
Abstract
Background
Chronic obstructive pulmonary disease (COPD) is a complex respiratory condition that is characterised by progressive decline in lung function, reduced quality of life, impaired exercise capacity, and increased risks of mortality and healthcare resource utilization. 1 Among individuals with COPD, some may experience sudden deteriorations known as Acute Exacerbation of COPD (AECOPD), triggered by factors such as respiratory infections, temperature variations, and air pollution.2,3 Research conducted in the United Kingdom (UK) has shown that individuals with more severe COPD are particularly susceptible to frequent exacerbations. 4 Furthermore, a large UK observational study revealed that individuals with higher baseline exacerbation frequency and severity face an elevated risk of mortality from various causes, including COPD and cardiovascular issues. 2 According to statistics from the National Health Services (NHS), over 128,000 people in the UK were hospitalised due to COPD exacerbation between the years 2016 and 2017 and caring for individuals with COPD disease in the UK costs the NHS an estimated £3 billion annually. 5
Despite the well-documented impact of Acute Exacerbation of COPD (AECOPD) on individuals and healthcare resources as highlighted in quantitative research,3,6,7 there remains a limited qualitative exploration of its burden on patients. A study by Kessler et al. 8 involving 125 outpatient individuals with COPD, revealed that participants experienced variety of symptoms and emotions during exacerbations, including breathlessness, cough, fatigue, pain, anxiety, isolation, and increased reliance on others for daily activities. 8 In a smaller qualitative study, researchers examined how individuals with COPD in an outpatient clinic typically identify an impending exacerbation. In this study, participants reported worsening physical symptoms such as cough, sputum production, functional limitations, and various chest sensations, including soreness and heaviness. 9
Further contributing to this body of research, Harrison et al. 10 conducted a qualitative study to explore patient illness perceptions in a post-AECOPD population. This investigation categorised post-AECOPD individuals into three distinct clusters: (1) in control, (2) disengaged, and (3) distressed patient groups. The distressed cluster exhibited higher levels of breathlessness, greater emotional burdens characterised by symptoms of anxiety and depression, poorer health status, and reduced self-efficacy compared to participants in clusters one (in control) and two (disengaged). 11
While these qualitative studies provided valuable insights into how individuals with COPD experience exacerbations, it is important to note that the data primarily originated from studies that recruited participants in the post-discharge phase. This reliance on patients’ retrospective accounts of their AECOPD experiences may lead to underestimations or overestimations of the true impact during the actual episodes.
To enhance the continuity of care for this population, clinicians must gain a comprehensive understanding of the true impact and burden of acute COPD exacerbations. This understanding should encompass the entire exacerbation experience (before, during, and after attack), which is crucial for identifying unreported barriers that might hinder patient engagement in valuable non-pharmacological discharge services, primarily aimed at improving physical activity, such as Pulmonary Rehabilitation (PR) and community based programmes, which are known for their low uptake within this population,12–14 despite previous efforts to design targeted interventions to enhance participation.10,15
Therefore, the primary objective of this study is to gather an in-depth and comprehensive insight into patients’ real-time experiences during AECOPD, capturing the most authentic account of COPD exacerbation while it is still fresh in their minds. By doing so, this research aims to uncover any unrecognised burdens of exacerbation that may serve as barriers to engagement with non-pharmacological interventions designed for this population and offered at discharge.
Methods
Design
Semi-structured interviews were used to collect the data. The study interview guide was developed by the study author (BA), experts in the field of pulmonary rehabilitation (SS and THD) and a consultant in Respiratory Medicine (NG); (the interview guide is attached in the online supplemental E1). The process started with brainstorming a list of questions related to the AECOPD experience. Open-ended questions were used, and the questions were organised in a logical order using the funnel technique, moving from general questions to more specific ones. 16 Prompts and probes were added to the questions to enable participants to expand on their answers and provide more detail, and a clean-up question was added at the end of the interview to allow participants to raise any uncovered aspects that they considered important. Finally, the questions were tested internally with the study’s authors, and the topic guide was revised to its final version for testing externally on a small cohort of target participants (four AECOPD patients), which then did not result in any further changes.
Setting and recruitment
Participants were recruited from a single secondary care NHS site in the East Midlands, UK. Potential participants were identified from the patient admissions list of the hospital respiratory ward.
