
Abstract
Objectives:
To identify exercise tests that are suitable for home-based or remote administration in people with chronic lung disease.
Methods:
Rapid review of studies that reported home-based or remote administration of an exercise test in people with chronic lung disease, and studies reporting their clinimetric (measurement) properties.
Results:
84 studies were included. Tests used at home were the 6-minute walk test (6MWT, two studies), sit-to-stand tests (STS, five studies), Timed Up and Go (TUG, 4 studies) and step tests (two studies). Exercise tests administered remotely were the 6MWT (two studies) and step test (one study). Compared to centre-based testing the 6MWT distance was similar when performed outdoors but shorter when performed at home (two studies). The STS, TUG and step tests were feasible, reliable (intra-class correlation coefficients >0.80), valid (concurrent and known groups validity) and moderately responsive to pulmonary rehabilitation (medium effect sizes). These tests elicited less desaturation than the 6MWT, and validated methods to prescribe exercise were not reported.
Discussion:
The STS, step and TUG tests can be performed at home, but do not accurately document desaturation with walking or allow exercise prescription. Patients at risk of desaturation should be prioritised for centre-based exercise testing when this is available.
Introduction
As a result of the COVID-19 pandemic, many pulmonary rehabilitation programmes have transitioned rapidly to remote delivery models. 1,2 While studies have shown it is possible to deliver exercise training, physical activity counselling, education and self-management training remotely, with similar outcomes to traditional centre-based pulmonary rehabilitation, 3,4 all existing clinical trials have included an in person exercise test prior to programme commencement, to assess safety of exercise (e.g. degree of oxyhaemoglobin desaturation) and enable accurate exercise prescription. 3,5 During the COVID-19 pandemic centre-based or in person assessments of exercise capacity are not able to be performed in most centres. As a result, some pulmonary rehabilitation programmes have commenced exercise testing at home, using tests with minimal space requirements such as sit-to-stand (STS) or step tests, and with or without remote monitoring of oxyhaemoglobin saturation (SpO2) and heart rate. Other programmes are not conducting any exercise testing prior to commencing patients on pulmonary rehabilitation programmes at home. It is not clear which of our current tests of functional exercise capacity are suitable for home and / or remote administration.
The research questions for this rapid review were: Which functional exercise tests have been conducted in the home setting in people with chronic lung disease? Which functional exercise tests have been conducted remotely in people with chronic lung disease? What are the clinimetric properties of tests that have been conducted at home or remotely, including feasibility, reliability, validity and responsiveness to pulmonary rehabilitation? Can these functional exercise tests be used to assess safety (particularly oxyhaemoglobin saturation) and prescribe exercise intensity, either in person or remotely?
Methods
The protocol was registered on PROSPERO (CRD42020182375) on 27 April 2020.
We did not include case studies. Review articles were not included, but we reviewed their reference lists for studies that met our inclusion criteria. Otherwise there were no restrictions on study design. We included studies investigating clinimetric properties, descriptive studies and studies where the test was used to evaluate the effects of an intervention. Only studies published in English were included.
Data extraction and management: One author conducted data extraction using a standardised template, with random checks on accuracy by a second reviewer. The following information was extracted: Methods of study (date/title of study, aim of study, study design, primary outcome, other outcomes) Participants (diagnosis, age, sex, disease severity, inclusion criteria, exclusion criteria, method of recruitment of participants) Intervention (if applicable, description of the intervention) Exercise test – name, details of protocol (if provided), location of test (home, centre, other) and monitoring (in person, remote, none), variables monitored Outcomes pre/post intervention data where applicable, details of clinimetric properties if applicable Details of any physiological monitoring, including but not limited to pulse oximetry Whether the results of the test were used to prescribe exercise and if so, the methods used.
Assessment of risk of bias: We considered risk of bias according to study design and methods of analysis, and this was documented in the data extraction form. As this was a rapid review we did not conduct a formal assessment using a risk of bias tool.
Outcomes: The main outcomes of interest were the number of reports of home or remote administration of each exercise test. Additional outcomes were patient variables monitored for each test (e.g. SpO2, heart rate, symptoms, blood pressure); methods used to prescribe exercise training intensity; and clinimetric properties for each test – feasibility, reliability, validity and responsiveness, using the metrics reported by the authors.
