
Abstract
Compared to other criminal offenses, individuals convicted of a sexual offense experience higher levels of stigmatization, with the public often expressing feelings of fear and disgust. Many individuals who serve time for a sexual offense will reintegrate back into society amongst community members who often believe that sex crimes are on the rise, recidivism rates are high, and that individuals who commit sexual offenses are more dangerous than those who commit other offenses. Little research has explored how the presence of a mental health disorder impacts public attitudes toward reintegration. The current study uses thematic analysis with reflexive elements to explore attitudes toward individuals with a mental health disorder who have committed a sexual offense. Participants (N = 262) were randomly assigned a vignette depicting an individual who has either schizophrenia or depression and is reintegrating into their neighborhood after committing a sexual offense. Findings suggest that while many participants support reintegration and rehabilitation, attitudes varied when considering the mental health disorder; some participants attributed offending behavior to schizophrenia, while others—particularly in the depression condition—suggested mental illness is not associated with sexual offending. Implications for mental health providers and future research directions are discussed.
Previous literature has demonstrated that the public holds varying levels of stigma and negative beliefs regarding the reintegration of individuals based on the types of crimes they have committed (Richards & McCartan, 2018; Tan et al., 2016). Specifically, Harper et al. (2024) found that people accused or convicted of a sexual offense experience heightened levels of stigmatization compared to those convicted of other offenses. Discriminatory and punitive views from the public increase barriers to intervention and the promotion of programming upon reintegration (Harper & Harris, 2017). Similarly, although on a lesser scale, individuals living with a mental health disorder can also experience stigmatization and/or dehumanization from society, which may be expressed through fearfulness toward this population (Boysen et al., 2020; Casados, 2017). A predominantly punitive societal attitude toward those with sexual offense convictions and individuals with mental health challenges reduces the accessibility of preventative approaches, potentially contributing to an increase in recidivism (Chui & Cheng, 2014; Murphy & Harris, 2007). Despite this, research has yet to explore how the presence of a mental health disorder in someone convicted of a sexual offense may impact public perceptions and attitudes toward their reintegration process.
Public Stigmatization of Sexual Offending
Individuals who have committed a sexual offense often face significant stigmatization from the public, with stigma persisting before, during, and after incarceration (Evans & Cubellis, 2015; Tewksbury, 2012). Emotional reactions from society toward individuals convicted of sexual offenses often include fear and/or disgust (Kernsmith et al., 2009; Spencer & Ricciardelli, 2017; Stevenson et al., 2015). Kernsmith et al. (2009) examined fear reactions toward those who have committed different types of sexual offenses (e.g., incest, statutory rape, marital rape), finding that every type of sexual offense that was explored induced some amount of fear from participants. Similarly, Spencer and Ricciardelli (2017) interviewed 100 Canadian correctional officers and found that negative perceptions of those with sexual offense convictions permeates correctional centers, with participating correctional officers noting that it is against their moral judgment to associate with and assist incarcerated individuals convicted of sexual offenses.
Common misconceptions regarding sexual offending often influence negative perceptions of individuals who have committed these types of offenses (Harper et al., 2017; King, 2019). For example, there is an overarching belief that individuals convicted of a sexual offense are bound to reoffend, assuming high recidivism rates compared to other offenses (King, 2019). Indeed, Levenson et al. (2007) found that the American public believes recidivism rates for sexual offending are approximately 75%. In reality, while recidivism can be higher among certain subgroups (e.g., 35% after 15 years for those who offend against extrafamilial male children), rates of sexual reoffending in general tend to be much lower—between 8–20% (although rates increase over time, Lussier et al., 2023; for example, 20% after 10 years, Harris & Hanson, 2004). The public also tends to believe the myths that sexual offending rates are on the rise and that individuals who have committed sexual offenses are more dangerous, more uncontrollable, and more unpredictable than those convicted of other offenses (Koon-Magnin, 2015; Levenson et al., 2007; Zatkin et al., 2022). Overall, public stigmatization surrounding sexual offending is complex, harmful, and fueled by misconceptions, and has negative implications for the rehabilitation and reintegration of individuals who have committed sexual offenses (Schultz, 2014).
Rehabilitation and Reintegration
Rehabilitation and reintegration are often combined when discussing public perceptions of individuals convicted of criminal offenses. While rehabilitation includes a range of psychosocial programs and services to address needs associated with offending behavior (Wormith et al., 2007), reintegration refers to the adjustment and transition from prison to the community in hopes of maintaining a crime-free lifestyle (Davis et al., 2012).
The public tends to favor harsh punitive sanctions for individuals convicted of a sexual offense rather than considering the importance and effectiveness of rehabilitation (Levenson et al., 2007), a perspective likely associated with offense-related stigma. Viki et al. (2012) found that participants who dehumanized individuals convicted of a sexual offense showed less support for their rehabilitation, recommended harsher sentences, and were more in favor of excluding them from society. However, a study by Mears et al. (2008) demonstrated that although 97% of Americans believed that a sentence in prison or jail was the most appropriate punishment for the sexual assault of a person aged seventeen or younger, 52% said they would pay taxes to support the treatment of individuals convicted of a sexual offense. While many in the public are hesitant to believe that rehabilitation is effective in treating sexual offending (Mancini & Budd, 2015), research has shown that treatment programs for those who have sexually offended are effective in reducing recidivism (Barros et al., 2022; Schmucker & Losel, 2017).
