
Abstract
Objectives
Individuals dependent on long-term mechanical ventilation (LTMV) for their day-to-day living are a heterogenous population who go through several transitions over their lifetime. This paper describes three transitions: 1) institution/hospital to community/home, 2) pediatric to adult care, and 3) active treatment to end-of-life for ventilator-assisted individuals (VAIs).
Methods
A narrative review based on literature and the author’s collective practical and research experience. Four online databases were searched for relevant articles. A manual search for additional articles was completed and the results are summarized.
Results
Transitions from hospital to home, pediatric to adult care, and to end-of-life for VAIs are complex and challenging processes. Although there are several LTMV clinical practice guidelines highlighting key components for successful transition, there still exists gaps and inconsistencies in care. Most of the literature and experiences reported to date have been in developed countries or geographic areas with funded healthcare systems.
Conclusions
For successful transitions, the VAIs and their support network must be front-and-center. There should be a coordinated, systematic, and holistic plan (including a multi-disciplinary team), life-time follow-up, with bespoke consideration of jurisdiction and individual circumstances.
Keywords
Introduction
Individuals dependent on long-term mechanical ventilation (LTMV) for their day-to-day living are a heterogenous population whose prevalence has steadily been rising secondary to technological and clinical care advances.1–3 With this associated increase in survival, the ventilator-assisted individual (VAI) may experience several crucial healthcare transitions during their lifetime. Rose et al. 4 defined seven key transitions in a 2014 Delphi study: 1) acute care to prolonged mechanical ventilation (PMV)/LTMV, 2) PMV to LTMV, 3) PMV/LTMV to acute care 4) no ventilation to PMV/LTMV, 5) institution/hospital to community/home, 6) pediatric to adult PMV/LTMV, and 7) active treatment to end-of-life (EOL). 4 Healthcare transitions are monumental for VAIs as they represent important shifts in care, commonly involve unanticipated complexities, and are often regarded as challenging or overwhelming.5–8 Based on the literature and our collective clinical and research experience, this narrative review 9 will describe three of the most complex and multi-faceted transitions experienced by VAIs including 1) institution to community, 2) pediatric to adult care, and 3) active treatment to EOL care.
Methods
There are many clinical practice guidelines1,2,10–15 that provide systematic and evidence-based information for adults and pediatric VAIs. There are various definitions of LTMV; for this review we only included articles addressing populations who are dependent on mechanical ventilation for ≥6 h/day for ≥21 consecutive days. 4 Mechanical ventilation included invasive via tracheostomy and non-invasive. Abstracts only, protocols, letters, editorials, and articles describing other LTMV transitions were excluded.
Although this is a narrative review a systematic search of Medline, CINAHL, Cochrane CENTRAL, and Scopus (SUPPLEMENT) was conducted (onset-June 2022). MLN removed duplicates in Endnote™ (Philadelphia, USA), then in Covidence (Melbourne, Australia), followed by MLN and RA independently reviewing all title/abstracts. Each author took lead in summarizing the literature for one of the three transitions. During the writing of these sections authors also hand searched reference lists of relevant articles to supplement content. All authors contributed to the Introduction/Background, and Discussion.
Results
Study selection
Our search produced 4,459 articles (Figure 1) with 895 duplicates, and 148 full text articles reviewed for eligibility. After an additional 30 articles from manual searches, a total of 99 articles were included. PRISMA flow diagram.
Transition from hospital to home
The transition from hospital to home for VAIs requires careful planning and coordination with the VAI and their support network, the healthcare team, equipment providers, and funding bodies.1,2,10,12,13,16 A seamless transition requires timely acquisition of medical equipment for discharge,4,17 early initiation of transition processes,4,18 and robust training programs. Transition delays have negative impacts on health status and quality of life 7 and increased monetary costs for both the VAI and healthcare system.19–22 Discharge home can be completed within weeks, but the “normality” of being at home takes years to be established.18,23–25
Healthcare/medical considerations
Before going home, the VAI must be physiologically stable, especially if there is a tracheostomized airway.1,2,10–13,26 The specific duration of stability differs from individual to individual. 27 The VAI should be moved from a critical care ventilator to a home mechanical ventilator, 28 have adequate gas exchange, and, if possible, be able to tolerate brief interruptions in ventilation.1,4 This period can range from 2-weeks (invasive ventilation) to 48 h (non-invasive ventilation), 1 dependent on the individual.
