
Abstract
Rates of reoffending among forensic patients discharged from secure hospital care are known to be low, but comparatively little is known about contact with health services after discharge. This study describes the patterns and correlates of health service contact among discharged Forensic Patients in New South Wales (NSW), Australia. Records of Emergency Department (ED) presentations, hospital admissions, and ambulatory mental health care were linked to the records of the 227 Forensic Patients. Two thirds of the sample had contact with ambulatory mental health services within a month of discharge, and most (81.5%) presented to an ED or were admitted to a hospital during the study period. Factors associated with earlier hospital contact included being of English-speaking background, anti-social personality traits, and having a non-homicide related index offence. Predictors of ambulatory mental health contact within one month included prior contact with mental health services, non-homicide related index offence, prior criminal charges, and co-morbid substance use disorder. Early and continued engagement with community mental health services is an important component of community forensic mental health care. The high rate of hospital admission in the sample may reflect the assertive follow-up received by most Forensic Patients through proactive engagement with mental health services and the low tolerance for signs of relapse.
Introduction
Most jurisdictions have provisions for the diversion of people with severe mental illness who have been found to have reduced criminal responsibility for serious offences. In New South Wales (NSW), Australia, those diverted to secure hospital care are known as Forensic Patients. Most Forensic Patients have a persistent psychotic illness, such as schizophrenia, which typically requires long-term adherence to antipsychotic medication. Comorbid conditions such as intellectual disability, acquired brain injury, substance use disorder and personality disorder are also common (Dean et al., 2021; Völlm et al., 2017), as are co-existing physical health conditions (Justice Health and Forensic Mental Health Network, 2016; Sweeney et al., 2015; Völlm et al., 2017). Forensic Patients are known to have higher rates of premature mortality and suicide (Fazel, Fiminska et al., 2016; Tabita et al., 2012).
Forensic Patients discharged from secure care to the community in NSW have been found to have low rates of reoffending compared to reported rates for those released from prison following a custodial sentence (Dean et al., 2021; Nielssen et al., 2019). The relatively low rate of post-discharge reoffending is likely to be due to the effective treatment of the mental illnesses that contributed to the original offending, along with interventions aimed at addressing psycho-social needs and identified risk factors. Most Forensic Patients who are conditionally released have had an extended period of graduated leave to the community prior to discharge, so that they are already well engaged with community treatment and service providers. Treatment and psycho-social interventions continue post-discharge, with Forensic Patients on conditional release orders required to engage with treatment and support. These requirements may include regular contact with community-based mental health services, residing in approved accommodation, supervision of adherence to medication and abstinence from substances. The level of supervision required is determined on a case-by-case basis, depending on individual needs and risk factors. Patients are typically managed by community mental health agencies using a standard case management model, with patients referred to other services for support where needed. In NSW, it is rare for a Forensic Patient to be unconditionally released without first progressing through conditional release (Lyons et al., 2022). However, there are comparatively few published studies reporting the extent to which Forensic Patients take up community-based mental health care following discharge.
Given the chronic nature of the mental illnesses typically experienced by Forensic Patients, some emergency health service contact and rehospitalization in the post-discharge period is to be expected. Emergency service contact may indicate early recognition of a deterioration in mental health and an increased risk of poor outcomes, including reoffending (Jewell et al., 2018). Early return to hospital may indicate a failure of community-based treatment of mental illness, as well as a low tolerance for relapse or non-adherence to conditions of release. Published rates of rehospitalization for discharged Forensic Patients vary from as low as 5% (Blattner & Dolan, 2009) to as high as 80% (Skipworth et al., 2006). A systematic review of 20 studies examining 21 individual cohorts discharged from secure psychiatric hospitals reported a pooled psychiatric readmission rate of 7,208 per 100,000 person years (95% CI 5 916-8,500, range 2,926 to 16,461) (Fazel, Fiminska et al., 2016), with the high heterogeneity between studies attributed to differences in the length of follow-up, the intensity of community support and thresholds for rehospitalization. Factors associated with rehospitalization reported in the literature include a primary diagnosis of schizophrenia (Fazel, Wolf et al., 2016), co-morbid substance use disorder (Fazel, Wolf et al., 2016; Green et al., 2014; Penney et al., 2018; Takeda et al., 2019), a history of psychiatric admissions prior to the index offence (Jewell et al., 2018) and the presence of residual symptoms of mental illness at the time of discharge (Hayes et al., 2014). Non-clinical factors include younger age, ethnicity, early childhood maladjustment (Jewell et al., 2018), offending or arrest after discharge from secure care (Alexander et al., 2006; Marshall et al., 2014), and being in independent rather than supported housing (Salem et al., 2015).
Less attention has been paid to patterns of contact with other types of health services, including Emergency Department (ED) presentations and contact with outpatient (or community) mental health services. People with mental illness released from prison have high rates of ED contact (Frank et al., 2013) but patterns of ED contact for discharged Forensic Patients have not been examined. Forensic Patients would be expected to have early and regular contact with community mental health services, as conditions of discharge typically include ongoing treatment, and any gap may reflect an inadequate level of care or avoidance of engagement on the part of the patient. There is evidence that receiving community-based care results in better outcomes for people with severe mental illnesses who are in contact with the criminal justice system. A randomized trial of a forensic community treatment program in California, for example, found that those who completed the program had a greater number of outpatient contacts and fewer days in hospital compared to a control group (Cusack et al., 2010). Comparable findings were reported for another study based in New York, where fewer criminal convictions were seen in the group participating in the community treatment program (Lamberti et al., 2017). Similarly, a study from Russia found that most of the recidivist homicides by people with schizophrenia took place in rural areas where outpatient care was less available (Golenkov et al., 2013).
The aim of the current study is to report on rates of contact with inpatient, emergency and community-based services in a cohort of Forensic Patients discharged from secure care in NSW. A secondary aim is to examine factors associated with post-discharge health service contact that may indicate a poor outcome, indicated by (a) early post-discharge hospital-based contact (i.e., inpatient or emergency) and (b) the absence of early post-discharge community-based mental health contact.