Furthermore, public perceptions of those who have sexually offended can influence the success of community reintegration. The stigma that individuals experience from the public upon reintegration can substantially impact their ability to secure employment and housing, as some employers and landlords may perceive them as untrustworthy (Dako-Gyeke & Baffour, 2016). Harassment from community members is consistently present (Kernsmith et al., 2016), and shame and ostracism can contribute to increased recidivism (Murphy & Harris, 2007). Overall, stigma toward this population continues to exist, with the public often holding punitive and negative views toward rehabilitation and reintegration.
Public Stigmatization of Mental Illness
In a similar vein, stigma is also experienced by individuals with a mental health disorder. Each year, one in five Canadians experience a mental illness (Smetanin et al., 2011), but many people still fear and dehumanize those with mental health disorders (Boysen et al., 2020). Since quantitative research on the prevalence of stigma experiences is limited, much of what is known comes from qualitative studies. Moses (2010) found that over half of those who live with a mental health disorder face stigma from those around them, including family and friends. Additionally, many individuals within the prison system struggle with a mental health disorder, creating intersectional stigma; this may contribute to increased difficulties and decreased social support, as the public may view these individuals as less likely to recover due to the dual nature of offense and disorder (Dorkins & Adshead, 2011; Sapers & Zinger, 2016).
Depression and schizophrenia are two mental health disorders with differing public attitudes. Depression is seen as more controllable and treatable, while schizophrenia is often associated with violence and danger, despite higher victimization risks (Krendl & Freeman, 2019; Norman et al., 2012; Wehring & Carpenter, 2011). About 60% of people view those with schizophrenia as dangerous (Pescosolido et al., 2019), a perception likely shaped by decades of research focusing more on violence by, rather than against, individuals with mental illness (Wehring & Carpenter, 2011). Given the highly stigmatizing nature of sexual offending, in addition to the stigma that can arise from having a mental illness, it is crucial to explore how the public perceives those with a mental health disorder who have committed a sexual offense.
Theoretical Frameworks Exploring Attitudes Toward Sexual Offending and Mental Illness
To aid in understanding perceptions of those who have committed sexual offenses, as well as attitudes toward mental illness, we highlight the following theories: the Belief in Redeemability Framework (Maruna & King, 2009), Moral Foundation Theory (Harper & Harris, 2017), and Attribution Theory—the latter of which can be used to understand the combination of attitudes toward sexual offending and mental illness.
Maruna and King's (2009) Belief in Redeemability framework draws on Attribution Theory to conceptualize beliefs about “deviants’” ability to reform, distinguishing between dispositional (crime as a personal choice) and situational (crime as a result of social forces) attributions. Their research identified four public views of offenders: (1) victims of society, (2) permanently damaged by society, (3) people who made bad choices, and (4) evil. These views influence punitiveness, with dispositional believers favoring punishment and situational believers supporting rehabilitation. Attribution Theory posits that stigma arises when the public attributes undesirable behaviours, such as mental illness or sexual offending, to internal, stable, and controllable causes. These attributions can result in negative emotional responses (e.g., anger, fear), and behavioural tendencies (e.g., social distancing, discrimination) (Corrigan et al., 2003; Weiner, 1995). When applied to mental illness, assumptions regarding the cause, controllability, and dangerousness of the disorder contribute to public reactions. Corrigan et al. (2003) found that causal attributions regarding mental illness affect beliefs about an individual's responsibility in causing their illness to occur, creating emotional responses to individuals with mental illness, which, in turn, fuel stigma. When applied to sexual offending, this model can explain negative attitudes toward this crime.
Similar to the Belief in Redeemability framework, Harper and Harris’ (2017) Moral Foundations Theory examines psychological factors shaping attitudes toward those who sexually offend, from punitive (pro-punishment) to progressive (pro-reform) views. Progressivism focuses on preventing reoffending based on evidence, while punitive attitudes often stem from misconceptions, such as viewing offenders as a homogenous, high-risk group unlikely to be rehabilitated. This theory suggests that core beliefs about the world are often unconscious and may lack rational decision making. Key ideas include: (1) a human instinct to protect the vulnerable, particularly children; (2) a desire to distinguish right from wrong and follow societal rules; (3) support for in-groups, which can foster animosity toward out-groups; and (4) disgust toward perceived impurity in societies valuing purity. Individuals may prioritize certain moral foundations (e.g., care, fairness, loyalty, purity) based on their experiences.