Data synthesis: A narrative synthesis was performed for each exercise test separately. For each exercise test we reported whether it had been performed at home or with remote monitoring, including the number of reports. Patient variables monitored for each test (e.g. SpO2, heart rate, symptoms, blood pressure) were reported descriptively. Any methods used to prescribe exercise training intensity were reported descriptively.
We reported clinimetric properties for each test, from all studies where these are reported, not just those performed at home. We reported feasibility (e.g. number of participants who could perform the test), reliability (e.g. intra-class correlation coefficient (ICC)), validity (e.g. correlation with gold standard exercise tests) and responsiveness to pulmonary rehabilitation (e.g. mean changes pre/post rehabilitation and measures of variability). Where possible we calculated an effect size to describe responsiveness.
We had intended to examine outcomes separately by subgroups with different lung diseases (e.g. COPD, ILD), but there were insufficient data for diseases other than COPD, so these analyses were not performed.
Results
The MEDLINE search identified 3778 studies (excluding duplicates) of which 3654 were excluded based on title and abstract. Of the 128 full text papers screened, 84 were included (85 reports). This included five studies examining the 6MWT, 7 –11 39 studies examining STS tests, 12 –50 35 studies examining step tests 19,24,50 –82 and 17 studies examining the Timed Up and Go (TUG). 17,19,24,33,42,49,50,83 –92 Ten studies examined more than one test, including four that examined STS and TUG, 17,42,48,49 four that examined two kinds of STS test, 29,32,44,45 and two studies (in three reports) that examined STS, TUG and step tests. 18,23,50 The PRISMA diagram is in Figure 1 and study characteristics are in Supplementary Tables S2-S5. An overall summary of the review findings is in Figure 2. No adverse events were reported in any studies.

Study selection.

Summary of review findings.6MWD = distance walked on 6-minute walk test, 6MWT = 6-minute walk test, STS = sit to stand, TUG = Timed Up and Go.
6-minute walk test
Home: One randomised crossover trial (RXT) compared home and centre-based 6MWTs 8 and one RXT compared an outdoors to a centre-based 6MWT. 7 Both included people with moderate to severe COPD. The centre-based 6-minute walk distance was significantly longer than the distance recorded at home 8 (Table 1) with a mean difference that exceeded the minimal important difference of 30 metres. 93 The 6MWT track lengths were shorter at home (mean 17 metres) compared to the centre (30 metres) and 42% of tests were conducted indoors. Comparison of indoor vs outdoors 6MWT (conducted on a flat sidewalk), both using a 30-metre track, showed no difference in the distance walked (Table 1). 7
