
Abstract
Childhood exposure to domestic violence (DV) can lead to mental health problems including internalizing symptoms. This systematic literature review aimed to identify individual-, familial-, and community-level factors that mediate or modify the effect of DV exposure on internalizing symptoms among children and adolescents. This systematic literature review was registered with PROSPERO, registration number: CRD42019127012. MEDLINE, EMBASE, and PsycINFO were searched between 1990 and 2018 for peer-reviewed, quantitative, longitudinal studies published in English. Backreferencing and key journal hand searches were conducted. Twelve longitudinal studies were included. These investigated how factors amenable to change either mediate or modify the effect of exposure to DV on internalizing symptoms (using validated measures) in children and adolescents up to 18 years within a general population. Study quality was assessed using the Newcastle–Ottawa risk of bias tool, and a sample of studies were second reviewed by authors. One individual-level mediator was identified, namely emotional intelligence, and two effect modifiers were identified: relational victimization and participation in extracurricular activities. Familial mediators included maladaptive parenting and parenting stress, while effect modifiers included positive parenting (maternal warmth and availability) and family social support. No community-level factors were identified. All research was conducted in the United States, most focused on risk, and the majority measured outcomes in middle childhood. Nevertheless, these findings suggest that interventions provided to families exposed to intimate partner violence need to target both child and familial factors in order to successfully reduce children’s internalizing symptoms.
Keywords
Rationale
Exposure to domestic violence (DV) during childhood is a global public health concern. DV is defined as “Any incident of threatening behaviour, violence or abuse (psychological, physical, sexual, financial or emotional) between adults who are or have been intimate partners or family members, regardless of gender or sexuality” (Home Office, 2013). Within this review, DV and intimate partner violence (IPV) are considered synonymous, and they are used interchangeably to coincide with the terminology used within individual publications. Exposure to DV is regarded as a form of child maltreatment (Gilbert et al., 2009), and children exposed to DV experience similar rates of internalizing and externalizing problems as those directly abused (Moylan et al., 2010). In the UK and the United States, approximately 20%–25% of children witness DV during childhood and adolescence (Finkelhor et al., 2015; Radford, 2011). The costs of child exposure to DV are significant, and the support of these children and young people has been estimated to cost UK taxpayers £1.4 billion in education, health care, residential, and crime costs (Pro Bono Economics, 2018). In the United States, the lifetime economic burden estimated to be US$70,000 per victim (Holmes et al., 2018).
Exposure to DV in childhood has been linked to psychosocial difficulties, physical, and mental health problems among children and young people (Holt et al., 2008; Wolfe et al., 2003). A meta-analysis has shown significant direct associations between IPV exposure and children’s internalizing, externalizing, and trauma symptoms (Evans et al., 2008), and researchers have started to explore potential risk and protective factors to better understand how DV impacts on child health and well-being, to inform the development of preventative interventions.
A previous systematic review showed that child age, gender, callous–unemotional traits, and cognitive appraisals were key moderators, and maternal mental health and quality of parenting mediated the association between IPV exposure and externalizing problems in children (Fong et al., 2017). Although there is likely to be an overlap, externalizing behaviors are considered to result in part from poor self-regulation, whereas internalizing behaviors are thought to occur from individuals overregulating their thoughts and emotions in a maladaptive way (Cicchetti & Toth, 2014; Merrell, 2008). Internalizing and externalizing problems have been shown to have different sets of risk and protective factors (contextual and genetic factors) despite their comorbidity (Cotter et al., 2016; Smokowski et al., 2017).
Objective
Studies exploring the causal pathway between child exposure to DV and internalizing symptoms have identified factors that are modifiable through intervention (amenable to change), such as self-esteem, and those which are nonmodifiable, or fixed, such as age, sex, maternal marital status, education, and socioeconomic status. (e.g., Gagne & Melancon, 2013; Spilsbury et al., 2007). This review aimed to extend the evidence base described above by exploring (1) mediators—factors that explain the causal pathway through which DV is associated with internalizing symptoms and (2) effect modifiers—factors that alter the strength of the association between DV and internalizing symptoms, among children and adolescents aged 0–18 years within predominantly community samples.
We focused on factors that were amenable to change, thus providing evidence for the components upon which interventions for children and young people exposed to DV could be targeted. An understanding of mediating factors will help to explain how exposure to DV leads to internalizing behaviors. For example, the stress caused by witnessing DV may lead to changes in a child’s ability to regulate their emotions, and this emotion dysregulation may lead to internalizing symptoms. Effect modifiers are factors that interact with the exposure (DV) so that the association is different under certain conditions of the effect modifier (Baron & Kenny, 1986). For example, if gender is a factor that moderates the association between exposure to DV and internalizing behavior symptoms, witnessing DV will be associated with internalizing behaviors among males and females in a significantly different way.
