
Abstract
Several retrospectivee described the association of interstitial lung disease (ILD) and ANCA-associated vasculitis (AAV). However, the relationship between the ILD and mortality in AAV patients have not been established so far. This study aims to estimate the relevance of AAV-associated-ILD (AAV-ILD) and mortality risk by conducting a systematic review and meta-analysis.A comprehensive systematic review was conducted in accordance with the guidelines of PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-analyses). PubMed, Embase.com and the Cochrane Library (Wiley) were searched for original observational studies. Summary estimates were derived with a random-effects model and reported as risk ratio (RR), tested for publication bias and heterogeneity. Ten retrospective cohort studies were included, comprising 526 AAV-ILD patients enrolled from 1974 to 2018. Meta-analysis yielded a pooled RR of 2.90 (95% confidence interval 1.77–4.74) for death among those with AAV-ILD compared to control group. UIP pattern was associated with an even poorer prognosis in comparison to non-UIP pattern (RR 4.36, 95% confidence interval 1.14–16.78). Sensitivity analysis suggested that the meta-RR result was not skewed by a single dominant study. ILD might be associated with a higher mortality risk in AAV patients.
Background
Antineutrophil cytoplasmic antibodies (ANCA) vasculitis are immune-mediated disease that is primarily characterized by ANCA positivity and affects various organs, such as the lungs, kidneys, skin, and nervous system. Based on clinical phenotypes and pathologies, cases of AAV are divided into three diseases: microscopic polyangiitis (MPA), granulomatosis with polyangiitis (GPA, formerly called Wegener’s granulomatosis) and eosinophilic granulomatosis with polyangiitis (EGPA, formerly called Churg–Strauss syndrome). 1,2
Interstitial lung disease (ILD) is a rare condition, whose prevalence and incidence rates were reported to be 97.9/100,000 and 19.4/100,000, respectively, in a recent French study. 3 During the last few years, an increasing number of publications have reported the association between ILD and AAV. 4 –16 Prevalence of ILD is higher in MPA than in GPA, in fact, ILD has been reported in about 23% of GPA patients and up to 45% of MPA patients. 4 –7,9,10,12,14 ILD occurs concurrently or antedates MPA in the majority of affected individuals. 4,5,7,17 –24 Among AAV patients with ILD, the most frequent CT scan pattern is usual interstitial pneumonia (UIP) in 43 to 83%. 11,25,26 UIP is characterized by reticular changes and honeycombing in the subpleural sections of the lower lobes on high-resolution computed tomography (HRCT). 27 However, these patients had various minor HRCT findings that were not typical UIP patterns, such as ground-glass opacity(GGO), bronchial wall thickening, consolidation, and increased attenuation around honeycombing, 4,11,26 and these findings can help one to consider radiologic diagnosis of AAV-associated-UIP. Other ILD patterns have also been described. In the study by Maillet et al., non-specific interstitial pneumonia (NSIP) was reported in about 39% of AAV patients with ILD. A few cases were reported that organizing pneumonia (OP) was clinically diagnosed in patients with active AAV. 28 –30 Combined pulmonary fibrosis with emphysema (CPFE) has also been reported in a few series of MPA. 11,26
Previous studies suggested that ILD seems to be a major prognostic factor in AAV patients. 8 –11, 13 –16,25,31 –33 To further investigation, we performed a systematic literature review and meta-analysis to estimate the impact of ILD had on mortality.
Methods
A comprehensive systematic review was conducted in accordance with the guidelines of PRISMA (Preferred Reporting Items for Systematic Reviews And Meta-analyses). 34 The review protocol was registered on 26 March 2020 in the International Prospective Register of Systematic Reviews database.
Search strategies
The databases PubMed (N.L.M.), Embase.com and the Cochrane Library (Wiley) were searched by two authors (PZ and JM) from their inception to March 2020. In brief, three search concepts were combined with the Boolean operator “AND”: (1) ANCA-associated vasculitis (AAV) or vasculitis, (2) interstitial lung disease (ILD) or pulmonary fibrosis (PF) and (3) mortality or survival rate. Search terms included indexed terms from Medical Subject Headings (MeSH) in PubMed, EMtree in EMBASE.com as well as free-text terms. The search strategy is available in Supplemental data 1. All identified studies were combined in a single reference manager file (EndNote). Abstracts for all articles of interest were reviewed for relevance, which is those that focused on the association between ILD and AAV and mortality or survival data in AAV-ILD patients. Full papers of selected abstracts were retrieved and assessed for eligibility based on the inclusion criteria.