Difference between centre-based and home or remote test administration.
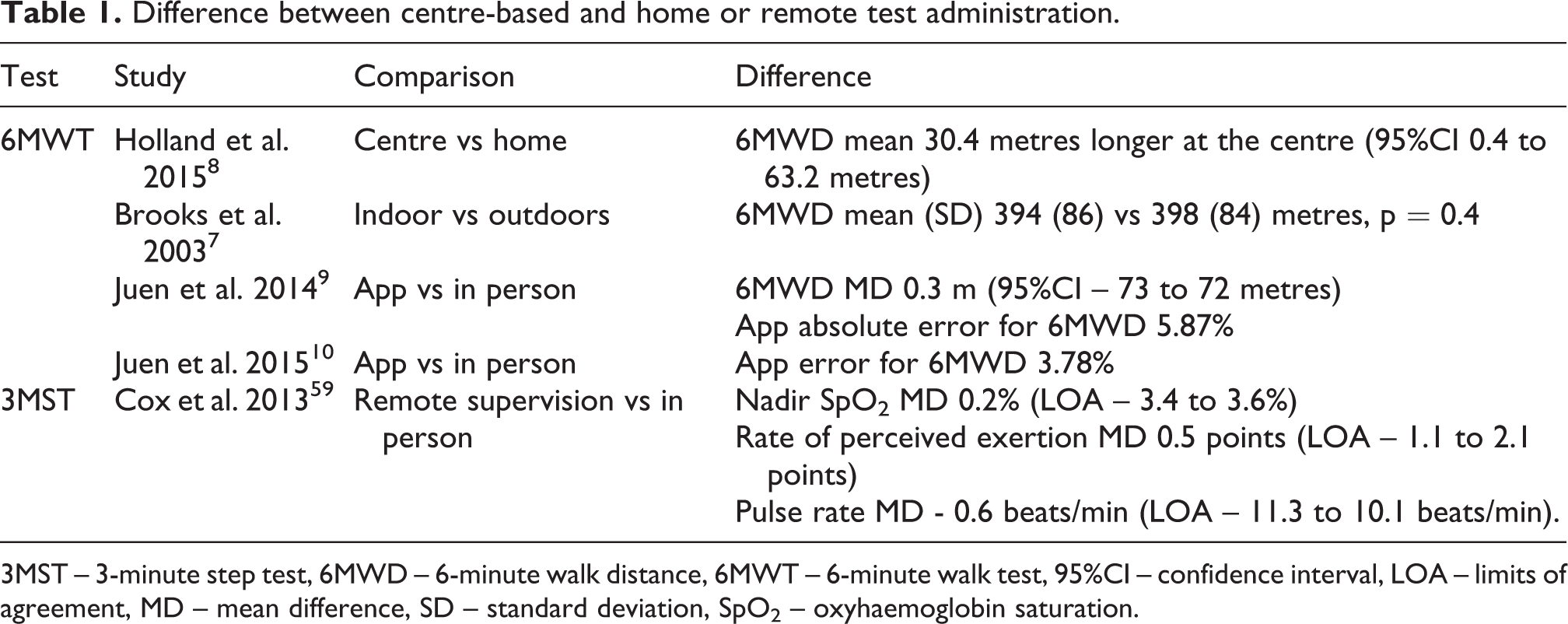
3MST – 3-minute step test, 6MWD – 6-minute walk distance, 6MWT – 6-minute walk test, 95%CI – confidence interval, LOA – limits of agreement, MD – mean difference, SD – standard deviation, SpO2 – oxyhaemoglobin saturation.
Remote: Two studies by the same group aimed to validate two different phone apps for remote monitoring of the 6MWT in people with chronic respiratory conditions (mostly COPD and asthma). 9,10 Both apps recorded the 6-minute walk distance using accelerometry, and one also provided voice and vibrating instructions. 9 Both apps included monitoring by pulse oximetry, however these data were not reported. The 6-minute walk distance measured by the apps was similar to that measured by the researchers in person (Table 1).
Feasibility: One study in participants with COPD reported that 58% of tests were conducted outdoors because a track of sufficient length was not available inside the home. 8
Clinimetric properties: Home-based 6-minute walk distance was highly reliable when performed twice on the same day, with ICCs ≥ 0.99. 8 Intra-rater reliability was high for both outdoor and indoor tests (ICCs 0.97 and 0.99 respectively). 8
Safety assessment: All studies reported monitoring the 6MWT using pulse oximetry and three also used symptom scales for dyspnoea and perceived exertion. 7,8,11
Exercise prescription: One study used the 6MWT for exercise prescription in 39 people with COPD. 11 Walking exercise was prescribed at 80% of the average speed walked on the 6MWT. This exercise prescription was well tolerated over 10 minutes of walking, generally achieving more than 60% of peak oxygen uptake (VO2) with a steady state by the fourth minute.
Sit-to-stand tests
Six different STS tests were used (Table S2). These were the five times sit to stand test (5STS, 14 studies), where the time taken to stand up and sit down five times from a standard height chair is recorded; the 10 times sit to stand test (10STS, 2 studies) using a similar protocol; the 30-second sit to stand test (30secSTS, 9 studies) where the number of sit-to-stand repetitions in 30 seconds is recorded; the 1-minute sit-to-stand test (1minSTS, 13 studies) as well as small numbers of studies using 2-minute tests (2minSTS, 1 study) and 3-minute tests (3minSTS, 2 studies).
Home: Tests used at home were the 5STS, 34,42 10STS, 19,24 and the 1minSTS. 50 Participants (n = 381) had COPD, some were using home oxygen therapy 50 and some were recovering from an acute exacerbation. 34 All home testing involved in person supervision from a researcher or clinician.