Mediators and effect modifiers may increase or decrease the likelihood of children and young people experiencing internalizing symptoms and therefore may be considered as risk (e.g., harsh parenting) or protective factors (e.g., social support). In line with the biopsychosocial model, these factors may be biological, behavioral, or social conditions, which may be measured at an individual (e.g., self-esteem), family (e.g., familial relationships), or community level (e.g., cultural influences). The focus on internalizing symptoms is important as such symptoms and disorders are often overlooked among children and young people (Merrell, 2008), given that they are harder to detect than externalizing behaviors (Forns et al., 2011). Nevertheless, internalizing symptoms are very common, often emerge in adolescence, and are associated with significant chronicity and mortality (e.g., suicidality; Korhonen et al., 2018; Piqueras et al., 2019).
Method
This systematic literature review was registered with the PROSPERO international prospective register of systematic reviews, registration number: CRD42019127012.
Information Sources and Search Strategy
The electronic databases EMBASE, PsycINFO, and Medline were searched for articles from the “second generation” of research in this area, published between January 1, 1990, and November 6, 2018. This was so as to exclude early research considered to be of poor quality with methodological limitations such as weak definitions and measurement of DV and reliance on shelter samples (Fantuzzo & Lindquist, 1989). The search strategy included words synonymous with “intimate partner violence,” “child or adolescent,” and “psychopathology” along with “risk or protective,” “mediat* or moderat*,” and “resilience.” The full search strategy can be found in Online Appendix A. The past 3 years (2015–2018) of the key three journals (Child Abuse & Neglect, Journal of Family Violence, and Journal of Family Psychology) were also hand searched, and backreferencing of all included studies and identified review articles was applied.
Study Eligibility Criteria
Studies were limited to peer-reviewed articles published in English and included if they were original, quantitative, longitudinal studies investigating potential mediators or effect modifiers of the relationship between child exposure to DV (from birth) and internalizing symptoms in children and adolescents from 0 to 18 years within predominantly community samples. These mediators and effect modifiers should be amenable to change within interventions. Studies must have measured DV as defined by the World Health Organization and must have used validated measure(s) to assess internalizing symptoms (anxiety, depression, somatic complaints, and social withdrawal) to allow comparison across studies. Studies of child maltreatment, family violence, stressful life events, or adverse childhood experiences (ACEs) were included if data specific to DV exposure could be extracted. Studies were excluded if they did not measure internalizing symptoms specifically or used a sample of children and/or adolescents from a nontypical population (e.g., children/adolescents with a chronic illness, intellectual impairment, autism spectrum disorder, or physical disability). Cross-sectional studies were excluded because the temporal relationships between variables cannot be disentangled, so they do not allow investigation of cause-and-effect relationships, and thus, causality cannot be inferred.
Study Records
Screening
After duplication and application of search limits, one author (B.C.) screened all titles and abstracts of citations for potential studies for inclusion. A random 5% sample of titles were reviewed by the three other authors (S.P., A.K., and A.D.; 180 each), together with a 30% sample of abstracts to reduce the likelihood of selection bias (Felson, 1992). Interrater agreement was very good (Fleiss et al., 2013) at both stages (κ = .85 and κ = .86, respectively). Full texts of relevant citations were obtained and read to determine eligibility, and data detailing the study characteristics and outcomes were extracted by the lead author using an extraction form created by the said author if the eligibility criteria were met. A 40% sample of full texts was assessed for eligibility by the three coauthors, and data were extracted if they were included. Again interrater agreement was very good (κ = .86). Any disagreements were discussed and resolved between all reviewers.
Quality appraisal and analysis
Studies were assessed for risk of bias by the lead author using the Newcastle–Ottawa Scale (NOS) for cohort studies (Wells et al., 2015), see Table 1 for study quality ratings.
Newcastle–Ottawa Scale Scores for Included Cohort Studies.
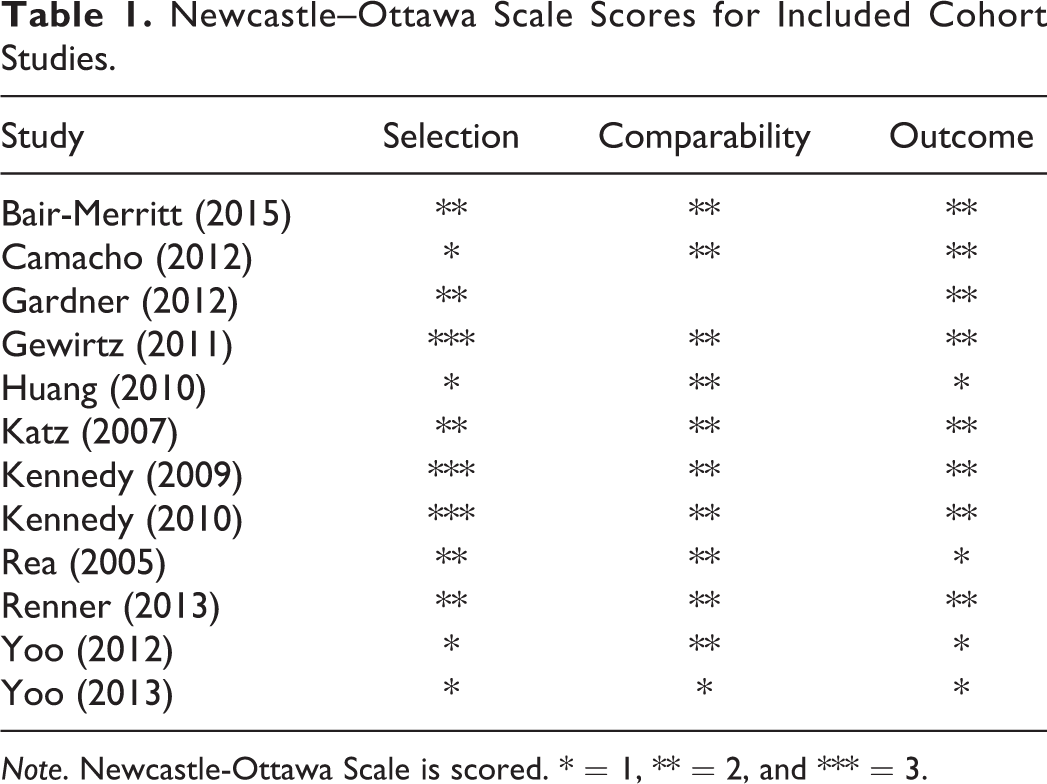
Note. Newcastle-Ottawa Scale is scored. * = 1, ** = 2, and *** = 3.