Methods
Sampling and Data Linkage
The NSW Mental Health Review Tribunal (MHRT) is responsible for deciding the placement, treatment and discharge of Forensic Patients. 1 Data was extracted from the NSW MHRT electronic records and paper case files on 477 Forensic Patients who received a Not Guilty by reason of Mental Illness (NGMI) verdict in NSW between 1 January 1990 and 29 July 2016. This included demographic, clinical, criminal justice and administrative data for the sample, which has been described elsewhere (Dean et al., 2021). The MHRT's electronic database was used to identify the 227 patients who had been granted conditional or unconditional discharge prior to 30th November 2017. Conditional discharge typically includes the requirement to live in an approved location, take prescribed medication, abstain from alcohol or drugs, have regular drug tests, attend appointments with case managers and a treating psychiatrist and not travel out of the State without approval.
Health service contact in the post-discharge period was established by linking the discharged cohort to several statewide administrative health datasets. The NSW Admitted Patient Data Collection (APDC) contains records from all NSW public, private, psychiatric and veterans’ hospitals in NSW from 1 January 2001 until 31 December 2018. Hospital admissions are recorded as ‘episodes of care’ which end with either discharge, transfer or death. Admissions with any principal diagnosis type and mental or behavioural disorder diagnoses according to the ICD-10-AM were examined. The NSW Emergency Department Data Collection (EDDC) contains information on ED presentations at most NSW public hospitals between 1 January 2005 and 31 December 2018. The principal diagnosis associated with the presentation was classified according to the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9CM), International Classification of Diseases, 10th Revision, Australian Modification (ICD-10AM) or SNOMED CT coding systems. ICD-9CM and SNOMED CT codes were mapped to the corresponding ICD-10AM codes. Two categories of diagnosis were examined – ED presentations for any reason and presentations with a primary diagnosis of mental or behavioural disorder (ICD10-AM Chapter V diagnosis, codes F00-F99). The NSW Mental Health Ambulatory Data Collection (MH-AMB) contains information on the assessment, treatment and rehabilitation service use of mental health outpatients from 1 January 2001 until 30 June 2018. This includes mental health day programs, psychiatric outpatient services, substance use services and outreach community mental health services. Each activity recorded in the dataset is assigned a unique Service Event ID that links together individual activities performed within a single mental health service contact. The follow-up period was defined as the time from initial release to the end of the linked health dataset collection period, resulting in wide variation.
Record linkage of the cohort members to the health datasets was independently conducted by the NSW Centre for Health Record Linkage (CheReL). Identifying information for cohort members, including names, aliases, dates of birth and sex, was provided by the data custodians of the MHRT data to the CheReL to enable linkage to the datasets, based on probabilistic methodology. The health datasets and the original MHRT dataset were then returned with identifying information removed and each cohort member allocated a unique Person-specific Project Number (PPN). The health datasets were then merged with the MHRT dataset using the PPN's to allow for analysis of de-identified data.
Statistical Analysis
Statistical analysis was conducted using Statistical Package for the Social Sciences (SPSS) version 25. Descriptive statistics were generated to provide an overview of the sample characteristics and to establish the pattern of patients’ health contacts following discharge from secure care, the time between discharge and first contact, and the median number of post-discharge contacts per patient.
A combined outcome variable was created to indicate any post-discharge hospital-based contacts. Demographic, clinical and criminal justice characteristics of patients with any post-discharge hospital-based contact (i.e., recorded in the APDC or EDDC) were then compared to those without any post-discharge contacts. Cox proportional hazards regression was conducted for this purpose. Incidence rates of hospital-based contact per 100 person-years, Hazard Ratios (HR) and the relevant 95% confidence intervals (CI) were calculated. Cell sizes less than five were not reported to minimize the risk of re-identification.
A conservative definition of an expected level of contact with an ambulatory mental health service within one month of discharge was adopted. Univariate logistic regression analysis was used to determine the demographic, clinical and criminal justice factors associated with post-discharge health service contact. Odds ratios (OR) and 95% CI were reported to assess the magnitude and precision of the associations, with p-values of less than 0.05 considered statistically significant.
Ethical Approval
Approval for this study was obtained from the NSW Population and Health Services Research Ethics Committee (AU RED Reference: HREC/18/CIPHS/48; Cancer Institute NSW Reference: 2018HRE1003) and the Aboriginal Health and Medical Research Council (reference no. 1749/20). A waiver of consent was provided by the ethics committee in accordance with the criteria specified in the National Statement on Ethical Conduct in Human Research (2023). A waiver was granted as the research carried no more than low risk to participants, it was impracticable to obtain consent from individual participants given the large sample size, and the data was de-identified to protect participant privacy.
Results
Sample Overview
Table 1 describes the sociodemographic, clinical and criminal justice characteristics of the 227 Forensic Patients included in the final sample. Most were male (n = 185, 81.5%), did not identify as Aboriginal and/or Torres Strait Islander (n = 204, 89.9%) and spoke English as their first language (n = 162, 71.4%). Almost half of the sample (n = 95, 44.6%) had a history of trauma or neglect in childhood. The most common primary diagnoses were schizophrenia related disorders (n = 179, 78.9%). Most patients (n = 184, 81.1%) had contact with mental health services prior to the index offence and a little over half of the sample (n = 124, 54.6%) had a criminal charge recorded prior to the index offence.
Sample Characteristics (N = 227).