Observational studies that met the following criteria were assessed: (1) clearly defined AAV identified by either the American College of Rheumatology 1990 classification criteria or the 2012 Chapel Hill Consensus Conference disease definitions, and (2) provided ILD-related risk ratios or hazard ratios, or can be calculated from the studies.
Criteria were used for the diagnosis of ILD mostly depending on radiological evidence on chest X-ray and HRCT (such as reticular abnormality or honeycombing with or without traction bronchiectasis), which can be combined with other examination results(such as lung function testing and/or histopathology).The control group was considered to diagnose AAV without ILD but were likely to have other common clinical manifestations, such as sinus pain, nasal discharge, or crusting, ear pain, or deafness, foot drop or wrist drop, hematuria and oliguria. Articles analyzing connective tissue disease-associated ILD (CTD-ILD) or collagen vascular disease-associated ILD (CVD-ILD), and not specifically AAV-ILD, were excluded.
We also searched the reference lists of identified papers and conference abstracts for additional relevant publications. In cases of duplicate data used in more than one study, the sample with the most up-to-date data was selected for review. No additional exclusions were made on the basis of study design, quality of the study, or duration of follow-up. The study identification and selection process are summarized in Figure 1.
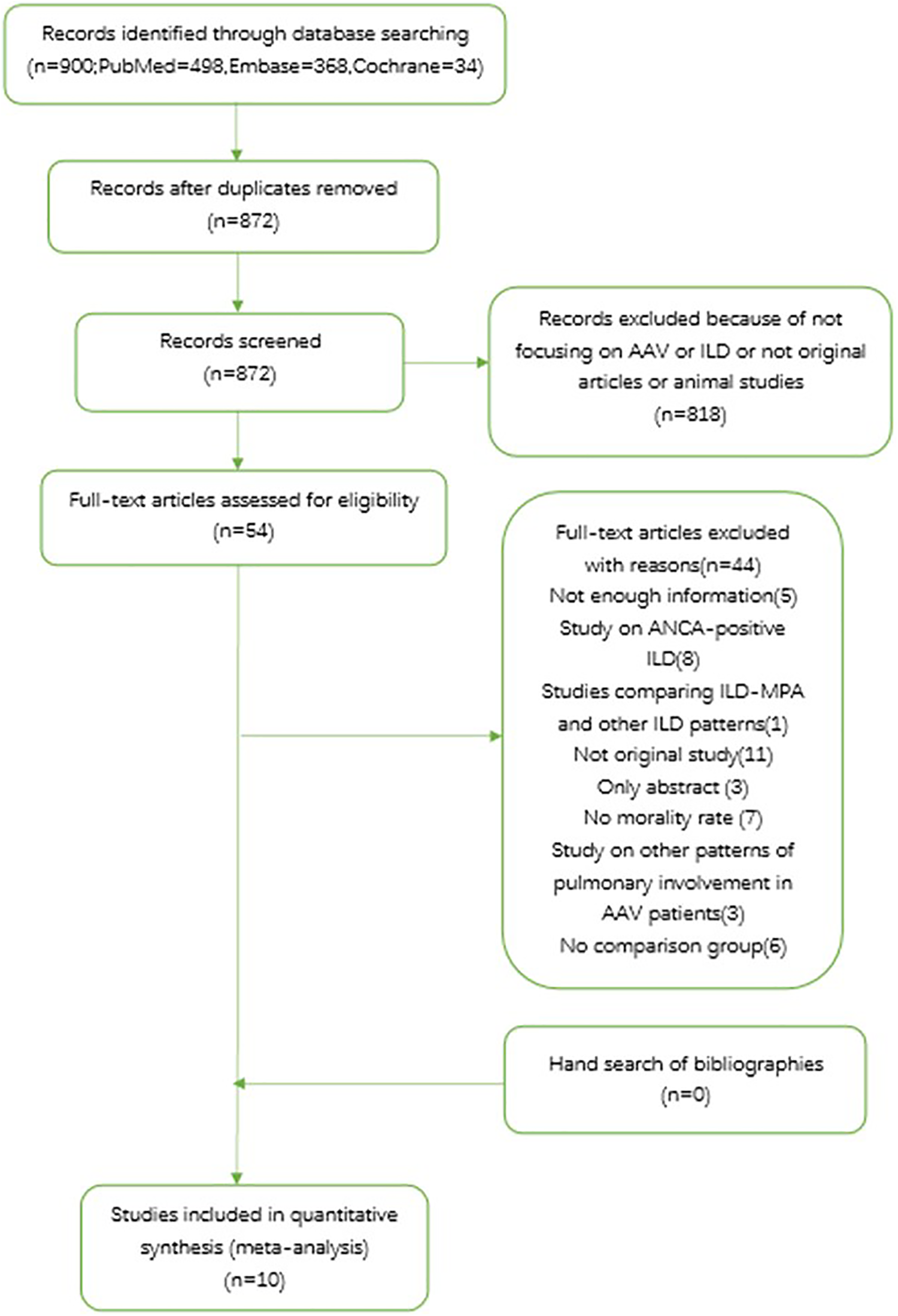
PRISMA flow chart of study selection from literature search.AAV: ANCA-associated vasculitis; ANCA: antineutrophil cytoplasmic antibodies; ILD: interstitial lung disease; MPA: microscopic polyangiitis.
Data extraction
Data were collected through a standardized extraction sheet. One reviewer (PZ) extracted and the second reviewer (JM) checked the data. Disagreements were discussed and resolved. From eligible studies, the following data were collected: year of publication, enrollment period, study design, country, sample size and demographics, mean follow-up duration, number of AAV-ILD patients, survival or mortality data.
Quality assessment
Study quality was assessed using the Newcastle-Ottawa scale (NOS). 35 In this scale, studies are scored across three categories: selection of study groups (four questions), comparability of study groups (one question) and ascertainment of the outcome of interest (three questions) for cohort studies. Two authors (PZ and JM) performed quality scoring independently, with differences resolved by consensus.
