most of the included studies used a randomised-controlled design, almost all made an effort to implement manualised or standardised interventions or intervention components. The interventions were generally gender-inclusive and addressed populations with a broad range of interpersonal trauma experiences. The findings show not only a benefit of school-based interventions for a range of posttraumatic outcomes, but also that trained school staff is able to implement these interventions with support of mental health professionals. In summary, the current systematic review adds to existing research and knowledge about the possible benefit of school-based mental health interventions. Previous systematic reviews on school-based interventions had only assessed PTSD as posttraumatic outcome (Rolfsnes & Idsoe, 2011) or included all types of trauma, including non-interpersonal (Rolfsnes & Idsoe, 2011; Yohannan & Carlson, 2019; Zakszeski et al., 2017). Considering the broad range and severity of psychosocial and health consequences of interpersonal violence (e.g. Jimenez et al., 2016; Kien et al., 2018; Larson et al., 2017; Maercker, 2013; Norman et al., 2012), these findings imply not only that school-based interventions may be beneficial for the specific sample of children and adolescents exposed to interpersonal violence, but also that they can be used to address a range of posttraumatic outcomes following interpersonal violence.
Conclusions
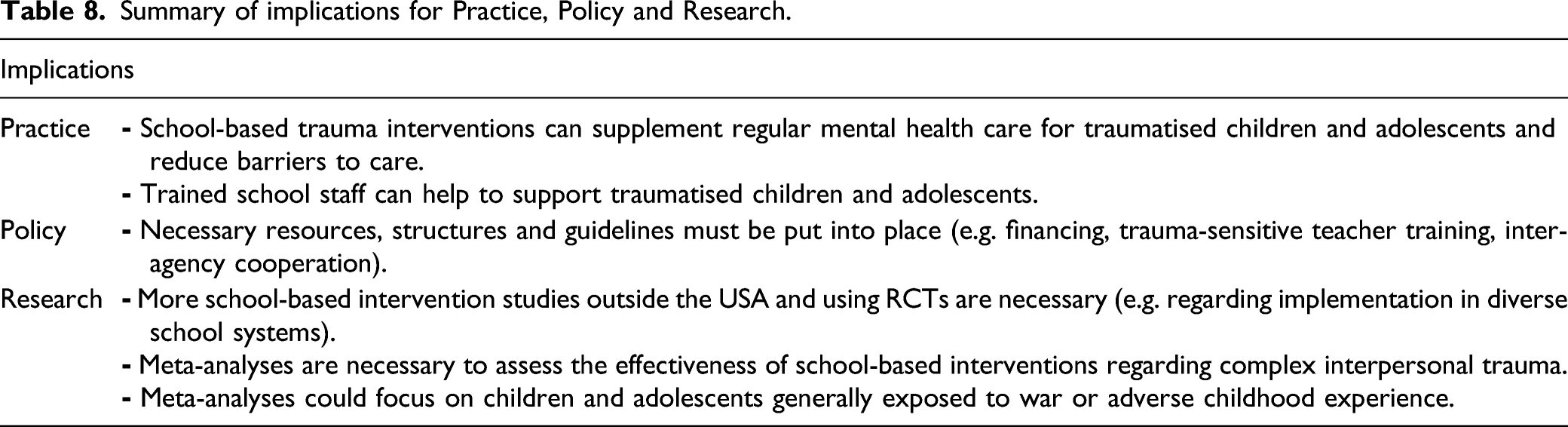
Summary of implications for Practice, Policy and Research.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.