
Abstract
Kinship care is a global phenomenon with a long history, which in high-income countries (HICs) at least, is being increasingly formalized through legislation and policy. There are many benefits to kinship care, including improved child mental health and well-being when compared to other types of out-of-home care. Despite this, kinship care is not without its risks with a lack of support and training for kinship carers putting children at an increased risk of abuse and neglect. This scoping review was conducted across 11 databases to explore the breadth and depth of the literature about abuse and neglect within kinship care in HICs and to provide initial indications about the relationship between kinship care and abuse. Of the 2,308 studies initially identified, 26 met the inclusion criteria. A majority of studies were from the United States, and most used case review methods. From the included studies, rates of re-abuse, and particularly rates of physical and sexual abuse, appear to be lower in kinship care settings when compared to other out-of-home care settings, but rates of neglect are often higher. This review has demonstrated that a small but significant number of children living in kinship care experience neglect or abuse.
Kinship care, the practice of children living with extended family, has long been practiced across cultures (Delap & Mann, 2019). These arrangements can be informal but many countries now have legal frameworks for kinship care. In the UK, for example, special guardianship orders (SGOs) came into effect in 2002 as an alternative to adoption (Harwin & Simmons, 2019). Children subject to SGOs are placed with legal guardians with whom there are existing relationships, such as a foster carers or relatives. Guardians gain parental responsibility and children are no longer the responsibility of local authorities. There are, however, concerns that children may in some cases be subject to an SGO without proper consideration of the long-term stability of the placement (Webb & Douglas, 2017). The Kinship Care and Fictive Kin Reform Act in the United States gives state foster care programs the right to place children with relatives (kinship) or others who are not related but have a significant relationship with the child (fictive; American Legislative Exchange Council, 2017). While kinship care arrangements in many Western countries are regulated, most kinship care in Africa is arranged informally, remaining unregulated by authorities (Assim, 2013).
Globally, 1 in 10 children lives without their biological parents, most of them living with relatives (Martin & Zulaika, 2016). However, rates vary significantly between regions and countries. In South Africa, around 1 in 10 children are cared for by relatives (De Wet, 2019), compared with 1 in 74 in the UK (Wijedasa, 2015). In Australia, almost half of all children recorded in out-of-home care were living in formal kinship care (Australian Institute of Health and Welfare, 2016). In 2014 around one third of children in foster care were living with relatives in the United States (Children’s Bureau, 2015).
Rates of kinship care are increasing globally and the reasons for this are complex. In their report, Delap and Mann (2019) identify seven interconnected factors that explain the continued and growing use of kinship care: poverty; lack of access to services; parental ill health and death; migration, emigration, and national immigration policies; disasters and conflict; cultural beliefs; and child protection policy response. The influence of these factors can vary, especially between high-income countries (HICs), and low- and middle-income countries (LMICs). In HICs, formal kinship care is usually a response to child protection issues, significantly more so than in lower income countries. Policy decisions in the industrialized world have, over the last two decades, prioritized kinship care over other out-of-home care (Connolly et al., 2017). This has partly been in response to shortcomings in residential and foster care settings, but also, especially in the United States, Australia and New Zealand, to provide appropriate care for black and minority ethnic or indigenous groups (Boetto, 2010; Fernandez & Atwool, 2013; Rufa & Fowler, 2016).
There are many benefits to kinship care, especially for children who have experienced abuse, neglect, parental drug and alcohol misuse, parental incarceration or domestic violence, circumstances more likely to be the reason for kinship care in HICs than LMICs. International evidence suggests that kinship care offers greater placement stability than nonrelative foster care (Brown et al., 2019). Children in nonrelative foster care are more likely to be adopted than children in kinship care, but the reverse is true for guardianship (Winokur et al., 2018). Furthermore, child mental health and well-being are significantly better in kinship care than in nonrelative foster care (Winokur et al., 2018). It may be that the familiarity of family and culture allows children to adjust to a different care setting more readily (O’Brien, 2012); indeed, children identify care by relatives as preferable (Save the Children UK, 2015).
