
Abstract
To inform recommendations for the exercise component of a healthy lifestyle intervention for adults with obesity and treated obstructive sleep apnoea (OSA), we investigated the total energy expenditure (EE) and cardiorespiratory response to weight-supported (cycling) and unsupported (walking) exercise. Individuals with treated OSA and a body mass index (BMI) > 30 kg/m2 performed an incremental cardiopulmonary exercise test on a cycle ergometer and a treadmill to determine the peak oxygen uptake
Introduction
Obesity is increasing in prevalence across the socio-economic spectrum, with currently over one-third of adults being overweight and over one-tenth being obese worldwide. 1 Although obese individuals who maintain their fitness have a lower cardiovascular mortality than their unfit counterparts, 2 the majority of obese individuals are less physically active than those of normal weight and do not achieve the recommended levels of physical activity to maintain health. 3,4 The inactivity associated with obesity may be compounded in the presence of obstructive sleep apnoea (OSA), itself known to be associated with fatigue and inactivity, which persists even when the OSA has been effectively treated with continuous positive airway pressure therapy (CPAP). 5 The presence of OSA among obese individuals is also an independent risk factor for cardiovascular disease 6,7 such that those with OSA and obesity have a higher morbidity and mortality than those with obesity alone. 8,9 Therefore, there is interest in developing lifestyle interventions that target both weight loss and cardiorespiratory fitness, for adults with obesity-related OSA, with the aim of reducing long-term cardiovascular risk. 10 –12
Health organizations have merged recommendations on diet, physical activity and obesity 13 acknowledging that a healthy lifestyle is better realized by a combination of diet and exercise than by diet alone. 14 –16 However, although many studies have compared different diets and their impact on weight loss 17 few have investigated which exercise training modality is the most effective for individuals with obesity to achieve healthy weight loss whilst improving cardiovascular fitness. 10
Weight loss attributable to exercise will be directly proportionate to the energy expenditure (EE) that is, work, whilst cardiorespiratory fitness, as measured by peak oxygen uptake
Although the ideal modality for adults with obesity requires significant EE whilst stimulating improved fitness, the relationship between intensity, modality, exercise tolerance and total EE in this population remains unknown. In healthy individuals, it is established that
In order to better inform recommendations for exercise, this study evaluated whether weight-supported exercise (cycling) was associated with a greater total EE at a matched aerobic intensity to intolerance compared with unsupported exercise (walking) in adults with obesity and treated OSA. We hypothesized that individuals with obesity would sustain cycling for longer than walking, resulting in their achieving greater work, due to the weight being supported with cycling.
Methods
Study design
This was a cross-sectional study (clinicaltrials.gov NCT01930513) approved by the local ethics board (JREB2010-10). After providing written informed consent, each participant completed six tests by attending four assessment visits each separated by at least 48 hours. The first two visits comprised, in random order, an incremental treadmill (ITM) and cycle (ICE) test. The third and fourth visits comprised, in random order, two constant speed tests on a treadmill and two constant power tests on a cycle ergometer. Age, gender, height and weight were documented and spirometry completed. 25
Participants
Individuals with a BMI > 30 kg/m2 were recruited from a sleep clinic. All patients had OSA treated with CPAP for at least 3 months. As part of their referral for sleep apnoea patients underwent a medical evaluation. Individuals with chronic lung or heart disease diagnosed by history, examination or pulmonary function tests or other conditions that might interfere with exercise, were excluded.