Harper and Harris (2017) link this theory to political tendencies, suggesting liberals prioritize care, harm, and fairness, while conservatives value purity, authority, and loyalty. Liberals often emphasize rehabilitation, believing behavior can change, whereas conservatives tend to be more punitive, viewing crime as a violation of morality and societal rules. However, the authors note that attitudes toward sexual offenders are more nuanced, and we expect that asking people to consider mental health status will add further complexity. Together, these theories inform our study and may help us understand the context of our findings on stigma in relation to those who have sexually offended with a mental health disorder.
The Present Study
There is limited research that has examined the public's attitudes toward the reintegration of individuals with a mental disorder who have also committed a sexual offense. Therefore, the present study utilized thematic analysis with reflexive elements to explore Canadians’ opinions toward such an individual re-entering into the community. This study is situated within a social constructivist epistemology, acknowledging relativism as an ontological approach—both suggesting multiple realities exist and that it is through sharing multiple views and honoring differences that one comes to understand the human situation more fully (Berger & Luckmann, 2016; Guba & Lincoln, 1994).
Method
Participants and Procedure
The current study is part of a larger mixed methods study (N = 398). Participants were Canadians over the age of 18 who were recruited through Amazon's Mechanical Turk (MTurk; a crowdsourcing platform that allows Requesters to submit Human Intelligence Tasks for Workers to complete) and Prolific (a crowdsourcing platform that connects researchers with participants who can take part in studies, surveys, and experiments) (n = 129), social media (n = 65), as well as an undergraduate research participant pool available at the authors’ institution (n = 68). All respondents provided informed consent and researchers received ethics approval from the Saint Mary′s University research ethics board.
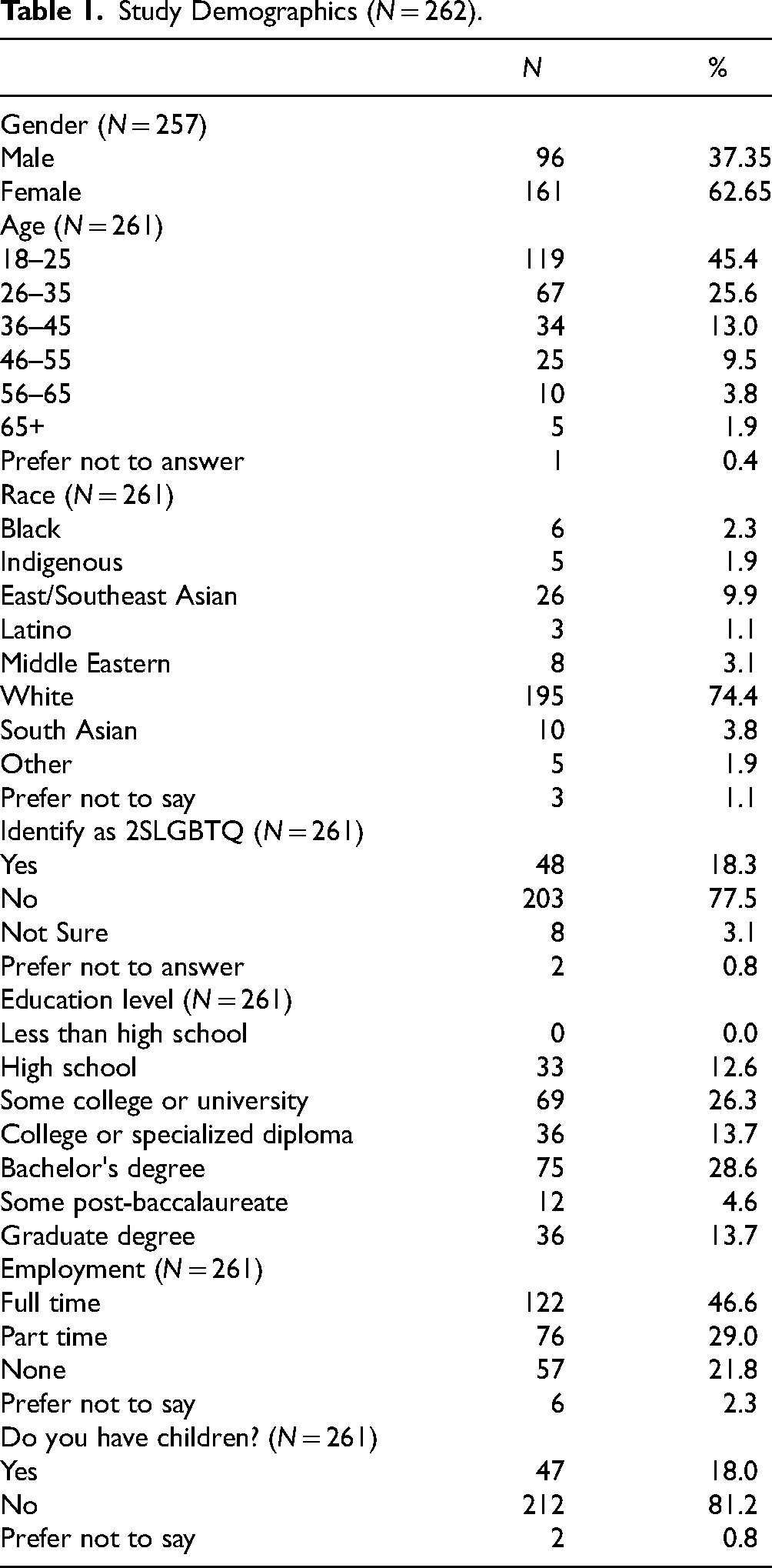
Demographic data included age (45.4% between 18–25 years old), gender (62.7% women), sexual orientation (18.3% identify as 2SLGBTQ+), race (74.4% white), education level (28.6% held a Bachelor's degree), and employment (see Table 1 for further details on demographics). Participants were randomly assigned to one of three conditions where they were provided with a vignette depicting an individual (Mr. Baker) who was reintegrating into the participants’ neighborhood after being convicted of a sexual offense. The vignettes depicted Mr. Baker as having no mental disorder (control), a psychotic disorder (schizophrenia), or a mood disorder (depression). After reading the vignette, participants were asked to respond to four open-ended questions regarding their feelings and actions if Mr. Baker was their neighbor (see supplemental file). Two hundred sixty-two participants were included in the qualitative analysis with responses from the control condition being removed, as the goal of this study was to concentrate specifically on the impact of different mental health disorders on public attitudes toward reintegration, rather than attitudes in general or comparison to a baseline.