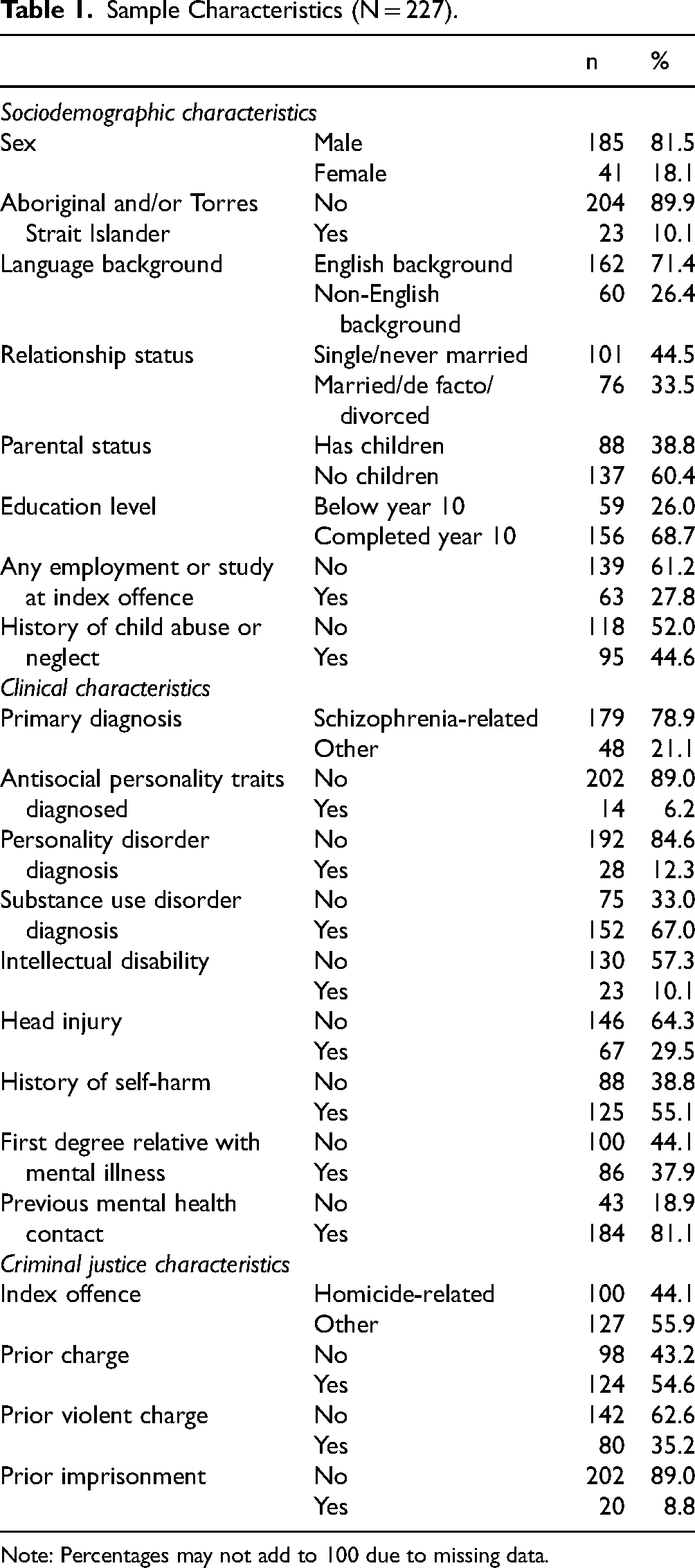
Note: Percentages may not add to 100 due to missing data.
Hospital Admissions
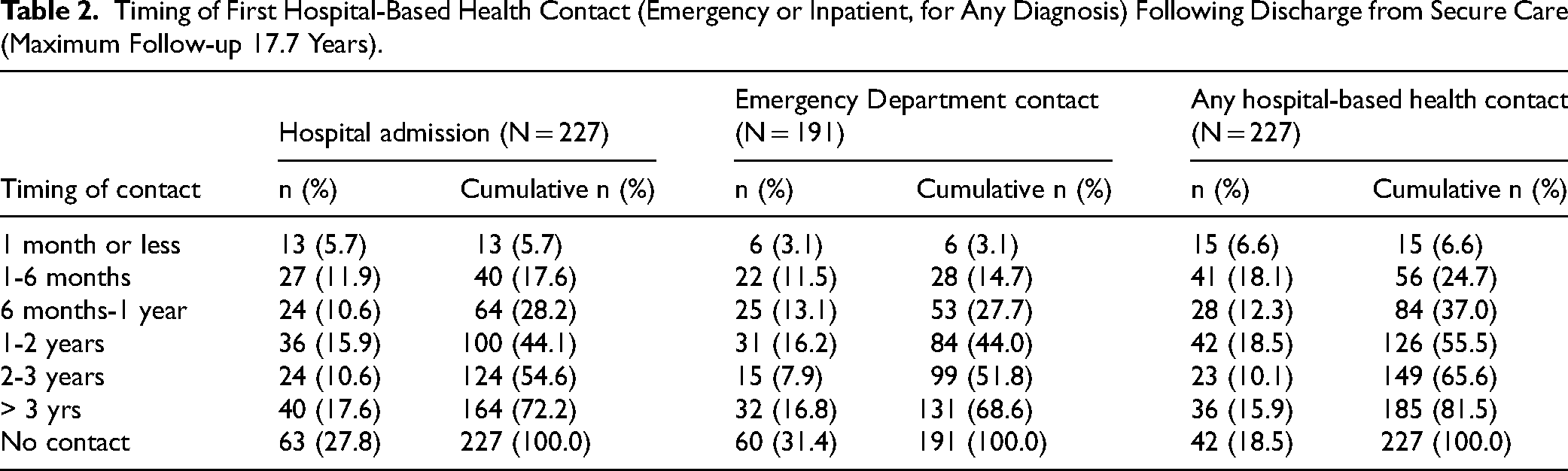
A total of 227 Forensic Patients were discharged from secure care following the APDC data availability start date (i.e., 1 January 2001). At the point of first discharge, eight patients (3.6%) were discharged without conditions, while the remaining 219 patients were conditionally released. More than a quarter (n = 64, 28.2%) had at least one hospital admission for any reason within the first year after discharge, and nearly three quarters (n = 164, 72.2%) had at least one hospital admission by the end of the follow-up period (Table 2). The mean number of post-discharge hospital admissions per patient was 6.4 (sd = 7.6, range = 1-47). The most common reason for the admission was mental and behavioural disorder (n = 77, 47.0%), followed by injury, accidents and poisoning (n = 17, 10.4%) (Table 3).
Timing of First Hospital-Based Health Contact (Emergency or Inpatient, for Any Diagnosis) Following Discharge from Secure Care (Maximum Follow-up 17.7 Years).
Principal Diagnosis Recorded at the First Post-Discharge Hospital-Based Contact for Any Reason.
