
Abstract
Introduction:
Despite the high prevalence of intimate partner violence (IPV) perpetration by men who use substances, limited evidence exists about how best to reduce IPV among this group.
Method:
A systematic narrative review with meta-analysis determined the effectiveness of interventions to reduce IPV by men who use substances. Inclusion criteria were randomized and nonrandomized controlled trials; adult heterosexual male IPV perpetrators where at least 60% of participants were alcohol and/or drug users; the intervention targeted IPV with or without targeting substance use (SU); outcomes included perpetrator and/or victim reports of IPV, SU, or both. Methodological quality was assessed.
Results:
Nine trials (n = 1,014 men) were identified. Interventions were grouped into (1) integrated IPV and SU interventions (n = 5), (2) IPV interventions with adjunct SU interventions (n = 2), and (3) stand-alone IPV interventions (n = 2). Cognitive behavioral and motivational interviewing therapies were the most common approaches. Data from individual trials showed a reduction in SU outcomes in the short term (≤3months; n = 2 trials) and IPV perpetration at different time points (n = 3 trials) for interventions compared with treatment as usual (TAU). Meta-analysis with integrated IPV and SU interventions showed no difference in SU (n = 3 trials) or IPV outcomes (n = 4 trials) versus SU TAU.
Conclusions:
Little evidence exists for effective interventions for male IPV perpetrators who use substances. Outcomes in integrated interventions were not superior to TAU in meta-analysis. Future trials should consider the nature of the relationship between IPV and SU in intervention design, duration of intervention, and type and timing of outcome measures.
Intimate partner violence (IPV), defined as threatening or coercive behavior, violence, or abuse between ex/current partners, is a recognized global public health issue, resulting in harm to those who experience it and their families (Scarduzio, Carlyle, Harris, & Savage, 2017; Vos et al., 2006). While the prevalence of IPV among Lesbian, Gay, Bisexual, Transgender+ (LGBT+) individuals is equivalent or higher than in heterosexual relationships (Stiles-Shields & Carroll, 2015), women are purportedly more likely to be victims of sexual violence, severe physical violence, or murder by their male partner (World Health Organization, 2013 As a result, IPV interventions have predominantly focused on measures to protect women (Rivas et al., 2015). Although crucial, such interventions only respond to one aspect of this complex phenomenon, often resulting in short-term success (Clarke & Wydall, 2015). Thus, attention has turned to secondary prevention by seeking to rehabilitate those who perpetrate IPV (Bowen, Brown, & Gilchrist, 2003). A coordinated response that prioritizes the needs of victims and survivors while concurrently addressing the behavior of perpetrators is likely to be more effective in preventing future violence (Clark & Wydall, 2013; Davies & Biddle, 2018; Diemer, Humphreys, Lmaing, & Smith, 2015). However, the effectiveness of current perpetrator programs remains unclear.
Current perpetrator programs largely adhere either to a psychoeducational feminist perspective (e.g., the 26-week Duluth program) or to a cognitive behavioral therapy (CBT) approach (Pence & Paymar, 1993). Two meta-analyses on the effectiveness of psychoeducational interventions indicate low effect sizes on recidivism, with similarly poor results being found for CBT interventions (Feder & Wilson, 2005; Feder, Wilson, & Austin, 2008; Smedslund, Dalsbø, Steiro, Winsvold, & Clench-Aas, 2011; Tarzia, Forsdike, Feder, & Hegarty, 2017). Criticisms include inconsistent (noncomparable) measurement of outcomes, insufficient evaluation of context, and short-term follow-up (Gondolf, 2012). Reviews of motivational interventions have also found inconclusive evidence of the effectiveness of IPV perpetrator programs (Miller & Rollnick, 1991; Vigurs, Schuchen-Bird, Quy, & Gough, n.d.). However, recent UK health service guidance highlights that the cost of IPV is “so significant that even marginally effective interventions are cost effective” (National Institute for Health and Care Excellence, 2014). Thus, in addition to uncertainty surrounding the effectiveness of IPV perpetrator interventions, there is a need for rigorous evaluation of existing interventions.
Robust evidence supports an association between substance use (SU; i.e., alcohol and drug use) and IPV, with a consensus that SU can increase both the frequency and severity of violence (Cafferky, Mendez, Anderson, & Stith, 2018; Leonard & Quigley, 2017). Substance abuse or dependence are significantly stronger correlates of IPV perpetration for males (Cafferky et al., 2018). Findings have highlighted that rates of physical or sexual violence perpetration among men receiving treatment for SU are far higher than those within the general population (Gilchrist et al., 2015; Gilchrist, Radcliffe, Noto, & Flavia, 2017; O’Farrell, Fals-Stewart, Murphy, & Murphy, 2003; O’Farrell, Murphy, Stephan, Fals-Stewart, & Murphy, 2004; Taft et al., 2010; Ten Have, de Graaf, van Weeghel, & van Dorsselaer, 2014). Additionally, one study concluded that 14% of physical IPV in the general population was attributable to SU (Ten Have et al., 2014). One substance particularly attributed to violence is that of alcohol, with the suggestion that the elimination of hazardous drinking would result in a reduction of general population violence by 44% (Fergusson, Boden, & Horwood, 2013). Such findings have led many to identify a need to acknowledge a relationship between IPV and SU (Gilchrist, Radcliffe, Noto, & Flavia, 2017) and focus on developing integrated IPV and SU interventions (Capaldi, Knoble, Shortt, & Kim, 2012; G.Gilchrist & Hegarty, 2017; Leonard & Quigley, 2017; McMurran, 2017).
Illustrative of this, a narrative review by Tarzia, Forsdike, Feder, and Hegarty (2017) concluded that while there was little evidence in terms of the effectiveness of IPV interventions in health settings, those that addressed both IPV and SU concurrently demonstrated promise. Furthermore, naturalistic studies have identified associations between reductions in IPV perpetration and successful completion of SU treatment (Murphy & Ting, 2010). This review aims to determine the effectiveness of interventions to reduce IPV perpetration for men who use substances.
Method
A systematic review with meta-analysis was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (Moher et al., 2015). This protocol was registered with the International Prospective Register of Systematic Reviews (Huntley et al., 2017; PROSPERO 2017: CRD42017056596).
Search Strategy
Identified via published articles and by consulting experts, searches were performed combining three topics: IPV, interventions, and SU (online file). Citations were managed using Endnote software (Version 6, 0.1). The following databases were searched from inception date to May 25, 2018, for relevant studies: MEDLINE, EMBASE, CINAHL, PsycINFO, SSCI, IBSS, and Social Services Abstracts, with an update in MEDLINE to April 8, 2019. Clinical trial databases were searched to identify additional studies (National Institute for Health Research Register; www.who.int/ictrp/ and National Health; and Medical Research Council, Australia). Consultations with experts and forward–backward reference list searches of recent reviews were also conducted.