Due to heterogeneity between the studies in methods and outcomes, which was assessed qualitatively, a narrative synthesis of results was conducted and presented by the level of the factor: individual and familial.
Results
Study Characteristics and Overview
The search identified 7,772 articles after de-duplication and search limits applied. Following application of the eligibility criteria, the full texts of 121 articles were obtained, and 12 longitudinal cohort studies were included in the review (see Online Appendix B).
All studies were conducted in the United States. All studies focused on outcomes within the primary school–aged group (5–11 years) with four including adolescent outcomes (12–18 years). None of the studies investigated preschoolers’ outcomes (under 5 years). Three studies investigated individual factors and nine explored familial factors.
The average length of follow-up within the studies was 30 months, and the sample sizes ranged from 35 to 6,228 children. Study characteristics including type of DV studied and the measures of DV and internalizing symptoms used are presented in Table 2.
Characteristics of Included Longitudinal Studies.
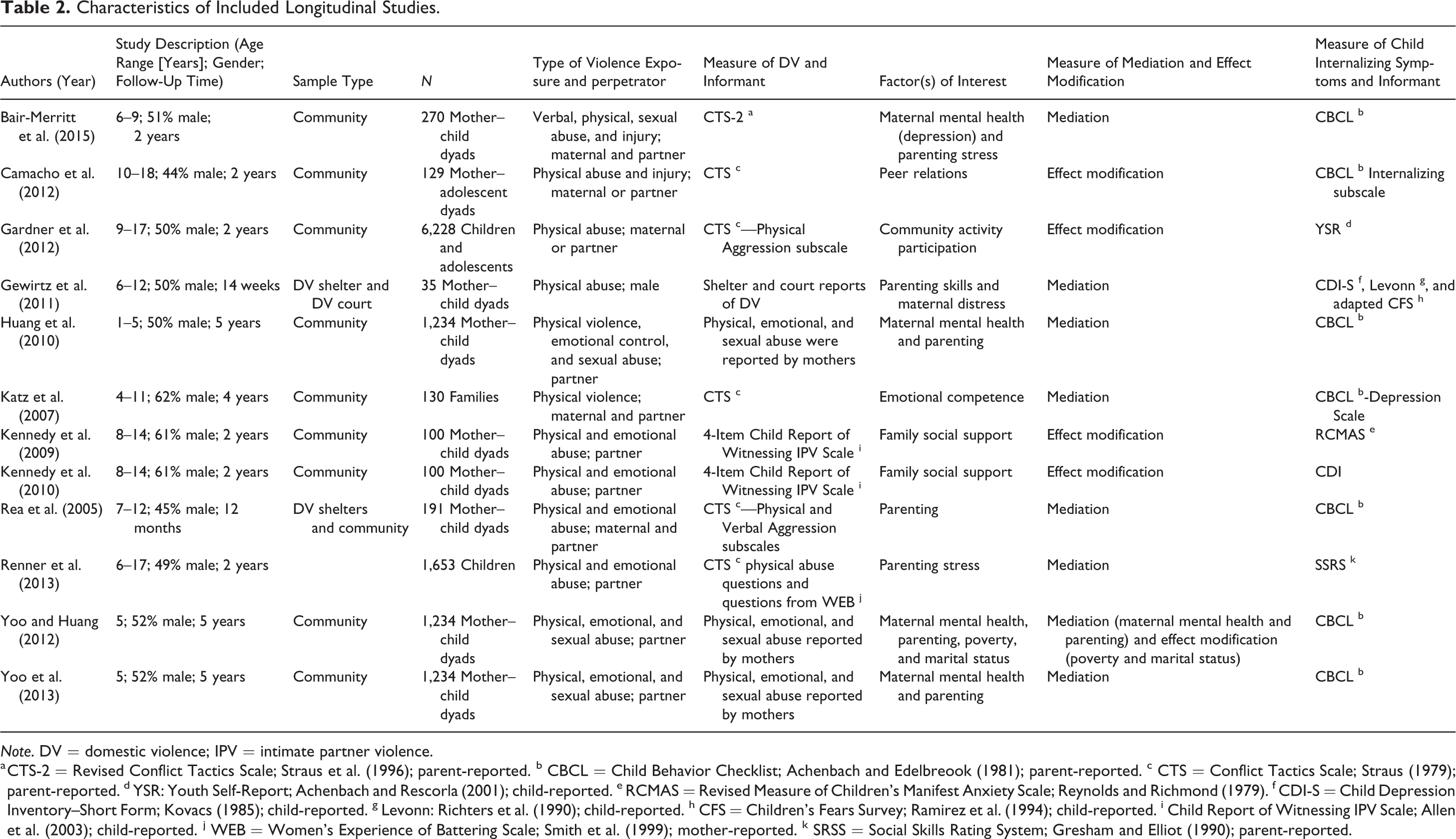
Note. DV = domestic violence; IPV = intimate partner violence.