Remote: No studies reported remote administration or monitoring of a STS test.
Feasibility: In a study of patients with stable COPD (n = 475), 15% of participants were unable to complete the 5STS. 27 Those who were unable to complete the test were significantly older (mean (SD) 73(10) vs 68(10) years), had higher levels of chronic dyspnoea (Medical Research Council scale 4.1(1.0) vs 3.3(1.1) points), lower quadriceps maximal voluntary contraction (44(13) vs 60(17)%predicted) and lower incremental shuttle walk distance (84(66) vs 224 (126) metres). A study comparing the 5STS to the 30secSTS in 128 people with moderate to severe COPD reported that all participants could complete the 5STS but 7% could not complete two trials of the 30secSTS. 45 One additional trial reported that 3 of 50 participants with COPD (6%) could not complete any repetitions of the 30secSTS. 26 Of those participants who felt it was strenuous to undergo a STS (69%), most (93%) found the 30secSTS more strenuous than the 5STS. 45 In a clinical trial of inpatient pulmonary rehabilitation including 60 participants with moderate to severe COPD, all could complete both the 30secSTS and the 1minSTS. 44 No feasibility data were reported for the 10STS, 2minSTS or 3minSTS.
Clinimetric properties: Reliability, validity and responsiveness of STS tests are in Table 2. Test-retest reliability was high for the 5STS, 30secSTS and 1minSTS. The 5STS, 30secSTS and 1minSTS had moderate to strong correlations with other measures of exercise capacity, with higher values for the 1minSTS than the other tests. There were moderate correlations with quadriceps strength and weak correlations with daily life physical activity. Predictive validity was demonstrated only for the 1minSTS, with lower values predicting increased mortality at 2 and 5 years. 21,36 Responsiveness to pulmonary rehabilitation was evident for 5STS, 30secSTS and 1minSTS, with moderate to large effect sizes.
Clinimetric properties of sit-to-stand tests.

Data are mean (95% confidence interval) except where specified.
1minSTS – 1-minute sit to stand test, 2minSTS – 2-minute sit to stand test, 3minSTS – 3-minute sit to stand test, 30secSTS – 30-second STS test, 5STS – five times sit to stand test, 6MWD – 6-minute walk distance, 95%CI – 95% confidence interval, AUC – area under the curve, CCI – Charlson Comorbidity Index, CF – cystic fibrosis; COPD – chronic obstructive pulmonary disease; HR – hazard ratio, ILD – interstitial lung disease; ISWT – incremental shuttle walk test, LT – lung transplant; MD – mean difference, NR – not reported, r – Pearson’s correlation coefficient, SD – standard deviation, VO2peak – peak oxygen uptake.
Safety assessment: Most studies did not report using any monitoring during the STS test (24 / 40 studies, 60%, Table S2).
A comparison of three STS tests in people with COPD found significantly greater desaturation on the 1minSTS than the 30secSTS or 5STS (mean −3(SD 4) vs −1(2) and −1(2) respectively). 32 Greater desaturation on 1minSTS than 30secSTS was reported in a second study in COPD (mean −2.6 (2) vs 2(1.8). 44 The 1minSTS also gave rise to significantly greater increases in heart rate than the 30secSTS or 5STS (mean 22(13) vs 16 (10) and 7(7)) and higher fatigue scores (median 2 vs 0.5 vs 0). 32 Dyspnoea scores on 1minSTS did not differ from the 30secSTS but were significantly greater than 5STS (median 2.5 vs 1 vs 0) with a similar pattern of findings for systolic blood pressure (median 30 vs 20 vs 0 mmHg). 32
In comparison to the 6MWT and cardiopulmonary exercise test (CPET), the 1minSTS provoked less oxyhaemoglobin desaturation and a smaller rise in heart rate (Table 3). The VO2peak was also significantly lower during 1minSTS than during the CPET (median 1.68 [IQR 1.38, 2.29] vs 1.25 [1.03, 1.86]). 37 Symptom scores for dyspnoea and fatigue were variable, with some studies reporting that they were similar across the tests, 25,39 higher on CPET than 1minSTS, 37 higher on 6MWT than 1 minSTS, 35 or higher on 1minSTS than 6MWT. 16
Fall in oxyhaemoglobin saturation and rise in heart rate on 1-minute sit-to-stand test compared to conventional exercise tests.