Statistical analyses
In this meta-analyses, the outcomes of interest were pooled RR for AAV-ILD, HR were assumed to be numerically the same as the RR. Forest plots and pooled estimates were derived with inverse variance weighting and a random-effects model. The heterogeneity among studies was tested with Cochran’s Q test. Significant heterogeneity was defined as a value of P < 0.10. The I2-statistic was used to quantify the heterogeneity. 36 Source of heterogeneity was determined by subgroup analysis. All included studies were classified according to enrollment period (2010 to 2015 vs 2016 to 2020), center (single center vs multicenter), ethnicity (Asian patients vs non-Asian patients), analysis method (adjusting by covariates vs without covariate), follow-up period (no more than 48 months vs more than 48 months), the use of immunosuppressants for induction therapy, and the pattern of interstitial lung disease (usual interstitial pneumonia was classified as a specific pattern). Furthermore, a univariate meta-regression analysis was then used to interpret the difference in RRs between the subgroups. 37 We evaluated the robustness of the results using jackknife sensitivity analysis, by repeated meta-RR analyses with removal of a single study in succession each time. 38 A funnel plot was conducted to detect publication bias (i.e. bias resulting from the greater likelihood of studies with positive results to be published compared with negative results) or the small-study effect (i.e. a tendency for treatment effect estimates in small studies to differ from those in larger studies). 39 Furthermore, we used Egger’s regression as an objective, quantitative test statistic to test for the presence of asymmetry in the data. 40 Data analysis was performed with Review manager (RevMan) version 5.3 and Stata statistical software V.StataSE14 (stataCorp LLC, College Station, Texas, USA).
Results
A total of 900 records were processed for a final selection of 10 articles. Most records were irrelevant, and of the 54 records were reviewed based on full text. The most frequent reasons for exclusion upon full text review were studies focusing on ANCA-positive ILD or lack of mortality data. Finally, 44 records were removed according to inclusion criteria and the remaining 10 studies were included in the meta-analysis. A list of the excluded articles was provided in Supplemental data 2.