Despite the increasing use of kinship care and the many benefits that it affords, it is often neglected by policymakers and practitioners. Kinship care frequently receives less support than other types of care. In many countries, kinship carers receive no, or only limited financial support, and significantly less than nonrelative foster carers (Nandy & Selwyn, 2013; Zuchowski et al., 2019). The issues raised by lack of support are manifold. Lack of support, financial or other, can increase carer stress, which in turn may lead to negative outcomes for children, potentially risking their safety. Both lack of support and stress are known risk factors for child abuse, as is a lack of understanding about children’s needs (Runyan et al., 2002). Kinship carers often do not receive the training and support they need to be able to care for the children (Selwyn et al., 2013). Alongside the lack of support, there is also a lack of oversight of kinship care placements, which raises concerns for the welfare of children (Save the Children UK, 2015).
Kinship care has been a neglected area of research (Delap & Mann, 2019) but is gradually receiving more attention as illustrated by the expanding number of literature reviews, for example, on special guardianship in England, and services (Lin, 2014) and interventions (Kinsey & Schlösser, 2012) for kinship care families. We have identified only one review that specifically explores safety in kinship care (Winokur et al., 2018), in which only four studies were identified. From our knowledge of the topic, we know there is a greater, if still somewhat sparse literature on safety in kinship care and we, therefore, conducted a scoping review to identify the literature that explores and identifies the risks of child abuse/child protection issues for children and young people in kinship care. Due to the differences in causes and experiences of, and policy responses to kinship care between HICs and LMICs, the focus of this review is HICs.
Method
We conducted a scoping review of the literature on the prevalence and experiences of child protection/abuse issues for children and young people in kinship care. Scoping reviews have been increasing within the health and social science care literature over the past 20 years. The first methodological guidelines were published in 2005 (Arksey & O’Malley) and have been updated by various authors (e.g., Levac et al., 2010). They differ from systematic reviews in their purpose, which is to identify and map the literature on a topic, rather than to answer questions of effectiveness (Munn et al., 2018). While scoping reviews can be used to determine the value of a systematic review, they can also be undertaken as standalone exercises (Peters et al., 2015). In line with scoping review indications (Munn et al., 2018), this review method was chosen to enable us to examine the design and conduct of research in this area, to explore the breadth and depth of the literature on this topic, and to provide initial indications about the relationship between kinship care and abuse. The Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR; Tricco et al., 2018) checklist was followed in reporting this review.
Search Strategy
We conducted an initial exploratory exercise in April 2020 to develop the review objectives, search terms and inclusion/exclusion criteria, using the Population, Experience, Outcomes (PEO) framework: child or young person under the age of 18 (population), formally or informally living in kinship care (experience), child protection/safeguarding/abuse (outcomes). Using the process described by Arksey and O’Malley (2005), we developed the search terms and inclusion criteria in an iterative process, revisiting searches until we were satisfied that the searches were broad enough to capture the literature relevant to our objectives while not so broad as to become unmanageable. From this exercise, it became evident that we did not need search terms relating to the population, because this was implied by the experience, that is, people living in kinship care are by their very nature under the age of 18.
We conducted searches of 11 databases: ASSIA, Embase, Medline, Web of Science Core Collection, Cinahl, PsycINFO, Scopus, Google Scholar, Ethos, OpenGrey, Proquest Dissertations & Theses between April and May 2020. Two sets of search terms were used relating to the experience and outcomes, see Table 1. Results were limited to English-language only; no date restrictions were set. To supplement the database searching, forward and backward chain searching was conducted to identify further papers, a process involving identifying papers that cite included studies and searching the reference lists of included studies. Relevant research identified in the course of our academic and clinical work was also added.
Search Terms (Combined With AND/OR).

Selection of Sources
A two-stage process of paper selection was undertaken, comprising a review of titles and abstracts, then full-text papers, the same process as a systematic review. All references were exported into Rayyan, an online tool for screening and selecting studies in a review (Ouzzani et al., 2016) to allow independent screening and decision-making. Title and abstract screening was conducted by two independent reviewers (all authors), reviewing against the inclusion and exclusion criteria detailed in Table 2.
Inclusion Criteria.

Data Charting Process
Data from all included studies were charted using a data extraction framework. The framework was pilot tested by two authors with five papers to ensure consistency and minor changes were made. The following data were charted where available: citation, aim, study design, study characteristics and methods (country, data collection, data analysis), participants (including characteristics and sample size) and findings relating to the aim of the review.