Ongoing support and lines of communication from an interprofessional healthcare team, with a “most responsible physician” to lead care is key, all with expertise and experience in LTMV.1,2,10–13,29 Long-term and holistic support is required because this population is medically fragile with trajectories characterized by frequent intercurrent illnesses and/or a declining prognosis.1,2,23 Representatives from both the hospital and community setting are integral 30 including providers responsible for overall care coordination, managing the underlying illness, respiratory and ventilation needs, nutrition, ambulation, physical rehabilitation, psychological and social needs, counseling services, day-to-day care, and equipment provision.1,2,10–13 The healthcare team is an asset when advocating, communicating, and providing care and education. 23 However, there is a point when they must “let go” of the expectation (moral distress 31 ) of a “perfect” home situation and concentrate on the family’s strengths and circumstances.1,23,31
VAI and their support network
It is very important that the VAI and their support network make an informed choice to live at home.2,4 If the VAI has the capacity, being able to direct their own care contributes to a successful transition.1,4
Having informal or family caregivers available is paramount,1,2,4,32 with minimum two trained primary family caregivers at home.1,11 This support network must be willing and able to provide care and have realistic expectations as they become “care coordinators” for all aspects of care.1,2,4,32 This is especially true in geographical areas where access is limited.7,23
Caring at home is a financial hardship. Family caregivers often leave careers, resulting in loss of income.1,18 There are several expenses including healthcare visits, equipment, supplies, medications, transportation, mobility devices, home and car modifications, all exacerbated with acute illness.1,18,20,21 In addition, the impact of a “downward trajectory in economic status” 31 should not be underestimated. Since a large proportion of healthcare costs are attributed to family caregiving,20,21 financial and personal support should be sought out, for example, home healthcare professionals, respite, not-for-profit or charities, and third-party or public funds.1,2,4,7,33 One of the greatest challenges is finding and retaining qualified providers, especially overnight or off-hours for personal support and/or nursing.22,30,34
Social, psychological and emotional support is key from the start of the transition process, and over the VAI’s lifetime. 23 Caregivers are sleep deprived, feel isolated, fatigued, can have high levels of depressive and anxiety symptoms and poor quality of life – all which impact their relationships with the person they are caring for and other family and friends.18,24,35–37 Although this transition is stressful for the VAI and the family, they often state it is worth the effort to do so, 23 especially when there is a high level of trust during all aspects of the process. 38 It is also important to consider the family caregivers as parents/spouses/relatives/friends first, and caregivers second. 24
Education and training
A structured, multi-modal and consistently delivered education and training program for both the VAI and their support network is crucial.1,2,4,7,18,30,39 Incorporating verbal, written, demonstrated, participatory, audio and video, along with advanced modes such as high fidelity simulation can help enhance learning.18,40 Ongoing training is necessary when new technology or interventions are developed and when the support team changes or includes new providers.1,2 Training new providers in the home is a challenge because providers often have little experience with the population, or there is frequent turnaround due to human resource issues.7,16,30
Items commonly found in a training program include foundational knowledge on respiratory anatomy and ventilation, airway care, use and troubleshooting equipment and devices, feeding, medication administration, infection control, skin care, 26 and mucous clearance.1,2,10–13,18,41 It is essential to have an emergency plan to recognize and act if there are changes in the VAI’s physical condition (e.g., disease progression, accidental decannulation, and acute illness), including who to contact (e.g., healthcare team versus Emergency Medical Services (EMS)). 18 Caregivers should also be certified in Basic Life Support. 1