Study characteristics
Characteristic features of the studies included in this meta-analysis are summarized in Table 1. The studies were published between 2010 and 2019, enrolled from 1974 to 2018; All of these were retrospective cohort studies, four of which were from multicenter. Locations included six Asian studies, of which four from Japan, one from China and one from Korea, and the remaining studies came from Greece, London, Germany, Argentina respectively. The sample sizes in the individual studies ranged from 9 to 301 AAV-ILD patients and 526 in total. One study used three other control groups, including alveolar hemorrhage, bronchial asthma and pulmonary granuloma. The other study used bronchiectasis as an additional control group. Five studies adjusted mortality for Birmingham Vasculitis Activity Score (BVAS), age, cardiovascular involvement, alveolar hemorrhage, serum creatinine level etc. The included studies were of high quality, scoring 7 to 9 points according to the Newcastle-Ottawa Scale.
Characteristics of the 10 included studies.

a: Research center was classified as single center and multicenter.
b: Cohort type was classified as inception cohort and non-inception cohort.
c: Study quality was assessed using the Newcastle-Ottawa scale (NOS).
AAV: ANCA-associated vasculitis; I: inception cohort, ILD: interstitial lung disease; M: multicenter; MPA: microscopic polyangiitis; N/A: not available; N-I: non-inception cohort, S: single center, UIP: usual interstitial pneumonia.
Causes of death
Table 2 details the causes of death in the included studies if were available. The majority of the deaths were respiratory failure and infectious pneumonia.
Causes of death.
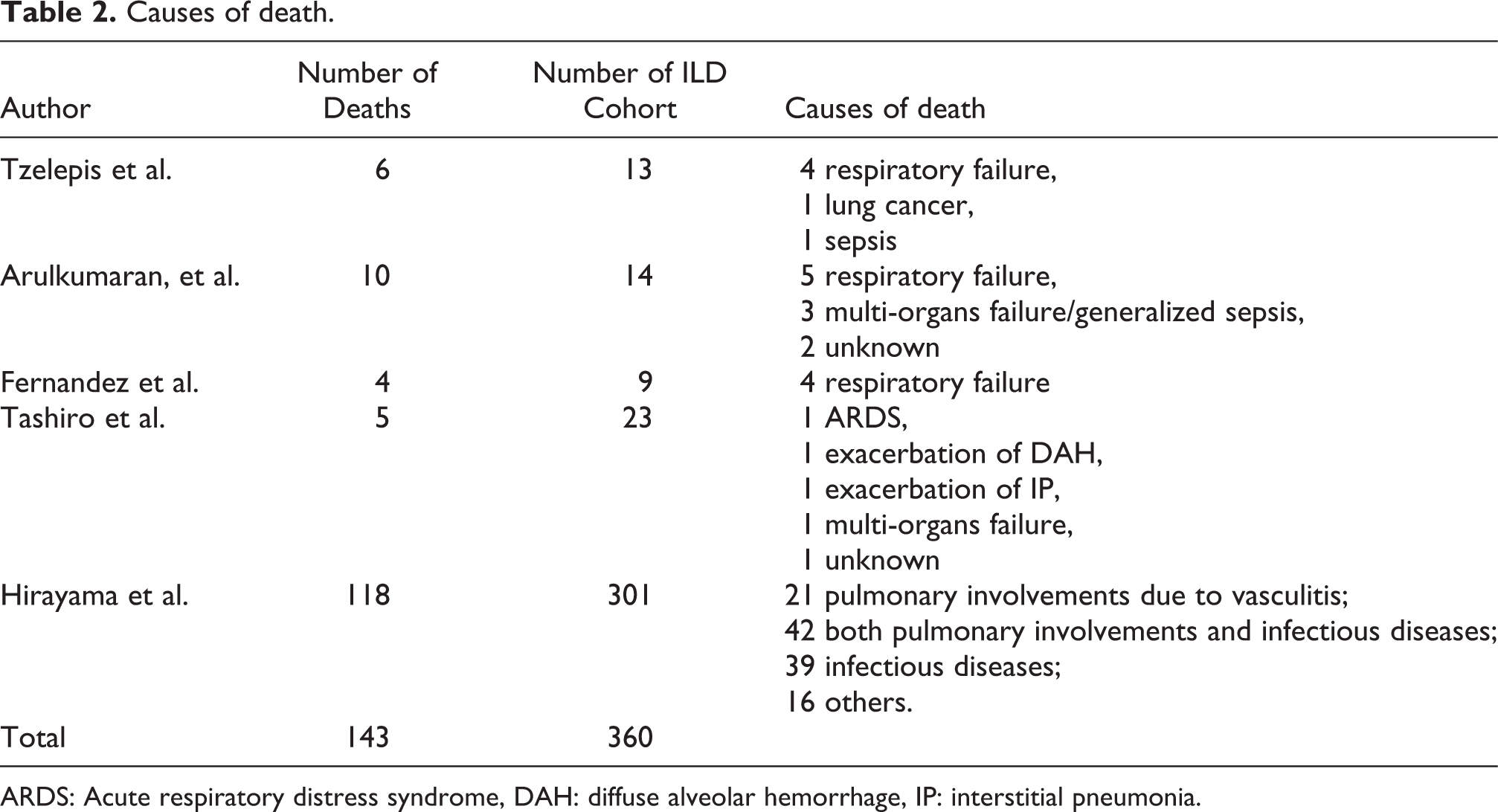
ARDS: Acute respiratory distress syndrome, DAH: diffuse alveolar hemorrhage, IP: interstitial pneumonia.
Impact of ILD on mortality in AAV
We pooled the results of all 10 studies comparing mortality risk between AAV-ILD and control groups and observed an increase in mortality among ILD, [risk ratio (RR) = 2.90; 95% confidence interval (CI) 1.77–4.74]. There was a significant heterogeneity among the studies, I2 = 72% (p < 0.0001) (Figure 2).

Meta-analysis of 10 studies on the risk ratio for all-cause mortality in ANCA-associated vasculitis patients with interstitial lung disease.
Sensitivity analysis
The results of jackknife sensitivity analysis are shown in Table 3. The RRs remained significantly increased regardless of each study exclusion sequentially, with the value estimated ranging from 2.55 to 3.60 in all analyses. This suggested that the meta-RR result was robust and not skewed by a single dominant study.