Study Demographics (N = 262).
Data Analysis
The current study involved inductive thematic analysis with reflexive elements. We followed Braun and Clarke's (2006, 2019) six-step model, starting with data familiarization, whereby the first three authors read and re-read the full dataset to gain an understanding of participant responses before coding. An inductive approach was followed when coding the data; codes were not determined prior to data familiarization. Consistent with a complete coding approach, codes were mostly words or short phrases that were applied to units of data, which in this case, were participant responses to each question. In some instances, multiple codes were applied to a given unit. Codes were both semantic and latent. The first three authors coded each condition by hand (using digital highlighters), consistently engaging in open discussion with each other. These authors then collated the data by grouping all instances of each code together, while simultaneously generating initial themes based on patterns across the dataset. Themes were later refined several times through an iterative process.
Finlay (2021) distinguishes between different types of thematic analysis, highlighting that some are “scientifically descriptive,” while others are “artfully interpretive” (p.104). Finlay (2021) notes that many qualitative researchers, in part, prescribe to both camps, with Braun et al. (2023) agreeing that “some approaches combine elements of both” (p. 20). For example, researchers may take a systematic, stepwise approach to coding, ensuring themes are justified, well-evidenced, and even validated by co-researchers—all while emphasizing the creative component of analysis that is positioned within their own biases (Finlay, 2021). Drawing on this, we believe our approach to analysis combined scientifically descriptive and artfully interpretive elements. Further details regarding the analyses and reflexivity are included in the supplemental file.
Results
We generated five themes that were representative of the thoughts, opinions, and feelings of Canadians toward mental health disorders and individuals who have committed a sexual offense: (1) The Complexities of Mental Health and Accountability, with subthemes: Conflating Mental Illness and Sexual Offending and Mental Illness is not an Excuse, (2) Everyone Deserves a Chance, with subtheme: The Necessity of Treatment, (3) Concern for Others, (4) “I Support Him, But …,” and (5) You’ve Made Your Bed, Lie In It.
The Complexities of Mental Health and Accountability
When voicing their opinions about Mr. Baker, some participants explicitly referenced his mental health disorder. Those in the schizophrenia condition often linked Mr. Baker's disorder to treatment, reintegration, and accountability—attributing the sexual offense to the disorder. Conversely, participants in the depression condition sometimes mentioned mental health more broadly or dismissed its relevance to the offense. To fully unpack these layered viewpoints, two subthemes were created: Conflating Mental Illness and Sexual Offending and Mental Illness is not an Excuse.
Conflating Mental Illness and Sexual Offending
Particularly among responses in the schizophrenia condition, Mr. Baker's mental illness was discussed in relation to his offense and reintegration. One individual indicated they would support Mr. Baker with readjusting to society because schizophrenia is “an uncontrollable disorder” (P#379). Similarly, another wrote: “I believe some people with schizophrenia act out when they don't mean it. Tho sexual assault is a terrible crime he has served his time and hopefully is on good medication now and can start his journey of [recovery]” (P#284). This demonstrated the likely assumption that Mr. Baker's sexual offense was linked to his schizophrenia, suggesting that some people believed the offense could be attributed to his disorder. Although the vignette did not state that Mr. Baker's mental health disorder contributed to his criminality, it was evident that some respondents assumed the two went hand-in-hand.
While the participants quoted above appear to be supportive and lenient toward Mr. Baker because of his schizophrenia, others took the opposite viewpoint: Mr. Baker requires serious treatment, and we are all aware that schizophrenia is challenging to treat, if treatment is even possible. Taking this into consideration, it would be better to place him in a specialized facility where he can receive the specific treatment and care he needs (P#311).