Incremental exercise
The purpose of the incremental test was to determine
Constant power exercise
The purpose of the constant power tests was to observe the tolerability of exercise and measure the EE achieved at two recommended training intensities (simulating exercise training sessions) with the different modalities. Two constant speed treadmill tests and two constant power cycle tests were performed, in separate sessions, at a matched intensity of 80 and 60%
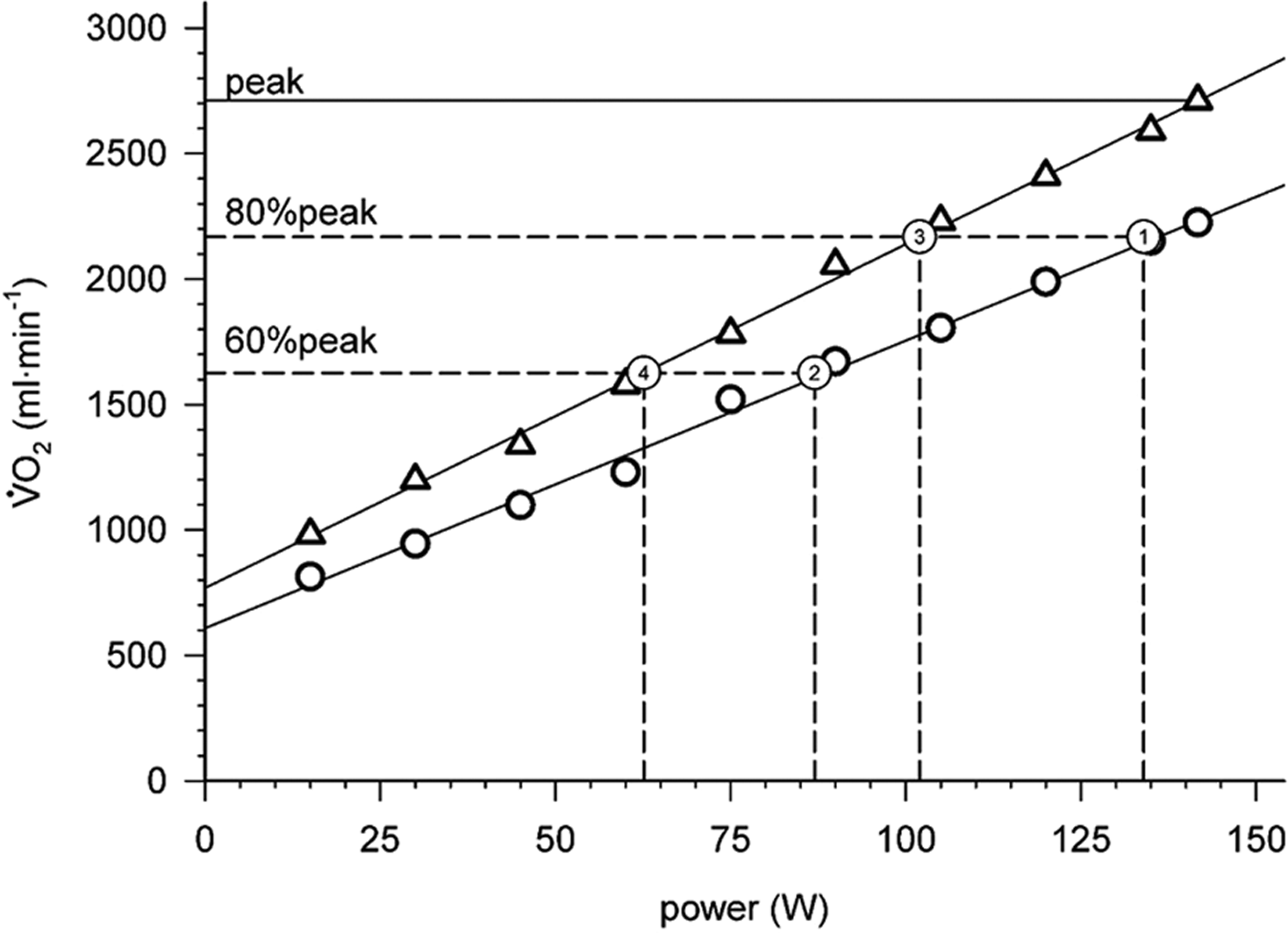
An example of how the power was calculated for the constant power tests from the incremental treadmill (triangles) tests and cycle (circles) tests. The
EE for exercise and recovery phases was estimated from the measured
Statistical analysis
The baseline demographics are presented as mean (SD) for normally distributed variables and median (interquartile [IQ] range) for variables not normally distributed. The peak parameters for the ITM and ICE were compared by paired t-tests for parametric data and Wilcoxon rank test for non-parametric data.
The EE of the constant power tests was analysed using a repeated measures analysis of variance (2 × 2) with factors of intensity (moderate and vigorous) and modality (treadmill and cycle). In the event of significant effects, post hoc comparisons were made using paired t-tests for parametric data and Wilcoxon rank test for non-parametric data.
A qualitative visual comparison of the average cardiorespiratory response was produced by smoothing individual tests into epochs of 10% increments of the test duration (i.e. deciles) using a negative exponential data transformation and then calculating the group mean at each decile.
Sample size was determined to ensure adequate statistical power to test the hypothesis of a significant effect of modality on exercise tolerance resulting in greater work. The estimated standard deviation of the difference in exercise time in repeated constant power exercise is 2.8 minutes. 33 A difference of 3.4 minutes would be considered a large effect. 34 We used a more conservative approach, medium effect (2.1 minutes), to ensure an adequate sample size. To reject the null hypothesis of no difference between modality using a two-tailed paired t-test (power = 0.80 and significance level = 0.05) of dependent means, we estimated that 16 participants needed to complete this study.