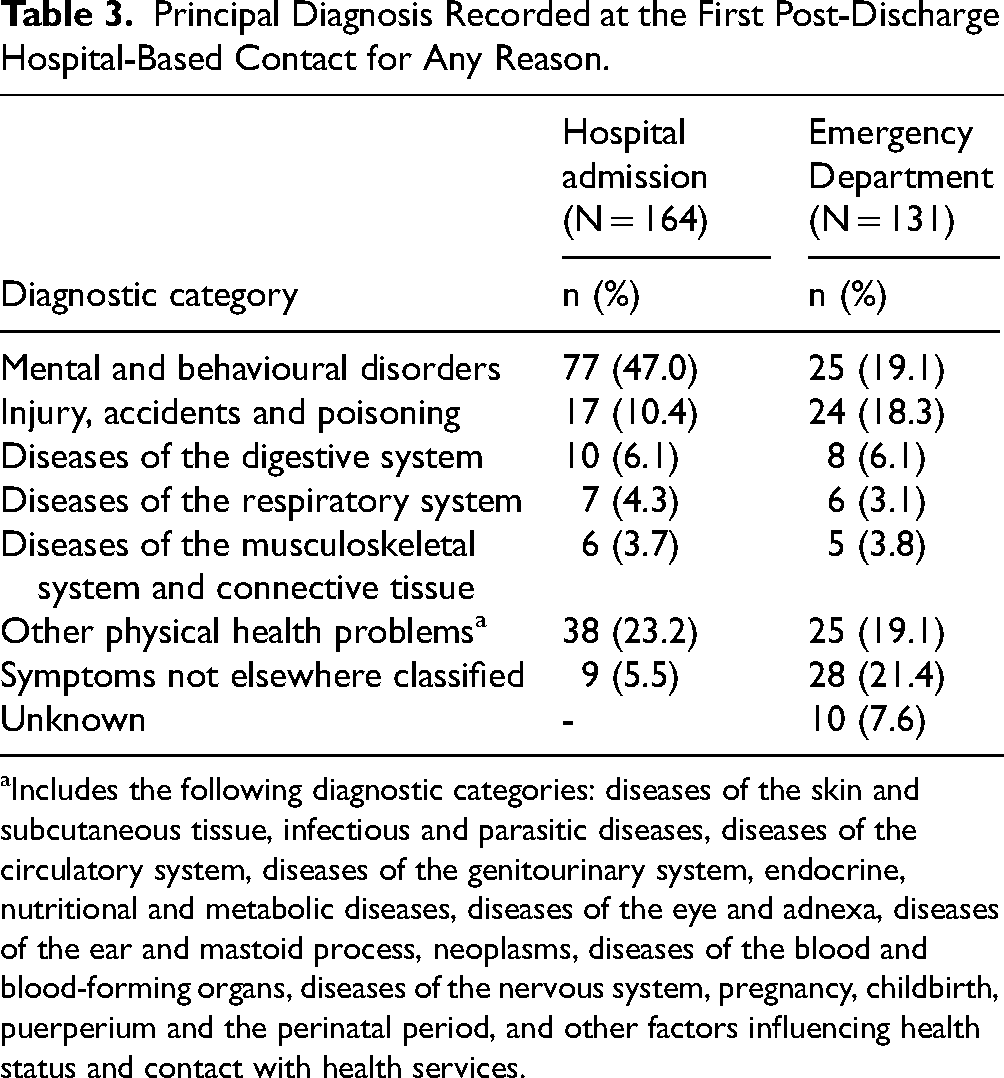
Includes the following diagnostic categories: diseases of the skin and subcutaneous tissue, infectious and parasitic diseases, diseases of the circulatory system, diseases of the genitourinary system, endocrine, nutritional and metabolic diseases, diseases of the eye and adnexa, diseases of the ear and mastoid process, neoplasms, diseases of the blood and blood-forming organs, diseases of the nervous system, pregnancy, childbirth, puerperium and the perinatal period, and other factors influencing health status and contact with health services.
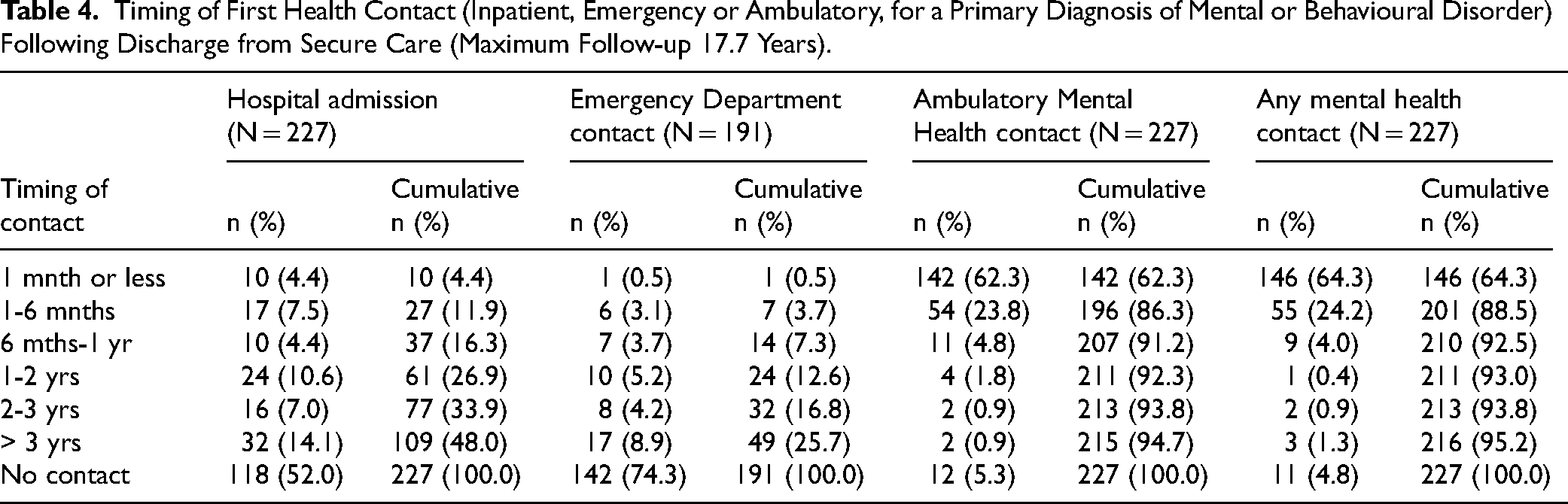
About half of those discharged were admitted to hospital for a mental health condition at some point during the follow-up period (n = 109, 48.0%;), with 16.3% of all discharged patients (n = 37) having a mental health-related admission within a year of discharge (Table 4). The mean number of psychiatric hospital admissions was 4.5 (sd = 5.4, range = 1-45). Not surprisingly, most of the first post-discharge contacts were for treatment of a schizophrenia-related condition (n = 78, 71.6%) (Table 5).
