
Abstract
This study aims to translate, culturally adapt, and test the reliability and construct validity of the Brazilian Portuguese version of the Basic Psychological Needs in Exercise Scale (BPNES) for patients with Chronic Obstructive Pulmonary Disease (COPD) and Interstitial Lung Disease (ILD). Pulmonary function, dyspnea, quality of life, anxiety and depression symptoms, and functional status were assessed, and two raters independently applied the BPNES. BPNES scores were compared between raters' applications to assess reliability, internal consistency, and agreement. Confirmatory Factor Analysis was used to assess the factor structure of the BPNES model.
Results
59 patients were included (61% with COPD and 39% with ILD). BPNES factor scores were not significantly different between raters’ assessments (p > 0.05). The internal consistency was 0.70 for autonomy, 0.76 for competence, and 0.80 for relatedness. Inter-rater and test-retest reliability were good to very good for autonomy (ICC = 0.78, 95%CI 0.62–0.87; ICC = 0.75, 95%CI 0.57–0.86, respectively), competence (ICC = 0.81, 95%CI 0.68–0.89; ICC = 0.65, 95%CI 0.43–0.80, respectively), and relatedness (ICC = 0.79, 95%CI 0.65–0.88; ICC = 0.70, 95%CI 0.50–0.83, respectively). Significant correlations were observed between BPNES factors and quality of life, anxiety, depression, and functional status. In conclusion, this study confirmed the reliability and construct validity of the Brazilian Portuguese version of the BPNES in patients with COPD and ILD.
Keywords
Introduction
Pulmonary rehabilitation (PR) aims to improve the overall health status of patients with chronic lung diseases by promoting health-related behavioral changes, especially in physical activity.1,2 Although guidelines recommend promoting exercise-related behavior change, the use of behavior change theories and strategies to implement these approaches is not widespread in most rehabilitation interventions.3–5
The latest report on pulmonary rehabilitation from the American Thoracic Society includes only two behavior change techniques as desirable components: goal setting and physical activity counseling. 2 Despite notable progress, there is still a lack of coordination between prescribing rehabilitation programs, promoting behavior change interventions, and utilizing theories underlying such changes. This lack of implementation could contribute to the difficulties in fostering health-related behavior changes among patients undergoing pulmonary rehabilitation. 5
The need to promote behavior change 6 was even more evident during the COVID-19 pandemic, 7 which exposed people to physical inactivity and sedentary behavior 8 due to restrictions imposed. For instance, most patients with Chronic Obstructive Pulmonary Disease (COPD) were unable to maintain their exercise routines at home since the rehabilitation programs they attended failed to promote behavior change. 9 Alternatively, telerehabilitation has been shown to improve outcomes equivalent to traditional center-based pulmonary rehabilitation for individuals with chronic respiratory disease. 10 However, exercise-related behavior change has still not been acquired.
Frameworks such as the Self-Determination Theory (SDT) explain the role of motivation in the behavior-change process.11,12 The quality of a person’s motivation is affected by the degree to which the social context fulfills their Basic Psychological Needs (BPNs), namely autonomy, competence, and relatedness. 13 This fulfillment facilitates maintaining behaviors such as exercising more autonomously. 14 Autonomy relates to choice, where individuals choose their behavior. Competence reflects the ability to interact positively with the environment, while relatedness pertains to acceptance, belonging, and meaning.11,15
Considering the vital role that BPNs play in promoting behavior change,16,17 PR should assess this outcome with a valid and reliable tool. The Basic Psychological Needs in Exercise Scale (BPNES) assesses how people perceive the fulfillment of autonomy, competence, and relatedness in organized exercise settings.18,19 The BPNES has been proven to be valid and reliable previously in the general healthy population of exercise participants who speak Greek,19,20 English, 18 Spanish, 21 and Portuguese from Portugal, 22 but not in Brazilian Portuguese.
Thus, this study aims to translate, culturally adapt, and test the reliability and construct validity of the Brazilian Portuguese version of the BPNES for patients with COPD and Interstitial Lung Disease (ILD).
Methods
The study involved translation, cultural adaptation, reliability, and construct validation. It was approved by the Ethics Committee for Research Involving Human Beings of Santa Catarina State University (CAAE: 39702214.6.0000.0118 and 02360518.3.0000.0118). All participants signed the free and informed consent form.