Eligibility Criteria
The PICOD (i.e., Population, Intervention, Control, Outcome, and Design) format was applied in formulating inclusion criteria, using the hierarchy assessment method of eligibility. Randomized controlled trials (RCTs) or nonrandomized controlled trials were eligible if (1) the intervention targeted IPV or relationships among adult heterosexual males; (2) included samples where at least 60% were described as people who currently drank hazardously or who met criteria for abuse or dependence on alcohol or drugs (i.e., SU); (3) interventions were compared to either IPV perpetrator or SU treatment as usual (TAU) or an intervention of a lesser intensity or frequency; and (4) outcome measures included perpetrator and/or victim reports of IPV perpetration, and/or SU, and/or marital satisfaction/conflict. There were no language restrictions.
Screening and Inclusion
Titles and abstracts were assessed by G.G. and E.G., with disagreements resolved by D.S.-L. Several authors (G.G., E.G., M.M., G.F., A.H., D.S.-L., A.J.) assessed full texts against eligibility criteria. Conflicting results were resolved by a third reviewer (D.S.-L., A.J., or J.H.). Two authors (D.S.-L., A.J.) extracted data from eligible trials into a custom spreadsheet.
Methodological Quality
Two authors (D.S.-L., A.J.) independently assessed trial methodological quality as high, medium, or low risk using the Cochrane Effective Practice and Organisation of Care (EPOC) tool for assessing risk of bias (Higgins et al., 2011). Nine standard criteria were assessed: random sequence generation, allocation concealment, baseline outcome measurements similar, baseline characteristics similar, incomplete outcome data, knowledge of the allocated interventions adequately prevented during the study, protection against contamination, selective outcome reporting, and other risks of bias. Each criterion was scored according to whether there was high, low, or unclear risk of bias. Conflicting assessments were resolved through discussion.
Data Extraction, Synthesis, and Statistical Analysis
The better reporting of interventions: Template for intervention description and replication checklist was used to describe and compare interventions (Hoffmann et al., 2014). Specifically, information around the intervention goals and approach, associated materials and procedures followed, facilitators, intervention frequency and duration, delivery mode, setting and modifications made were extracted. In addition, outcome assessments and outcomes were tabulated. This standardized approach of data extraction allowed interventions, participants, settings, and outcomes across trials to be described and compared (Ryan, Hill, Prictor, & McKenzie, 2013). To allow comparison of heterogeneous intervention models, trials were grouped and analyzed separately: (1) integrated IPV and SU interventions (i.e., interventions that simultaneously addressed IPV and SU), (2) IPV interventions with adjunct SU interventions (i.e., IPV interventions with a separate session or intervention on SU), and (3) stand-alone IPV interventions (i.e., these interventions did not address SU).
In terms of statistical analysis, if sufficient in number, and suitable in terms of statistical and methodological heterogeneity, a comparison was made between intervention and control group data (Higgins et al., 2019). Specifically, the analysis plan required at least two RCTs with combinable data for the prespecified outcomes. A meta-analysis using a random effects model was performed using Review Manager Version 5.1. Statistical heterogeneity was estimated using the I-squared (I2) statistic, where I2 > 50% may be indicative of substantial heterogeneity. Due to limited data, it was not possible to examine the effectiveness of individual components of interventions on outcomes.
Results
Study Selection
Following removal of duplicates, 5,202 citations were identified from the search and screened, and 176 full-text articles were assessed for eligibility. Application of the inclusion criteria resulted in a total of 13 manuscripts from nine trials being included in the review (Figure 1). These trials were grouped into three intervention types (Table 1): (1) integrated IPV and SU interventions (n = 5), (2) IPV interventions with adjunct SU interventions (n = 2), and (3) stand-alone IPV interventions (n = 2). The meta-analysis included four trials from the integrated IPV and SU interventions group (Easton, Crane, & Mandel, 2018; Easton, Mandel, Hynkele, Nuch, Rounsaville, & Carroll, 2007b; Kraanen, Vedel, Scholing, & Emmelkamp, 2013; Mbilinyi et al., 2011). There were insufficient data to conduct meta-analyses for the two other intervention types.
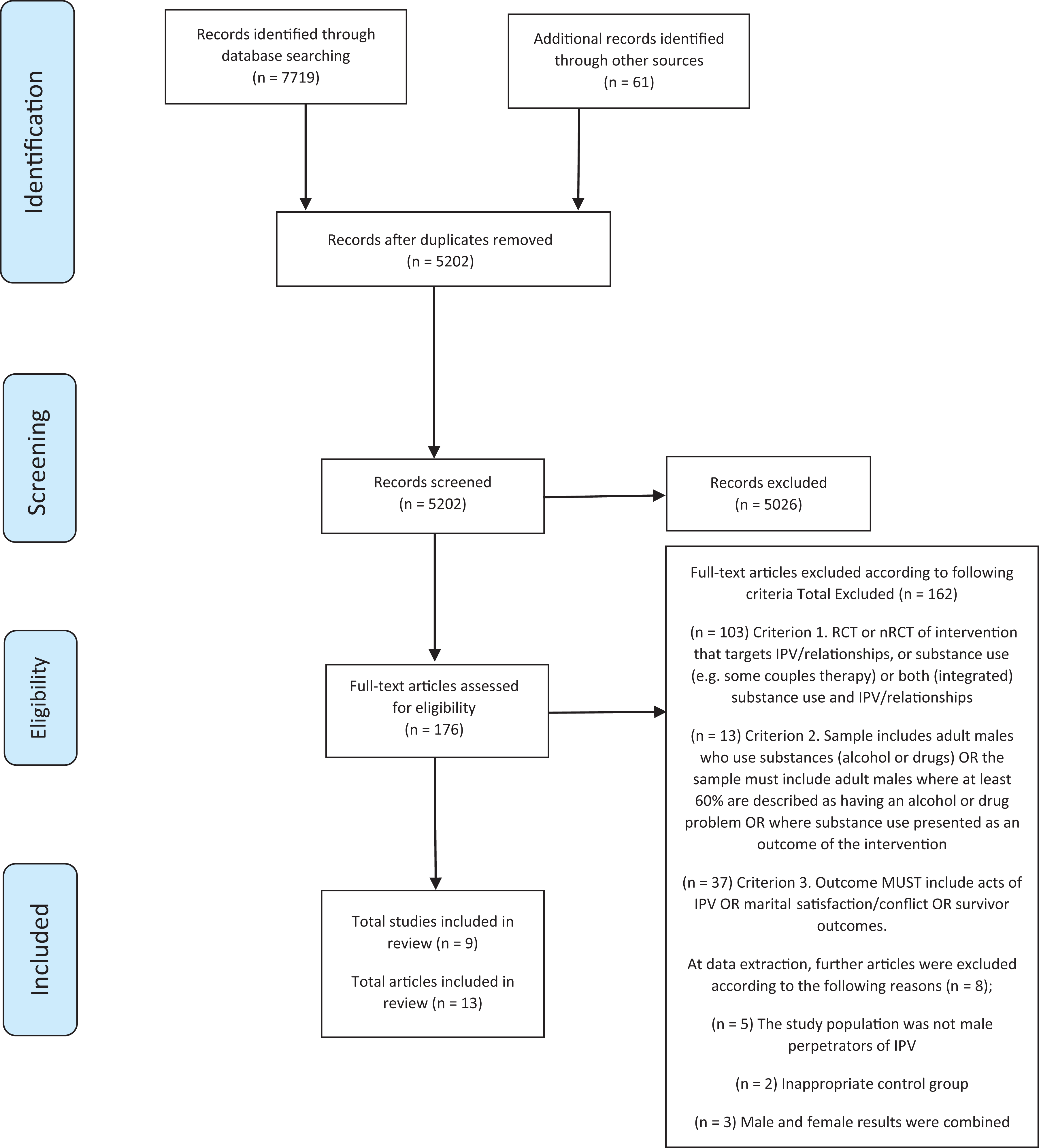
preferred reporting items for systematic reviews and meta-analyses flow-chart of the data strategy process.