Participants and sampling
The participants were conveniently sampled based on the inclusion and exclusion criteria. To be eligible for the study, participants were required to meet the following criteria; (I) be admitted to the hospital with an AECOPD, defined as requiring a significant change in treatment (e.g., bronchodilators, steroids, antibiotics); (II) have the ability to provide informed consent; (III) have a prior clinical diagnosis of COPD; (IV) have suffered from one or more AECOPD exacerbation attacks in the past requiring a hospital admission (to facilitate inquiry about the recovery time point); (V) have a smoking history of >10 pack-years); (VI) have a functional limitation when stable (Extended Medical Research Council Dyspnoea Scale 17 (eMRCD) dyspnoea grade 3–5); and VII) be at least 40 years old. Participants were excluded if they were eligible for palliative care (as scope of needs for this population might be different than our target population).
Data collection, analysis, and reporting
This qualitative study was conducted by a female researcher (BA) with a background in respiratory care and clinical rehabilitation. Detailed, face-to-face, semi-structured interviews (online supplement E1) were conducted at a single time point during hospitalisation, either at the patient’s bedside or in a nearby ward day room. Participants were approached within 48 h of admission, and Potential eligible participants were identified following a daily review of the respiratory ward admission list. Participants recruitment took place between August 2019 and March 2020. The interviews were audio-recorded, and an authorised external transcription service transcribed the data. After each interview, the researcher made field notes, contributing to a comprehensive understanding of the research findings for each patient. 18 Data collection continued until data saturation was deemed to be reached, which was determined through a preliminary analysis of seven patients’ transcripts. 19 Thematic analysis (TA) was primarily conducted by BA, with support from the second reviewer, AB. TA is a method for identifying themes and patterns of meaning in relation to the research question. 16
The TA process involved seven stages: (I) Transcription, (II) data familiarization, (III) generating initial codes, (IV) searching for themes, (V) reviewing themes, (VI) defining and naming themes, and (VII) producing the analysis report. 16 Deductive, semantic, and latent coding techniques were used during the coding process to explore the pre-identified research concepts (experiences before, during and post AECOPD attack). Base themes were generated during the preliminary analysis of the transcripts. Subsequently, further analysis was conducted on the remaining five patients, during which no new base themes emerged. 16 The textual data analysis was conducted in NVivo, a qualitative data analysis software. 20
This manuscript has been written in accordance with the Consolidated Criteria for Reporting Qualitative Research (COREQ). 21 Finally, this qualitative study was part of a larger research project that further explored AECOPD population.
Results
Participant demographics (n = 12).

Footnote- COPD. Severity Classification.
a = COPD severity classified according to the Global Initiative for Chronic Obstructive Lung Disease.
beMRCD = Extended Medical Research Council Dyspnoea Scale.
Semi-structured interviews
The interviews conducted in this study captured three phases (before, during, and post) the AECOPD experience. Through the analysis, three overarching themes, eight themes, and three sub-themes were identified (refer to Figure 1). Thematic map.
Overarching theme 1: Health deterioration phase
Thematic analysis and illustrative participant quotes.

Theme A) COPD symptom flare ups
It was evident that many of the participants perceived their breathlessness to be the first sign of their health deterioration and regarded this as the primary cause behind their hospital admission before any other COPD related symptom that might have co-existed during the AECOPD. Moreover, participants perceived other symptoms as further reasons behind their hospital admission. These symptoms were described as a secondary effect of the breathlessness symptom itself, for example, a decrease in mobility and suffering from panic attacks, or as a standalone exacerbated symptom that happened to cause a heightened level of burden during the exacerbation attack such as suffering from constant cough or mucus build up.
Theme B) Associated co-existing health conditions, and environmental, social and residential risk factors
Flare-up of other co-existing health conditions such as asthma and cardiac diseases were identified as contributing factors to the participants’ current AECOPD. Additionally, challenges such as cold weather, and inability to live in a smoke-free environment due to unsupportive partner were among the stated reasons behind the participants’ health deterioration and subsequent hospitalisation.
Sub-theme C) Help seeking from secondary care services
Participants articulated various medication-related reasons for their help-seeking behaviour, such as complications from prolonged use of inhaled corticosteroids, lack of availability of rescue medication, and the need for modifications to their prescribed treatments. Additionally, positive treatment outcomes the participants received during their last hospitalisation due to an exacerbation, along with their inability to self-manage their condition in the community during these attacks, were also reported as significant reasons that drove them to seek care from secondary healthcare services
Overarching theme 2: Implications of AECOPD and the associated hospitalisation
Thematic analysis and illustrative participant quotes.