The duration of the training depends on the readiness, availability, and abilities of the VAI and their support network.1,18 This is at least 6–8 weeks for invasive, and usually shorter for non-invasive LTMV. 1 Having a trial where the VAI’s support network assumes care while they are in the hospital is common, with a final reassessment just prior to discharge.1,18 Some jurisdictions have access to a step-down unit or long-term rehabilitation hospitals, allowing more time to prepare before going home.18,24,42 Given the complexity of LTMV, taking into account cultural and language differences, self-efficacy and confidence, mental health, and learning styles and pace helps facilitate the “stickiness” of knowledge and skills.7,18,30,31,37,43
Equipment and environment considerations
The optimal home ventilator model and parameters will depend on type of ventilation (invasive or non-invasive), availability, and funding.1,2 Access to ventilators (and related equipment) can come from community-based agencies or companies that supply and/or fund the device.2,20,21 Trialing the ventilator early is important physiologically, but also to ensure individual comfort and adherence. 1 This includes testing interfaces (e.g., masks, speaking valves), and allowing time for titration and bedside assessments. 1
Other adjunct equipment is often necessary including oximetry, suctioning, and non-respiratory items such as enterostomy feed and catheterization supplies, and mobility devices. 1 Providing checklists for the types and maintenance of various equipment and supplies will help facilitate the transition and ongoing care in the home. 30
The community setting (home or assisted living) may require physical space modifications to accommodate the VAI and equipment.1,2,4 This includes adequate electricity, water, telephone access to the EMS, heating and cooling, smoke and carbon dioxide detectors, and fire extinguishers.1,18 Ideally the VAI should have a designated space/room and adequate storage that is easy to access. 1 An emergency plan in case of fire and/or power outage should be established, including informing local EMS and utility companies.1,2,11 In addition, having a plan to address issues related to the technology should be in place both day and night.1,2,11
Overall discharge and transition plan
A structured protocol and/or detailed discharge plan is necessary to consider the numerous factors related to the transition.1,4,12,13,24,30,32,41,43–47 Although a common and overarching process should be established, it is important that each transition plan be individualized and consider the family unit, and their social status within the greater community.7,17,31,43 It should be developed with the VAI, their support network, and multi-disciplinary teams from both the institutional and community side.4,30 Plans consider all the issues described above and incorporate ongoing clinical and educational follow-up, for example, tracheostomy changes, 26 ventilation reassessment. 1 A “road map” should be provided that includes timelines and responsibilities that may occur over the VAI’s lifetime. 18 Providing mechanisms for peer-support is also a facilitator for ongoing support both in-person and remotely.16,30,48
Ideally all of the key processes for transition from hospital to home would be integrated within a publicly or government funded LTMV program or framework.2,19 However, community-based LTMV programs vary widely, from well-supported to piecemeal or non-existent.3,25,33,36,43,46,49 Variations usually are due to differences in jurisdiction and legislation, occurring at the national, state/provincial level, and/or regional/municipal level.31,33
Pediatric considerations
Children transitioning home often require equipment that is catered to their size, including interfaces such as masks and tracheostomy tubes. 13 There should also be consideration for long-term developmental issues such as schooling and relationship with siblings.1,23,32 Children with a tracheostomy are especially advised to have “24/7” care by a trained, awake and alert caregiver 1 because a main cause of death is tracheostomy-related events.1,50
Transition from pediatric to adult care
Given the advances in clinical care and technological support, an increasing number of children using LTMV are now surviving into adulthood. Transition is a purposeful, planned movement of adolescents with chronic medical conditions from child-centered to adult-oriented healthcare. 51 Many of the experiences early in the transition process can have lasting negative effects highlighting the paramount importance of a cohesive, collaborative transition process between the VAI, their parental caregivers, the pediatric and adult healthcare providers as well as the community supports.