Trial Groupings and Intervention Characteristics.
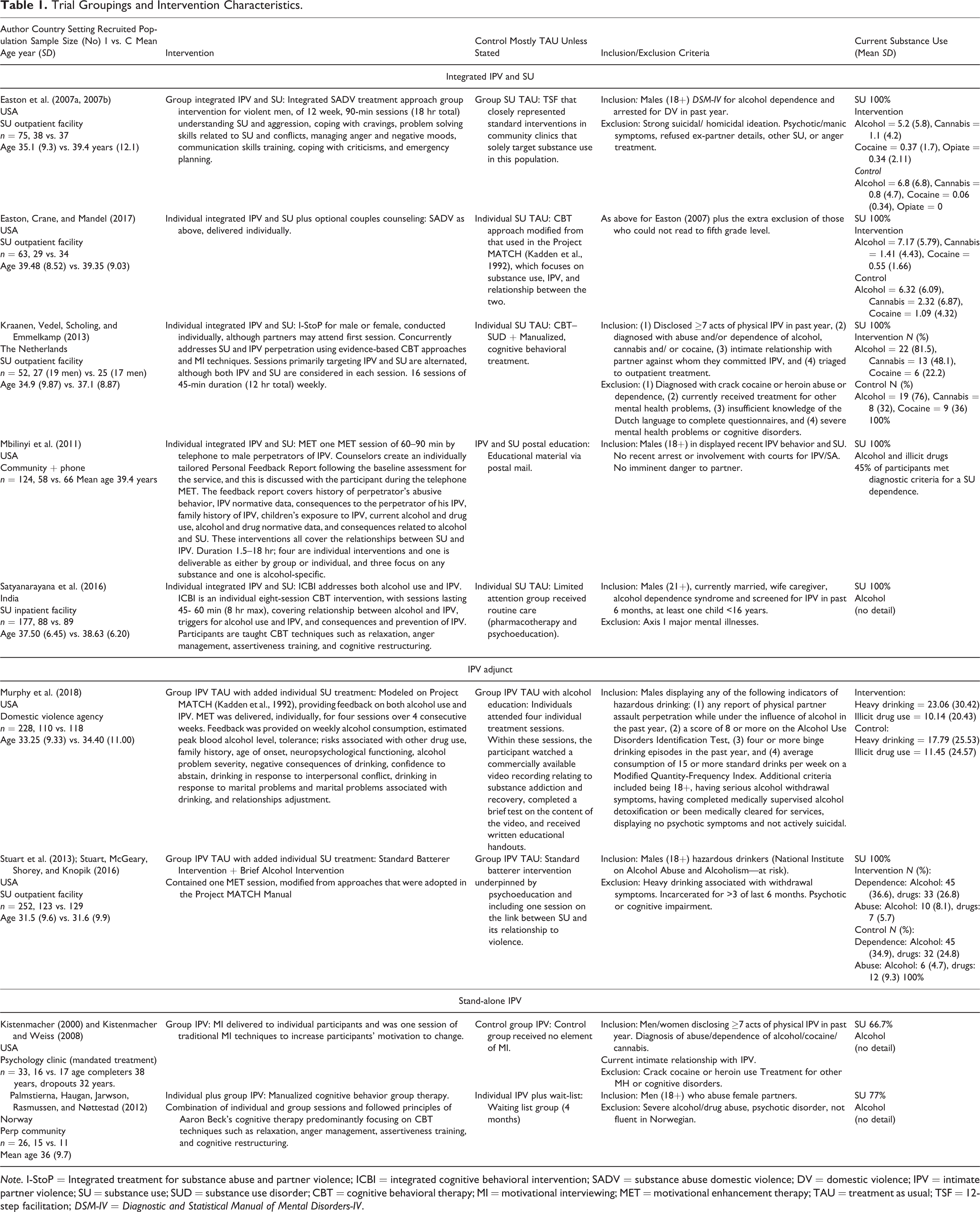
Note. I-StoP = Integrated treatment for substance abuse and partner violence; ICBI = integrated cognitive behavioral intervention; SADV = substance abuse domestic violence; DV = domestic violence; IPV = intimate partner violence; SU = substance use; SUD = substance use disorder; CBT = cognitive behavioral therapy; MI = motivational interviewing; MET = motivational enhancement therapy; TAU = treatment as usual; TSF = 12-step facilitation; DSM-IV = Diagnostic and Statistical Manual of Mental Disorders-IV.
Quality Assessment
Quality assessment found that the trials were conducted with low risk of bias, but there was a lack of information or clarity for some assessment domains. Specifically, in line with the EPOC tool for assessing risk of bias, in the integrated IPV and SU interventions, three of the five trials did not describe allocation concealment (Easton et al., 2007a; 2007b; Krannen et al., 2013; Mbilinyi et al., 2011); one reported uneven baseline measures (Easton et al., 2017), but did attempt to correct this in analysis, and three did not comment on how incomplete outcome measures were dealt with (Easton et al., 2007a; 2007b; Mbilinyi et al., 2011; Satyanaranya et al., 2016). Knowledge of allocation and contamination was not described except for one that suggested potential contamination issues (Satyanaranya et al., 2016). Of the two trials of IPV interventions with adjunct SU interventions, one was assessed as high risk of bias in terms of allocation concealment and incomplete outcome measures (Stuart et al., 2013), while the other did not describe allocation concealment and did not comment on allocation contamination (Murphy et al., 2018). In the stand-alone IPV interventions, one trial had contamination between groups (Kistenmacher, 2000).