Sensitivity analysis for the included studies.

RR: risk ratio.
Subgroup analyses
Subgroup analyses showed that meta-RRs were higher in non-Asian group, multicenter group, adjusted covariates group, less follow-up period group, UIP group and in cohorts enrolled after 2015. No statistical difference of RR was found in “immunosuppressive treatment” subgroup. Only “follow-up period” was significantly associated with the observed heterogeneity using meta–regression analysis (Supplementary Figures 1–7, Table 4).
Assessment of publication bias
The funnel plot is shown in Figure 3. Visual inspection of the funnel plot was asymmetrically located. Using the Egger’s test for publication bias with the 10 studies, the p value less than 0.10 indicating that there is an evidence for publication bias. We further evaluated the number of missing studies in this meta-analysis by the application of the trim and fill method and recalculated the pooled risk estimate with the addition of those missing study. There was no significant change in the value of summary statistic, suggesting that publication bias had no significant impact on the result.

Funnel plot of 10 cohort evaluating publication bias of mortality studies in AAV-associated-ILD. AAV: ANCA-associated vasculitis; ILD: interstitial lung disease.
Discussion
This is the first meta-analysis of observational studies assessing the mortality risk in AAV-ILD. We found a 2.9-fold increased risk of death in patients with AAV-ILD when compared with control group. The RR remained significantly increased by sensitivity analysis, suggesting that the meta-RR result was robust and not skewed by a single dominant study. Given the heterogeneity observed in the pooled risk estimate, subgroup analyses were conducted. Subgroup analyses showed that a number of factors might have influenced the mortality risk. Meta-RRs were higher in non-Asian cohorts, in multicenter studies, in patients with UIP pattern, in studies with shorter follow-up duration (no more than 48 months), in cohorts adjusted by covariates and in cohorts enrolled later than 2015 (Table 4, Supplementary Figures 1–6). Theses subgroups showed significantly increased mortality risk compared to the general population. There was no beneficial effect in immunosuppressive treatment subgroup (Supplementary Figure 7). Despite the differences in mortality within subgroups, only “follow-up period” was significantly associated with the observed heterogeneity using meta–regression analysis (p = 0.04).