Summarizing the Results
Descriptive statistics were used to group study characteristics, and methodological and population data. Due to the heterogeneity of the findings meta-analysis was not possible therefore the “synthesis without meta-analysis” (SWiM) framework was followed (Campbell et al., 2020). Studies were first grouped by outcome (e.g., type of abuse, investigated/substantiated maltreatment). As this is a scoping review with no attempt to summarize effect estimates, we looked for any evidence of the effect of kinship care on rates of abuse/child protection concerns by using vote counting based on the direction of the effect. Data were extracted according to findings relating to the aim of the review, identifying studies that compared kinship care with other care settings, comparison between formal and informal kinship care, studies that identified rates of neglect, abuse, maltreatment recurrence and investigated/substantiated allegations, perpetrator and other. For studies that compared kinship care with other care settings, we identified whether rates of abuse were higher or lower in kinship care. For studies without comparisons, or studies that reported data other than rates, we provide a narrative synthesis of the results.
Due to the heterogeneity of the methods studies were scored 1–3 on their usefulness (1. very little of relevance to the research question; 2. some useful information about abuse in kinship care, but not directly relevant; 3. extremely useful and directly relevant to the research question, providing insight into abuse in kinship care.) and quality (1. did not satisfy basic criteria of rigor, or were flawed in some other way, or bias had not been addressed; 2. satisfied with the overall design and methods, and attempts to address bias had been taken, or at the very least, acknowledged; 3. the research was rigorously designed and undertaken, and potential bias had been addressed; Taylor et al., 2012). Studies that scored 1 for either usefulness or rigor were discussed between the authors to decide whether to include or not. Decisions are detailed in the results.
Results
Overview