a CTS-2 = Revised Conflict Tactics Scale; Straus et al. (1996); parent-reported. b CBCL = Child Behavior Checklist; Achenbach and Edelbreook (1981); parent-reported. c CTS = Conflict Tactics Scale; Straus (1979); parent-reported. d YSR: Youth Self-Report; Achenbach and Rescorla (2001); child-reported. e RCMAS = Revised Measure of Children’s Manifest Anxiety Scale; Reynolds and Richmond (1979). f CDI-S = Child Depression Inventory–Short Form; Kovacs (1985); child-reported. g Levonn: Richters et al. (1990); child-reported. h CFS = Children’s Fears Survey; Ramirez et al. (1994); child-reported. i Child Report of Witnessing IPV Scale; Allen et al. (2003); child-reported. j WEB = Women’s Experience of Battering Scale; Smith et al. (1999); mother-reported. k SRSS = Social Skills Rating System; Gresham and Elliot (1990); parent-reported.
Individual Factors
Mediators
Emotional intelligence
Emotional intelligence is the ability to recognize, process, and regulate feelings (Mayer & Salovey, 1997). Emotion regulation, an aspect of emotional intelligence, was thought to lie on the causal pathway between exposure to DV and internalizing symptoms. One study (Katz et al., 2007) showed that emotion dysregulation mediated the association between DV exposure at 5 years and internalizing symptoms at 11 years such that DV exposure led to emotional dysregulation and subsequent internalizing symptoms. Katz et al. (2007) also investigated emotional awareness and reported it to mediate the effect of DV exposure measured at age 5 on internalizing problems at 11 years. This study showed that awareness of negative emotions had a negative association with internalizing problems, suggesting that emotional awareness acts as a buffer against internalizing symptoms (Katz et al., 2007).
Peer relations
Camacho et al. (2012) investigated the indirect effect of peer relation quality in the relationship between IPV and internalizing symptoms in a longitudinal study of preadolescents and adolescents aged 10–18 years. The quality of peer relations was assessed by levels of peer support, prosocial behaviors, overt victimization, and relational victimization (exposure to behaviors aimed at damaging relationships or social reputation). They reported that peer support received and prosocial behavior did not act as a mediator on the pathway between child exposure to DV and internalizing symptoms.
Effect modifiers
Extracurricular activities
One included study investigated the effect of participating in extracurricular activities and reported that intensive participation in either extracurricular activities or after-school programs, but not moderate participation, has been reported to modify the impact of DV exposure on internalizing symptoms among adolescents, suggesting that it may act as a protective factor within this developmental stage (Gardner et al., 2012).
Relational victimization
Camacho et al. (2012) reported that relational victimization modifies the effect of DV on children’s internalizing symptoms such that those who experience high levels of relational victimization and exposure to DV are at increased risk of internalizing symptoms compared to those who have been exposed to DV but have experienced low levels of relational victimization.
Familial Factors
Mediators
Parenting skills
Parenting skills are likely to be diminished in violent families, and this in turn is likely to impact on children’s internalizing symptoms. The “spillover” hypothesis, developed by Easterbrooks and Emde (1988), proposes that “the emotions, affect, and mood generated in the marital realm transfers to the parent-child relationship” (Krishnakumar & Buehler, 2000, p. 26). Thus, hostility within the parental relationship is predicted to reduce parent’s abilities to provide warm/responsive parenting and increased hostile and harsh parenting. Three cohort studies investigated the role of parenting skills on the causal pathway between child exposure to DV and internalizing symptoms (Gewirtz et al., 2011; Huang et al., 2010; Rea & Rossman, 2005).
In a longitudinal study of 905 young children, Huang et al. (2010) found no evidence of a pathway between DV at 1 year of age, negative parenting (unresponsiveness, harshness, and poor communication skills) at year 3, and internalizing symptoms at year 5. However, spanking in particular was found to mediate the pathway between DV and internalizing symptoms among the children. Another study replicated these findings using the same longitudinal data set (Yoo & Huang, 2013).
Rea and Rossman (2005) conducted a cohort study with children aged 7–12 years and their mothers, the majority of whom had been exposed to IPV and reported that authoritarian parenting, and in particular verbal hostility, increased the risk of internalizing symptoms over time, after controlling for the effects of initial psychological functioning, life adversity, and exposure to IPV. This suggests that negative parenting acts as a mediator for primary school–aged children but not among preschool-aged children. No study included a sample of adolescents; therefore, the impact of parenting practices on internalizing symptoms during adolescence following exposure to DV is unknown.