Intervention Characteristics
Table 1 outlines RCT characteristics. Seven interventions were delivered to men individually (Easton et al., 2017; Kistenmacher, 2000; Kraanen et al., 2013; Mbilinyi et al., 2011; Murphy et al., 2018; Satyanarayana et al., 2016; Stuart et al., 2013). Of these, six were delivered face-to-face, with one delivered by phone (Mbilinyi et al., 2011). One intervention was delivered to men in a group (Easton et al., 2007a; 2007b) and one provided both group and individual sessions (Palmstierna, Haugan, Jarwson, Rasmussen, & Nøttestad, 2012). Four interventions employed the principles of CBT (Easton et al., 2007a; 2007b; Easton et al., 2017; Palmstierna et al., 2012; Satyanarayana et al., 2016). Of these, three adopted CBT in targeting both IPV and SU simultaneously (Easton et al., 2007a; 2007b; Easton et al., 2017; Satyanarayana et al., 2016), while the remaining intervention targeted IPV alone (Palmstierna et al., 2012). Another trial adopted both CBT and motivational interviewing (MI; Kraanen et al., 2013), using both approaches to target IPV and SU simultaneously. One included a standard IPV program, using MI in targeting SU specifically (Stuart et al., 2013). Of the final two trials, one used MI in targeting IPV and SU simultaneously (Mbilinyi et al., 2011), while the other used MI in targeting IPV alone (Kistenmacher, 2000).
Population SU Characteristics
Kistenmacher (2000) and Palmstierna, Haugan, Jarwson, Rasmussen, and Nøttestad (2012) included samples, where 67% and 77% of the samples, respectively, were men who drank hazardously or who were dependent on alcohol. Kistenmacher (2000) considered self-reported referrals to drug and/or alcohol treatment in the past, while Palmsterina et al. (2012) assessed SU through self-reports of violence perpetration while intoxicated. The remaining seven RCTs included samples, where 100% reported hazardous drinking, abuse, or dependence on alcohol, cannabis, cocaine, or heroin. Hazardous use was assessed using the Alcohol Use Disorders Identification Test (Murphy et al., 2018; Stuart et al., 2013) and the Short Inventory of Problems (Miller, Tonigan, & Longabaugh, 1995; Stuart et al., 2013). Drug and alcohol abuse and/or dependence were assessed using the Diagnostic and Statistical Manual of Mental Disorders-VI for five trials (Easton et al., 2007a; 2007b; Easton, Crane, & Mandel, 2018; Mbilinyi et al., 2011; Satyanarayana et al., 2016; Stuart et al., 2013). Kraanen, Vedel, Scholing, and Emmelkamp (2013) assessed alcohol and drug abuse and/or dependency using Measurements in The addictions For Triage and Evaluation (Schippers, Broekman, Buchholz, Koeter, & van den Brink, 2010), while Murphy et al. (2018) assessed alcohol abuse and/or dependency using the Clinical Institute Withdrawal Assessment for Alcohol tool (Sullivan, Sykora, Schneiderman, Naranjo, & Sellers, 1989). Kraanen et al. (2013) excluded those who were diagnosed with crack cocaine or heroin abuse and/or dependency due to them requiring more intensive inpatient treatment. Furthermore, two trials excluded men if deemed to have severe alcohol or drug dependency (Palmstierna et al., 2012; Stuart et al., 2013). Table 1 outlines recruitment settings, SU characteristics, and trial inclusion/exclusion criteria.
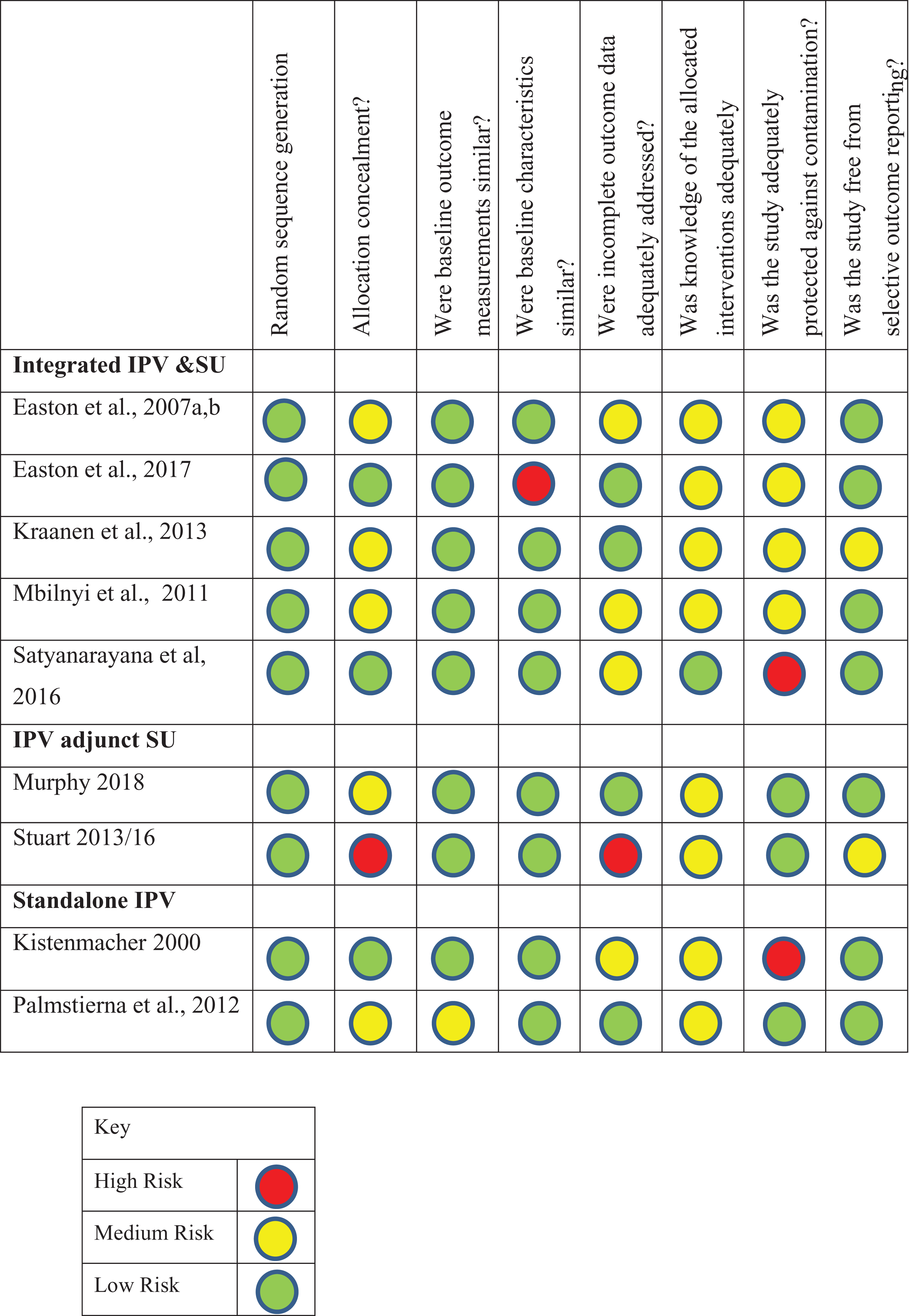
Risk of bias of included trials.