Data are mean (SD) or median [interquartile range). Data are decrease in SpO2 from baseline, with the exception of Briand et al and Crook et al, which are nadir SpO2.
1minSTS – 1-minute sit-to-stand test; 6MWT – 6-minute walk test; CF – cystic fibrosis, COPD – chronic obstructive pulmonary disease, CPET – cardiopulmonary exercise test; ILD – interstitial lung disease.
Exercise prescription: No studies used any of the STS tests for exercise prescription.
Step tests
Five different step tests were used (Table 3): 6-minute stepper test (6MStepper) (15 studies), using a hydraulic stepper; a 3-minute step test (3MST) (9 studies), most at a fixed cadence (7 studies); incremental step tests (5 studies), where the stepping rate increases regularly throughout the test, using either the Chester protocol (4 studies) or a version modified for patients with lung disease (modified incremental step test, MIST, 3 studies); a step oximetry test (4 studies) involving either stepping on and off a single step 15 times (3 studies) or for as long as possible (1 study); and a 6-minute step test on a single step at a free cadence (2 studies).
Home: Two studies (3 reports) used the 6MStepper to assess exercise capacity before and after a rehabilitation programme at home. 19,24,50 These tests used a hydraulic stepper with in person supervision in the home. Participants (n = 337) had moderate to severe COPD and some were using long-term oxygen therapy.
Remote: One study compared a remotely supervised 3MST to a 3MST monitored in person in 10 adults with CF and moderate lung disease. 59 Remote supervision took place via videoconferencing and included measures of SpO2 and pulse rate via pulse oximetry, with the monitor visible to the health professional via videoconferencing. Measures of dyspnoea and perceived exertion were also collected. There was good agreement between the directly supervised and remotely supervised tests for nadir SpO2, pulse rate and rate of perceived exertion (Table 1). Nine of 10 participants indicated no preference for in person or remote supervision, with one participant preferring in person supervision.
Feasibility: Feasibility varied across the different step tests. One study reported that in patients with bronchiectasis the Chester Step Test was not as well tolerated as the MIST, which starts at a lower cadence and increases more slowly. 57 The Chester Step Test was stopped more frequently than the MIST by the examiner (58% vs 41% of tests), either because the participant could not maintain the cadence, or due to desaturation. 57 In contrast the entire 3MST at fixed cadence was completed by 97 of 101 adults with CF. 68 One study reported that all participants (n = 84 with ILD) could complete the 6minStepper test, 64 however people using supplemental oxygen were not included. Some studies excluded participants with orthopaedic problems that would have prevented them undertaking the test, 76 making it difficult to assess the feasibility of tests across the population of people with chronic lung disease.
Clinimetric properties: Reliability, validity and responsiveness of step tests are in Table 4. The 6minStepper, MIST and Chester step tests demonstrated good test-retest reliability, with limited data for other tests. Although the ICC for the 6minStepper was high (0.94) the second test recorded up to 42 steps more than the first test, due to warming of the hydraulic jacks in the stepper device. 55,58 There was some evidence of criterion validity for all tests, with moderately strong correlations to other important measures such as 6-minute walk distance or physical activity in daily life. Data for responsiveness to pulmonary rehabilitation was only available for the 6minStepper and 3MST (free cadence), with variable effect sizes.
Clinimetric properties of step tests.
