
Abstract
The aim of this study was to describe the level and perception of control in severe asthma in Trinidad after the introduction of revised guidelines for asthma management. Adult asthmatics (N = 329) at Trinidad’s chest clinics were cross-sectionally examined for guideline-defined disease control. Patients’ mean (SD) age was 54.36 (14.9) years, with body mass index = 28.54 (7.4) kg/meter2, and females were proportionally more (246, 74.74%). Measured (45.29%) and perceived (18.96%) uncontrolled disease were poorly concordant (κ statistic = 0.197). Co-morbidity (≥2 conditions) correlated with uncontrolled disease in 55.80% of patients (Spearman correlation p = 0.03). Absolute peak expiratory flow was higher (p < 0.001) in controlled and/or partially controlled disease than in uncontrolled asthma. Routine work limitation, night-time disturbances, work absenteeism, exacerbations, rescue inhalation and perceived control correlated with uncontrolled asthma (p < 0.001). Few patients self-monitored lung function (9.73%) or kept an asthma diary (6.69%), but 65.1% believed they had to live with their symptoms. The asthma burden was at least one hospitalization (53.80%) and emergency department visit (66.36%) in the past year, cough (74.49%), dyspnoea (84.50%), wheezing (80.55%) and chest tightness (66.87%). After the revised guidelines, uncontrolled asthma and related morbidity remain suboptimal, with disagreeing actual and perceived control. Efforts to transform guidelines into patient care with realistic interpretation of control are recommended.
Introduction
The Global Initiative for Asthma (GINA) emphasizes disease control as an essential focal point in its guidelines. Achieving and maintaining symptom control is one of the GINA-identified goals for successful management of the disease. The appropriate pharmacological strategic intervention by the patient and/or family in collaborative agreement with the physician makes clinical control of asthma possible. 1 The goal of asthma management is to achieve complete control of the disease and prevent morbidity irrespective of the severity of the condition. 2 Guidelines call attention to achieving and sustaining control, yet studies suggest asthma control is suboptimal with exacerbations and disease progression. In 2006, GINA put forward a classification of asthma based on the level of control rather than on the earlier disease severity. 3
The targeted aim of asthma management is disease control so that chronic symptoms are either minimal or non-existent, exacerbations are absent or infrequent, emergency department visits or use of rescue medication is absent and daily activities are not limited. 3 The Gaining Optimal Asthma ControL study demonstrated that guideline-derived asthma control was achieved in most patients using the appropriate combination of long-term treatment. 4 Yet, for the most part, guideline-defined disease control is not achieved in the patient with asthma.
Asthma’s health burden is a major global public health concern. In the 2012 World Health Survey, clinical/treated asthma affected 315 million individuals and nearly 623 million were estimated to be currently living with some degree of asthma-related symptoms. 5 Large surveys in adults and children, which assessed the current level of asthma control in Europe (AIRE), 6 the Asia-Pacific region, 7 America 8 and Latin America, 9 show asthma continues to be globally undertreated and adherence to guideline-based management remains suboptimal.
Caribbean asthma guidelines based on the GINA guidelines were first produced in 1997 by the Caribbean Health Research Council (The Caribbean Health Research Council was then known as the Commonwealth Caribbean Medical Research Council), in collaboration with the GINA. The guidelines were revised in 2009 10 and widely disseminated to the ministries of health in CARICOM (Caribbean Community, mainly English-speaking parts of the Caribbean region, Dutch-speaking Suriname and French-speaking Haiti) member countries. They were discussed at professional continuing medical education meetings in the region with a view to implementation. To our knowledge, a formal evaluation of asthma control has not been done since in any Caribbean country. In this article, 5 years after the revised guidelines were implemented, we examined asthma control and perceived control of the disease in patients attending chest clinics in the island of Trinidad.
Methods
The study examined the level of disease control using the Caribbean guidelines and documented perceived control by patients attending the chest clinics. This was an observational cross-sectional study between January and June 2013, in the three outpatient chest clinics in the country. Participating centres were in the north (Port of Spain General Hospital), central (Eric Williams Medical Sciences Complex) and the south (San Fernando General Hospital) of the island. The study was approved by the Ethics Committee of the University of the West Indies, St Augustine Campus, Trinidad, and received institutional approvals from the chest clinics.
