
Abstract
Aims:
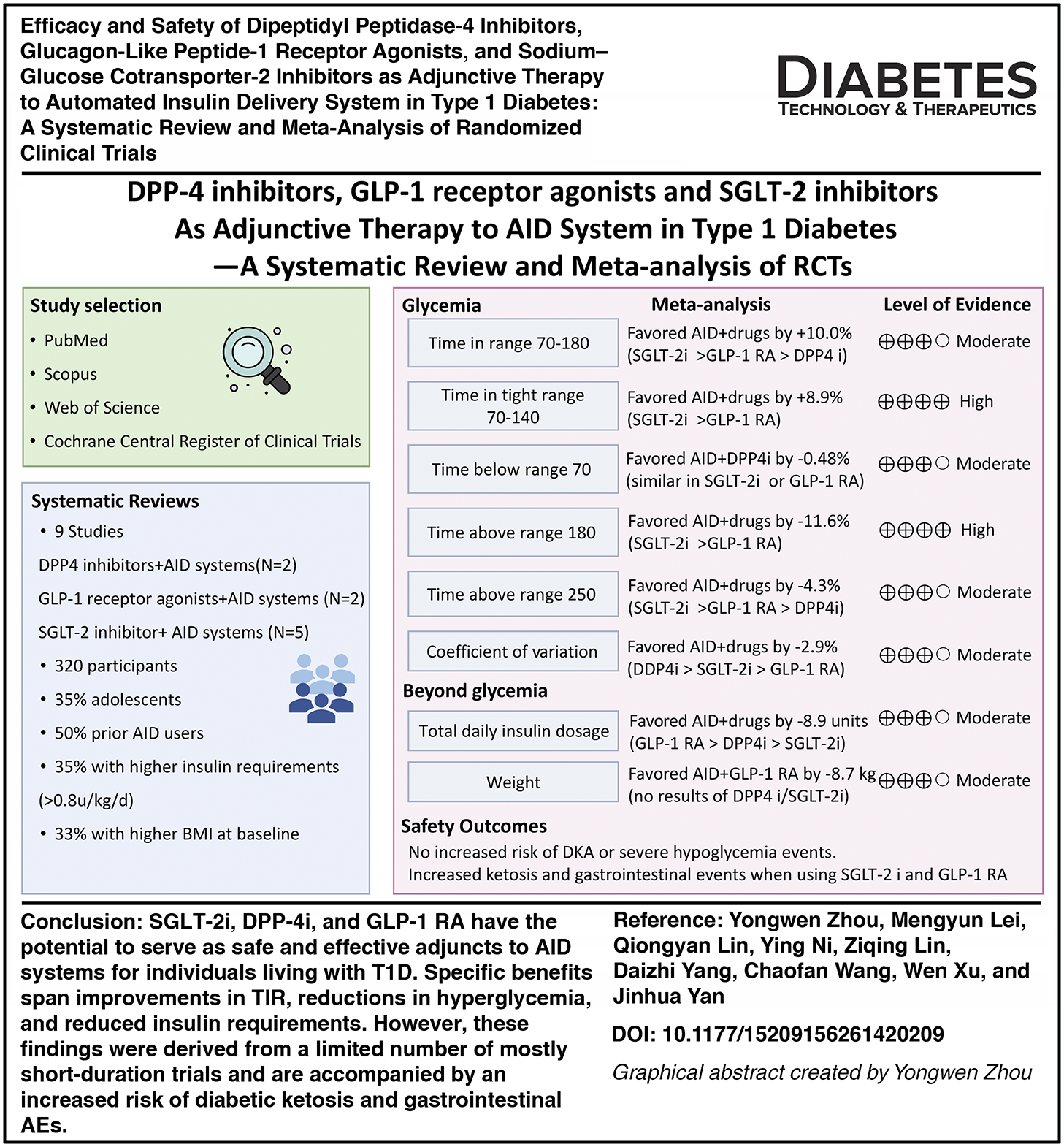
The efficacy of adding various noninsulin hypoglycemic drugs to automated insulin delivery (AID) systems in patients with type 1 diabetes (T1D) was investigated in randomized controlled trials (RCTs), yet no meta-analysis has been conducted. This study aimed to systematically analyze the existing evidence.
Methods:
Four datasets were searched up to August 31, 2025. Inclusion criteria were as follows: T1D populations of any age; comparing any type of noninsulin hypoglycemic drug added to AID systems or not; and reporting primary outcomes (time in range [TIR] = 70–180 mg/dL, 3.9–10.0 mmol/L). Results were pooled using a random-effect meta-analysis. Risk of bias was assessed using the Cochrane RoB2 tool. Quality of evidence was assessed by the Grading of Recommendations Assessment, Development, and Evaluation approach (Registered number: CRD420251107996).
Results:
Nine RCTs met the inclusion criteria, investigating sodium–glucose cotransporter-2 inhibitor (SGLT-2i) (N = 5), glucagon-like peptide-1 receptor agonist (GLP-1 RA) (N = 2), and dipeptidyl peptidase-4 inhibitor (DPP-4i) (N = 2), respectively. Overall, these drugs with AID systems improved TIR by +10.0% (7.4%–12.6%) and time in tight range (TITR; 70–140 mg/dL, 3.9–7.8 mmol/L) by +8.9% (6.8%–11.0%) with I2 of 60.4% and 15.4% (P < 0.001). These improvements were primarily driven by reductions in time above range (TAR) >250 mg/dL (>13.9 mmol/L; −4.3 [−5.8 to −2.8] %), TAR >180 mg/dL (>10.0 mmol/L; −11.6 [−14.7 to −8.5] %), and coefficient of variation (−2.9 [−4.5 to −1.4] %) without increased hypoglycemia. Daily insulin dose decreased by 8.9 units. Among these, SGLT-2i conferred the greatest TIR improvement (+12.5%), followed by GLP-1 RA (+7.1%) and DPP-4i (+6.4%). No significant differences were found in severe hypoglycemia (SH) and diabetic ketoacidosis (DKA).
Conclusions:
SGLT-2i, DPP-4i, and GLP-1 RA may serve as effective and safe adjuncts for T1D individuals using AID systems, offering improvements in TIR, reductions in hyperglycemia, and reduced insulin requirements without evidence of increasing DKA and SH.
Get full access to this article
View all access options for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.