Theme A) On-going physical struggles
This theme encompasses the symptoms that contribute to the ongoing physical challenges during hospitalisation phase and has categorised the captured information into three distinct sub-themes. I) Primary symptoms
This sub-theme encompasses the symptoms that led to ongoing physical struggles for the participants and were consistently prioritised in their discussions. The primary symptoms identified were breathlessness and chest tightness II) Secondary symptoms
This sub-theme included symptoms that were expressed or linked by the participants as a consequence of suffering from the primary symptom (breathlessness and chest tightness), and included difficulties with balance, decreases in mobility, pain, fatigue, mucus build-up and cough. III) Associated complications from co-existing conditions
This sub-theme includes both diagnosed and undiagnosed comorbidities that existed during the AECOPD and hospitalisation, impacting the patient’s overall health and exacerbating their physical struggles. These included abdominal aneurysm, hernia, and sleep disturbance.
Theme B) Mental hardship and the associated psychological conditions
Participants described various emotions and psychological conditions during the AECOPD and hospitalisation. Some participants expressed a growing sense of pessimism about their recovery and prognosis stemming from to the continuous deterioration of their health and the perception that their treatment options were becoming increasingly limited.
Additionally, participants reported feelings of uselessness, loss of independence, and vulnerability associated with their current health state. They also experienced sensations of panic and fear, which were often triggered by their inability to breathe as normally as they were accustomed to.
Anxiety emerged as another commonly reported psychological condition, driven by participants’ awareness of their health status and their understanding of the inevitable deterioration associated with AECOPD.
Theme C) Challenges with the hospital environment
Some participants reported feeling agitated by the dryness of the hospital environment, which contributed to pronounced sleep disturbances during their hospitalisation. Additionally, they faced challenges in implementing the new advice provided by their healthcare providers to manage their current condition. One participant noted experiencing pain while attempting the breathing techniques suggested by their healthcare provider, while others reported conflicts with hospital staff and fellow patients.