Maternal mental health
Three cohort studies that investigated the role of maternal mental ill-health on psychological adjustment were included (Gewirtz et al., 2011; Huang et al., 2010; Yoo & Huang, 2013). Overall, evidence suggested that poor maternal mental health does not lie on the pathway between DV exposure and internalizing symptoms; however, these studies were conducted with young children under 6 years, and it was unclear whether maternal mental health may have a greater impact among older children and adolescents.
Gewirtz et al. (2011) reported that maternal distress, defined as any current psychopathology or post-traumatic stress symptoms, was only positively associated with depression symptoms in children, among the range of internalizing symptoms. In addition, maternal distress did not significantly impact changes in internalizing symptoms over time nor did it mediate the association between parenting skills and internalizing symptoms. A larger study with a sample of 905 young children also found that, although DV at year 1 was associated with maternal mental health problems at year 3, there was no pathway between DV at year 1, maternal depression at year 3, and children’s internalizing behavior problems at year 5 (Huang et al., 2010). Similarly, Yoo and Huang (2013) reported that, among preschool children, maternal anxiety and depression did not mediate the association between exposure to DV at year 1 on internalizing problems at year 5.
Parenting stress
Evidence for the role of parenting stress on the causal pathway between DV exposure and internalizing symptoms among children and adolescents was mixed. Renner and Boel-Studt (2013) conducted a cohort study with approximately 3-years follow-up and found that parenting stress (stress caused by fulfilling the parenting role) fully mediated the association between exposure to psychological IPV and internalizing behaviors among 6- to 12-year-olds, but no such pathway was found among adolescents (Renner & Boel-Studt, 2013). Moreover, in this study, no direct or indirect pathways were found between physical IPV and internalizing behaviors in either age group. Bair-Merritt (2015) reported that parenting stress did not mediate the significant association between IPV and internalizing symptoms among 6- to 9-year-olds. More research is needed to understand the conditions under which parenting stress accounts for significant variance in children’s internalizing symptoms following DV exposure. It may be that parenting stress is associated with internalizing symptoms through additional mediational pathways such as via parenting skills.
Family functioning
Evidence to support family functioning as protective against developing internalizing symptoms is mixed. Owen et al. (2009) found that family cohesion may be a protective factor in school-aged children. However, neither maternal reports of family cohesion or family adaptability nor child reports of family adaptability mediated the relationship of exposure to DV and children’s internalizing symptoms (Owen et al., 2009). Owen et al. (2009) also found weak evidence for a mediating role of family relatedness, defined as emotional quality and proximity seeking to primary attachment figures. The effect of DV on internalizing symptoms was found to be mediated through children’s perceptions of the emotional quality of family relationships; however, no such mediating pathway was found for maternal reports of emotional quality or child reports of proximity (Owen et al., 2009).
It may be that family functioning is a more powerful mediator of the link between maternal IPV and children’s internalizing symptoms in European American children rather than African American families (Nievar & Luster, 2006), yet more research is needed to establish whether this is true.
Effect modifiers
Positive parenting
Studies have explored the positive impact of effective parenting. Gewirtz et al.’s (2011) small (N = 35), short-term longitudinal study following recent exposure to IPV found that effective parenting modified the effect of IPV exposure on children’s internalizing symptoms such that the behaviors decreased over time among those whose mothers demonstrated positive parenting skills, whereas internalizing symptoms remained stable over time among those with poorer parenting skills.
Family social support
Evidence suggesting family social support to be protective against developing internalizing symptoms following childhood exposure to DV is mixed. In a longitudinal study with a sample of 100 school-aged children, it was found that changes in family social support moderated the effect of changes in witnessing DV on depression symptoms over time. However, a three-way interaction showed that the impact of social support depended on gender. Reductions in witnessing IPV over time were associated with fewer depression symptoms over time except among boys who reported low levels of family social support initially (Kennedy et al., 2010). This finding implies that social support is a protective factor against depression following exposure to IPV, particularly among boys. When considering anxiety symptoms as the outcome, Kennedy and colleagues (2009) found, using the same sample, method, and procedure, that family social support did not moderate the association between IPV exposure and anxiety among children.
A summary of the findings above is presented in Figure 1 along with a number of hypothesized associations between factors that require further exploration as the current evidence base is inconclusive.