SU and IPV Outcome Measures
The timeline followback (TLFB) interview, a calendar-assisted structured interview (Fals-Stewart et al., 2000), measured SU in most trials (Easton et al., 2007a; 2007b; Easton et al., 2017; Mbilinyi et al., 2011; Murphy et al., 2018; Stuart et al., 2013). The revised Conflict Tactics Scale (CTS-2; Staus, Hamby, Boney-McCoy, & Sugarman, 1996) was used to measure IPV in all but one trial (Murphy et al., 2018). Three trials requested both female partners and male participants complete the CTS-2 (Easton et al., 2007a; 2007b; Easton et al., 2017; Kraanen et al., 2013), while one measured partners’ responses alone (Satyanarayana et al., 2016). Table 2 outlines SU- and IPV-related outcome measures and findings.
Substance Use (SU) and Intimate Partner Violence (IPV) Characteristics, Outcomes, and Findings.
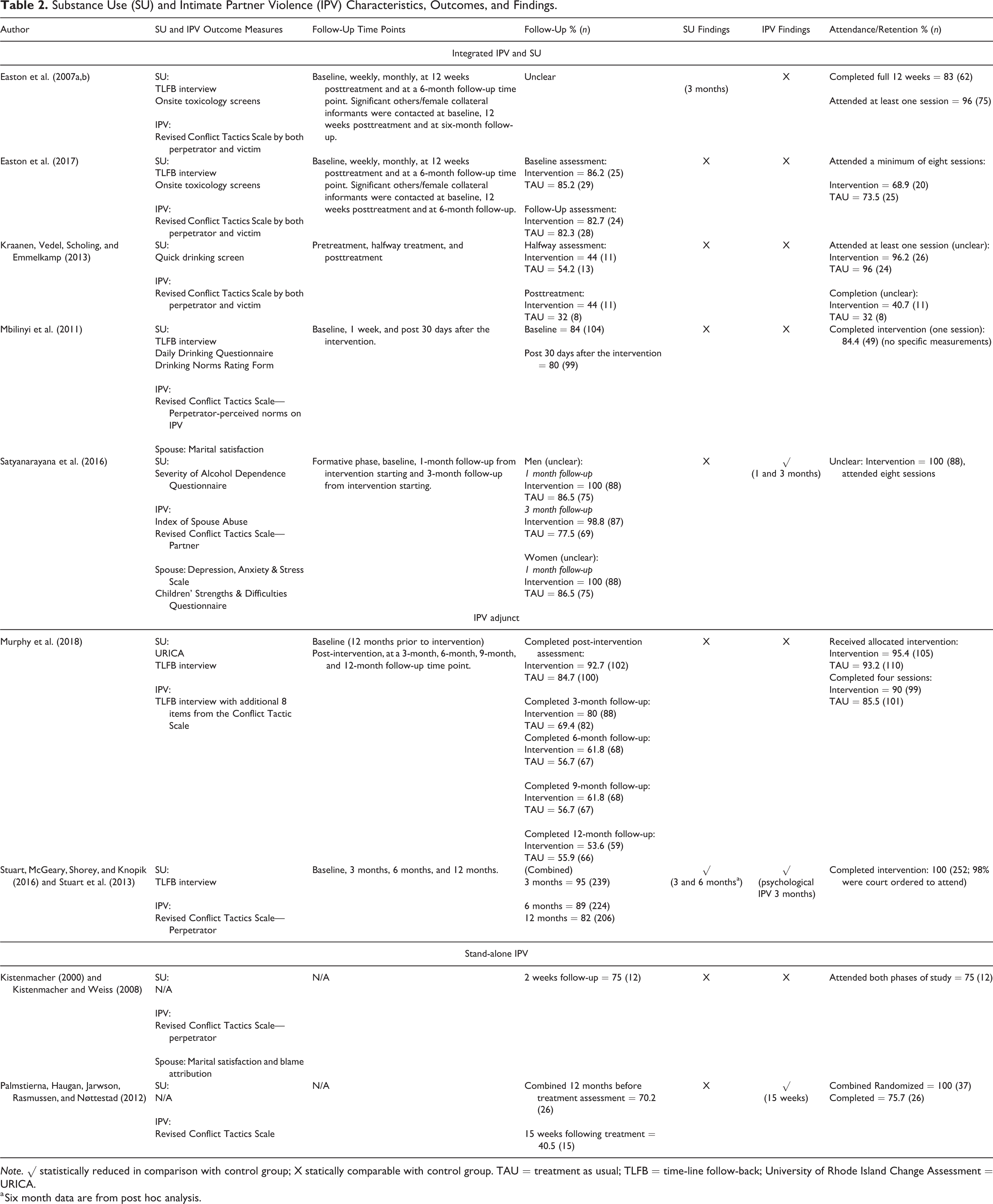
Note. √ statistically reduced in comparison with control group; X statically comparable with control group. TAU = treatment as usual; TLFB = time-line follow-back; University of Rhode Island Change Assessment = URICA.
a Six month data are from post hoc analysis.
Trial Authors’ Findings and Conclusions
Integrated IPV and SU interventions
Easton et al. (2007a; 2007b) compared a group SU TAU (12-Step Alcohol Course) with an integrated SU and IPV group intervention finding a nonstatistically significant reduction for the treatment group in the frequency of violent episodes across time than the TAU group. Furthermore, a statistically significant reduced number of self-reported days of alcohol use across the 12 weeks of treatment was found for the SADV group as compared to the TAU group (p < .02). Mean attendance for both groups was 9/12 sessions with no significant differences (p < .14). More recently, Easton, Crane, and Mandel (2018) compared individual SU TAU (CBT modified from Project MATCH; Kadden et al., 1992), with SADV delivered individually with optional couples counseling. As above, men in this study were in treatment for alcohol and/or cannabis and/or cocaine and/or opiate dependency and use. Men receiving SADV self-reported that they were less likely to engage in aggressive behavior after a drinking episode (primary outcome). Additionally, men self-reported fewer episodes of physical IPV and had fewer cocaine-positive toxicology screens and positive breathalyzer results during treatment than the drug counseling control group at a 3-month posttreatment follow-up. However, these effects were not statistically significant. Seventy-one percent across the two groups completed 8/12 of the treatments.