Definition of the pediatric to adult healthcare transition
There is a growing recognition of the requirements from pediatric and adult healthcare providers as well as VAIs and families to ensure a successful transition. In 2002, a joint consensus statement from the American Academy of Pediatrics (AAP), the American Academy of Family Physicians (AAFP), and the American College of Physicians-American Society of Internal Medicine (ACPASIM) stated the importance of supporting and facilitating the transition of adolescents with special healthcare needs into the adult healthcare setting. 52 Furthermore, in 2011 the AAP published a clinical report outlining the six sequential core elements 53 : 1) discussion of transition policy; 2) transition tracking and monitoring; 3) transition readiness and/or orientation to adult practice; 4) transition planning; 5) transfer of care; and 6) transition completion and ongoing care with the adult healthcare team. In addition, the 2011 adult 2 and 2017 pediatric 1 Canadian Thoracic Society guideline recommendations for LTMV transition included early planning with disease-specific education and VAI preparation, identification of a family physician, joint pediatric‐adult transition clinic visits, and awareness of the changes in pediatric to adult funding of homecare support services. A priori preparation of adolescents and their families for the change in healthcare delivery in the adult care setting is paramount to a successful transition. 53
Pediatric to adult healthcare transition for VAIs: Current state
Over the past few decades, disease-specific transition programs have evolved for many conditions.28,54,55 However, despite their medical complexity and intense care needs, there is not a standardized process for adolescent VAIs. A survey was conducted across pediatric pulmonary programs in the United States to explore the presence of a formalized process for the pediatric to adult transition of adolescent VAIs. 56 Most respondents, 78% (25/32) reported not having a standard protocol for transition and 41% (12/29) had no formal process in place; the readiness to transition was evaluated by only 14% of survey participants. 56 Coordinating the transition with other specialists was provided by only 31% of programs. 56
Consequences of a suboptimal pediatric to adult healthcare service transition
The literature is lacking for pediatric to adult healthcare service transition for VAIs. However, several studies in other clinical populations have reported the negative consequences of a suboptimal transition. An abrupt or incomplete transition of care from pediatric healthcare services to a network of adult health providers has been associated with disengagement from healthcare, deteriorating health status and increased rates of hospitalization.57–60 Adolescents lost to medical follow-up are more likely to utilize acute care healthcare services and experience increasing disability.61,62 Healthcare service interruption would be particularly detrimental for VAIs who are characterized by complex comorbidity requiring multispecialty care with intense use of acute healthcare services. 63
Transition facilitators and barriers to the transition from pediatric to adult healthcare services for LTMV
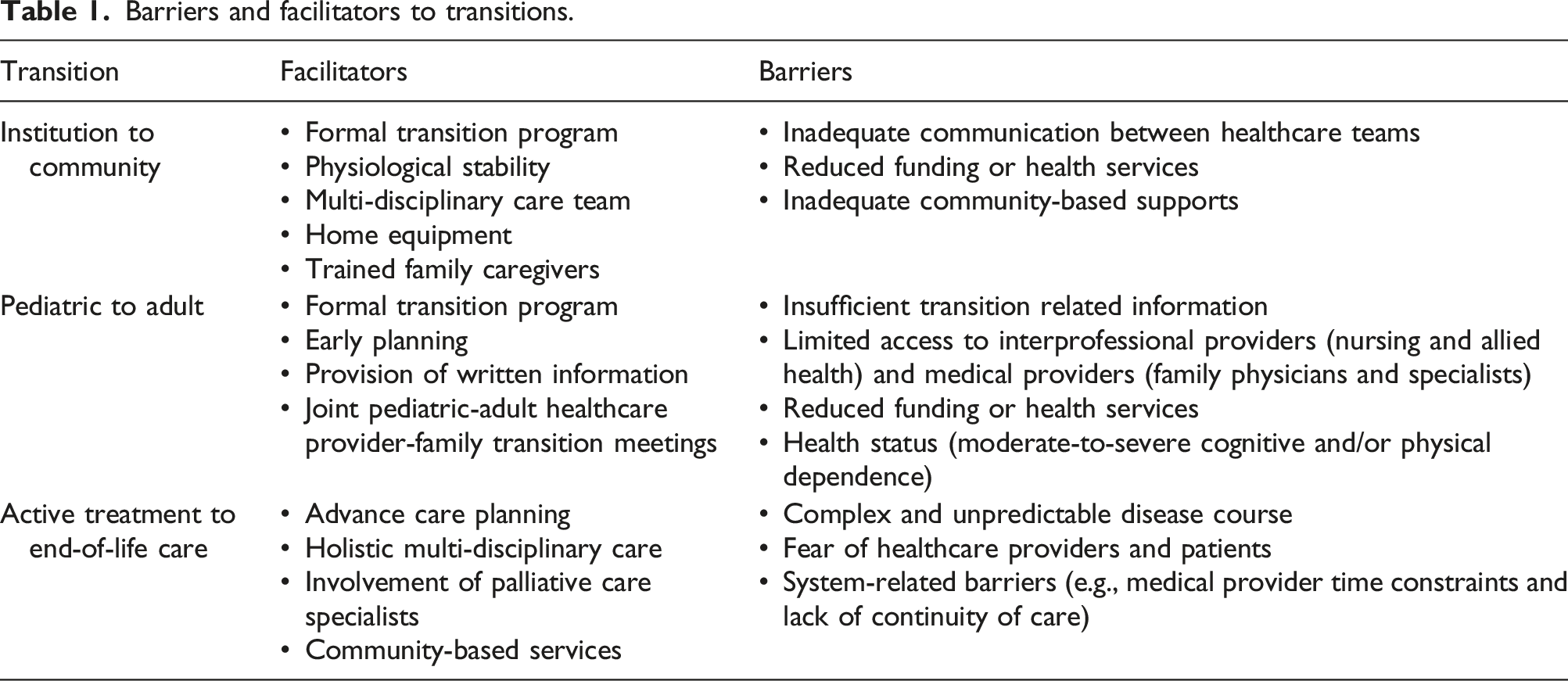
There have been only two studies which have formally explored the barriers and facilitators of pediatric to adult healthcare service transition for VAIs; both are qualitative studies conducted in Canada.6,64 Dale et al. 6 conducted 18 semi-structured telephone interviews (14 transitions) with adolescents and family caregivers who had recently initiated or completed transition to adult healthcare services from three academic institutions. Most of the adolescents were using non-invasive ventilation during 11 of the 14 (79%) transitions. Facilitators for transition included early planning, provision of written information and joint pediatric-adult healthcare provider-family transition meetings. 6 The barriers included insufficient transition related information, limited access to interprofessional (nursing and allied health) providers and reduced funding or health services. 6 Challenges encountered by VAIs and families during the transition process resulted in service fragmentation, a sense of "medical homelessness" as well as intensification of the caregiver role. 6 Notably, families caring for VAIs with moderate-to-severe cognitive and/or physical dependence reported transition difficulties more commonly. 6