From 2,302 papers identified in database searching and six records identified from other sources, 26 papers were identified as meeting the inclusion criteria (Figure 1). As shown in Table 3 papers were published between 1996 and 2020 at a rate of 0–2 per year. Most papers (n = 18) came from the United States; four were from the UK/England; one was from each of Australia, Canada, and New Zealand; and one was an international review.
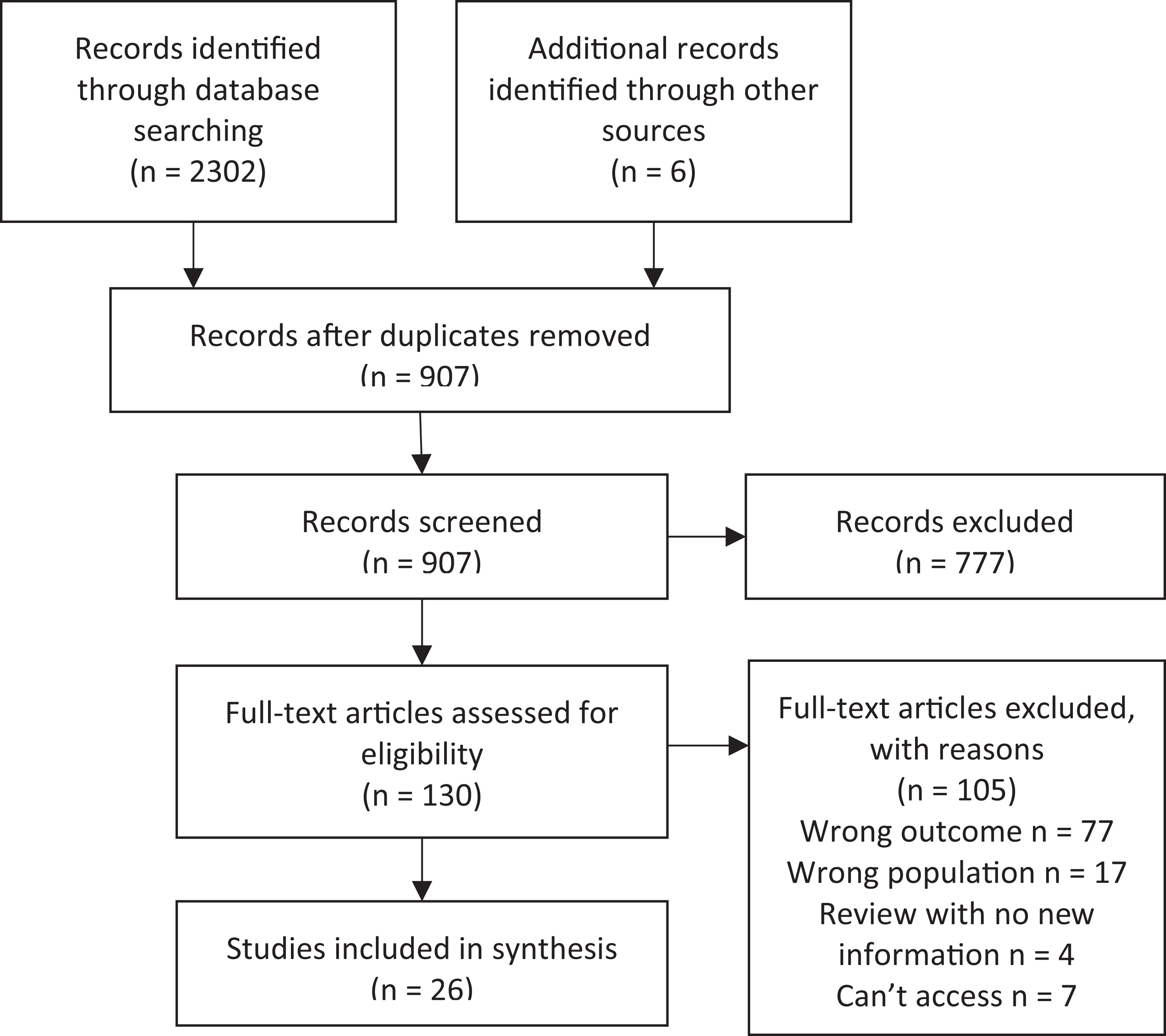
Flowchart of study selection.
Study Characteristics.
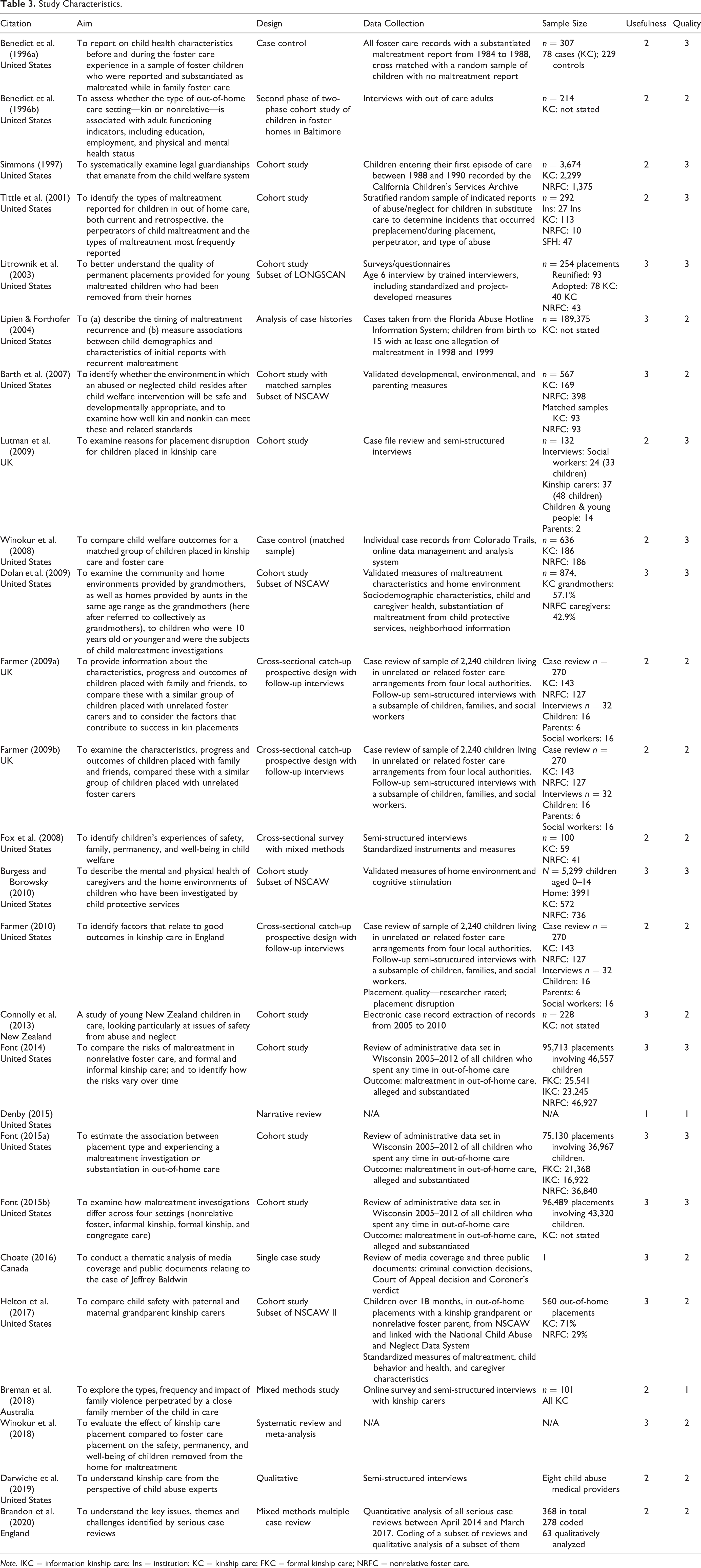
Note. IKC = information kinship care; Ins = institution; KC = kinship care; FKC = formal kinship care; NRFC = nonrelative foster care.
Study Characteristics
Most studies either used case files (n = 9) or databases (n = 11) to extract data. Of the databases, six used administrative databases, three used the National Survey of Child and Adolescent Well-Being (NSCAW) database (Barth et al., 2007; Burgess & Borowsky, 2010; Dolan et al., 2009), one used NSCAW II (Helton et al., 2017) and one used the Longitudinal Studies of Child Abuse and Neglect (LONGSCAN) database (Litrownik et al., 2003). NSCAW is a longitudinal survey of children and families who have been in protective services in the United States, which began collecting data in 1997 and is onto its third cohort. LONGSCAN is a consortium of longitudinal studies of children and their families, conducted at five different sites, with children under the age of four being followed until the age of 18. Data collection began in 1991 and ended in 2012. One study was a 10-year cohort study with children in two local authorities who were placed with extended family or friendship networks (Lutman et al., 2009), which supplemented a case file review with interviews of social workers, kinship carers, children and young people, and parents.
One study provided a mixed-method analysis of all serious cases reviews (SCRs) in England over a 3-year period (Brandon et al., 2020). SCRs are conducted by multiagency bodies within local authorities when a child is seriously harmed or has died, there is suspected abuse or neglect, and there is concern about authority or professional safeguarding. One study used a single case design to explore a child’s death at the hands of his grandparents (Choate, 2016). Four