The process by which patients are recruited into the clinics is of relevance here. Patients are accepted into the clinics when they are referred for uncontrolled or difficult-to-treat asthma by their general practitioners or after discharge from the emergency department (ED)/department of medicine of the respective hospital. Once stable, patients are discharged to the appropriate primary care facility.
Consenting diagnosed adult patients (>18 years), receiving treatment for asthma were eligible to participate and consecutively recruited as they presented at the clinics. Patients with unstable cardiovascular disease, recent abdominal, thoracic or eye surgery, or any condition that could affect peak expiratory flow (PEF) readings and/or performance were excluded. Researchers documented peak flow measurements in the sitting position using the Clement Clarke Arizona pocket-sized peak flow meter (European Union scale). Since the personal best PEF rate (PEFR) values were unknown, predicted values were used to assess asthma control.
Guideline-defined asthma control was the absence of daytime symptoms, limitation of activity, nocturnal awakenings, need for rescue medication in the past week, no exacerbation in the past year and normal lung function. PEF, absolute and predicted, was used to determine lung function. Partial control was present if limitation of routine work and nocturnal awakenings were present during any day of the week, use of rescue inhaler and daytime symptom disturbance occurred more than twice in the past week and at least one exacerbation was present in the past year. Lung function in this category was <80% predicted. The presence of three or more features of partially controlled disease with an exacerbation in any week was defined as uncontrolled asthma.
Statistics
Data were analyzed using SPSS version 12 for Windows. Continuous variables were described by mean and standard deviation (SD) and discrete variables by number (%). Control was categorized as uncontrolled or not uncontrolled and relationships examined by t-test or χ 2-square test as appropriate. The κ statistic was applied to determine concordance between guideline-based and perceived control.
Results
Patient characteristics
Three hundred and thirty one consenting patients were sampled (100% response rate). Data on two were missing, hence analysis was done on 329 patients. Baseline characteristics are presented in Table 1. The mean age of the sample was 54.36 years, and about 50% of subjects were educated to primary school level. Females were proportionally better represented (74.74%) and 40.43% of patients reported one parent suffered from asthma. Approximately, two-thirds (65.39%) of the population were of East Indian descent, and 68.69% earned less than Trinidad and Tobago (TT$) 5000 per month, (6.3TT$ = 1US$). The mean body mass index (BMI) of the population was 28.54 kg/m2 and was ≥ 25 kg/m2 in 66.46% of participants. Only 65 (20.0%) patients were current or ex-smokers; 11 patients admitted to current smoking.
Characteristics of the patient population.

Asthma control
Asthma control differed between the proportions of patients meeting guideline-defined parameters of control and those perceiving themselves as controlled. (Figure 1). Close to half (n = 149, 45.29%) of the sample had uncontrolled asthma but only 62 (18.96%) patients perceived their disease was not controlled. Many (80.73%) patients said their disease was either controlled (39.45%) or partially controlled (41.28%), though measured complete and partial control was observed in 25.53% and 29.18% of patients, respectively. The κ statistic of 0.197 showed poor concordance for guideline-based and perceived disease control. Asthma was uncontrolled in 44.20% of patients whose BMI ≥ 30 kg/m2. Over two-thirds of patients (65.05%) suffered from another condition, of which hypertension was the most frequent (50.46%) and in 55.80% of patients with ≥2 co-morbid conditions, asthma was not controlled (Spearman correlation p = 0.03).