Dale et al. 64 subsequently conducted a prospective, longitudinal qualitative study of adolescent VAIs and their family caregivers as they transitioned through a newly established pediatric to adult healthcare service transition program. This transition program consisted of: formal transition discussions with the adolescent and family caregivers in the last year of pediatric care; conversations to support the autonomy of the adolescent regarding communication with healthcare providers; collaborative evaluation of transition readiness by the VAI, family and medical team, and; a formal handover from the pediatric to adult LTMV teams via a detailed written summary and accompaniment by a member of the interprofessional pediatric LTMV team to the first clinic visit at the adult hospital. 64 Serial, semi-structured interviews with 12 dyads of VAIs and their caregivers were conducted at three time points: pre-transition, transition and 12-months post-transition. The study participants all perceived a lack of transition readiness in their ability to manage health communication and coordination across multiple adult care providers despite their involvement in the formalized pediatric to adult transition program. 64 Notable barriers to transition included a lack of other specialist referrals, insufficient a priori information about adult homecare service funding and limited involvement of family physicians. 64
Transition from active treatment to end-of-life care
Although LTMV is associated with increased survival and improved quality of life,65–67 LTMV is unable to modulate the incurable and progressive disease process necessitating ventilatory support. While the trajectory invariably includes a terminal phase and death, prognostication is often imprecise68,69 and variability is exacerbated by unpredictable events that may mediate death. The term EOL is used to refer to a unique period of irreversible decline before death with a prognosis of “months” or less. 70 The following discussion will describe the role of ventilation for VAIs at the EOL. Unlike the previous two transitions discussed, this transition focuses on a theoretical shift in management as opposed to a concrete transfer of care.
Advance care planning
A deep understanding about an individual and their family caregiver’s wishes, preferences, and needs is essential for a successful transition to EOL care. Advance care planning (ACP) “enables individuals to define goals and preferences for future medical treatment and care, to discuss these goals and preferences with family and healthcare providers, and to record and review these preferences if appropriate.” 71 ACP should begin early in an individual’s disease trajectory and continue across their life span when there is clinical evolution so that decisions can be made outside of a crisis situation. 72
There are several considerations for ACP specific to VAIs. Open discussions should begin early when individuals are considering the initiation of LTMV. 73 Early ACP may be particularly important for VAIs because of the risk for unexpected deteriorations. 8 ACP should be reviewed when transitions in ventilatory care are considered, such as changing from non-invasive to invasive ventilation or nocturnal to diurnal ventilation. Further, caregivers and VAIs with a progressive irreversible disease should understand at the time of ventilation initiation that withdrawal of therapy in the future is their decision.
Despite interest in ACP by both VAIs and healthcare providers, many VAIs report that they have not engaged in these discussions with medical professionals.74,75 The implementation of ACP may be complicated by 1) a complex and unpredictable disease course, 2) healthcare providers fearing they are taking away individuals’ hope, and 3) system-related barriers including time constraints and lack of continuity of care. 75 Further research on implementing ACP in pediatric and adult healthcare is required.
Ventilation at the end-of-life
There is significant variability in the care for VAIs at the EOL. 76 Some VAIs may choose to continue nocturnal ventilation because of symptomatic benefits, 77 while others wish to discontinue it if the benefits have been lost or do not outweigh therapy. Less commonly, VAIs may request compassionate withdrawal of mechanical ventilation. 78 In all situations, holistic care at the EOL requires a multi-disciplinary care approach including primary and specialist physicians, hospice/palliative care specialists, social work, spiritual care, and family members.