Results
Participants
Eighteen patients agreed to participate. One was excluded due to undiagnosed COPD and another sustained an injury at home. Sixteen participants completed all six exercise tests (Table 1).
Demographics.

BMI: body mass index, FEV1: forced expired volume in one second; FVC: forced vital capacity; CPAP: continuous positive airway pressure; AHI: apnoea-hypopnoea index. aMean [SD] unless which represents Median [interquartile range].
Incremental exercise
A comparison of the results at peak exercise between the ITM and ICE tests.a

ITM: oncremental treadmill test; ICE: incremental cycle ergometer; HR: heart rate; SpO2: oxygen saturation; BP: blood pressure;
aMean (SD) HR predicted = 220 – age (years), NA: not applicable.
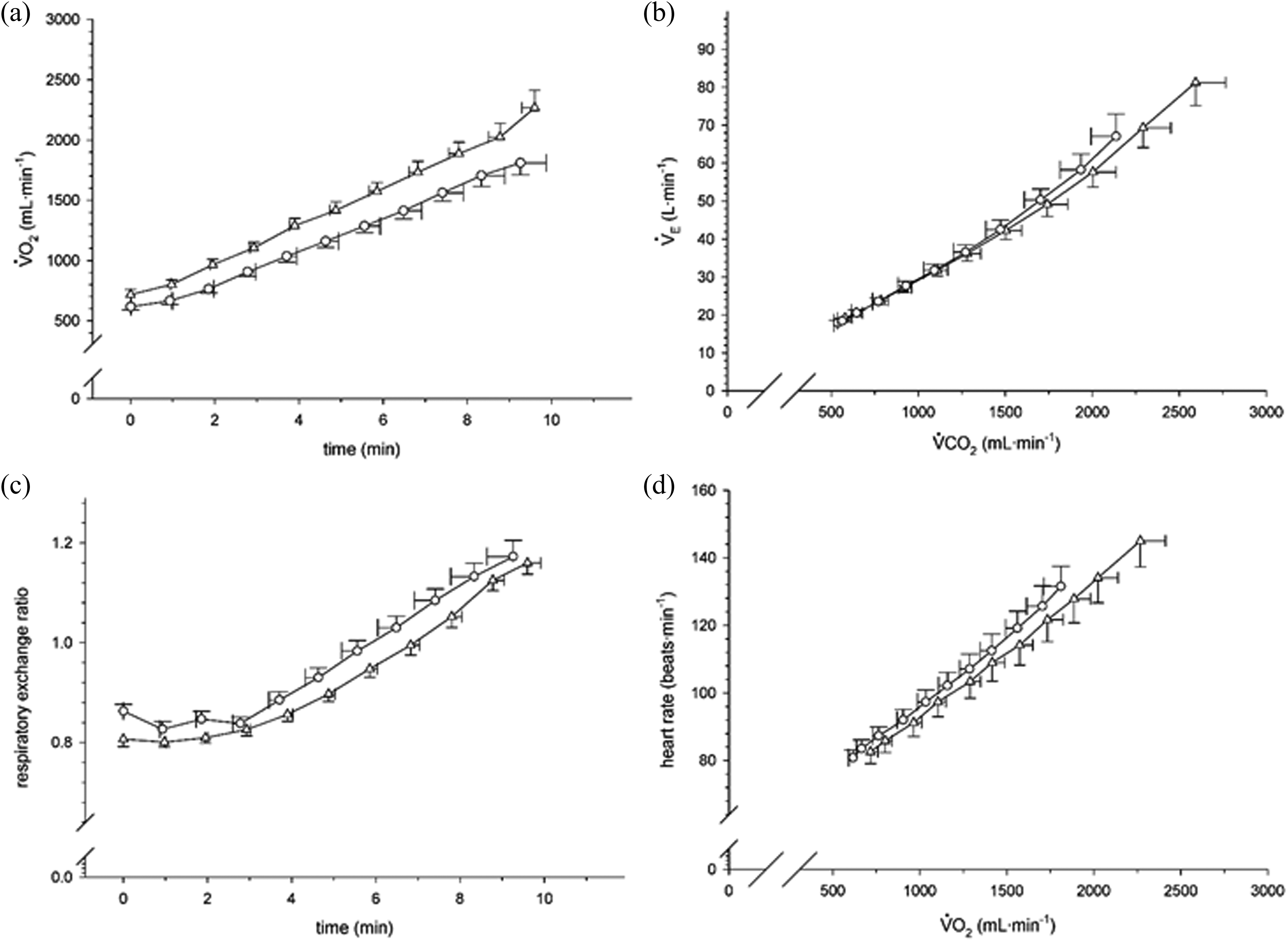
A comparison of the exercise cardiorespiratory responses between incremental treadmill (triangles) and cycle (circles) ergometer tests in adults with obesity.