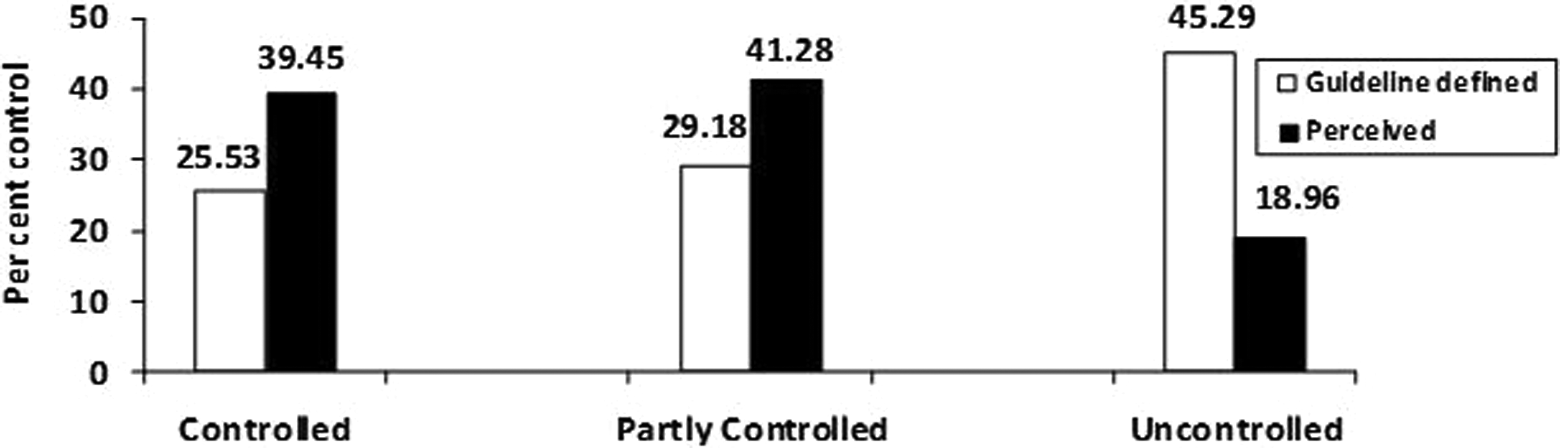
Asthma control (%) evaluated on the Caribbean guidelines and as perceived by patients.
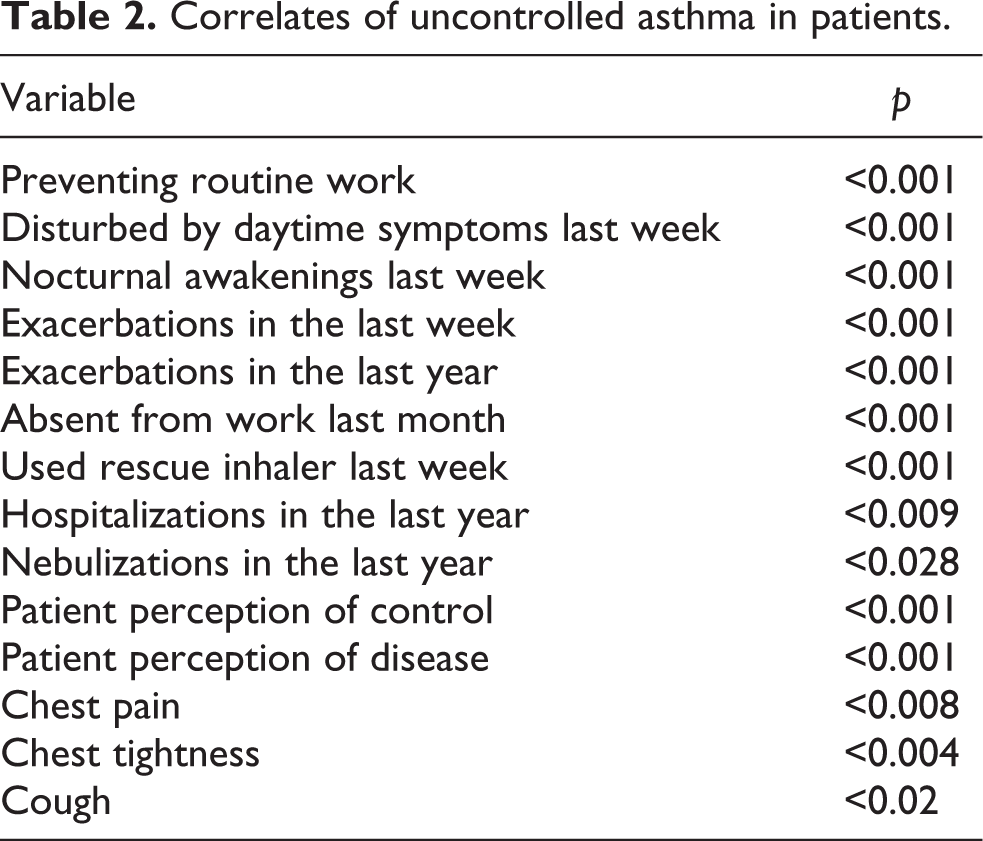
Correlates of poor disease control according to the guideline rubric are seen in Table 2. Uncontrolled asthma was associated with preventing routine work, daytime disturbances, nocturnal awakenings, absenteeism from work, disease exacerbations, inhaling rescue medication and poor subjective perception of control (p < 0.001). Poor control of asthma was related to cough (p < 0.02), chest tightness (p < 0.004), chest pain (p < 0.008), nebulizations (p < 0.028) and hospitalizations in the past year (p < 0.009).