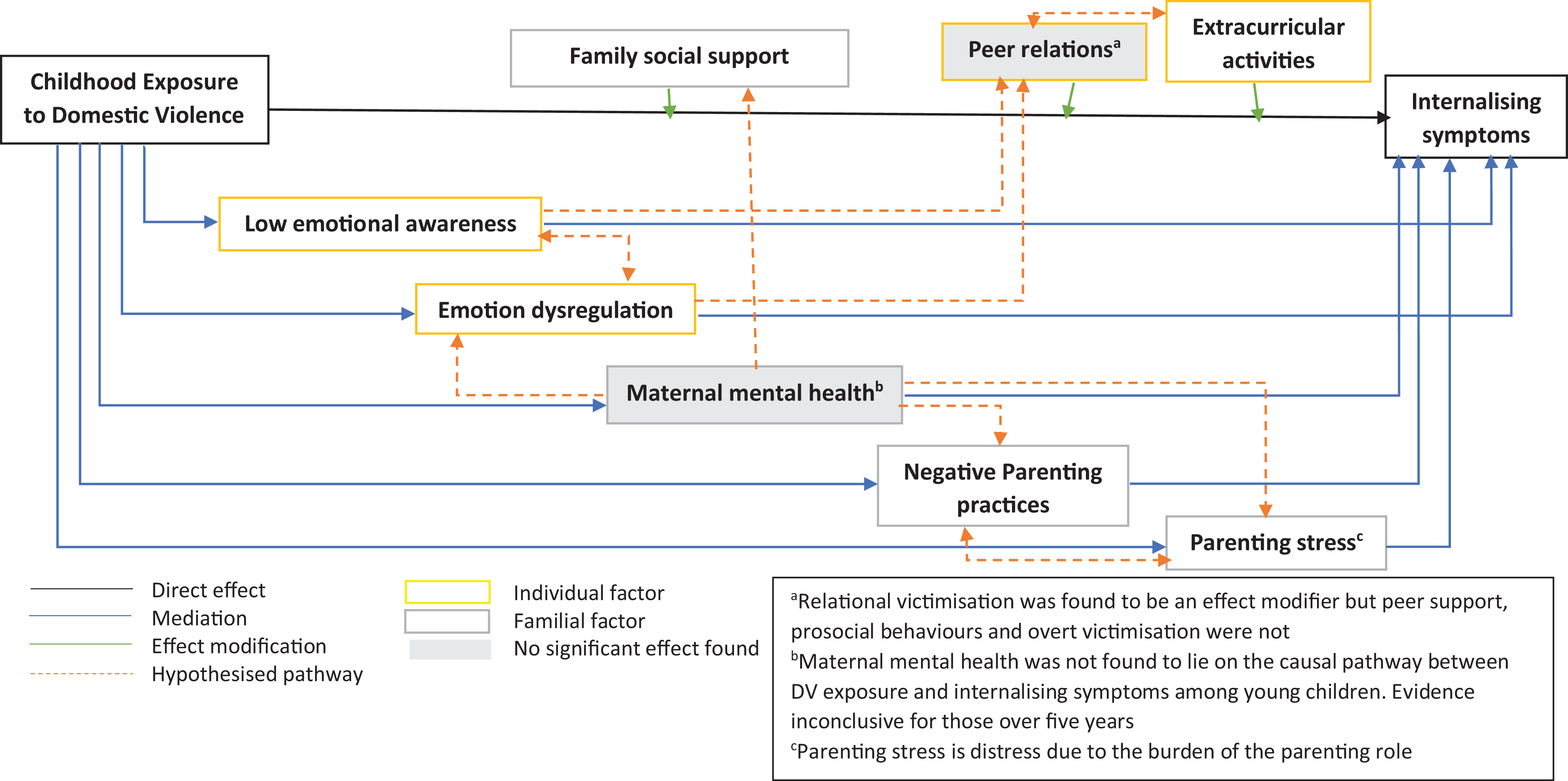
Directed acyclic graph illustrating the relations between factors identified within this review along with hypothesized associations between factors.
Risk of Bias in Individual Studies
Most studies were of reasonable quality given their observational nature and the sensitive topic; however, all introduced some risk of bias for several reasons. A full evaluation of the risk of bias using the NOS can be found in Table 1.
Most studies adjusted for several important confounders. The lack of consistency among measures of DV made it difficult to compare results and potentially introduced further bias. Few studies included emotional abuse, those that did sometimes omitted physical abuse, and none mentioned measuring all forms of DV described above, so the full extent of the abuse was not obtained. Most studies only investigated DV events within the past year, so the impact of past exposure, cumulative, and chronic exposure over time was not explored. Furthermore, a few studies included child reports of DV exposure, yet the majority relied on parental reports, which may not truly reflect childhood exposure and may have been affected by social desirability.
All the included studies introduced risk of bias using self-report measures to assess internalizing symptoms rather than data linkage to medical/education records or blind assessment of behavior by clinicians. Most of the studies also relied on maternal reports of their child or children’s internalizing symptoms rather than child self-reports introducing potential response bias, as mothers may not be aware of their child’s internal suffering resulting in underestimates, or they may overestimate their children’s psychological distress if they are stressed and distressed themselves. Studies that included both child and parental reports demonstrated that the two do not always correlate, and therefore, results may not be interpreted confidently. In this context, however, using record linkage to identify internalizing symptoms could also introduce bias as only those with severe, clinical levels of internalizing symptoms would be recorded, unlike self-report measures.
Discussion
This review has consolidated evidence for mediators and effect modifiers on the causal pathway between DV exposure and internalizing symptoms in children and adolescents that are modifiable. One individual-level mediator was identified, namely emotional intelligence, and two effect modifiers were identified: relational victimization and participation in extracurricular activities. Familial mediators included maladaptive parenting and parenting stress, while effect modifiers included positive parenting (maternal warmth and availability) and family social support. No factors were identified at a community level.