Timing of First Health Contact (Inpatient, Emergency or Ambulatory, for a Primary Diagnosis of Mental or Behavioural Disorder) Following Discharge from Secure Care (Maximum Follow-up 17.7 Years).
Principal Diagnosis Recorded at the First Post-Discharge Health Contact with a Primary Diagnosis of Mental or Behavioural Disorder.
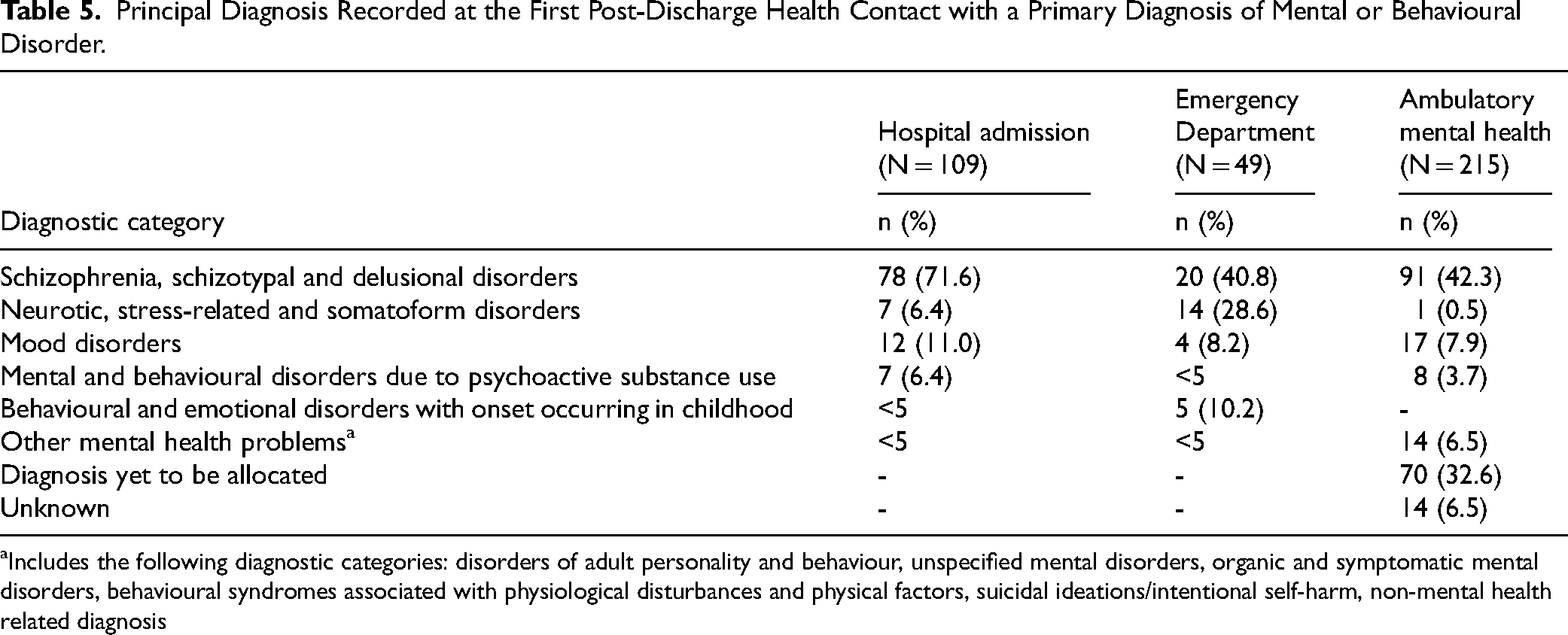
Includes the following diagnostic categories: disorders of adult personality and behaviour, unspecified mental disorders, organic and symptomatic mental disorders, behavioural syndromes associated with physiological disturbances and physical factors, suicidal ideations/intentional self-harm, non-mental health related diagnosis
Emergency Department Presentations
A total of 191 patients were discharged from secure care after the EDDC start date for data availability (i.e., 1 January 2005). Just over a quarter of the sample had an ED presentation (n = 53, 27.7%) within one year of discharge from secure care, and more than two thirds (n = 131, 68.6%) of the total sample had at least one ED contact by the end of the follow-up period. Most of these patients had their initial post-discharge ED presentation recorded as occurring in a metropolitan area (n = 93, 71.0%). The mean number of post-discharge ED presentations per patient was 5.1 (sd = 6.6, range = 1-58). As shown in Table 3, the most common diagnoses received at the first post-discharge contact were for ‘symptoms not elsewhere classified’ (n = 28, 21.4%) and for mental and behavioural disorders (n = 25, 19.1%). Injury, accidents, and poisoning (n = 24, 18.3%) were also recorded as common reasons for presentation.
Table 4 presents information on the timing of post-discharge ED health contacts for a primary diagnosis of mental or behavioural disorder. About a quarter of the sample (n = 49, 25.7%) presented to the ED for mental health reasons on at least one occasion following discharge, which is not surprising, as most acute admissions in NSW are now via ED. The mean number of post-discharge ED presentations with a primary diagnosis of mental or behavioural disorder was 2.6 (sd = 2.9, range = 1-16). The most common diagnosis received at the first post-discharge ED contact was for a schizophrenia-related condition (n = 20, 40.8%), followed by neurotic, stress-related and somatoform disorders (n = 14, 28.6%), which suggests that many of the Forensic Patients with persistent psychotic disorder presented to ED for other reasons.