Overarching theme 3. Recovery journey
Thematic analysis and illustrative participant quotes.
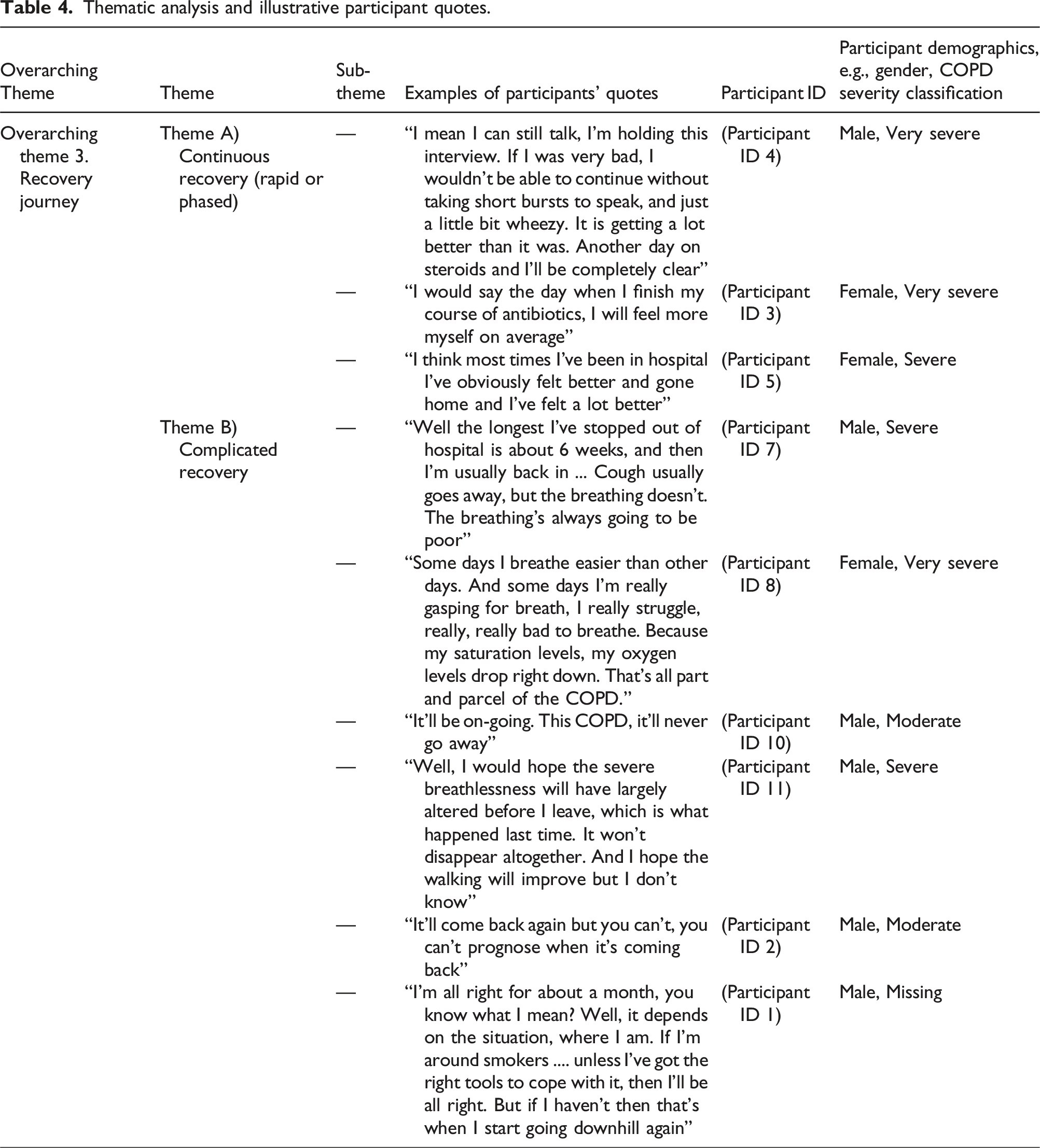
Theme A) Continuous recovery (rapid or phased)
In this theme, some participants reported achieving full recovery in a rapid manner during hospitalisation due to the pharmacological treatment they received, while others experienced a phased recovery, beginning in hospital and continuing to progress after discharge.
Theme B) Complicated recovery
Several participants articulated that they could achieve full recovery from other related respiratory symptoms such as cough, but they consistently noted that breathlessness would always be present, viewing it as a never-ending struggle. Additionally, another participant emphasised that any improvement in breathlessness would be in terms of its severity, but it would never completely disappear.
An element of uncertainty regarding prognosis and anticipation of another relapse of symptoms was also evident in the participants’ statements. One participant articulated that their recovery largely depended on their ability to effectively manage their exposure to passive smoking. They believed that their current living situation with an actively smoking partner would likely lead to further COPD events in the future.
Discussion
This study aimed to explore the experiences of individuals with AECOPD at different exacerbation phases (before, real-time, and post-AECOPD). By obtaining firsthand accounts of the exacerbation event, we aimed to minimise potential recall bias often found in retrospective studies.8,9 Our study revealed that breathlessness was consistently identified as the primary and most burdensome symptom contributing to health deterioration during AECOPD. Participants sought help from secondary healthcare services, as they believed that their current medical regimen and self-management strategies were inadequate to resolve their exacerbated condition. Exacerbated comorbidities and seasonal changes were identified as perceived risk factors for hospitalisation. Notably, mental hardship emerged as a critical theme during the hospitalisation phase, highlighting the emotional toll experienced by individuals with AECOPD.