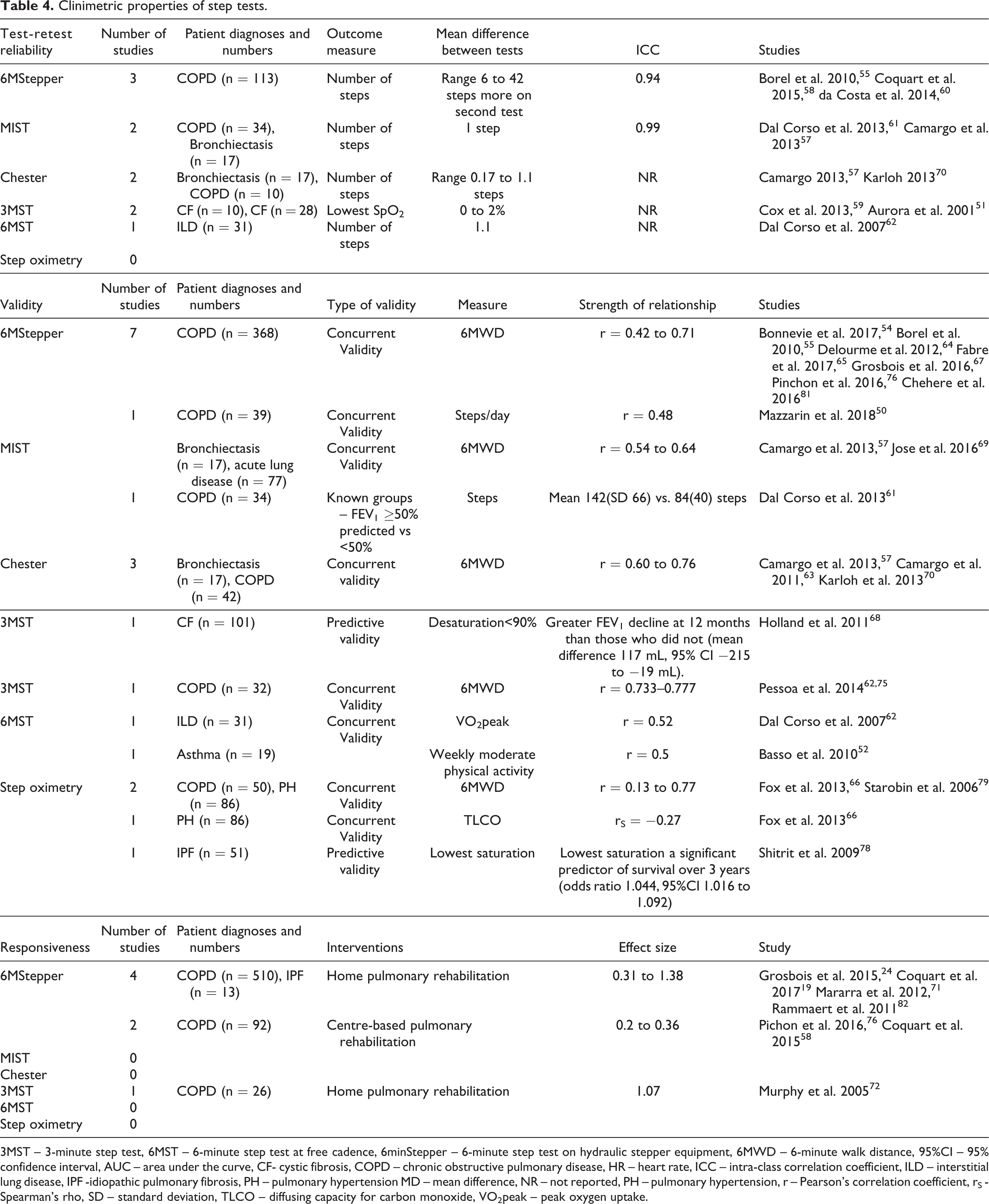
3MST – 3-minute step test, 6MST – 6-minute step test at free cadence, 6minStepper – 6-minute step test on hydraulic stepper equipment, 6MWD – 6-minute walk distance, 95%CI – 95% confidence interval, AUC – area under the curve, CF- cystic fibrosis, COPD – chronic obstructive pulmonary disease, HR – heart rate, ICC – intra-class correlation coefficient, ILD – interstitial lung disease, IPF -idiopathic pulmonary fibrosis, PH – pulmonary hypertension MD – mean difference, NR – not reported, PH – pulmonary hypertension, r – Pearson’s correlation coefficient, rS - Spearman’s rho, SD – standard deviation, TLCO – diffusing capacity for carbon monoxide, VO2peak – peak oxygen uptake.