Subgroup analyses and meta–regression analyses.

a: P(a), p value of each subgroup.
b: P(b), p value between two subgroups.
N/A: not available; RR: risk ratio.
The association between ILD and AAV was confirmed in our study, revealing that 26% of AAV patients showed ILD. The prevalence of ILD in MPA patients was well-established. ILD was found in 7–54% of MPA patients. Meanwhile, ILD was found in 15% of patients with GPA, and in 17% of those with PR3-ANCA positive. 8,13 All of these cohorts were from Japan, which might be partly explained by our findings about geographic differences. ILD has been reported more frequently in Asian cohorts with AAV compared to Western patients. 5,9,12,14 A higher prevalence of MPO-ANCA antibodies in Asian patients have been proposed as possible explanation for these differences. Several hypotheses might support that correlation between ILD and MPO-ANCA positive AAV. The first, which fits better with ILD usually occurring before AAV, is that ILD could induce MPO-ANCA production. 15,41 The second hypothesis is based on animal models showing that MPO-ANCA have pro-fibrotic activity leading to progressive fibrosing ILD. 42 Thirdly, an increased frequency of alveolar hemorrhage and a higher prevalence of MPO-ANCA antibodies in Asian patients have been proposed as possible explanation for these differences as well. 43,44
Current studies suggest that ILD, especially UIP, mainly affects the long-term survival. Our study confirmed that the RR-value is higher in UIP subgroup than ILD group (RR 4.36 vs RR 2.90). The lack of effectiveness of immunosuppressants among these patients seems to be a major reason. At the same time, a higher risk of infection deteriorates the outcome of UIP patients. UIP was found only in patients with MPA, which was consistent with the previous studies suggesting a poor prognosis in MPA than GPA. 4,5,7,11 Survival of other types of ILD have also been reported in some small-scale studies and case reports. A study on 38 AAV-UIP and 24 AAV-NSIP patients suggested that systemic AAV manifestations are significantly more common in AAV-NSIP, and there was no evidence to support the association between NSIP and long-term survival. 11,25 A spontaneous improvement case of OP associated MPO-ANCA has been reported, another case also revealed that the deterioration of the general condition improved rapidly via steroid and immunosuppressive treatment. 28,29 These data suggest that the prognoses of non-UIP patients are relatively better, which may attribute to their better response to glucocorticoids and immunosuppressants. Therefore, differences of ILD patterns according to AAV subtypes may explain their distinctions in outcome: MPA is associated with poorer prognosis, and GPA is more effective to immunosuppressive therapy while more prone to relapse. To our knowledge, there is no sufficient evidence to reveal the correlation between different patterns of ILD, future studies need to pay attention to the changes of CT images during follow-up.
Of interest, mortality risks were even higher in studies with shorter follow-up duration (no more than 48 months) and enrolled later than 2015, suggesting that ILD is not only associated with long-term survival, but also a risk factor for poorer prognosis within 48 months. One of the possible reasons for differences was controversial therapeutic approach. Standard therapy for AAV is considered also as a possible treatment in patients with ILD and includes mainly systemic glucocorticoids, cyclophosphamide, rituximab, mycophenolate mofetil, methotrexate and azathioprine. 45 However, a study on 62 AAV-ILD patients suggested no improvement for patients treated with immunosuppressants and also other reports confirmed the lack of effectiveness of immunosuppressants. 5,19,25 According to our meta-analysis, immunosuppressants for induction therapy had no beneficial effect on patient survival (RR 1.00, 95% CI 0.95–1.05), which was in line with previous studies. Given the limited data provided by the included studies, we cannot further assess the impact of immunosuppressive therapy during maintenance remission. Our study reported that infectious complication was one of the most frequent causes of death, 4,5,7,12 and maintenance therapy with corticosteroids and immunosuppressants increased the risk of infection. 8,13,31,46,47 Pulmonary fibrosis frequently existed before systemic involvement, which also aggravated the possibility of infection. Therefore, we postulated that immunosuppressants for maintenance therapy might associated with poor prognosis. However, none of the included studies in our meta-analysis focused on the clinical benefit of antibiotic prophylaxis for AAV-ILD patient. Further investigation is needed to better characterize patterns of ILD, predict progression, and determine optimal therapeutic regimens.