The prominent and on-going burden of breathlessness was also reported in a previous retrospective qualitative study that looked into patients’ experiences of identifying approaching AECOPD. Participants identified increased breathlessness, labelled the “invisible symptom” as a burden that has to be faced during the acute exacerbation phase. 9 Additionally, this qualitative study highlighted other findings similar to our study with regard to the presence of other exacerbated symptoms, which they called the “visible symptoms” that individuals usually experience during an exacerbation attack, such as cough and limited mobility. 9 The recent findings, along with our own, could help clinicians understand the most commonly perceived symptomatic burden experienced by individuals with acute exacerbations of chronic obstructive pulmonary disease (AECOPD). This understanding could guide interested clinicians in implementing symptom management strategies for AECOPD patients that focus on the most burdensome impacts. Ultimately, this approach could further enhance the patient-centered care and potentially improve engagement in health-related discharge interventions. 23
Similarly, a previous quantitative study by Calverley et al. 24 identified the level of breathlessness score (measured by the modified Medical Research Council scale breathlessness score) was among the most critical risk factors of hospitalisation due to COPD. 24 Furthermore, it has been reported in the literature the dyspnoeic experience causes AECOPD sufferers to exhibit a cycle of emotional and physical disabilities that have a complex relationship, which can result in intractable breathlessness that leads individuals to display help-seeking behaviours in the form of emergency room visits and subsequent hospitalisation. 25
Participants in our study identified cardiac disease and adverse weather conditions as significant risk factors for their hospitalisation. This aligns with recent research that has established a link between cardiac comorbidities and AECOPD readmissions. 26 Common cardiovascular diseases associated with AECOPD include pulmonary arterial hypertension, systolic dysfunction, and coronary artery disease. 27 Moreover, another study found that AECOPD hospital admissions peaked during the midwinter months, 28 and highlighted seasonal factors as an independent contributor to increased hospitalisations. 29
Interestingly in our study, some participants noted that a lack of available rescue medication during their COPD exacerbation led them to seek help from secondary healthcare services. This finding may explain the frequent and short hospital admissions experienced by certain groups of patients with AECOPD. It highlights the vital role of a comprehensive COPD action plan, which empowers patients to effectively manage their symptoms.
A previous study investigated primary and secondary care perspectives in multiple European countries regarding self-management approaches for AECOPD. In this study, many respiratory clinicians expressed support for using rescue packs, which may include steroids alone or in combination with antibiotics, as a means for patients to self-manage exacerbation attacks. However, they emphasised that access to these options should be limited to selected patients who have received appropriate education and risk management. 30
The idea of a pharmacy-based model of the COPD action plan has been implemented recently in a pilot study, 31 which has shown promising results; however, its proven efficacy requires further investigation in larger trials. By prioritising medication management and patient education, these innovative strategies hold considerable potential to enhance self-management and reduce frequent hospital admissions.
During hospitalisation, individuals with AECOPD in our study often encountered mental challenges, such as panic attacks triggered by the sensation of breathlessness. Barrera et al. 32 described how panic attacks in COPD patients can be induced by the combination of breathlessness and a heightened state of anxiety, leading to physiological sensations and anxious apprehension that culminate in a panic attack. 32 Research has shown that individuals with panic attacks tend to engage in avoidance behaviours, such as evading breathlessness, which can lead to reduced physical activity, increased risk of disability, diminished quality of life, and higher hospitalisation rates among COPD patients.33,34 In the case of AECOPD, individuals experiencing complex recovery due to breathlessness may develop even more escalated avoidance behaviour, potentially influencing their decision to participate in non-pharmacological interventions with an exercise component, such as pulmonary rehabilitation (PR), which they might perceive as a reason that could lead to a heightened level of breathlessness.
Furthermore, our study findings align with previous research, indicating that ongoing anxiety about future breathlessness episodes and feeling vulnerable due to AECOPD have a significant psychological impact, leading individuals to express pessimistic attitudes about never achieving full recovery and feeling of being useless.35,36 These pessimistic attitudes can be understood as a consequence of the challenging recovery journey experienced by patients. In the literature, complicated recovery post-AECOPD has been associated with viral and cold symptoms, wherein the affected individuals usually require oxygen therapy and assistance with physical limitations to extend beyond hospitalisation.37,38
Moreover, our data suggest that the accumulated experiential knowledge of individuals with AECOPD during complex recovery, along with the perception that breathlessness is an inherent part of COPD, may contribute to patients declining new treatment options in the future, as they might perceive that nothing seems to work for their deteriorating condition. These findings uncover hidden barriers that might influence uptake of discharge services such as PR within this population, indicating a growing need to incorporate targeted behavioural interventions as intermediate interventions before patients are prompted to make decisions about discharge services. Among the interventions that have shown promising results with COPD and other chronic illnesses in tackling negative illness perceptions and fostering positive transformative changes in behaviour and illness perceptions are Cognitive Behavioural Therapy (CBT), 39 Acceptance and Commitment Therapy (ACT) 40 and the Meaning Perspective Transformation Model (MPT).41–43
Overall, this study highlights the multifaceted experiences of individuals with AECOPD and underscores the importance of integrating both pharmacological and behavioural interventions for effective AECOPD management. However, it is essential to acknowledge that our study demonstrates one key strength and several limitations that merit consideration.