Patients referred to the Center of Assistance, Teach, and Research in Pulmonary Rehabilitation (NuReab) from Santa Catarina State University were screened from 2018 to 2020. The inclusion criteria for the study were patients with a clinical diagnosis of COPD (confirmed by spirometric classification GOLD II-IV) 23 or ILD (confirmed by computed tomography or pulmonary biopsy), 24 aged 18–80 years, and clinical stability in the previous month (without worsening of dyspnea, cough, or sputum; medication changes or hospitalization). Exclusion criteria were cardiovascular, neurological, or other diseases in which clinical manifestations and symptoms would interfere with the assessed outcomes, inability to understand the questionnaires (a Mini-Mental State Examination score of 18/19 for patients without formal education and a score of 24/25 for patients with formal education), 25 smoking in the previous 6 months, and current participation in PR or discharge from it in the last 6 months. The last two could also influence motivational profiles.
The entire protocol was conducted according to standardized guidelines for the translation and cross-cultural adaptation process 26 and to the Consensus-based Standards for the Selection of Health Measurement Instruments (COSMIN). 27
Translation and cross-cultural adaptation
The translation into Brazilian Portuguese was performed using the 11-item version validated in English 18 since the original 12-item scale is in Greek. 19 First, two independent translators, one of whom was not from the healthcare field, translated the scale into Brazilian Portuguese. Afterward, a single version was developed in Portuguese to be back-translated to English. A native English speaker, fluent in Brazilian Portuguese and without contact with the scale, performed the back-translation process. Finally, the back-translated English version was sent to the primary author of the original BPNES article, who, along with other health professionals and translators, was part of the committee that had approved the first version of the scale. The first version of the Brazilian Portuguese BPNES was tested with 10 patients, to identify comprehension problems and doubts. These patients were selected based on the same inclusion and exclusion criteria and only participated in this phase of the process. All of them had COPD, with five male and five female participants, aged 71.6 ± 6.57, and FEV1 39.1 ± 13.2% of the predicted value. Detailed information about this phase can be found in the supplemental material. No modification in the BPNES were necessary, and the validation process was completed successfully. Therefore, the final version of the Brazilian Portuguese BPNES scale could be administered to the study sample. This version of the BPNES in Brazilian Portuguese is available at https://www.udesc.br/cefid/nureab
Data collection
Independent raters (Rater 1 – R1: HFF and Rater 2 – R2: SGG) administered the BPNES as an interview between the rater and patient, twice on day 1, with an interval of 25–35 min between assessments. After 15–20 days, R2 reapplied the BPNES.28,29
The BPNES assesses the patient’s perceptions regarding the fulfillment of BPNs in exercise. It consists of 11 items divided into three factors: autonomy, relatedness, and competence, with Likert-type responses ranging from 1 (“I disagree”) to 5 (“I completely agree”). Each BPN score can be presented by the average of the items, which ranged between one and five. 18 The higher the score, the greater the satisfaction of BPNs.
Other assessments performed on day one were: 1) pulmonary function using the MasterScreen Body whole-body plethysmograph (Erich Jaeger®, Friedberg, Germany) or EasyOne® spirometer (Ndd Medical Technologies, Zurich, Switzerland); 30 2) dyspnea (modified Medical Research Council scale - mMRC); 31 3) quality of life (St George Respiratory Questionnaire - SGRQ); 32 4) symptoms of anxiety and depression (Hospital Anxiety and Depression Scale - HADS); 33 5) functional status (London Chest Activity of Daily Living - LCADL). 34 Raters (R1 and R2) were physiotherapists with a comprehensive experience in these outcome assessments. At the time of the assessments, no patient was engaged in PR.
Statistical analysis
IBM SPSS Statistics® version 20.0 (IBM Corporation, Armonk, NY, USA) was used for data analysis, except for the Confirmatory Factor Analysis (CFA), which was conducted using Jamovi free software Version 2.3.16.0 (The jamovi project 2022. Retrieved from https://www.jamovi.org). GraphPad Prism version 5.0 (GraphPad Inc., San Diego, CA, USA) was used to create figures.