Comparing CBT-informed individual TAU for SU with an individual integrated IPV and SU intervention (Integrated treatment for Substance abuse and Partner violence) for men in treatment for alcohol and/or cannabis and/or cocaine abuse and dependency, Kraanen et al. (2013) reported significant reductions in both SU and IPV perpetration for men in both treatment arms posttreatment. However, no differences in outcome were found between treatment arms. Only 36.5% of participants completed 75% of treatment intervention, with no difference between the groups. Overall, the authors concluded that it was more cost-effective and efficient to implement the SU TAU rather than the intervention. Mbilinyi et al. (2011) found no statistically significant changes in any of the outcomes or differences between MI intervention and SU educational material delivered via mail. Between groups, 14% of the intervention group were lost to follow-up and one discontinued versus 9% lost to follow-up with two discontinued in the TAU group. There were no differences between groups regarding marital satisfaction, although it was unclear as to whether the perpetrator or spouse completed this measure.
Finally, Satyanaranya et al. (2016) reported that, compared with TAU (psychoeducational and pharmacological treatment for SU), the integrated cognitive behavioral intervention (ICBI) group reported significantly lower IPV perpetration at both 1- and 3-month follow-ups (p = .004, p = .005, respectively) after adjusting for baseline values, age at first drink, and baseline alcohol dependence scores. Twenty of the 177 men randomized were lost to follow-up. Alcohol consumption in the men was not significantly different between the treatment groups. Depression, anxiety, and stress scores in the spouses were significantly lower in the ICBI group at both 1- and 3-month follow-ups, compared to TAU (p = .04, p = .006, p = .01, respectively). Although preliminary, the authors concluded that findings demonstrated the feasibility and effectiveness of an integrated SU and IPV intervention with an alcohol-dependent population.
IPV intervention with adjunctive SU intervention
Murphy et al. (2018) compared four individual MI sessions followed by a standard IPV program with TAU (IPV program) with four additional SU educational sessions. A significant reduction in alcohol-abstinent days, percentage of heavy drinking days, percentage of illicit drug use, and percentage of partner violence were reported for men in both treatment arms at 12-month follow-up. However, no significant Treatment × Time interaction was found. The authors reported good adherence for both the intervention and control arms (completed 99/110 vs. randomized 101/118). Similarly, Stuart et al. (2013) compared a standard IPV program plus a 90-min brief alcohol intervention with TAU (IPV program). Those in the treatment arm reported consuming fewer drinks per drinking day at 3-month follow-up (p = .04) but not at 6-month follow-up using repeated measure analyses. Adherence to intervention was found to be good at 3 and 6 months but dropped off at 12 months and more so in the intervention compared with the TAU group (completed 95/123 vs. randomized 112/129). In a post hoc analysis, men receiving the intervention reported greater abstinence from alcohol at 3 and 6 months post randomization (p = .002, p = .01, respectively), less severe psychological aggression and fewer injuries to partners at 3- and 6-month follow-up (p = .04, p = .03). However, there were no significant differences in physical IPV between the groups and no statistically significant differences at 12 months for any outcome in any analysis. Thus, it was concluded that while a brief alcohol intervention could show promise in improving alcohol and IPV outcomes, this was limited in duration.
Stand-alone IPV interventions
For both trials (Kistenmacher, 2000; Palmstierna et al., 2012), around 70% of the men used substances. There were no separate data presented for SUs versus non-SUs. Kistenmacher (2000) compared a group IPV program with a no treatment control group, with no difference in IPV recidivism reported between the groups at the 6-month follow-up (p = .47) or on a self-report measure of motivation to change violent behavior (p = .8). Completion rates were 94% of controls compared to 75% in the intervention group (p = .18). Men in this trial reported dependence or abuse of alcohol and/or cocaine and/or cannabis.
Finally, comparing an individual plus group IPV intervention with individual IPV plus wait-list control, Palmstierna et al. (2012) reported that the intervention group improved in terms of IPV measured as physical violence, verbal aggression, and material violence at 15 weeks (p < .001) when compared with the control group. Dropout rates were similar between intervention and control groups. Authors from both trials concluded positive findings for MI (Kistenmacher, 2000) and CBT (Palmstierna et al., 2012) but with a need for further replication with larger samples.
Statistical Power
Of the nine trials, five included sample sizes of less than n = 75 (range N = 26 –252), resulting in a lack of power to determine effectiveness. One trial was a pilot (Easton et al., 2007a; 2007b), four trials did not report a power calculation (Easton et al., 2017; Satyanarayana et al., 2016), although two acknowledged a small sample size (Kistenmacher, 2000; Palmstierna et al., 2012). Four trials reported power calculations (Kraanen et al., 2013; Mbilinyi et al., 2011), although two did not reach recruitment targets (Murphy et al., 2018; Stuart et al., 2013).
Meta-Analysis
The data were limited for meta-analysis due to the heterogeneity of the interventions included in the review and the variations across control groups. Five trials either did not report appropriate or combinable outcome data for analysis. Data were examined for IPV and SU outcomes for the remaining four trials in the integrated IPV and SU interventions group (Easton et al., 2007a; 2007b; Easton et al., 2017; Kraanen et al., 2013; Mbilinyi et al., 2011). There was a lack of precision of estimates (i.e., wide confidence intervals [CIs]) as reflected in the meta-analysis results and I2 heterogeneity measures.
Integrated IPV and SU interventions
SU outcomes
Data on SU from three of the integrated trials were combined (Easton et al., 2007a; 2007b; Easton et al., 2017; Kraanen et al., 2013). Data for abstinence from drug use and alcohol use at 12 weeks were available for two of the trials (Easton et al., 2007a; 2007b; Easton et al., 2017). Neither drug nor alcohol abstinence was statistically significantly different (mean difference [MD] = 3.74, CI [−0.10, 7.58], p = .06, I2 = 59%, MD = 3.38 [−0.867, 15.41], p = .58, I2 = 87%, respectively; Figure 3Bi). Data from all three trials were combined for abstinence from overall SU at 8–12 weeks and did not show a statistically significant effect in favor of the integrated interventions, rather a direction of effect in favor of the SU TAU group was found (MD = 2.07, CI [0.00, 4.13], p = .05, I2 = 0%). However, it is important to note that this analysis was dominated by one trial as illustrated by the 0% heterogeneity (Easton et al., 2017; Figure 3Aii). One trial used the outcome measure of substance dependency and showed no difference between groups at the final end point of 12 weeks (MD = −0.80, CI [−3.55, 1.95] p = .57; Figure 3Aiii) These meta-analyses reflect the individual data from the five trials presented above in which only one trial (Satyanarayana et al., 2016) had a statistically significant effect on alcohol use. However, it was considered important to combine the data available to provide a directional overview of the interventions’ effectiveness.