Here, participant #311 reinforced the common misconception that schizophrenia is untreatable (Crisp et al., 2005). It appears they could also be equating Mr. Baker's schizophrenia to his offending behaviour, suggesting that his schizophrenia is untreated, and that housing him in a secure facility would prevent offending, reflecting a deeper belief that those with schizophrenia should be institutionalized or cannot live safely in the community.
Similarly, we noticed a broader pattern across the data, reflecting a tendency to view sexual offending as a mental illness (Richards, 2018), a belief rooted in early 1900s policies involving indefinite psychiatric commitment for “sexual degenerates” (Harper & Harris, 2017). Participants sometimes used terms like “illness” or “condition” ambiguously, suggesting a conflation of mental health disorders and sexual offending.
Mental Illness Is Not an Excuse
Despite some participants drawing a connection between the two, others clearly separated Mr. Baker's mental health disorder from his sexual offense: … sex offenders belong in prison, regardless of whether or not they are mentally ill. Just because they were ‘cured’ of said illness doesn't mean they aren't dangerous or likely to reoffend, especially since having a mental illness doesn't cause someone to sexually offend. Schizophrenia in of itself doesn't cause anyone to commit sexual assault, and the vast majority of people with schizophrenia are more likely to harm themselves than others. That was an action he decided to take and therefore should be held criminally responsible and kept away from the public … (P#359)
Here, participant #359 recognized that not all who sexually offend have a mental illness and vice versa. Despite this, they took a punitive stance, suggesting all sexual offenders belong in prison, reflecting a strong belief in personal accountability. This was further reflected by participant #337, who noted “a crime is a crime regardless of mental state. If a mentally stable person were to commit the same sexual offense, they would not receive government support to reintegrate”. Although participant #359 seemingly rejects rehabilitation for those who commit sexual offenses and participant #337 emphasizes reintegration, both view crime as a choice, reflecting a dispositional (individual) belief that Mr. Baker cannot change. These responses underscore the complex relationships among mental illness, criminality, and accountability.
Some respondents carefully considered the mental health component of the vignette while maintaining that Mr. Baker's mental illness does not change the seriousness of the sexual offense: “I would support his recovery from schizophrenia, but would not support his sexual offence” (P#355). Reading between the lines, the data suggest that this participant believes that supporting rehabilitation means supporting or excusing the criminal act that was committed.
There were also instances in which participants in the depression condition distinguished between Mr. Baker's mental health disorder and his offense. For example, one participant said, “someone with depression is still fully conscious and aware of their actions towards others, and for someone to sexually assault another human, and traumatize and scar that person for life is in my opinion truly unforgivable” (P#218). Another wrote, “I would feel disgusted. Nothing about his depression bothered me it was his sexual offence” (P#143). Notably, we found no instances of respondents in the depression condition attributing Mr. Baker's offense to his mental disorder, as noticed in the schizophrenia condition and described in the previous theme, possibly because depression has become normalized in society (Snell-Rood & Carpenter-Song, 2018). Individuals in the schizophrenia condition were more likely to view the mental disorder as potentially attached to the criminal behavior, whether it is an excuse or not.
Everyone Deserves a Chance
Many participants believed Mr. Baker deserved the chance to reintegrate and rehabilitate. While “rehabilitation” was not written in the open-ended questions, respondents often used this word in their responses, alongside reintegration, to discuss Mr. Baker's opportunities to change. For this reason, the main theme focuses on reintegration, while the subtheme The Necessity of Treatment addresses rehabilitation.
Throughout responses, many participants used phrases such as “another chance” and “second chance” when discussing reintegration. For example, one participant stated: “he is a citizen & person. He may have only made one mistake. He deserves a chance to live a normal life” (P#138, depression condition [DC]). Another respondent wrote: “he deserves to have a second chance and has [the] right to receive the proper support to ensure a successful community reintegration” (P#176, DC).
Some participants were aware of the benefits of reintegration in comparison to incarceration. For example, “reintegration is more productive than staying in prison or a hospital” (P#171, schizophrenia condition [SC]). Similarly, another stated: I don't see anything wrong with helping someone try to improve their situation. Reintegrating back into society is better than being in and out of prison or homeless, if no support is given you can't expect him to deal with all of this on his own and succeed. (P#198, SC).
These respondents compared reintegration to alternatives that are likely unhelpful, and sometimes costly to society, including incarceration, hospitalization, and homelessness. Other participants discussed the opportunity for reintegration as it relates to reoffending. For example, one participant stated: Yes, I am willing to use the tax money to support Mr. Baker's reintegration program and services. I believe that the reintegration of sexual offenders is conducive to reducing social discrimination and conflict and promoting social harmony. If they are excluded for life, it may cause them to deteriorate psychologically and commit crimes again (P#174, DC).
Overall, participants within this theme supported the idea of reintegration and believed Mr. Baker deserves a second chance, whether it be for personal growth, positive change, or public safety.