Safety assessment: All studies reported monitoring step tests with pulse oximetry and most also used symptom scales for dyspnoea and perceived exertion (Table S3). Several studies reported that the degree of desaturation was less on the 6minStepper than on 6MWT (SpO2 2.3 to 3% more desaturation on 6MWT, 4 studies). 64,71,76,81 Desaturation on the 6MST with free cadence was not different to 6MWT 52 or CPET. 62 A 15-step oximetry test resulted in similar desaturation to a 6MWT in patients with idiopathic pulmonary fibrosis (mean nadir SpO2 86(SD 8)% vs 86 (7)%). 77 In contrast, an incremental step test (MIST) resulted in greater desaturation than a CPET (−7(5)% vs −3(3)%), but with similar rise in heart rate and similar symptoms. 61 A 6MST with free cadence caused a greater rise in heart rate and more lower limb fatigue than a 6MWT, 52 with similar findings for the 6minStepper. 64
Exercise prescription: Three studies of the 6minStepper had developed equations for exercise prescription. Two studies generated reference equations for prescribing aerobic training based on heart rate during the 6minStepper, but the equations were not validated. 54,65 and there were no reports of their use to set training intensity in pulmonary rehabilitation programmes. A third study developed reference equations for prescription of resistance training and compared actual vs predicted training load (70% of 1 repetition maximum (1RM)). 53 The mean difference was 30 kg, and the authors concluded this difference was not clinically acceptable and the prediction equation should not be used as a substitute for a 1RM measure. No other step tests had been used for exercise prescription.
Timed Up and Go
Home: The TUG was administered at home in 4 studies (5 reports), 19,24,42,50,92 where it was used to evaluate the effects of a home pulmonary rehabilitation programme 19,24,42,50 or to evaluate change over 12 months. 92 Participants (n = 381) had moderate to severe COPD (FEV1%predicted mean 27 to 42%) and some were using home oxygen therapy. 50 All home testing involved in person supervision from a researcher or clinician.
Remote: No studies reported remote administration or monitoring of the TUG.
Feasibility: Two studies reported excluding participants who could not perform the TUG (13% and 3% of those recruited). 89,90
Clinimetric properties: Reliability, validity and responsiveness of the TUG are in Table 5. Test-retest reliability was high. Concurrent validity was demonstrated by moderate to strong relationships between TUG time and other measures of exercise capacity (6-minute walk distance, peak work, peak VO2) and peak quadriceps force, although one study reported no relationship between leg press and TUG time (data not reported). 49 The TUG time was longer in fallers than non-fallers, and in oxygen users vs non-oxygen users. 83,85,86 Responsiveness varied, with effect sizes ranging from small to large, and the minimal detectable change (95%) ranging from 14 to 33.5%.
Clinimetric properties of Timed Up and Go.

6MWD – 6-minute walk distance, 95% CI – 95% confidence interval, AUC – area under the curve, COPD – chronic obstructive pulmonary disease, ICC – intra-class correlation coefficient, IPF – idiopathic pulmonary fibrosis, MD – mean difference, MDC -minimal detectable change at 95% confidence level, NR – not reported, r – Pearson’s correlation coefficient, PR – pulmonary rehabilitation, SD – standard deviation, VO2peak – peak oxygen uptake.
Safety assessment: Only one out of 16 studies (6%) reported any monitoring of physiological variables during the TUG (Table S4).
Exercise prescription: No studies used the TUG to prescribe exercise.
Discussion
This rapid review identified a range of exercise tests that have been used at home with supervision in people with chronic lung disease (6MWT, STS, 6minStepper and TUG) and a more limited range of tests that have been administered remotely (6MWT, 3MST). Administration of the 6MWT at home may be limited by short track lengths inside the house, although outdoors administration may provide a valid alternative where this is possible. The STS, step tests and TUG are feasible to perform in the home environment but do not reveal the full extent of desaturation with walking. These tests are useful to quantify improvements in physical function with home-based pulmonary rehabilitation but a gap remains in exercise prescription. Consideration should be given to identifying patients at risk of desaturation in whom centre-based exercise testing should be prioritised when local circumstances allow this to be performed safely.