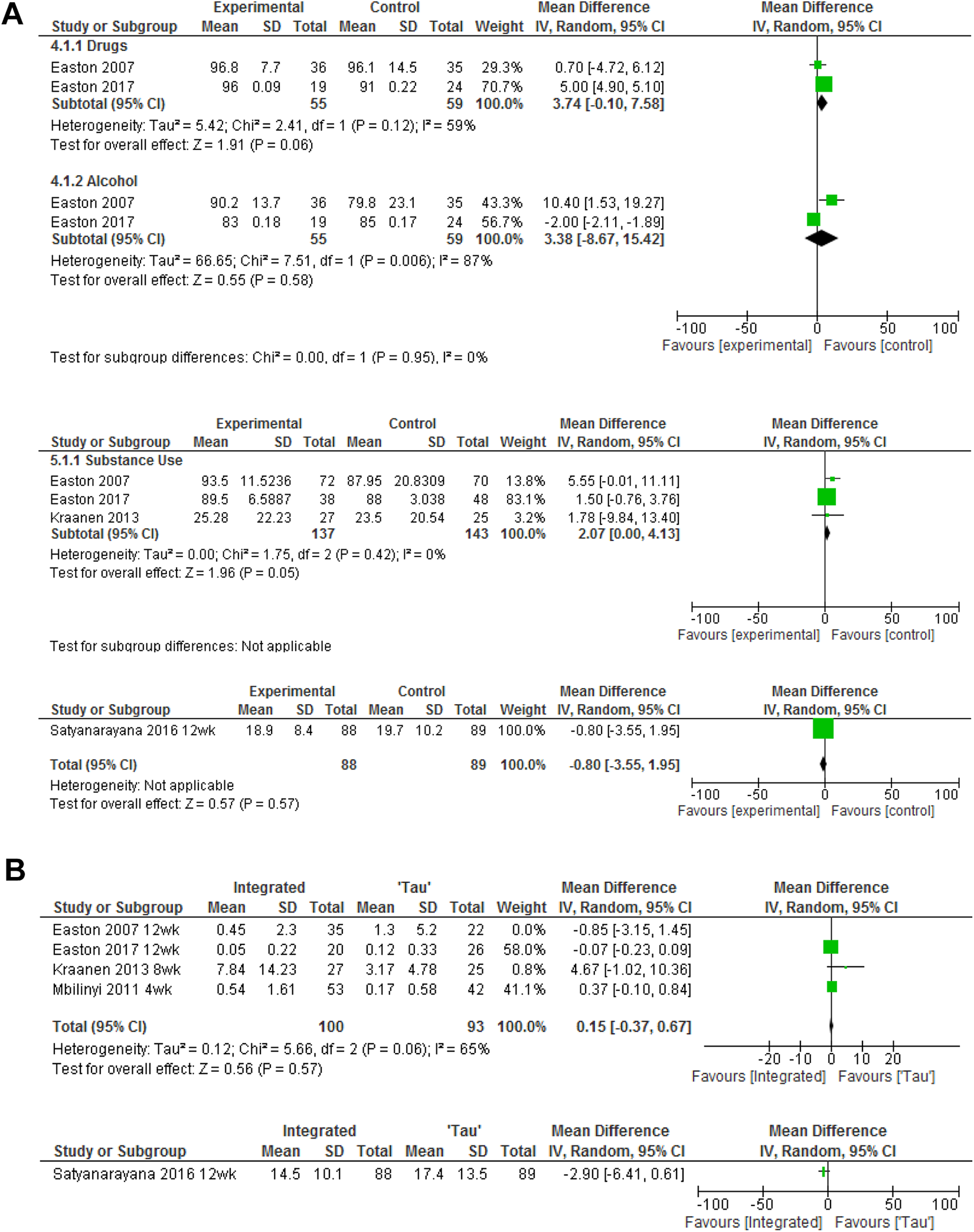
(A) Substance use (SU) analysis. (i) Abstinence from drug use and alcohol use at 12 weeks. (ii) Abstinence from overall SU. (iii) SU outcome–dependency. (B) IPV analysis. (i) IPV as measured by CTS-2. (ii) IPV–outcomes–ISA.
IPV Outcomes
Data from the CTS-2 physical violence subscale were combined from four of the five trials at 4–12 weeks data points using mean and standard deviations to produce an MD for each (Easton et al., 2007a; 2007b; Easton et al., 2017; Kraanen et al., 2013; Mbilinyi et al., 2011). It is of note that this analysis was subject to moderate heterogeneity (I2 = 51%). The combined MD was 0.1 (CI [−0.37, 0.57], p = .68; Figure 3Bi). One trial (Satyanarayana et al., 2016) used the outcome measure of incidence of spousal abuse (Hudson & McIntosh, 1981). Although the intervention group demonstrated significantly lower IPV perpetration at both 1- and 3-month follow-ups compared to the control group (p = .004, p = .005, respectively), there was no statistically significant difference at the final end point of 12 weeks (MD = −2.90, CI [6.41, 0.61]; Satyanarayana et al., 2016; Figure 3Bii).
Discussion
Overall, the results of a small number of individual trials demonstrated some reductions in SU and IPV outcomes in the short term. However, meta-analysis of four trials showed no statistically significant differences between integrated interventions and their SU TAU groups. There were insufficient data to conduct meta-analysis for the other two intervention group types (IPV interventions with adjunct SU interventions and stand-alone IPV interventions). Thus, it is difficult to address the objectives of this review in determining the effectiveness of intervention in reducing IPV perpetration by men in SU treatment. That said, this review does indicate some important factors for future trials targeting IPV perpetration by those who use substances.
Although a variety of outcome measures were used in the trials, the CTS-2 was used to assess IPV in eight of the included trials and embedded within the TLFB approach for one trial (Murphy et al., 2018). While this was predominantly completed by the perpetrator, current or ex-partners also completed the CTS-2 in four trials. However, within their measurement of IPV, many of the trials remained focused on physical forms of IPV, often failing to account for coercive control (defined as an “act or a pattern of acts of assault, threats, humiliation and intimidation or other abuse that is used to harm, punish, or frighten their victim,” Section 76 of the Serious Crime Act, 2015) and other forms of abuse. Conversely, for SU, outcome measures adopted were variable across trials with some covering pattern of use and/or abstinence. While all the trials recruited users of different substances, including alcohol, cannabis, cocaine, and opiates, and reported numbers using some substance types, no results were reported for substances used nor was there any differentiation provided in relation to the severity of use by participants (i.e., dependency, hazardous, abuse). Additionally, none of the trials detailed the relationship between the IPV and SU within their populations. As such, it was impossible to evaluate the relationship between the substances used and type of violence. Furthermore, it is difficult to make sophisticated and meaningful comparisons between trials in gauging the effectiveness of both integrated and stand-alone interventions in reducing SU. Additionally, while physical IPV must be considered, it is necessary to draw on appropriate measures capturing the more nuanced aspect of violence and abuse, including psychological and coercive control (Gilchrist et al., 2019).