studies utilized cross-sectional methods; of these three were based on a single data set (Farmer, 2009a, 2009b, 2010). One study interviewed child abuse medical providers about their experiences of the kinship care system (Darwiche et al., 2019). The final study was a systematic review and meta-analysis of the effects of kinship care on safety, permanency, and well-being outcomes (Winokur et al., 2018).
A majority of studies contained findings that were either useful (n = 9) or extremely useful (n = 9) to the aim of the review. Two studies included in this review did not satisfy the basic criteria of rigor. Breman et al. (2018) provided scant details of their methods but were included in the analysis due to the usefulness of the findings. Denby (2015), who also scored 1 for usefulness, only provided a figure for child maltreatment recurrence but with no information about the source of the figure, therefore it was excluded from further analysis.
Data Extraction
Most studies provided a kin/nonkin comparison (n = 17) and/or kinship care rates (n = 14) of neglect, abuse, maltreatment, or investigated/substantiated allegations. Comparators included nonrelative or family foster care, specialized care and institutions. Only four studies provided a comparison between different types of kinship care settings, and six explored the perpetrator. The “other” categories were oversight and support, parenting styles and discipline, length of the placement and impact of violence.
Neglect
Rates of neglect, are consistently higher in kinship care settings when compared with other settings (nonrelative foster care, specialized foster care, institutions), in the United States at least (Burgess & Borowsky, 2010; Font, 2015b; Simmons, 1997; Tittle et al., 2001). Apart from according to one study, which found no neglect in children in kinship care, with all identified cases of neglect being in nonrelative foster care (Benedict et al., 1996a). Rates in informal kinship care may be higher than in formal kinship (Font, 2015b). We identified only one study exploring this outside the United States, which found 6% of children had experienced neglect in the 3 years following a special guardianship placement (Harwin et al., 2019).