The Necessity of Treatment
Many participants emphasized the need for rehabilitation for individuals with mental health diagnoses who have been convicted of a sexual offense. For example, one participant commented: “I think the justice system and public systems should [be] focusing on rehabilitation rather [than] retribution. People should be given second chances.” (P#194, DC). It is apparent that this participant does not believe punishment provides someone like Mr. Baker with an opportunity to rehabilitate, suggesting the need for support and assistance from public services. This is furthered by other responses, such as: “… I believe that people with mental health disorders deserve treatment whether or not they have been convicted of a crime” (P#71, SC).
Reflecting on the importance of rehabilitation, participant 318 wrote: I don't think it'd make much sense to hope for a world where less sex offenses are committed, while simultaneously restricting access to resources for programs and services that work to achieve this. It'd be like wanting to live in a world with less fires, while also restricting fire department's access to funding and equipment. It's just counterproductive (P#318, SC).
This participant noted that reducing sexual offending requires greater access to support services, which are often limited and stigmatized. A reduction in sexual violence depends on making these resources available to those who offend.
Acknowledging that some individuals believed in the rights of Mr. Baker to receive treatment, while still feeling unsure about him and what he has done, participant #177 stated: “while I would personally feel uncomfortable around him, it won’t stop him from being there. He is probably struggling mentally since being released and anyone experiencing mental health concerns deserves a chance of getting help” (P#177, DC).
Concern for Others
Many participants expressed concern for others when contemplating Mr. Baker moving to their neighborhood. Perhaps most salient was the concern for children and families within the neighborhood. Participants spoke about informing members of their family about Mr. Baker: “I would make sure that I informed others in my neighbourhood that he is living there and if I had children I would make sure that they were aware of the situation and to remain cautious” (P#71, SC). Some participants took an educational stance in relation to informing and protecting children, “I think I will strengthen the communication with Mr. Baker … so as to better judge whether there is any abnormal situation. At the same time, to educate children how to protect themselves, enhance the awareness of prevention” (P#138, DC). This reflects support for primary prevention of child sexual abuse by raising awareness among children and families to help identify and prevent abuse (Austin & Salter, 2023).
Others were so concerned about living near Mr. Baker that they expressed a willingness to relocate: “I would likely leave that community if it was possible. Since having my daughter it has made me think more about people like Mr. Baker” (P#194, SC). Interestingly, despite the vignettes having no mention of victim typology, some participants felt children were particularly prone to potential victimization at the hands of Mr. Baker, with some describing him as a “pedophile”. One participant, when asked how they'd feel if he were their neighbor, said, Concerned … if I lived next to a community park with many children and schools in the area I would have a few questions. If I were to live somewhere where there was not many kids, or nearby schools or parks it would be less concerning (P#65, DC).
Participants were also concerned for other members of the community and the impact that Mr. Baker's actions had on the life of the hypothetical victim. For example, “I think sexual assault is a serious social problem, and it must be very heavy and worrying for victims and their families to learn that sexual assault is living next door” (P#138, DC). Finally, participants would sometimes discuss how best to support society and how the government can play a role in the wellbeing of the community. One participant said they would support their tax dollars going to reintegration services because “I believe it helps everyone in the long run. Mr Baker can reintegrate into society and the community is safer” (P#212, DC). Another wrote: “I am in support. However, the government must do all it can to protect society” (P#39, DC).
“I Support Him, But..”
Many participants expressed willingness to support Mr. Baker, contingent on certain factors. This conditional support manifested in various ways, such as questioning Mr. Baker's adherence to treatment and medication, the details of his crime, and whether he was truly remorseful—all of which could be seen as aligning with societal standards. For example, one participant stated that they would support Mr. Baker readjusting to society “if he was truly repentant and taking his meds and trying” (P#314, SC), with another saying, “Yes I support it, depending on if Mr. Baker is extremely remorseful and wanting to readjust to society” (P#370, SC).
In a similar vein, many participants stated they would offer support, but in an apprehensive, hands-off manner. For example: “Would I personally support him? No. Would I agree that he should be supported? Yes.” (P#74, SC). Similarly, another participant stated, “I support him getting counseling he needs but I personally would not be comfortable supporting him” (P#173, DC). Like individuals who indicated they would want to move upon learning Mr. Baker was going to reside in their community, these individuals recognize the need for support and services, but do not want to personally be involved in any capacity.
While many participants acknowledged the benefits of rehabilitation programs and services, others expressed doubts and questioned their efficacy. For example: “… as long as there is evidence of these programs and services in supporting these people” (P#398, SC). Another respondent wrote: “Only if doctors could provide evidence that he has changed his ways. But that doesn't mean I still would not have my guard up when he is around” (P#313, SC). Emphasized here is the notion that the public is willing to support Mr. Baker if rehabilitation efforts have been successful. Studies have shown that treatment programs for individuals who have committed sexual offenses effectively reduce recidivism (Barros et al., 2022; Schmucker & Losel, 2017); providing data on rehabilitation effectiveness could strength the public's cautious support.
Many participants wanted more detail on the nature of Mr. Baker's offense before forming an opinion, implying their feelings were dependent on specific circumstances: Yes. However I really think it depends on the severity of the sexual assault committed. But if professionals deem him able to be released into society, I should be able to put my trust into those who are trained to work with individuals like Mr. Baker to know when offenders are ready to begin their readjustment period (P#384, SC).