This rapid review addresses an important challenge for pulmonary rehabilitation clinicians during the COVID-19 pandemic. While delivery of pulmonary rehabilitation programmes at home is feasible 3,5 and international bodies are advocating for remote delivery, 1,2 assessment of exercise capacity remains a key gap for many services. This review identifies a number of simple exercise tests that can be performed at home with supervision, when social distancing restrictions allow. These tests allow quantification of pulmonary rehabilitation outcomes, which is particularly important to evaluate in the context of a rapidly changing model of care. The small number of studies on remote administration of the 6MWT and 3MST provides some evidence that this approach would be feasible in selected patients (e.g. those not at risk of falls), but more data are required. While the 6minStepper has been used to prescribe exercise in a small number of studies, reliability of this test may be limited by the equipment required, which appears to require a variable warm up period for the hydraulic jacks. 55,58 Outdoors administration of a 6-min walk test may be possible in some settings, 7 depending on local weather and physical environment, which would allow both assessment of desaturation and prescription of exercise. This approach may prove more acceptable to some patients than an in-home or centre-based test, allowing social distancing to be better maintained. Important considerations for home administration of exercise tests include those specific to the pandemic, including availability of personal protective equipment, as well as those pertinent to all home testing including availability of equipment (standard height chairs and steps) and ensuring a safe testing environment for patients and health professionals.
Limitations to this review relate to both the body of evidence and the review process. A rapid review process was selected to ensure we could quickly address the immediate challenge facing the pulmonary rehabilitation community. We used accepted methodological approaches for a rapid review in order to speed up the process, including searching fewer databases; restricting the types of studies included (e.g. English only); a limited time frame for article retrieval (year 2000 onwards); limiting dual review for study selection and data extraction; and limiting risk of bias assessment. 95 Inherent limitations to our review must therefore be acknowledged. These include searching a single electronic database (Medline) and only including studies published in English, which may have resulted in relevant studies being missed. A single author undertook study selection, and a single author performed data extraction with accuracy checks on a random sample by a second reviewer; this may have increased the risk of error and reduces confidence in the findings. We did not perform a formal quality assessment, although data extraction included risk of bias related to study design and analysis, which was considered during data synthesis. A formal risk of bias assessment may have identified important limitations to study conduct and reporting that were not evident during this rapid review process, which may also reduce the strength of conclusions that can be drawn. The included studies often included a small number of participants and used a wide variety of testing protocols, which limited data synthesis. Feasibility of the tests was poorly documented and key patient groups were often excluded from studies (e.g. those using oxygen therapy or those who could not perform the test). Clinimetric properties of tests were rarely assessed in the home setting, but given the nature of the tests (STS, step and TUG) and the use of face-to-face supervision, these seem unlikely to vary substantially from those properties documented in centre-based testing. A wide variety of testing protocols were used across the included studies, with reports of six different variants of STS and five variants of step tests, sometimes with differences in protocols between studies of the same test. This is a limitation to consistent clinical application. We only evaluated tests where we identified reports of their use in the home or remotely, so other tests that may be feasible in the home setting (e.g. treadmill testing, gait speed tests) were not included. A small number of studies were available for patient groups other than COPD.
In conclusion, pulmonary rehabilitation clinicians can confidently perform STS, step and TUG tests at home in people with chronic lung disease, where in person supervision is possible. Remote supervision may also be possible in selected patients, although few data are available. These in-home tests are useful to quantify the outcomes of home-based pulmonary rehabilitation, but do not reveal the full extent of desaturation on exercise, and validated methods to prescribe exercise intensity are not available. Consideration should be given to identifying patients at risk of desaturation in whom centre-based exercise testing should be prioritised, when local circumstances allow this to be performed safely.
Supplemental material
Supplement_19June - Home-based or remote exercise testing in chronic respiratory disease, during the COVID-19 pandemic and beyond: A rapid review
Supplement_19June for Home-based or remote exercise testing in chronic respiratory disease, during the COVID-19 pandemic and beyond: A rapid review by Anne E Holland, Carla Malaguti, Mariana Hoffman, Aroub Lahham, Angela T Burge, Leona Dowman, Anthony K May, Janet Bondarenko, Marnie Graco, Gabriella Tikellis, Joanna YT Lee and Narelle S Cox in Chronic Respiratory Disease
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: CM is partially supported by the Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPq) (process number: 200042/2019-0), and Coordenação de Aperfeiçoamento de Pessoal de Nível Superi – Brazil (CAPES) – Finance Code 001. NSC holds a National Health and Medical Research Council (NHMRC) Early Career Fellowship (GNT 1119970).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.