This review’s findings partially support another recent systematic review, which synthesized evidence for factors promoting emotional–behavioral resilience in children following exposure to IPV (Fogarty et al., 2019). (Fogarty et al., 2019)Emotional and behavioral outcomes were defined as internalizing and externalizing difficulties, and the authors identified protective factors against such problems only, not risk factors. Our review identified low social support, emotion dysregulation, negative parenting practices (e.g., spanking), and parenting stress to increase the risk of internalizing symptoms following exposure to DV. Potential factors promoting resilience identified by Fogarty et al. (2019) included emotion coaching, authoritative (warm and responsive) parenting, and easy child temperament. Emotion coaching may be an effect modifier that improves children’s emotional intelligence, identified within this review to be a mediator on the causal pathway between DV exposure and internalizing symptoms. Positive maternal mental health was also reported by Fogarty et al. (2019) to predict emotional–behavioral resilience among children exposed to IPV; however, this review has found that, when only longitudinal studies are included, poor mental health does not lie on the pathway between DV exposure and internalizing symptoms; however, this has only been reported among young children (Gewirtz et al., 2011; Huang et al., 2010; Yoo & Huang, 2013). However, the studies identified in this review did not include children over the age of 5 years, so it may be that maternal mental health has a greater impact when children are older and have a greater understanding of the situation.
The results from this review have highlighted that there is little evidence to date for the factors that impact the association between exposure to DV and internalizing symptoms in adolescence. Increasing age has been found to be protective (Spilsbury et al., 2007), implying recent DV exposure has a smaller effect on internalizing symptoms in adolescents. However, other studies have shown that internalizing symptoms are still pronounced in adolescence following IPV exposure and argue that adolescence may be a sensitive period for the impact of IPV exposure on internalizing symptoms, given the already increased vulnerability to psychopathology due to developmental, behavioral, hormonal, and neurological changes (Menon et al., 2018; Vu et al., 2016). A practical limitation may be that cohort studies investigating life course effects are expensive, yet longitudinal data do exist and allow exploration of the effects of time between the exposure (DV) and the outcome as well as exposure duration.
Implications for Interventions
This review has identified potential modifiable factors, which may be important to target in interventions for children, young people, and their families who have suffered from DV. For example, interventions targeting children’s emotion regulation and emotion awareness could help prevent children who have been exposed to DV developing internalizing behaviors. Family interventions may benefit from focusing on positive parenting such as using positive reinforcement and calm limit-setting rather than corporal punishment such as spanking, as this is likely to be a further risk factor for children developing internalizing symptoms (Yoo & Huang, 2013). Furthermore, interventions aiming to foster children’s feelings of family cohesion and positive sibling relationships may help buffer children from experiencing negative psychological outcomes following DV exposure. Furthermore, as intensive participation in extracurricular activities was found to moderate the link between DV and internalizing behaviors (Gardner et al., 2012), helping support children to attend groups and classes may help prevent children and adolescents exposed to DV from developing poorer psychological adjustment. It is important to note that intervention studies were not included in this review. Such interventions may already exist, however this review cannot provide scientific evidence for such programs.
Most studies included in this review have tended to adopt the traditional risk–outcome approach, focusing on identifying and reducing risks and operationalizing protection as absence of risk (e.g., poor maternal mental health is a risk and absence of psychological disorders is protective). In contrast, a strength-oriented approach is preventative and considers protective factors within an individual, family, and community that modify the effects of negative events, enabling children and young people to be resilient and “bounce back” in the face of adversity (Luthar et al., 2000; Rutter, 2000). These factors include having at least one positive relationship with an adult, and having an internal locus of control over events (Luthar et al., 2000). Focusing on protective factors helps children, adolescents, and families build resilience through developing valuable skills, knowledge, and relationships that help counteract risk exposures and contribute to positive outcomes (Masten, 2001).
Limitations
The main limitation of this review is that it provides breadth but not depth as studies have explored a number of potential mediators and effect modifiers, but the majority have only been studied once or twice. Therefore, the conclusions that can be drawn about each factor and its role in the relationship between DV and internalizing symptoms among children and adolescents are limited. Additionally, in trying to understand the association between DV exposure and internalizing symptoms, studies have investigated one exposure and outcome, failing to consider the complexity of families who have experienced DV. Furthermore, the tendency to focus on a single mediator or effect modifier within each study prevents the exploration of relationships between factors and the identification of which factors are most important to focus upon within interventions.
All the included studies were conducted in the United States, and different factors may be prominent risk factors or key to protecting children and adolescents exposed to DV against internalizing symptoms in other countries and cultures. Additionally, cultural views and responses toward DV may influence the complex association between DV and child and adolescent internalizing symptoms. Thus, it is not clear whether the findings identified in this review are generalizable to other ethnic and cultural groups. In addition, countries differ in their social care interventions and the state may intervene at different points, which is likely to affect the duration and severity of DV children and adolescents are exposed to across countries, reducing generalizability.
Many of the studies in this review included wide age ranges but did not explore differences across developmental or educational stages, which complicated the interpretation of findings, given that risk and protective factors may vary across these parameters. This could be addressed by cohort studies taking a life course approach to the impact of early and/or prolonged exposure to DV and other adversities.