Moreover, when asked if they would support Mr. Baker in readjusting to society after his release, one participant stated: “Depending on whom his sexual assault was against (was it what I am, young and female, or a child for example) then only if he came to me for assistance, I would not go out of my way to seek him out” (P#223, DC). While this participant suggests that they would help Mr. Baker only if he came to them and requested support, it is not obvious whether this participant means they would be more or less likely to support him if the victim of his crime was similar in profile to the participant themselves, or how this compares to their support had the victim been a child—it is possible that they are worried they may become the next victim if they get too close to Mr. Baker. This would be an interesting line of future inquiry.
You’ve Made Your Bed, Lie in It
Unlike responses offering apprehensive support, this theme encompasses individuals who felt very strongly against Mr. Baker. “You’ve made your bed, lie in it” is typically said to someone who must accept the unpleasant results of something they have done. Within this theme, participants believed that Mr. Baker should be punished, is undeserving of assistance, and has an inability to change his offending behaviour. For example: “He deserves to be in jail” (P#175, DC). Other participants shared this notion, indicating that imprisonment, or being locked away for life, would be best suited for the nature of the crime. Responses within this theme also demonstrated implicit notions as to why Mr. Baker does not deserve support: “I believe these people did this to themselves so they should have to find their own way back into their social life” (P#369, SC). There were also participants who believed that individuals like Mr. Baker will not change and may reoffend if given the opportunity. For example: “… a person changing their ways is pretty unlikely” (P#317, SC). Although this participant alludes to the idea that Mr. Baker would not change, their wording of “a person” might suggest that all individuals, not just people who have committed a sexual offense, are unlikely to change. Further, participant #65 disagreed with spending tax dollars on supportive programs and said, “… You only get one chance with certain things, and if you commit actions that you will permanently traumatize and affect the relationships of the victim for life, you've forfeited the right to your own” (P#65, DC).
Discussion
The current study brings a new perspective to the literature on the reintegration of individuals who have committed a sexual offense, literature that has typically highlighted punitive or unsupportive attitudes from the public. Research has shown that when considering individuals who have committed a sexual offense reintegrating back into the community, the public exhibits emotions such as fear, disgust, and moral outrage (Kernsmith et al., 2009; Stevenson et al., 2015). However, many participants in the present study held generally positive views toward Mr. Baker's reintegration. Our findings suggest that many Canadians support improving mental health services for individuals reintegrating into the community, although attitudes were nuanced when considering the reintegration of an individual with a mental health disorder who has committed a sexual offense. For example, some participants believed Mr. Baker's sexual offending was inherently because of his schizophrenia, but there were no instances of participants attributing the sexual offense to his depression. In fact, some participants in the depression condition agreed that mental illness is not an excuse for sexual offending. Our findings align with Corabian (2017), showing Canadians generally hold neutral views on treatment and endorse both rehabilitation and punishment for those who commit sexual offenses, unlike the more punitive attitudes seen in the United States, Australia, and the United Kingdom (Cowan et al., 2021; Shackley et al., 2014). The current study extends this literature by considering mental health disorders in this population.
While psychotic disorders may influence sexual offending behaviour (Lewis & Dwyer, 2018), most individuals with schizophrenia or depression will never commit a sexual offense (Desmarais et al., 2014). However, Marshall (2007) argued that treating comorbid disorders, particularly psychotic or mood disorders, can reduce sexually deviant tendencies and aid treatment. Some participants in this study agreed, stressing the importance of treating Mr. Baker's mental illness, while others, particularly in the depression condition, saw no connection between his mental health and offending behavior. Moreover, since the public may assume those who commit sexual offenses are inherently mentally ill (Richards, 2018), participants may have overlooked the vignette's mental illness component, as it aligned with this assumption.
Respondents in the present study offered both dispositional and situational explanations for Mr. Baker's sexual offending behavior, aligning with the Belief in Redeemability framework (Maruna & King, 2009). Some participant responses in the You’ve Made Your Bed, Lie in It theme clearly suggested that Mr. Baker's actions were irredeemable and he was unlikely to be rehabilitated. Conversely, responses in the Everyone Deserves a Chance theme were consistent with the belief that people can change, supporting rehabilitation. Some respondents wrote about the treatability of the mental disorder and the potential for rehabilitation, while others suggested that the mental disorder is treatable, but the offending behavior is not. Some emphasized the irredeemability of anyone who has committed a sexual offense, no matter their mental health status. As highlighted by Maruna and King (2009), dispositional attributions aligned with punitive recommendations, although there were also examples of situational attributions associated with punitive recommendations. Mental illness reflects a complex interaction of both dispositional and situational influences, suggesting the need for a more complex framework to capture the range of attitudes toward individuals with a mental health disorder who commit a sexual offense.