The trials were conducted with low risk of bias, although there was heterogeneity in the population recruited, intervention delivered, duration and intensity, as well as the availability of combinable data. It is important to note that men in the TAU groups in the integrated IPV and SU trials were all receiving help for their SU, thus results should be interpreted with caution. A further issue was the small sample size in a number of the trials possibly resulting in the underpowering of most of the trials. Trials were further weakened by the levels of adherence to treatment and follow-up attrition. Nonetheless, the trials provided reasonable descriptions surrounding attendance, with similar attendance between treatment arms. However, nearly half (n = 4) of the trials did not explain how their analysis accounted for attrition or session attendance.
Future Trial Recommendations
Considering the inconclusive results surrounding the effectiveness of IPV interventions in the trials reviewed, recommendations for practical development can only be tenuous. The nine trials recruited a number of men from an array of settings, with a number of different substances recorded. Additionally, in terms of mental health, a number of trials excluded potential participants due to mental health diagnoses (n = 5). In terms of future progression, it is important that IPV and SU interventions consider what works best for whom. Research has demonstrated variability in associations between SU and IPV perpetration across differing substances. For example, while a strong association has been found between alcohol and/or cocaine use and IPV (Cafferky et al., 2018; Smith, Homish, Leonard, & Cornelius, 2011; Stith, Smith, Penn, Ward, & Tritt, 2004), associations have been noted when considering cannabis and/or opioid use or polydrug use. As such, the type of substances used, and the level of use (dependence, abuse, hazardous), need to be clearly defined and measured. Such considerations will enable interventions to be designed to clearly address treatment needs and tailor these in relation to individual factors such as specific substances used, mental health, and demographic factors. Future trials must also incorporate measures accessing the multifaceted nature of abuse in relationships. In addition to physical IPV, it is essential that outcome measures include instruments accounting for other nuanced forms of abuse (including coercive control; G. Gilchrist & Hegarty, 2017). This is particularly important when considering the complex nature of substance-using relationships (Gadd et al., 2019; G. Gilchrist et al., 2019). Additionally, such measures would be best administered to both perpetrators and their current or ex-partners to strengthen overall validity from corroborated evidence around abuse (Capaldi & Langhinrichsen-Rohling, 2012). As a result, the integration of support services to ensure victims’ safety is paramount (Capaldi & Langhinrichsen-Rohling, 2012). Overall, considering the substances used by perpetrators, their level of use and type of perpetration will enable a more complex understanding of the relationship between these factors as well as the treatment needs of those seeking support (Gadd et al., 2019).
The five integrated intervention trials and the one IPV with adjunct SU intervention predominantly utilize CBT and MI approaches. While research suggests that CBT and MI are suitable for this population, there needs to be focus on how integrated interventions can be delivered to best draw on the benefit of these approaches (Crane & Easton, 2017; Lila, Gracia, & Catalá-Miñana, 2018). One issue in need of research is the optimum duration of interventions. The current trials were, on average, 12 weeks in duration, but there was attenuation of positive treatment effect at follow-up. Research has indicated limitations with the brevity of MI sessions, suggesting more intensive MI interventions should be undertaken to develop participant engagement in addition to motivation for change (Scott, King, & McGinn, 2011). Furthermore, future trials need to extend the follow-up period to examine the duration of outcomes and, potentially, any delayed effects.
Overall, not only are there a lack of referral pathways available for male perpetrators of IPV who use substances (Radcliffe & Gilchrist, 2016), treatment adherence and outcomes are significantly poorer for substance-using men who are referred to stand-alone IPV interventions (Eckhardt, Samper, & Murphy, 2008; Klostermann, 2006; Timko et al., 2012). Given this, it would be prudent and more efficient to develop a theoretically integrated SU and IPV intervention, delivered within an SU setting and facilitated by highly trained substance treatment staff (Timko et al., 2012). It is imperative, however, that such an intervention incorporates an accessible model tailored to the complex needs of substance-using men who perpetrate IPV (E. Gilchrist et al., 2003).
Strengths and Limitations
This is the first systematic review and meta-analysis to consider efficacy of IPV interventions for men who use substances. We used a high-quality methodology with additional input from experts in both the IPV and SU fields. The statistical and narrative analysis of the trials can inform future trials in this area.
The main limitation is the low number of trials identified and the still lower number suitable for inclusion in the meta-analysis. There was heterogeneity in terms of the interventions studied as well as differences in comparison groups, delivery approach, length of follow-up, and assessment methods in determining IPV and SU behaviors. A further limitation is that two authors were not contactable to determine whether they could provide the appropriate data needed in completing the meta-analysis. This is a potential source of bias.
Conclusions
There is very little evidence for interventions for substance-using men who perpetrate IPV both in terms of number of trials and the useable data from the current trials for meta-analysis. Individual trials report improvements for men with SU and IPV perpetration in the short term, but meta-analysis showed no statistically significant differences between interventions and their comparison groups. There is a need to develop and evaluate evidence-based interventions for men who use substances and abuse their partners. Overall, the matters requiring attention are (1) the theory, content, mode of delivery, and duration of interventions; (2) the characteristics of the individuals requiring treatment, including the types of substances used, the type of abuse perpetrated, and the nature of the relationship between SU and abuse perpetration; and (3) what outcomes are assessed, where the information is sourced, and the duration of follow-up.
Footnotes
Authors’ Note
The views expressed in this publication are those of the authors and not necessarily those of the National Health Service, the National Institute for Health Research, or the Department of Health. The authors, Dr. Gail Gilchrist, Dr. Polly Radcliffe, Professor David Gadd, Professor Liz Gilchrist, Professor Mary McMurran, Professor Gene Feder, Sara Kirkpatrick, Professor Louise Howard, Professor Sir John Strang, Professor Sabine Landau, Professor Caroline Easton, Steve Parrott, and Eleanor Bateman, submit this publication on behalf of the ADVANCE research program investigators.
Danielle Stephens-Lewis is also affiliated with School of Natural and Social Sciences, University of Gloucestershire. Elizabeth Gilchrist and Amy Johnson are also affiliated with University of Edinburgh, Edinburgh.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This manuscript summarizes independent research funded by the National Institute for Health Research under its Programme Grants for Applied Research program (RP-PG-1214-20009).