Ambulatory Mental Health Contacts
A total of 227 patients were discharged after the MH-AMB data availability start date (i.e., 1 January 2001), and around two thirds of those had at least one contact within a month of discharge from secure care (n = 142, 62.3%), consistent with the usual conditions of discharge. Two thirds of the patients whose first post-discharge contact occurred within one month post-discharge were recorded as residing in a metropolitan area (n = 97, 68.3%). By the end of the follow-up period, most of the sample (n = 215, 94.7%) had at least one ambulatory mental health service contact, nearly all (n = 207, 91.2%) within the first year of discharge. The mean number of mental health service contacts per patient during the follow-up period was 431.3 (sd = 453.7, range = 1-4676), again, consistent with the requirement to attend regular scheduled appointments with case workers and treating psychiatrists.
Patterns of Combined Health Service Contact Types
As shown in Table 2, 81.5% of the sample (n = 185) had at least one type of hospital-based contact for any reason (hospital admission or ED contact) recorded after discharge (over a maximum follow-up period of 17.7 years). Over one-third of the sample (n = 84, 37.0%) had their first contact within one year of discharge. As shown in Table 4, nearly all of the sample (n = 216, 95.2%) had at least one mental health-related service contact following discharge, including an ED presentation or hospital admission with a primary diagnosis of mental or behavioural disorder, or an ambulatory mental health contact, usually within the first year of discharge (n = 210, 92.5%).
Factors Associated with Post-Discharge Health Service Contact Patterns
Table 6 presents the results of univariate Cox proportional hazard regression analysis of demographic, clinical, and criminal justice correlates of any hospital-based contact post-discharge for any reason. Significant univariate predictors of post-discharge hospital-based contact included English-speaking language background (HR = 1.63, 95% CI 1.16-2.30), the presence of a pattern of antisocial behaviour (HR = 2.12, 95% CI 1.20-3.75) and an index offence that was not homicide-related (HR = 1.44, 95% CI 1.07-1.94).
Univariate Cox Proportional Hazards Regression – Time to First Post-Discharge Hospital-Based Contact (Inpatient or Emergency, for Any Diagnosis).
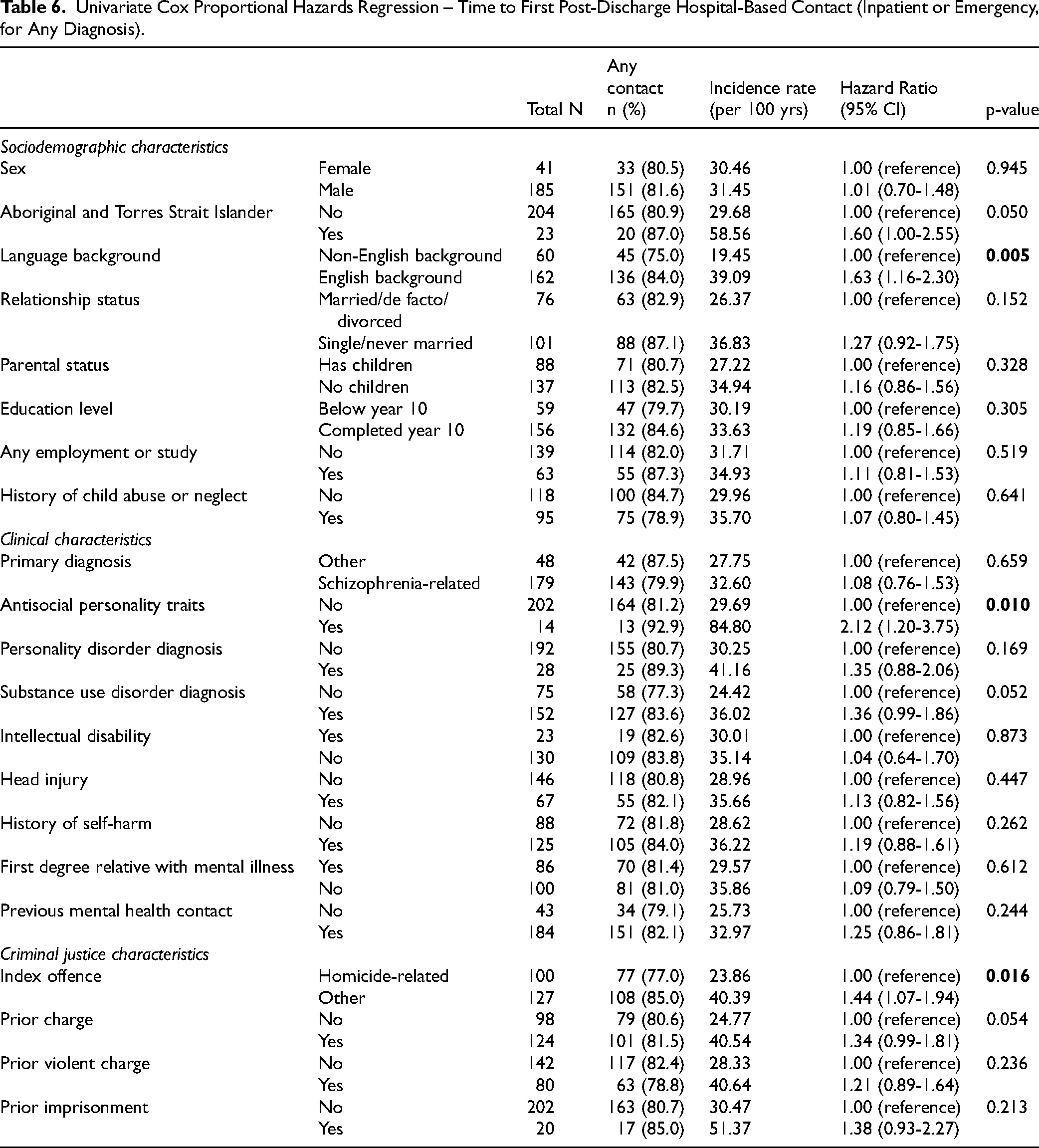
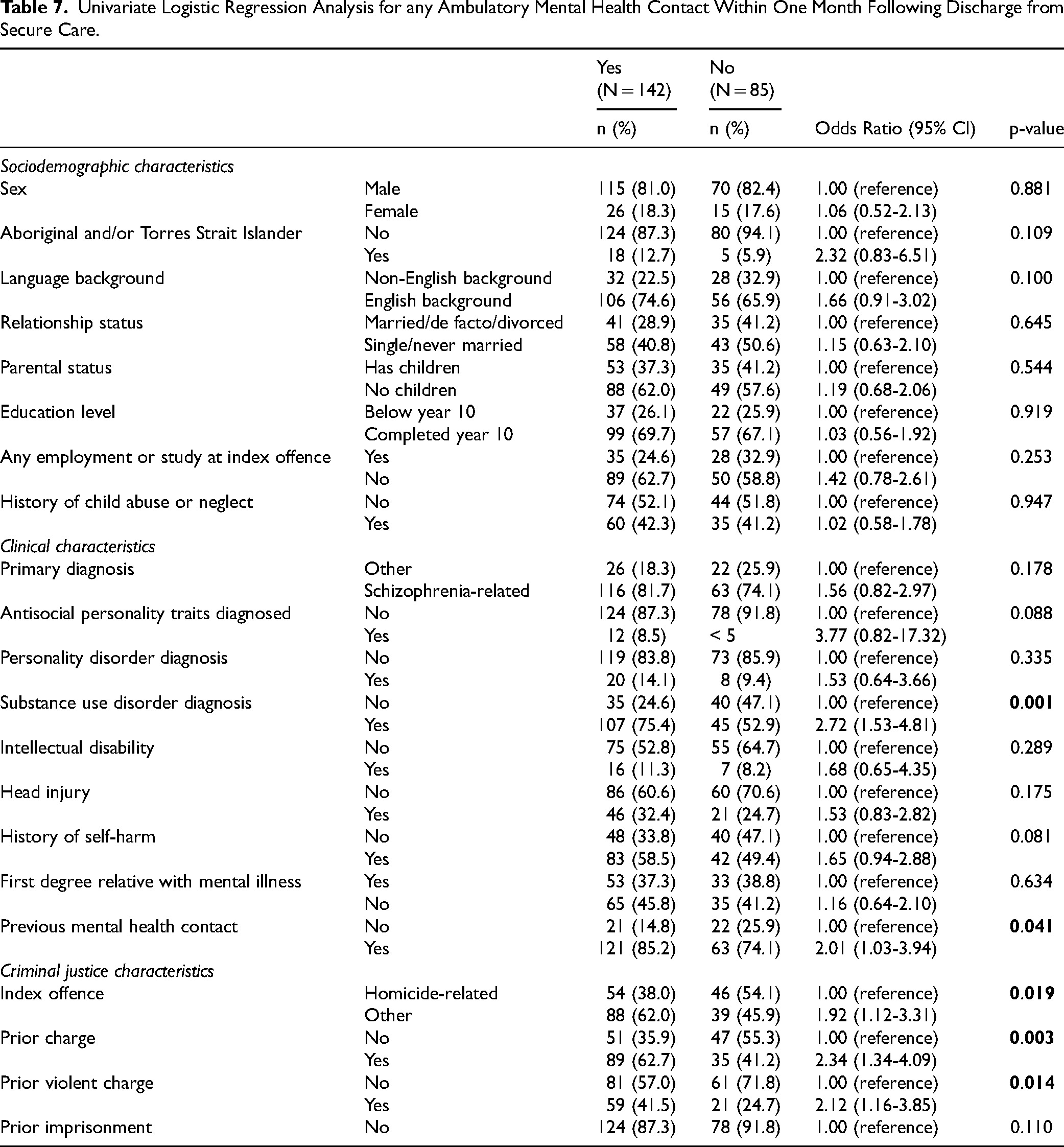
Table 7 details the results of univariate logistic regression analysis of demographic, clinical, and criminal justice factors associated with the odds of any ambulatory mental health contact within a month of discharge. Patients were more likely to have at least one ambulatory mental health contact if they had a diagnosis of substance use disorder (OR = 2.72, 95% CI 1.53-4.81) or had contact with mental health services prior to the index offence (OR = 2.01, 95% CI 1.03-3.94). Patients were also more likely to have contact within a month if they had an index offence that was not homicide-related (OR = 1.92, 95% CI 1.12-3.31) or had a criminal charge recorded prior to the index offence, either for any offence type (OR = 2.34, 95% CI 1.34-4.09) or a violent offence (OR = 2.12, 95% CI 1.16-3.85).