Moral Foundations Theory links liberal attitudes with care and conservative attitudes with punitiveness (Harper & Harris, 2017). While we did not examine political orientation specifically, as liberal researchers, we acknowledge its potential influence on participants’ responses and our analysis. For example, punitive You’ve Made Your Bed, Lie In It views likely reflect conservativism, given the “tough on crime” standpoint. Associated with the fairness foundation, this human construction of “right” and “wrong” is based on adherence to the rules of society (Harper & Harris, 2017). Across the dataset, the care foundation, protecting vulnerable members of society, especially children, was prominent, especially within the Concern for Others theme. Supportive views toward Mr. Baker's rehabilitation may also align with the care foundation, emphasizing harm prevention and the community benefits of rehabilitation.
Research shows that language matters and using phrasing like “sex offenders” is associated with higher levels of support for punitive measures compared to the neutral phrasing “those who have committed a sexual offense” (Harris & Socia, 2014). It is possible that many of our participants expressed supportive attitudes toward Mr. Baker because we used person-first language and never referred to him as a sex offender.
Limitations
Some limitations exist in the present study that can be addressed in future research. For example, this study consisted of open-ended survey questions, which can merit less in-depth responses from participants compared to richer interview-style research. Some respondents merely stated “yes” or “no” in response to open-ended questions, possibly because we did not ask them to explain their reasoning every question. Using an open-ended survey allowed us to reach participants across Canada and gather broad, qualitative insights. This flexible, anonymous method let participants respond at their convenience, encouraging input on a stigmatized topic from those who might otherwise avoid qualitative research (Braun et al., 2023). Future research could explore individuals’ narratives through interviews or focus groups to garner a more in-depth understanding of public attitudes.
Many participants assumed that Mr. Baker had offended against a child or wanted offense details, noting their attitudes would vary based on factors like severity or victim typology. Although our vignette was intentionally vague to explore general attitudes toward individuals with mental disorders who have committed sexual offenses, future research could examine how offense specifics influence these attitudes. While prior studies show factors like repeat offending and child victims elicit more punitive views (Harper & Harris, 2017; Kernsmith et al., 2009), it was unclear how the public perceives someone with a mental health disorder who has committed a sexual offense. Providing more detail may have shifted participants’ attention away from the mental health aspect.
Our recruitment methods may have influenced responses. Sharing the poster on Twitter likely attracted individuals with similar research interests (given that authors have used this platform to connect with like-minded academics), while using personal social media, MTurk, Prolific, and a university platform helped reach a more diverse Canadian sample. However, our participants were mostly young, female, White, and highly educated, which may not reflect the broader population. Few had child dependants, an important limitation as parents often hold more punitive views (Burrell & Laskey, 2017; Koon-Magnin, 2015). Therefore, our findings may not fully generalize to all Canadians.
Additionally, MTurk is prone to superworker bias, where participants are familiar with research measures (Chandler et al., 2015). In contrast, Prolific participants typically provide higher quality data, show greater engagement, and follow instructions more closely. Both platforms are widely used in social science research for accessing diverse samples (Albert & Smilek, 2023; Douglas et al., 2023; Peer et al., 2021). Using them in this study helped diversify our sample and yielded meaningful qualitative responses, supporting our recruitment approach.
Implications and Future Research Directions
This study offers practical implications for clinicians and researchers. Understanding public stigma toward those with mental health disorders who have committed sexual offenses can help shape treatment programs that build resilience against these attitudes. Treatment providers should recognize that this population, especially those with complex disorders like schizophrenia, may face additional reintegration barriers. Connecting them with specific community supports, including safe housing, could aid their reintegration. Our findings suggest Canadians conditionally support the reintegration of those who commit sexual offenses (i.e., if they receive treatment), underscoring the need to fund community resources like risk reduction and mental health programs. Public education campaigns targeting misconceptions about mental health (e.g., schizophrenia) and sexual offending could also be beneficial.
Given the limited research on public attitudes toward those with a mental health disorder who have sexually offended, future studies should expand on present findings by exploring other conditions (e.g., personality, substance use disorders) and quantitative methods, such as vignette designs, to examine within-group differences. Theoretical frameworks, such as Belief in Redeemability, Moral Foundations Theory, and Attribution Theory should also be explicitly tested to investigate how political, religious, or community factors influence attitudes.
Supplemental Material
sj-docx-1-fmh-10.1177_14999013251366447 - Supplemental material for Canadians’ Attitudes Toward Community Reintegration of Those with a Mental Health Disorder Who Have Committed a Sexual Offense
Supplemental material, sj-docx-1-fmh-10.1177_14999013251366447 for Canadians’ Attitudes Toward Community Reintegration of Those with a Mental Health Disorder Who Have Committed a Sexual Offense by Bridget Barry, Mallory Coish, Danyelle Fields, Payton McPhee, Jordyn Monaghan and Marguerite Ternes in International Journal of Forensic Mental Health
Footnotes
Acknowledgments
We would like to thank the Canadians who shared their thoughts for the purpose of this study. Thank you to Dr. Eden-Raye Lukacik for the feedback and guidance on this project.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Saint Mary's University.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data are not publicly available due to privacy concerns, but are available upon reasonable request to the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.