The CFA evaluated the overall model fit of the 3-factor BPNES. Descriptive statistics for the items were calculated to assess normality based on univariate item skewness and kurtosis, as well as the normalized estimate of Mardia’s multivariate kurtosis. For Mardia’s value greater than 5, the robust method by Satorra and Bentler was used to correct the fit indices for non-normality. 35 Multivariate outliers were identified using the Mahalanobis distance statistic D2. 36 The BPNES items were specified to load onto the originally described factors, latent factors were allowed to correlate, and item uniquenesses were specified as uncorrelated. The robust maximum likelihood method of estimation was used. Several goodness-of-fit indices assessed the model’s overall quality, 36 including the Satorra-Bentler scaled χ2 value (S-Bχ2), χ2/df, Comparative Fit Index (CFI), Incremental Fit Index (IFI), Root Mean Square Error of Approximation (RMSEA) with its’ 90% confidence interval (90% CI), and Standardized Root Mean Residual (SRMS). Acceptable values for these indices were defined as follows: S-Bχ2 with values below three, CFI and IFI with values higher than 0.95, and RMSEA and SRMS with values equal to or less than 0.08. 37
Cronbach’s alpha coefficient was used to verify internal consistency. 38 The intraclass correlation coefficient (ICC) was used to test data reliability based on the classification by Fleiss et al. 39 Limits of agreement between inter-rater (R1 vs. R2) and test-retest (R2, assessment one vs. R2, assessment two) applications were verified with Bland-Altman plots and with paired t-tests or Wilcoxon tests. The standard error of measurement (SEM) was calculated using the following equation: SEM = SD√(1-ICC), where SD is the standard deviation of the scale scores applied by R1. The minimum detectable change (MDC) was calculated using the equation MDC = 1.96.√2.SEM. 28 The proportion of the minimum and maximum scores calculated floor and ceiling effects. Construct validity of BPNES was tested using Pearson’s or Spearman’s correlation coefficient, considering the SGRQ (total score and domains), HADS (total score and domains), and LCADL (total score and percentage of total). The significance level was set at 5%. The sample size was determined based on the COSMIN recommendation of at least 50 patients. 40
Results
Characteristics of the sample regarding anthropometry, lung function, dyspnea, quality of life, functional status, and symptoms of anxiety and depression.

Values are expressed as mean (standard deviation) unless otherwise indicated:
aResults presented in absolute frequency.
bResults presented in median [interquartile range].
COPD: Chronic Obstructive Pulmonary Disease; ILD: Interstitial Lung Disease; BMI: body mass index; kg: kilogram; m: meters; kg/m2: kilogram per square meter; FEV1: forced expiratory volume in one second; FVC: forced vital capacity; L: liters; %pred: percentage of the predicted value; mMRC: modified Medical Research Council scale; mSGRQ: modified Saint George Respiratory Questionnaire; LCADL: London Chest Activity of Daily Living; HADS: Hospital Anxiety and Depression Scale.
Confirmatory factor analysis of the Basic Psychological Needs in Exercise Scale (BPNES).
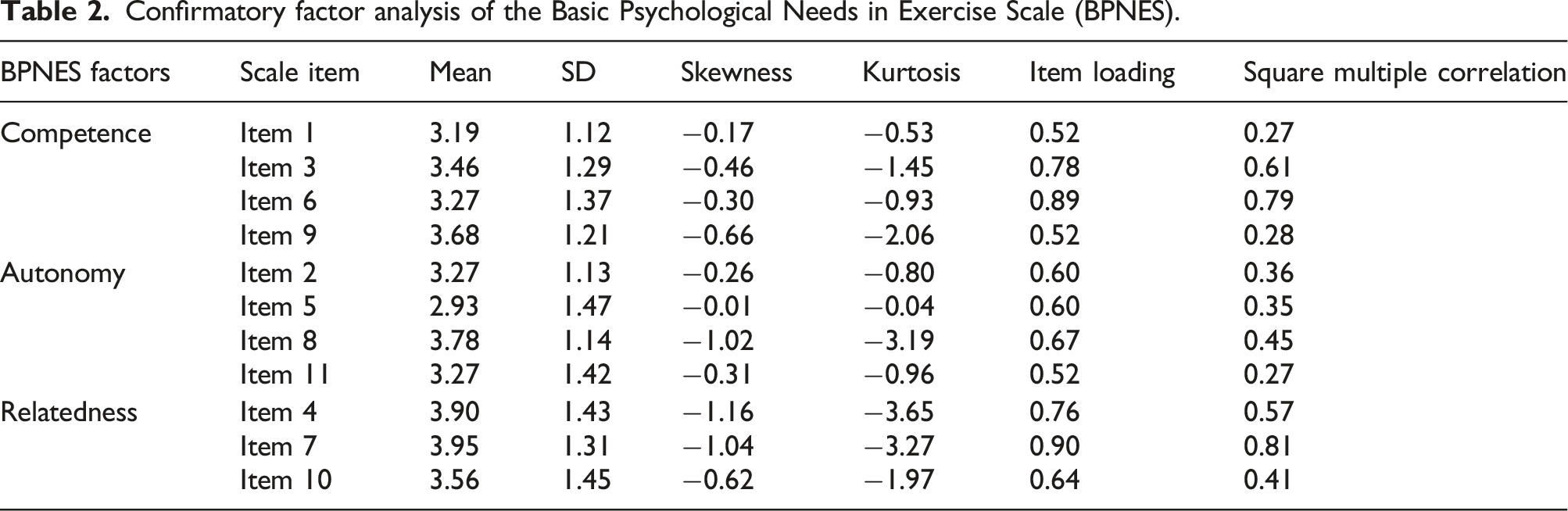

Confirmatory factor analysis of the Brazilian version of the Basic Psychological Needs in Exercise Scale (BPNES). Notes. BPNES: Basic Psychological Needs in Exercise Scale.
