
Abstract
Current evidence indicates that although they are correlated, health literacy (HL) and patient activation (PA) are distinct. This article describes how HL, PA and their determinants intersect and diverge and how these concepts might inform the development of self-management interventions. The concepts of HL and PA contribute to self-management interventions in different ways. HL includes the skills and confidence required for self-management while PA focuses more on motivation and ability to take action. In this light, communication of concepts on HL and PA needs to be more widely understood by academics, researchers and policy experts as each of them plays a unique role in promoting self-management for long-term conditions such as chronic obstructive pulmonary disease.
Keywords
Background
COPD self-management
Chronic obstructive pulmonary disease (COPD) self-management involves self-recognition and management of symptoms, taking medication and eating a healthy diet, coping with breathlessness, quitting smoking and engaging in regular physical exercise to maintain good health. 1 Self-management interventions improve COPD health-related quality of life compared to usual care. 2 However, patients are often not involved in self-management activities. 3,4
Patient activation (PA) (having the knowledge, skills and confidence to self-manage chronic illness and collaborate with healthcare providers 5 ) and health literacy (HL) (understanding health information and accessing health services 6 ) have been demonstrated to influence self-management behaviours. 3
What is HL and what are its determinants?
The World Health Organization defined HL as ‘the personal characteristics and social resources needed for individuals and communities to access, understand, appraise and use information and services to make decisions about health’. 7
Previous researchers have identified determinants of low HL including age, educational attainment and socioeconomic status, culture beliefs and practices (Figure 2) and communication skills (including language barriers) between professionals and patients. 8,9 This directly affects individual decisions, actions and their lifestyle behaviours and plays a key role in the prevention and management of chronic illness. 8,10
What is PA and what are its determinants?
PA refers to the knowledge, skills and confidence a person has in managing their own health and care. Activation involves four stages (Figure 1): (i) believing in the patient role, (ii) building patient confidence and knowledge for self-care, (iii) taking action to maintain and improve one’s health and (iv) staying the course even under stress. Measurement of PA informs tailoring confidence building strategies. 11

Stages in patient activation process. ©2018 Insignia Health. Patient Activation Measure® (PAM®) Survey Levels. All rights reserved.
Previous research has reported that symptom burden, illness perception, presence of comorbidities, age, body mass index, physical health status, depression, social support, financial distress and lack of understanding their role in care process were independently associated with lower PA in COPD patients. 12,13
HL and PA
Previous research was focused on the benefits of either HL or PA on health outcomes for COPD patients. 14 Interventions using both concepts are limited. A clearer understanding of HL, PA and their determinants would be useful in informing COPD self-management interventions.
Evidence
HL and health outcomes
Limited HL may be a hidden problem, which could have indirect or direct impacts of health outcomes. A wealth of evidence exists which has established the link between low HL and poor health outcomes or discrepancies in health service utilization. 9
A review published by Taggart et al. showed that improved HL is associated with reductions in SNAPW (smoking, nutrition, alcohol, physical activity and weight) risk behaviours for long-term chronic disease. 15 Likewise, a review published in 2017 by Wang et.al showed significant reductions in COPD-related hospitalizations and patients’ emotional distress and no improvement was observed in the areas of smoking cessation, pulmonary functions and dyspnoea. 16 Studies used individualized motivational interviewing and counselling; group education; combined-type intervention (combination of interventions); providing written materials; telephone coaching or counselling; and computer- or web-based online interventions. 15,16 Specifically, patients with low level of HL were less likely to believe in the chronicity of their disease and more likely to have larger negative emotional representations of their illness.
PA and health outcomes
Many public health initiatives around the world have aimed at changing the behaviour of chronic disease patients by involving them in management of their own health. 14
In the chronic illness care model, PA is a central concept but is the least well-developed component. 17 PA leads to improvements of health outcomes among COPD patients. 14 Similarly, tailored self-management programmes which are tailored to patients’ level of activation to manage their long-term conditions showed improvement in PA measured, quality of life and overall health status. 18
How are HL and PA different?