A comparison of the symptom responses between incremental treadmill (triangles) and cycle (circles) ergometer tests in adults with obesity.
Constant power exercise–simulated training sessions
The protocol resulted in a linear increase in
A comparison of the constant power endurance exercise parameters between treadmill walking and cycling at two matched intensities.

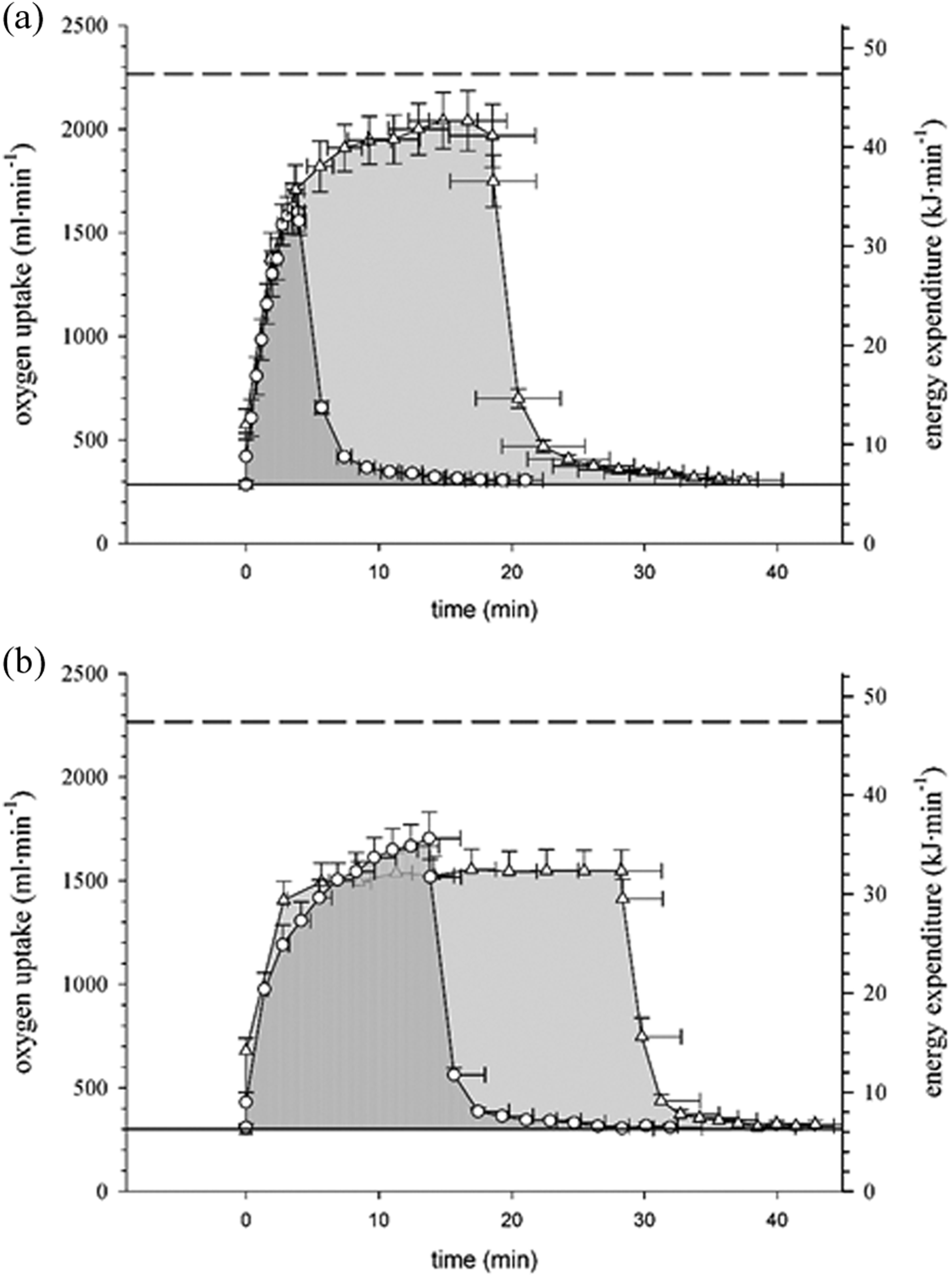
A comparison of the energy expenditure between weight-unsupported (treadmill) and -supported (cycling) exercise in adults with obesity. Treadmill (triangles) and cycling (circles) at high (a) and moderate (b) intensity exercise. The shaded area under the curve represents total energy expenditure, that is, work, above rest including recovery. Dashed line --- represents VO2pk.