Physical and Sexual Abuse
Most studies found that rates of physical abuse were lower in kinship care than in other settings (Benedict et al., 1996b; Burgess & Borowsky, 2010; Font, 2015b; Simmons, 1997; Tittle et al., 2001). However, one study, which asked young people if “grownups or other kids hit, push, or throw things at kids in this home” found no difference in responses from young people in kinship and nonrelative foster care (Fox et al., 2008, p. 72). Another study found higher rates of physical abuse in kinship care when compared with rates in nonrelative foster care (Litrownik et al., 2003). Rates of sexual abuse were frequently lower in kinship care than in other settings (Font, 2015b; Simmons, 1997; Tittle et al., 2001). However, Burgess and Borowsky (2010) and Barth et al. (2007) found no difference in rates between kinship and nonrelative foster care.
Other Types of Abuse
Studies suggest that there is little difference in rates of emotional or psychological abuse between settings (Burgess & Borowsky, 2010; Font, 2015b; Litrownik et al., 2003). However, children were more likely to respond in the affirmative to the statement “people in this home say mean things to me” in nonrelative foster care than in kinship care (Fox et al., 2008, p. 72). There appears to be little difference in rates of witnessed violence between nonrelative foster and kinship care (Fox et al., 2008; Litrownik et al., 2003).
Risk of Maltreatment Recurrence
Recurrence of maltreatment, that is, incidents occurring with children who had previously experienced maltreatment, tended to be lower in kinship care settings. When young people were followed up, recurrence of maltreatment or abuse was less likely in kinship care in families who received no services; risk of recurrence was highest for those who received in-home services (Lipien & Forthofer, 2004), and significantly less likely when comparing kinship care with nonrelative foster care (Winokur et al., 2008). Furthermore, in their meta-analysis of three papers, Winokur et al. (2018) found that children in nonrelative foster care had 3.7 times the odds of experiencing re-abuse than those in kinship care. However, Benedict et al. (1996a) found no difference in substantiated maltreatment between kinship and nonrelative foster care. Moreover, although few further safety issues were identified for children who had a child protection referral in New Zealand over a 5-year period, of the 48 children followed up in kinship care, four (12%) experienced substantiated maltreatment in a care setting compared with one (4%) of the other 352 who either remained with parents or were moved to family foster care (Connolly et al., 2013).
Type of Kinship Care
Few studies compared formal and informal kinship care settings. Font (2014) found that the lifetime risk of a substantiated claim against a caregiver perpetrator was significantly higher in informal kinship care than in either formal kinship or nonrelative foster care. Investigated claims of neglect were highest in informal kinship care followed by formal kinship care whereas investigated claims of physical abuse were lowest in informal kinship care (Font, 2015a). Conversely, Winokur et al. (2008) found that allegations of abuse or neglect were significantly higher (18.5% compared with 2.2%) in paid than unpaid kinship care.
Perpetrator
Of the studies that identified the perpetrator of abuse both investigated and substantiated, the out-of-home caregiver, that is, the kinship or nonrelative foster carer, was the most likely perpetrator (Font, 2015a, 2015b; Tittle et al., 2001). Peers accounted for a small number of the perpetrators and were more likely in nonrelative foster care than kinship care (Font, 2015b). Children and young people placed with maternal grandparents were less likely to be involved in maltreatment investigations than those placed with paternal grandparents (Helton et al., 2017). However, Choate (2016) explored what could be learnt from a Canadian perspective by exploring the case of Jeffrey Baldwin, who died aged five while in the care of his grandparents, who were convicted of second-degree murder. This case highlights the potential for cycles of abuse in kinship care. Jeffrey’s grandmother was raised by an alcoholic father and left school young to help raise her siblings (Choate, 2016). Jeffrey’s mother had all her children removed to the care of her parents. While in his grandmother’s care Jeffrey was “starved to death over a prolonged period” (Choate, 2016, p. 24).