Researchers have explored the association between HL and PA in both cross-sectional and prospective studies. These have shown that HL and PA are very different concepts and also function somewhat independently. Greene and colleagues showed that PA measures the patient’s self-confidence in self-management of disease whereas HL was more closely related to the ability to use information in health-relevant decisions. 19 A few studies that investigated relationships of HL and PA with self-management of chronic disease conditions showed that HL and PA were weakly correlated with each other, but independently correlated with health outcomes. 20,21
HL applies to broad notions of ‘declarative knowledge’ and ‘procedural knowledge’, where declarative provides factual information on health/healthcare or medicine, while procedural refers to guiding principles about the course of actions. 22 PA determines the patient interest to ease them into the role of an actor in the decision-making and taking responsibility for maintaining their own health. This clearly articulates that HL provides judgemental skills and underlying knowledge about the disease conditions and their management, while PA leads to situational and psychological empowerment of patients, which is essential for behaviour change.
Programmes aimed at HL delivery assume providing a good level of knowledge/skills can empower patients, thus improves health outcomes while those aimed at PA assume that providing specific information and motivation can bring positive outcomes. This clearly posits that intervention aimed at increasing HL might not activate patient, and those aimed at improving activation need not necessarily increase HL. Figure 2 depicts the role HL and PA in self-management of COPD and is supported by concept (Figure 3) presented by Schulz et al. 22

Role of health literacy and patient activation in self-management of chronic obstructive pulmonary disease (COPD).
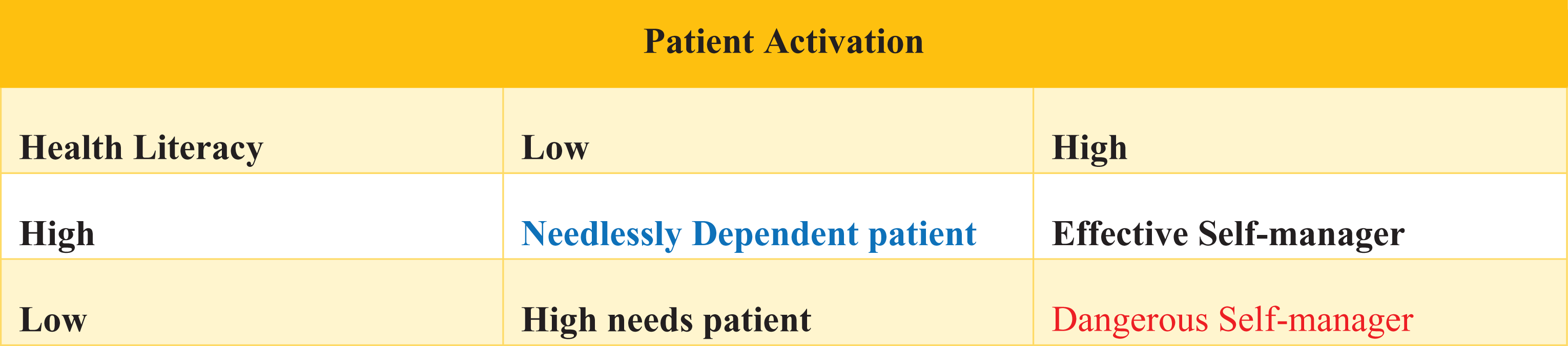
Health literacy, patient activation and self-management of behaviour.
Implications for practice
In seeking to address this gap, the concepts of HL and PA need to be widely understood among the academicians, researcher and policymakers. It is equally important to use both PA and HL in self-management intervention as each of them has unique roles in improving the behaviour of the patients for management of disease.This indicates the necessity of considering both HL and PA in the design of interventions of COPD. Framing a single intervention which integrates both the concepts might result in better health outcomes.
Footnotes
Authors’ note
UNY is receipt of University International Postgraduate Scholarship (UIPA) for PhD, without which the present study could not have been completed.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support from Centre for Primary Health Care and Equity, UNSW for the publication of this article.