Moreover, in patients with an UIP pattern, the histologic and radiologic similarities with IPF, may suggest the use of antifibrotic therapies, namely pirfenidone and nintedanib. A recent double-blind, placebo-controlled, phase 3 trial, NCT0299917, has proved the efficacy of nintedanib not only in idiopathic pulmonary fibrosis but in a broad range of fibrosing lung diseases as well. 48 Meanwhile, clinical trials (NCT03385668 and NCT02999178) are ongoing with the aims to evaluate the safety and the effectiveness of antifibrotic drugs in patients with MPO-ANCA-positive pulmonary fibrosis with or without AAV.
It is also interesting to note an increased mortality in studies adjusted covariates (RR 3.59, 95% CI 1.60–8.05). One reason might explain that the impact of ILD was latently masked by other factors involved, thus relevant RR was underestimated. Several factors may confound mortality in AAV-ILD patients, mostly including age, alveolar hemorrhage, Birmingham vasculitis activity score (BVAS), and renal involvement. 7 –10,13,14 Firstly, repeated episodes of alveolar hemorrhage could be the pathogenesis of pulmonary fibrosis. 19 However, this may lead researchers to mistakenly attribute ILD-related death to alveolar hemorrhage. Secondly, renal involvement was significantly more common in MPA, affecting 93% compared to 66% of those with GPA. Compared to GPA, serum creatinine levels were significantly higher in those with MPA. 9 Numerous patients eventually died from dialysis-related complications, thereby ignoring the potential impact of ILD. Moreover, pulmonary fibrosis (PF) occurs concurrently or antedates MPA in the majority of affected individuals. 15 In those cases when pulmonary fibrosis was diagnosed before MPA, the time range from a few months to 12 years. Among the studies with short-term follow-up, the impact of ILD may be ignored for these patients had not met the diagnostic criteria of AAV yet. It is necessary for future studies to explore the role of ILD during AAV development by prolonging follow-up time.
The strengths of our meta-analysis include the thorough systematic literature review, duplicate abstraction, careful exclusion of studies on overlapping populations, evaluation of study quality using the Newcastle-Ottawa scale. Both sensitivity and subgroup analysis were applied to evaluate the stability and heterogenous of findings. Although there is an evidence for publication bias, no significant change in the recalculated value of the summary statistic by the application of the trim and fill method, suggesting that publication bias had no significant influence on the result.
Our meta-analysis has few limitations. First, the data were insufficient for subgroup meta-analysis of survival based on different patterns of ILD. Second, immunosuppressants for maintenance therapy may also influence the results on infection prevalence and survival. Third, the values we used to assess including risk ratios and hazard ratios (HR); however, we chose the covariate adjusted HR to reduce the heterogeneity of the result as far as possible. Furthermore, a meta-analysis pooled estimate with high heterogeneity provides results at high risk of bias. This study reported potential explanation of heterogeneity by subgroup analyses. Finally, selection bias may have existed in the design of original included studies.
Conclusion
In summary, our meta-analysis indicated that ILD is a complication of AAV that might associated with poor prognosis. The risk of death in AAV-ILD patients remains relatively high over time, which warrants further investigation to better characterize patterns of ILD, predict progression, and determine optimal therapeutic regimens.
Supplemental material
Supplemental Material, sj-pdf-1-crd-10.1177_1479973121994562 - Impact of interstitial lung disease on mortality in ANCA-associated vasculitis: A systematic literature review and meta-analysis
Supplemental Material, sj-pdf-1-crd-10.1177_1479973121994562 for Impact of interstitial lung disease on mortality in ANCA-associated vasculitis: A systematic literature review and meta-analysis by Peining Zhou, Jing Ma and Guangfa Wang in Chronic Respiratory Disease
Footnotes
Acknowledgements
We would like to thank Professor Xueying Li in the Department of Medical Statistics of Peking University First Hospital for her helpful instruction in data analysis and statistics to the research.
Author Contributions
GW planned the study. JM helped guide the study and assisted in data collection.
Availability of data and material
All data and materials in this manuscript are available.
Consent for publication
The manuscript has been read and approved for publication by all the authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
All analyses were based on previous published studies, thus no ethical approval and patient consent are required.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.