Univariate Logistic Regression Analysis for any Ambulatory Mental Health Contact Within One Month Following Discharge from Secure Care.
Discussion
In this sample of Forensic Patients discharged from secure hospital care, more than one-third had at least one hospital-based health service contact for any reason within the first 12 months post-discharge. More than a quarter had a hospital admission within this time period. Not surprisingly, the most common reason for the first post-discharge inpatient or emergency service contact was for treatment of mental illness, but ED and hospital treatment after injuries, accidents and self-poisoning were also common. Post-discharge contact with hospital-based health services for any reason was more common amongst those from an English-speaking background, those recorded as having antisocial personality traits, and for those with a non-homicide index offence. Two-thirds of the cohort were found to have engaged as expected with community-based ambulatory mental health services by having at least one contact within the first month following discharge. Those engaging were more likely to have a co-morbid diagnosis of substance use disorder, a history of mental health service contact prior to the index offence, a non-homicide-related index offence and prior criminal justice system contact, perhaps indicating that those with complex needs were supervised more assertively after discharge. Given the nature of the mental illnesses experienced by Forensic Patients, relapse and contact with hospital-based health services do not necessarily indicate failure of mental health care, and instead reflect the ready access to care and an appropriate response to the early warning signs of deteriorating mental health as specific to the individual patient (Lyons et al., 2022).
The rates of post-discharge hospital admission found in the current study are comparable with the findings of studies conducted in Australia and elsewhere. Although calculated as a cumulative incidence over the first 12 months following discharge, rather than incident rate, the current study found 16.3% were readmitted for treatment of mental illness within a year of discharge from secure care, a figure at the upper end of the range reported in a published systematic review (Fazel, Fiminska et al., 2016), but lower than rates reported in samples of non-Forensic Patients with severe mental illness discharged from hospital. For example, the Study of High Impact Psychosis (SHIP) study in Australia found that almost half of those with psychosis living in the community presented to an ED or were admitted to hospital for mental health reasons over a one-year period (Sweeney et al., 2015).