The internal consistency was 0.70 for autonomy, 0.76 for competence, and 0.80 for relatedness. Excluding any item did not result in a higher Cronbach’s alpha for BPNs. The total items' internal consistency was 0.86. Inter-rater and test-retest reliability were good to very good for autonomy (ICC = 0.78, 95%CI 0.62–0.87; ICC = 0.75, 95%CI 0.57–0.86, respectively), competence (ICC = 0.81, 95%CI 0.68–0.89; ICC = 0.65, 95%CI 0.43–0.80, respectively), and relatedness (ICC = 0.79, 95%CI 0.65–0.88; ICC = 0.70, 95%CI 0.50–0.83, respectively). The mean scores of the BPNES factors in inter-rater and test-retest applications were not significantly different, reinforcing their reliability and agreement (p > 0.05, Figure 2) (Table 3). Regarding the ability of BPNES to reflect changes at extremes of the scale, the findings indicated that autonomy and competence had a ceiling effect of 3.4% and 5.1%, respectively, and no floor effect. Relatedness had a ceiling effect of 20.3% and a floor effect of 8.5%. Bland-Altman plots for the inter-rater reliability (upper) and test-retest reliability (lower) of the Brazilian version of the Basic Psychological Needs in Exercise Scale (BPNES): (a) Autonomy, (b) Competence, and (c) Relatedness. Basic psychological needs scores, comparison of scores between raters and between test-retest, and reliability of the Brazilian version of the Basic Psychological Needs in Exercise Scale (BPNES).

Autonomy correlated with mSGRQ total and Impact (r = −0.35; r = −0.27, respectively), HADS total and depression (r = −0.30; r = −0.34, respectively), and with LCADL%total (r = −0.32). Competence correlated with mSGRQ total, Activity, and Impact (r = −0.35; r = −0.35; r = −0.34, respectively), HADS total, and Depression (r = −0.30; r = −0.37, respectively) and with LCADL%total (r = −0.38) (p < 0.05 for all outcomes). Relatedness was not associated with any variable tested (p > 0.05).
Discussion
The results of the present study, which aimed to translate, culturally adapt, and test the reliability and construct validity of the Brazilian Portuguese version of the 11-item BPNES for patients with COPD and ILD, confirm its reliability and construct validity for assessing the BPNs related to exercise in this population. The three-factor scale structure of the 11 items was preserved. No cross-cultural adaptations were necessary, as the BPNES covers universal issues related to exercise practice, and no specific psychological terminology appears in the BPNES.