Studies tended to only include male-perpetrated violence or did not distinguish between male- and female-perpetrated abuse within analyses, and none considered same-sex couple violence. This may confound the effects of child gender, and it is unknown whether factors such as maternal mental health (or paternal mental health), along with other factors, would have the same impact if the DV was female perpetrated.
The exclusion of intervention studies limited this review, as they provide additional, compelling evidence for mediators and effect modifiers within natural settings. Further research is advised to systematically search intervention studies that have investigated the factors identified within this study to gather further evidence before future interventions are developed.
Finally, this review is likely to be affected by publication bias with an emphasis on publication of significant results rather than null results and may be affected by the duplicate publication bias, as multiple studies with a significant result are more likely to be published than a single study indicating a nonsignificant result, yet both contribute to the overall effect of a factor within a systematic review.
Directions for Future Research
Although mediators and effect modifiers of the causal pathway between DV and internalizing symptoms among children and adolescents have been identified, more research is needed to establish the extent of indirect pathways, particularly research exploring protective factors.
More longitudinal studies are needed to determine causal relations between potential mediating factors, to enable inferences to be drawn about causality, and to investigate the impact of chronic DV exposure over time or prior exposure rather than just current or recent exposure. Such studies would enable understanding as to whether certain risk and protective factors are important at different stages through childhood and adolescence. For instance, it may be that maternal factors are more influential during childhood; however, when children enter adolescence and gain greater freedom, social factors such as peer support or bullying may be more prominent. In particular, more research is needed to determine the effect of maternal mental health on the pathway between DV and internalizing symptoms among school-aged children and adolescents as currently this is unclear.
Other ACEs should be considered when investigating internalizing symptoms. Although DV exposure has been shown to be a strong risk factor for poor psychological adjustment, other influential traumatic experiences are likely to co-occur (Appel & Holden, 1998). Studies have shown the accumulation of ACEs to be associated with greater risk of psychopathology both in childhood (Flouri & Kallis, 2007) and across the life span (Chang et al., 2019; Felitti et al., 1998). Investigating multiple risk and protective factors consecutively rather than in isolation would enable researchers and clinicians to identify the most important factors for services and policies to target.
Another neglected line of research is the role of paternal characteristics. Understandably, the paucity of research in this area is likely due to issues of safety and a duty of care to the families participating in research. However, paternal parenting skills may be just as important as maternal parenting, and it may be that factors such as a positive mother–child relationship are only protective if the mother is the victim of DV rather than the perpetrator.
While much of the research surrounding childhood exposure to DV has focused on violence perpetrated by males (Wolak & Finkelhor, 1998), it is important to recognize that children may also be exposed to DV in which their mother is the perpetrator or bidirectional acts of violence between caregivers occur (Holmes et al., 2017). Outcomes and related risk or protective factors may be different when the mother is the perpetrator or violence is bidirectional. Furthermore, they may be different across diverse family profiles, including same-sex couples and kinship caregivers (e.g., grandparents); therefore, it is important that such families are included within DV studies.
Conclusion
This systematic literature review has provided an overview of the current evidence for the causal pathway between exposure to DV and internalizing symptoms among children and adolescents. This evidence is valuable for services working with children and young people who are experiencing internalizing problems following exposure to DV and their families. Key methodological issues have been highlighted, which may help improve future research in the field. Parenting stress and parenting skills appear to play critical roles in the indirect pathway between DV and internalizing symptoms at all three developmental stages. This demonstrates the need for mothers who have experienced DV to have access to a parenting support to maintain both their own and their children’s mental well-being. Overall, this knowledge is vital for guiding clinical and community interventions for children and young people exposed to DV and their families in order to prevent children from experiencing psychopathology.
Supplemental Material
Supplemental Material, sj-pdf-1-tva-10.1177_1524838020965964 - Mediators and Effect Modifiers of the Causal Pathway Between Child Exposure to Domestic Violence and Internalizing Behaviors Among Children and Adolescents: A Systematic Literature Review
Supplemental Material, sj-pdf-1-tva-10.1177_1524838020965964 for Mediators and Effect Modifiers of the Causal Pathway Between Child Exposure to Domestic Violence and Internalizing Behaviors Among Children and Adolescents: A Systematic Literature Review by Bethan Carter, Shantini Paranjothy, Alisha Davies and Alison Kemp in Trauma, Violence, & Abuse
Supplemental Material
Supplemental Material, sj-pdf-2-tva-10.1177_1524838020965964 - Mediators and Effect Modifiers of the Causal Pathway Between Child Exposure to Domestic Violence and Internalizing Behaviors Among Children and Adolescents: A Systematic Literature Review
Supplemental Material, sj-pdf-2-tva-10.1177_1524838020965964 for Mediators and Effect Modifiers of the Causal Pathway Between Child Exposure to Domestic Violence and Internalizing Behaviors Among Children and Adolescents: A Systematic Literature Review by Bethan Carter, Shantini Paranjothy, Alisha Davies and Alison Kemp in Trauma, Violence, & Abuse
Footnotes
Authors' Note
Shantini Paranjothy is now affiliated with Aberdeen Health Data Science Research Centre, University of Aberdeen, United Kingdom.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.