It is well known that people released from prison have high rates of ED contact (Frank et al., 2013; Kouyoumdjian et al., 2018), including for injury and self-harm (Young et al., 2020), but few studies have reported rates of post-release ED contact amongst Forensic Patients. The current study found a low rate of mental health-related ED contact of 7% in the first year after discharge, possibly because Forensic Patients are usually discharged from secure care with a high-level of supervision and support from community-based services and do not usually require emergency care. This suggests that the pathway to ED services may be initiated based on the discretion of a community-based wraparound service. The high rates of poor physical health and neglect of preventative health measures may be the reason for some of the ED contact in this sample. Some mental health facilities require all admissions (even planned admissions) to be via ED, so ED contact for mental health reasons may not indicate a crisis. Health crises from accidents, self-poisoning and other intentional self-harm will also be via ED. The data available does not allow identification of the reason for the mental health admission, making it difficult to say whether ED presentations reflected a breakdown in community-based care. Non-adherence to conditions is known to be associated with an increased likelihood of readmission to hospital following conditional discharge (Hayes et al., 2014).
As expected, most patients in the current study had at least one recorded contact with ambulatory mental health services following discharge. However, a surprising and possibly alarming finding was that a third of the sample did not have recorded contact within the first month. Previous research indicates that the factors associated with what appears to be closer supervision are also associated with a greater risk of relapse or reoffending post-discharge (e.g., Jewell et al., 2018; Takeda et al., 2019) and the earlier engagement of patients with these risk factors probably reflects more effective supervision. However, all Forensic Patients should have early post-discharge engagement with a nominated case manager, rather than relying on other mental health services, including those provided in private practice that were not recorded in this study.
The current study also considered contact with health services for reasons other than a mental health condition. There was a high rate of physical illness and injury, including self-injury and accidents, in this group, with Forensic Patients known to have high rates of physical illness, including metabolic syndrome and cardiovascular disease (Ma et al., 2021). Disabling psychotic illness affects the ability to maintain a healthy lifestyle and engage in preventative healthcare (Justice Health and Forensic Mental Health Network, 2016; Victoria Legal Aid, 2016). This study is the first to show a high rate of presentation after accidental injury, as well as self-injury, indicating a high rate of psychological distress and impaired self-care. Discharged Forensic Patients have been shown to have high rates of all-cause mortality, especially suicide (Fazel, Fiminska et al., 2016; Rees & Thomson, 2020), in line with the greatly reduced life expectancy of people with severe mental illnesses (Laurensen et al., 2014).
Previous studies have identified several clinical and demographic factors associated with readmission after discharge from secure care. On univariate analysis in the current study, Forensic Patients from an English-speaking background, those with clinically documented anti-social personality traits and those who were charged with a non-homicide index offence had a higher incidence of hospital-based healthcare contact after discharge. The finding that Forensic Patients from an English-speaking background had a higher incidence of readmission may relate to an increased ability to successfully navigate health systems and seek help (Monson et al., 2001), but it may also reflect elements of social disadvantage that increase risk of poor mental health outcomes, given the complex relationship between migration, ethnicity, language diversity and health outcomes (Jatrana et al., 2018). For example, Forensic Patients in NSW from an English-speaking background will include the majority of those of Indigenous heritage, while others from a non-English-speaking background may have moved to Australia as skilled migrants and may benefit to some extent from the ‘healthy migrant effect’ (Nielssen et al., 2013).
It is not surprising that antisocial personality traits and substance use disorder are associated with an increased incidence of post-discharge healthcare contact, given the higher level of supervision required (Fazel, Wolf et al., 2016; Green et al., 2014; Penney et al., 2018; Takeda et al., 2019). In the current study, the type of index offence was also found to be associated with an increased incidence of post-discharge hospital-based healthcare contact (i.e., those with a non-homicide index offence were more likely to have contact). A typology of Forensic Patients based on the presence or absence of an early onset of offending history, suggesting antisocial traits (Crocker et al., 2018; Hodgins, 2008), has identified groups with different post-release outcomes. Those with early onset of antisocial behaviour tend to commit a greater number of offences over time and demonstrate a greater range of offending but their index offence is less likely to be homicide-related than those who offend for the first time after the onset of mental illness. The association of post-discharge healthcare contact and non-homicide index offence found in the current study may reflect this typology, but a larger study with greater statistical power to investigate the multivariate relationships, both confounding and moderating, between factors would be required to disentangle these various associations. Duration of detention is likely to have varied with the type of offence, and greater care would be expected in the release of more serious offenders. Given the variety of factors identified as potential correlates of post-discharge readmission, in our study and others, an individual patient-centred assessment, formulation and management of identified risk factors is likely to be the most effective approach for reducing risk of post-discharge readmission.
Strengths and Limitations
The strengths of the present study include a complete sample of discharged Forensic Patients, the wide range of patient factors examined, access to the full spectrum of public health service contact and the use of record linkage methodology, which limited the potential impact of selection or information biases. Limitations include insufficient statistical power to identify predictors of post-discharge health service contact types separately, resulting in the need to combine contacts into one variable for analysis, and the inability to perform multivariate analyses. Moreover, the linked health datasets contained little information beyond the date and type of contact and the diagnoses recorded, and the reasons for contact, the treatment received, and the outcomes of treatment could not be examined. There was also no information about patients’ mental health status during the post-discharge period to determine whether health service intervention was needed but not provided. It should be noted that data was only available for patients found NGMI up to 2016, and decisions for release may also have been skewed by the change in procedure in 2009, in which the power to grant conditional release was vested in the MHRT, rather than the health ministry. Finally, there was no comparable control group.
Conclusion
The current study confirms the high rates of post-discharge healthcare contact for Forensic Patients. The intensive community care and the low threshold for healthcare intervention may explain the relatively low rate of criminal recidivism in this cohort. However, not all discharged Forensic Patients appeared to be engaged with community mental health services as early in the post-discharge period as might be expected. Overall, the care provided to discharged Forensic Patients provides a model of continuity of care for people with persistent psychotic illness, resulting in lower rates of emergency contact and rehospitalisation than is typically seen for those with severe mental illnesses in the community.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Kimberlie Dean is supported by Justice Health and Forensic Mental Health Network and NHMRC Investigator Grant (APP1175408).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.