Discussion
The optimal exercise prescription (the interactive effect of modality and intensity), to improve fitness and promote healthy weight loss, is unknown for adults with obesity. We measured EE and cardiovascular responses during two simulated exercise training sessions and noted that at a matched intensity the attainable total EE was greater during walking than cycling, for both vigorous (80%
Our observations project that a thrice weekly treadmill exercise regimen would result in a greater EE of 388 and 277 kcal/week, at 80% and 60%
To measure EE at comparable absolute cardiorespiratory intensities we matched the test intensity by oxygen uptake rather than by mode specific intensity of mechanical power or a physiological surrogate, for example, HR, for oxygen uptake. The former will be influenced by differences in movement economy between modalities. Whereas HR-based estimates of
Although the absolute aerobic capacity of this group was high, it was low relative to their body weight, with a
As OSA is common in the population with obesity and often undiagnosed, we circumvented this potential confounder by recruiting patients with OSA successfully treated with CPAP. Our study did not include non-obese control participants as it was designed to inform the exercise prescription by comparing modalities at matched intensities, among participants with obesity. Nor did it include individuals with obesity but without OSA or those with untreated OSA. Although in the absence of specific cardiopulmonary limitations it is unlikely that individuals with obesity but without OSA would respond differently from our population, the generalization of our observations to other populations should be independently confirmed. In individuals with obesity and confirmed OSA, the latter is promptly managed but the concomitant lifestyle modifications designed to reduce cardiovascular risk are much less frequently addressed. 39 As our study population was limited to participants with a BMI of mainly 30 to 40 kg m−2our observations may not directly extrapolate to Class III obese (BMI > 40 kg m2) individuals. We do note that the three participants with a BMI >40 kg m−2 had similar responses to the main group. Our observations may also not extrapolate to individuals with obesity and concomitant chronic respiratory disease, frequently referred for exercise training, in whom the ventilatory limitations to incremental exercise testing may be unaffected by the testing modality. 40 We have focused on the desirable outcomes of EE and cardiovascular response from endurance exercise bouts, but other factors such as individual preference, comfort and risk of injury may impact on exercise adherence and therefore outcome of longer term training.
We acknowledge, that, by design, the vigorous test was always completed first as it was predictably the shorter test. The factor of interest, however, was ‘modality’ and its order was randomized. The two endurance tests were completed on the same day due to participant preference during the protocol development. Figure 4 shows that the EE had returned to baseline before the subsequent test. Although there was potential for these two factors to bias the results, the magnitude of the differences between the moderate and vigorous tests would suggest that the impact was minimal. We used a semi-recumbent position for the cycle ergometer to ensure that discomfort from an upright cycle was not the limiting factor. There are some reports that show that there may be a slightly lower
In summary, individuals with obesity and treated OSA tolerated treadmill walking at moderate to high intensities better than cycling resulting in greater EE, with increased or similar cardiorespiratory responses. This observation may inform their exercise prescription to contribute to a negative energy balance whilst stimulating cardiorespiratory fitness. Although current guidelines for obesity suggest the equivalence of modalities, 19 the above observations would support walking as the preferred training modality for achieving the combination of weight loss and increased cardiorespiratory fitness.
Footnotes
Authors’ contributions
RAE contributed to the study conception and design, led the data collection, analysis and interpretation of data and drafted the manuscript. TED contributed to the study design, data collection, analysis and interpretation of data and revised the article critically for important intellectual content. PR contributed to data collection, interpretation of data and revising the article critically for important intellectual content. DB contributed to the study design, interpretation of data and revising the article critically for important intellectual content. RSG contributed to the study design, interpretation of data and revised the article critically for important intellectual content. Dr Goldstein is the guarantor of the article.
Author note
The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This article/paper/report presents independent research funded by the National Institute for Health Research (NIHR).