The study’s main strength lies in its recruitment of hospitalised individuals suffering from AECOPD, allowing for a more accurate capture of their experiences during the real COPD exacerbation event while it is still fresh in their minds. By conducting interviews during hospitalisation, the study overcomes the limitations of relying on post-event recollection, which can be affected by memory issues, particularly in older adults. 44 Episodic memory, defined as the long-term explicit memory of a person’s unique recollection of experiences and events, has been shown to improve with environmental support, such as cues or instructions. 45 Thus, the study utilised the patients’ current experiences as cues or stimuli to evoke their episodic memory, enhancing the authenticity of their recollections (reflecting on how challenging things were before, during (real time), and after the exacerbation while it is still fresh in their minds).
Conversely, It is important to mention that the results of this study are limited in their generalisability to the entire AECOPD population due to the qualitative design and specific limitations: a single-centre approach, a predominance of participants from a single ethnic group (White British), and a higher proportion of males. We believe that replicating this study with a more diverse participant group and employing different sampling techniques to capture maximum variation in the condition would facilitate future data triangulation. This would enable the building of evidence and provide a clearer and more inclusive picture of the lived experiences of these individuals. Additionally, in this study the fact that the second reviewer did not independently code the study’s transcripts during the initial steps of the analysis may be viewed by some qualitative researchers as a limitation to the reliability of the findings. Methods of quality checks in qualitative research, such as calculating inter-rater reliability, which involves two or more researchers coding the data independently and then assessing the level of agreement in a quantitative manner, have sparked considerable debate in the field. 16 Thus, we believe that since reliability checks pertain to the trustworthiness of interpreting textual data, the iterative process we employed in the subsequent steps of our analysis could still ensure a reasonable level of reliability in the produced findings. Furthermore, in this study, the sample from the targeted population was only involved in testing of the study guide, but not in its development. This could also be viewed as limitation to the validity of the constructed research tool, as involving participants in the development of the interview guides not only the testing is increasingly recognized as an important aspect of enhancing the face validity research tools.
Finally, in this study, we focused on individuals experiencing Acute Exacerbation of Chronic Obstructive Pulmonary Disease (AECOPD) during hospitalisation, aiming to help them use their current experiences as cues to recall how they felt before, during, and after the AECOPD event. However, it is important to note that while this approach may enhance their recall ability, it may not completely eliminate recall bias, as accounts of recovery were still collected retrospectively. Thus, we recommend conducting interviews at two distinct time points: during the AECOPD attack and after recovery. This dual approach could provide valuable insights and significantly enhance the quality of the research.
Conclusion
COPD symptoms, co-existing conditions flare ups, and lack of ability to self-manage these symptoms lead patients to a hospitalisation for AECOPD. In our study, it was evident that breathlessness was considered by the patients to be the most burdensome symptom throughout different COPD exacerbation time points. The on-going struggle with this symptom led to various other associated physical and psychological distress. Some individuals with AECOPD navigate a complicated recovery journey, which can lead to significant psychological consequences that require targeted behavioural interventions. It is crucial that interventions aimed at individuals with AECOPD are appropriately phased within the management process to facilitate patient engagement and optimise treatment outcomes.
Moreover, empowering patients with effective self-management strategies and resources is essential in reducing hospitalisations and improving quality of life. Future research should focus on the implementation of tailored interventions and evaluate their effectiveness in enhancing self-management and overall health outcomes for this population. By addressing these challenges, we can potentially move toward a more patient-centred approach in managing AECOPD and further enhance the healthcare delivery.
Supplemental Material
Supplemental Material - Real-time experience of an acute exacerbation of COPD: A qualitative exploration
Supplemental Material for Real-time experience of an acute exacerbation of COPD: A qualitative exploration by Bedor S. Alkhathlan, Amy C. Barradell, Neil J. Greening, Theresa Harvey-Dunstan and Sally J. Singh in Cross-Cultural Research
Footnotes
Ethical statement
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financially funded as part of a PhD scholarship by Jazan University and the University of Leicester. The sponsors were not involved at any stage of this study, from the design until manuscript submission.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The information regarding the interview guide are available within Figshare link 10.6084/m9.figshare.25254574.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.