A small but significant minority of children in kinship care not protected from abusive birth parents (Farmer, 2009b) and birth parents were more likely to be the perpetrator in kinship care than in other care settings (Tittle et al., 2001). Furthermore, difficult relationships between carers and birth family were higher in kinship care than nonrelative foster care (Farmer, 2009b). In a survey of 101 kinship carers, over half (51%) had experienced physical violence, psychological, verbal, or emotional abuse, or property damage since the start of the placement, perpetrated by a family member (Breman et al., 2018). The main perpetrators were the child’s mother (68%), the child (46%) and the child’s father (26%). Most of the violence was directed toward the carer (91%), but 68% was toward the child; many incidents had multiple victims.
Oversight and Support
From the few studies we identified, it appears that there is little oversight or support for kinship carers. In a majority (over two thirds) of the qualitatively analyzed SCRs in England, at least one child had lived with or been looked after by a relative (Brandon et al., 2020). The cases reviewed demonstrated a lack of assessment and support for kinship carers, and further, that professionals are often unaware of the support provided by friends and family to vulnerable children. Child abuse medical providers, when interviewed, believed that because kinship caregivers do not receive training to work with traumatized children they are more likely to beat the children in their care than other out of home carers (Darwiche et al., 2019).
Parenting Styles/Discipline
The evidence about parenting styles was inconclusive. Four studies explored parenting styles, behaviors and discipline with mixed results. Two studies found no difference between kinship care and other settings for harsh or severe parenting (Barth et al., 2007) and shouting when angry (Fox et al., 2008). However, caregiver slapping was witnessed more in kinship care than in other settings (Dolan et al., 2009). The caregiver, the child’s grandmother, of one child living in kinship care in New Zealand was given support with parenting skills to avoid inappropriate discipline (Connolly et al., 2013).
Length of Placements
The most risky time for young people is at the beginning of kinship care placements, and problematic kinship care placements may last longer than other care placements. The risk of a maltreatment investigation appears to be greatest in the first 3 months of placement, but this risk is significantly higher in nonrelative foster care than kinship care (Font, 2015b). However, even where there was no difference in the number of problem placements between kinship and nonrelative foster care (Farmer, 2009a), problematic kinship care placements were more likely to last for longer (Farmer, 2010). In 13% (n = 4) of disrupted kinship care placements in the UK, the main reason was cited as alleged or substantiated abuse or neglect (Lutman et al., 2009).
Impact of Violence
Only one study explored the impact of violence on children in kinship care. Breman et al. (2018) found that children who experienced or witnessed violence perpetrated by family members, often their mother, experienced stress and anxiety, psychological problems, behavioral issues, becoming clingy, difficulty sleeping, problems at school and a reluctance to see their parents, all directly related to the violence.
Discussion
As demonstrated by the limited research found for this review, especially outside of the United States, the literature on the risk of abuse and child protection issues within kinship care is sparse. The findings of this review suggest that while rates of re-abuse, and particularly rates of physical and sexual abuse, appear to be lower in kinship care setting when compared to other out-of-home care settings, rates of neglect are often higher. This review has demonstrated that a small but significant number of children living in kinship care experience neglect or abuse.
One of the great benefits of kinship care, the continuity of family, can also become a significant risk factor. In HICs, as included in this review, kinship care is often used as a response to child protection concerns. While for most children, remaining within the family produces positive outcomes in terms of education and well-being (Harwin & Simmons, 2019), a significant minority may be caught in a cycle of abuse, as suggested by our review at least. In some families, children whose parents have a history of neglect or abuse are at an increased risk of maltreatment (Jaffee et al., 2013). In families where the cycle of abuse has continued for generations, there is a risk that children with abusive or neglectful parents will be placed with abusive or neglectful grandparents.
Parental contact can be important for children living in care but can introduce protective issues (Kiraly & Humphreys, 2015). Our review suggests that birth parents are more likely to perpetrate abuse toward children in kinship care than in other settings. Complex family relationships can further exacerbate problems. Not only are children potentially at greater risk of contact with abusive parents in kinship care, but this review has found some evidence to suggest that carers may also be at increased risk.