The BPNs of autonomy, competence, and relatedness are central concepts of SDT and play an essential role in understanding individuals’ motivation toward a specific behavior.11,15 According to SDT, each BPN plays a distinct and necessary part in an individual’s life, and neglecting any of them can result in significant negative consequences. 41 Therefore, studying them individually in PR or other rehabilitation settings can provide helpful information on individuals’ motivational profiles. 22 For instance, it may provide valuable clues to an individual’s needs. Based on this profile, behavior change techniques can be intentionally selected and delivered, avoiding an ineffective one-size-fits-all approach.9,42
Theoretical assumptions of three distinct BPNs were confirmed, which is consistent with previous studies that demonstrated good model fit for both the 11- and 12-item BPNES in healthy exercise participants.18–20,22,43 As previously reported, 22 the items' structure represents each BPNES construct strongly. The correlations between the BPNES constructs are consistent with the theoretical foundations of SDT.41,44 This phenomenon seems to occur independently of the study population or the method used to measure the BPNs. 22
The BPNES is a suitable instrument for clinical practice, where various staff members can perform patient assessments on different days. Despite acceptable reliability, the ICCs, particularly test-retest, were lower than previously reported in larger general exercise participants samples.19,22,45 Although the disease’s symptoms were monitored to ensure the chronic respiratory disease’s stability throughout the entire protocol, it may have led to slight variability in responses on different days, depending on individuals' well-being fluctuations.15,46 Besides, the BPNES scores in each assessment confirm the agreement and stability of the measurements. Also, the MDC found for each BPN can guide the interpretation of interventional results. Alterations above the MDC are assumed to be real. 47
Previous studies showed higher BPNES factor scores than ours. Effects can differ for individuals whose reasons for exercising are disease-related, mainly when exercise is part of disease management. 48 Individuals with COPD and ILD may exercise for disease management purposes rather than personal interests or motivations. These diseases can lower one’s sense of self-worth, self-protection, or belief in their ability to carry out daily activities successfully, resulting in an unwillingness to engage in specific activities. 13 This may lead to lower satisfaction and even frustration, ultimately resulting in lower BPN scores.
In the present study, the floor and ceiling effects of the 11-item Brazilian Portuguese version of the BPNES were below the accepted cut point, 28 except for the ceiling effect of relatedness, which was slightly higher. A discussion regarding this topic can be found in the supplemental material.
The present study is the first to test and provide initial evidence supporting the construct validity of BPNES scores among individuals with COPD and ILD using other constructs such as quality of life, anxiety, depression, and functional status. The results suggest that the perceived support for autonomy and competence could reflect better disease-related quality of life, less anxiety and depression, and better functional status. The literature has extensively reported the relationship between BPNs and better health outcomes. 49
Since no other instrument is available in Brazilian Portuguese to assess the BPNs in exercise for general or disease-specific populations, criterion validity could not be tested. It could be pointed out as a limitation of this study, and future research must address this topic. In the absence of a gold standard instrument and to test at least one type of criterion validity of the BPNES, we decided to assess complementary constructs to verify its construct validity. Additionally, we present the reliability analysis with a sample size slightly smaller than recommended. 40 Although we reached the COSMIN recommendation of at least 50 subjects, we want to make a statement. Data collection was interrupted due to the COVID-19 pandemic for almost 2 years. Given the length of the interruption, we understood that restarting data collection to achieve a sample size close to 100 would create significant measurement bias. Furthermore, patient-reported outcomes, especially behavior-related ones, such as the BPNs, could have been drastically influenced by the restrictions imposed by COVID-19. 7 Despite this, all the analyses are aligned and consistent with previously described findings related to the BPNES in other languages, age groups, and contexts. This present Brazilian Portuguese version of the BPNES should be tested in other health conditions and populations, given the universal nature of the concepts of the SDT constructs.
This study was the first to test the reliability and validity of the Brazilian Portuguese version of the BPNES in individuals with chronic respiratory diseases of COPD and ILD. Using an instrument to assess the BPNs in exercise provides insight into future strategies to focus on the needs that are not highly satisfied. Specific behavior change strategies can be tailored to that particular BPN within the exercise protocol, creating a more autonomous and supportive environment to promote behavior change and adopt more active and healthy lifestyles in the long run.6,50 Furthermore, this study may serve as a starting point for future research on other measurement properties of the scale, such as responsiveness to PR and the establishment of cutoff points.
Conclusion
The Brazilian Portuguese version of the Basic Psychological Needs in Exercise Scale is reliable and valid for assessing Basic Psychological Needs related to exercise in patients with COPD and ILD.
Supplemental Material
Translation, cross-cultural adaptation, reliability, and construct validity of the Brazilian Portuguese version of the Basic Psychological Needs in Exercise Scale
Supplemental Material for Translation, cross-cultural adaptation, reliability, and construct validity of the Brazilian Portuguese version of the Basic Psychological Needs in Exercise Scale
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Fundação de Amparo à Pesquisa e Inovação do Estado de Santa Catarina, FAPESC/Brazil (PAP UDESC, Chamada Pública N° 04/2018, Termo de Outorga 2019TR658).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.