Continued use of mechanical ventilation at the end-of-life
Many VAIs may continue LTMV at the EOL to aid with comfort and anxiety. 79 For some VAIs and their caregivers, the treatment focus for LTMV may be life prolongation. In other cases, the treatment focus may transition to symptom or comfort-oriented care as LTMV may be used to relieve dyspnea, a significant symptom for VAIs at the EOL. 80
The goals of ventilatory support should be reviewed as the underlying disease progresses. 13 If the treatment goal is life prolongation, optimized ventilatory support and regular surveillance should be instituted. If the therapeutic goal changes to comfort-oriented care, treatment monitoring may focus on symptom relief. Treatment goals may fall anywhere along this continuum and management plans should be tailored to individual needs.
Compassionate withdrawal of mechanical ventilation
VAIs who are dependent on mechanical ventilation may request compassionate withdrawal at the EOL. 81 Although this an uncommon event, 80 there is evidence that many VAIs with amyotrophic lateral sclerosis (ALS) wish to stop LTMV at the EOL. 82 In a separate study of individuals with ALS in their final month of life, caregivers reported that half of all individuals on mechanical ventilation had it discontinued before death. 83 Individuals whose goal of care was comfort were more likely to discontinue ventilatory support. 83
The process of compassionate withdrawal must be carefully planned in conjunction with the VAI and their family caregivers to ensure that it is aligned with their wishes. The withdrawal may occur as a continuous reduction of mechanical ventilation or as a definitive cessation.13,70 Although compassionate withdrawal of mechanical ventilation for a ventilator dependent individual will inevitably lead to death, the timing is variable. 78 Therefore, it is vital that anticipatory treatment is implemented to reduce the dyspnea and respiratory distress that will occur shortly after discontinuation of ventilation.84–87 The Association for Palliative Medicine of Great Britain and Ireland released Guidance on the withdrawal of ventilation in individuals with ALS further outlining recommended symptom management. 84
Preferred place of death
The place of death for VAIs at the EOL is variable. A retrospective study found that 78/168 (46.4%) VAIs died at home, 70/168 (41.7%) in a medical ward, and 20/168 (11.9%) in an intensive care unit. 80 However, the preferred place of death may not always match the actual place of death. 79 A retrospective study on individuals with ALS found that although the majority preferred death at home or in hospice, a significant proportion died in hospital. 88
The wishes of the VAI and family caregivers for the preferred place of death should be elucidated early during the ACP process so that local resources can be mobilized to support this. The provision of chronic non-invasive ventilation as a palliative therapy in a hospice program is possible and should be facilitated when resources allow. 89 Further, mechanical ventilation may be used to stabilize an individual during the transition to home or hospice to allow for death in the preferred place of death.90–95
Discussion
Barriers and facilitators to transitions.
Current gaps in knowledge and potential research priorities.

Formal transition programs provide a standardized framework to optimize healthcare delivery and outcomes during transition processes. However, VAIs and families report significant barriers to care even when transitioning through a formal program. There is an urgent need for the development, implementation, and outcomes-based evaluation of transition models of care. VAI/family readiness for transition, a holistic coordinated process with other specialties, augmenting family physician involvement as well as awareness and advocacy for ongoing allied health and homecare supports in the adult healthcare system are identified priorities for the LTMV population.
The COVID-19 pandemic necessitated remote communications and saw the rise in the development and use of telemedicine to facilitate various transitions for VAIs.96–99 Although telecommunication technology existed prior to the pandemic,100,101 its complementary role to current care models provides an opportunity for permanent integration to support transition frameworks. Remote telemonitoring may be a cost-effective tool to reduce unplanned healthcare utilization,102,103 improve survival, 104 and increase patient satisfaction. 105 Its formal integration into transition models of care could help to facilitate smooth transition processes. In pediatric studies, telemedicine systems have been associated with higher ratings for care coordination 106 and family-centered care. 107 Further, telemonitoring may preclude the necessity of the transition from institution/hospital to community/home by facilitating the initiation of non-invasive ventilation directly in the home environment.101,108 Describing how telemedicine will fit within the overall transition care model will be of interest in future investigations.
Most LTMV programs described in this review exist in developed countries with funded healthcare systems and accessible community-based supports. The availability of community resources and robust healthcare systems are essential to supporting VAIs and their family caregivers during stressful periods of transitions. Supporting these vulnerable populations in lower resource settings represents an important research agenda.
Conclusions
Transitions from pediatric to adult care, hospital to home, and to EOL for VAIs are complex and challenging processes. Development of holistic and systematic processes that incorporate innovative technology, and how they can be integrated within the context of any healthcare environment, should be investigated in the future.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.