Several studies in this review found that problematic kinship care placements were likely to last longer than placements in other care settings, possibly because reduced oversite means that problems are not picked up as quickly; placements where kin carers are approved as foster carers appear to have fewer rates of disruption than those where they are not approved (Farmer, 2010). Literature from the United States and UK suggests that kinship carers have less monitoring than other carers and that they also have reduced levels of training and support, both financial and practical (Harwin & Simmons, 2019). This can cause an extra burden on carers, who often have to support children with substantial trauma histories. This might also account for the higher rates of neglect during informal compared with formal kinship care placements; informal carers likely receive even less support than formal carers (Selwyn et al., 2013). In the UK, kinship carers are not automatically entitled to financial support, compared with foster carers (Selwyn & Nandy, 2014). In the United States, however, some states provide payments to support children placed with relatives (Children’s Bureau, 2016). Few studies explored the difference between paid and unpaid kinship care, but some carers may be motivated by financial gain.
In HICs, policy decisions have prioritized kinship care in child protection proceedings (Delap & Mann, 2019). This has been driven by concerns about shortcomings of nonfamilial out of home care, an increased demand for care accompanied by a decrease in carers, economic benefits, and beliefs about the value of family-based care (Delap & Mann, 2019; McCartan et al., 2018). This final aim may in some circumstances have a paradoxical effect. Some have argued that the conflict between keeping a child safe from harm and maintaining family bonds skewed by a moral imperative to keep the child with the family (Featherstone et al., 2014). This has been described as leading to a view where child and family social workers operate a hierarchy of family forms; where a mother–infant dyad cannot be realized, then close kinship care is next in line even if there may be a risk of abuse (Morris et al., 2017).
Limitations
While this review gives a broad picture of the relationship between kinship care and risk of abuse, neglect, and maltreatment in the United States, little is known on this topic elsewhere. Globally, kinship carers tend to be female, and usually maternal relatives. In the United States, rates of kinship care increased significantly as a result of the crack cocaine epidemic in the 1980s (Sykes et al., 2002), making the United States in some ways unique. Reasons for kinship care and the demographics of kinship carer populations vary between countries, even when comparing HICs. There is substantial variation of kinship carers even within the countries of the UK; in England, black-African boys and Chinese and Asian children are overrepresented in kinship care, while in Wales, no kinship carers identify as anything other than white (Selwyn & Nandy, 2014).
There are some significant gaps in the literature. There was not enough detail in the studies under review to provide any analysis of child protection risks by ethnicity. We know that black and minority ethnic children, and indigenous children are overrepresented in kinship care settings. What we do not know is whether the benefits that connection to culture, family and community provided by kinship care, which may be especially important for these children, outweigh the risks of further safeguarding issues in these settings.
Formal kinship care, in the form of SGOs, was introduced as an alternative to adoption in England and Wales. It is therefore surprising that none of the studies has compared rates of abuse in kinship care settings to rates among children who are adopted. We posit that the rates would be significantly higher in kinship care due to the comprehensive assessments of prospective adoptive parents. This supposition is supported by clinical experience rather than empirical evidence, and further research is needed to explore this claim.
Conclusion
This scoping review has identified that in HICs, while risks of abuse appear to be lower in kinship care than in other out-of-home care settings, the risk of neglect may be higher, and that a small but significant number of children in kinship care do experience abuse, which may go on for longer before being identified. These risks may differ between formal/informal and paid/unpaid kinship care placements but this needs further investigation. The lack of training and support that is given to kinship carers is likely to exacerbate the risks to some children. With the increasing use of kinship care across many countries, and the enthusiasm of policymakers for kinship care over other out-of-home care, further investigation is needed to not only identify the risks to children but also the efficacy of interventions to ameliorate those risks.
Implications for Practice, Policy, and Research
Practice
Initiate robust monitoring records that identify children in kinship care who experience safeguarding issues, to include information about ethnicity.
Professionals working with children in kinship care families should consider offering additional support as children may continue to be at risk of neglect or further abuse.
Policy
Open the debate regarding financial reimbursement for kinship carers in line with foster carers.
Research
Research or review is needed in low- and middle-income countries to identify the abuse and neglect risks for children in kinship care, and the subsequent implications for practice.
Research into the relationship between kinship care, safety risks and ethnicity.
Greater exploration of the relationship between levels of support and training for kinship carers and the risks to child safety, examining formal and informal care settings, particularly outside of the United States.
Research into the relationship between financial reimbursement for kinship carers and risk of abuse.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.