Correlates of uncontrolled asthma in patients.
In 40.50% (n = 133) of patients, PEFR was >80%. The mean PEF in patients with partial and/or controlled asthma was 87.8% (SD = 26.6) of predicted, but in uncontrolled patients was 63.9% (SD = 22.3) (p < 0.001) of predicted. The absolute PEF in these respective patient groups was 326.9 (SD = 107.2) L/minute and 238.7 (SD = 95.0) L/minute (p < 0.001), respectively. Per cent predicted PEF in patients was lower (p = 0.042) in patients with co-morbid conditions (75.0%; SD = 27.0) than in those without co-morbidity (82.0%; SD = 27.7). The PEF in co-morbid asthma was 274.9 (SD = 105.6) L/min and 314.1 (SD = 115.9) L/min in the absence of co-morbidity (p = 0.004).
Patient knowledge and understanding
Nearly as many patients, who said asthma can be controlled (61.09%), believed they had to live with their symptoms (64.74%). Just over a quarter (28.27%) of patients said asthma can be cured, and very few (10.03%) knew the disease was not curable (Table 3). Many patients had ever been evaluated on spirometry (55.93%) and seen a PEF meter (58.66%), but very few (9.73%) knew how to use a peak flow meter at home to check lung function. More than three quarters of the sample (75.68%) said they knew the warning signs of an asthma attack and had discussed an asthma plan with their physician (84.50%); however, only 6.69% kept an asthma diary (Table 3).
Patient knowledge and understanding of disease.

Asthma burden
Asthma-burdened patients with hospitalizations (53.80%) and visits to the ED (66.26%) in the past year (Table 4). Two patients were hospitalized 20 times; 119 patients had been hospitalized a total of 286 times in the past year. Patients with a history of at least one hospitalization had more asthma attacks in the past year were less likely to have controlled asthma but more likely to perceive that their asthma was controlled (p < 0.05 in all cases).
The asthma burden on patients.

ED: emergency department.
At least two-thirds of patients continued to suffer with cough (74.49%), dyspnoea (84.50%), wheezing (80.55%) and chest tightness (66.87%). Approximately, equivalent proportions of patients suffered with nocturnal awakenings (27.96%) and could not perform routine work in the preceding week (27.66%). Nearly a third or more of patients had to inhale rescue medication (67.78%), and 35.87% experienced daytime symptoms in the past week.
Discussion
The principal findings of this study are that the asthma burden remains in difficult-to-treat patients, despite the implementation of revised Caribbean guidelines. Close to half the patient population have uncontrolled asthma, and a disconnect is observed between actual and perceived evaluation of disease control. The landmark AIRE study 6,7,9 and successive worldwide surveys in adults and children consistently demonstrate the continuing asthma burden with control far below the goals of current international guidelines in all countries and regions wherever studied.
A 2009 Trinidadian study revealed uncontrolled asthma was 77.8% and 82.0%, using the Asthma Control TestTM (ACT) and the Royal College of Physicians’ (RCP) three questions test, respectively. 11 However, that report used the ACT and RCP evaluation, as validated tools to provide clear-cut numerical values guiding disease management to defined targets. These instruments do not distinguish between controlled and partially controlled disease, neither do they use the criteria of the GINA-based Caribbean guidelines employed in the current study. Guideline-based evaluation aligned with an expert consensus of control, offers a simple, understandable and valid instrument to assess asthma control on lung function and symptoms. Vermeulen et al. 12 reported GINA scoring showed the lowest percentage of controlled and the highest percentage of uncontrolled asthma when studying agreement between the GINA evaluation, the ACT, the RCP score, the Asthma Therapy Assessment Questionnaire and the Asthma Control Questionnaire. The Caribbean guidelines based on the GINA instrument are sensitive enough to evaluate controlled and uncontrolled asthma.
In the present study, uncontrolled asthma was 18.96% when perceived and 45.29% when assessed on the guidelines. Poor concordance between assessed and perceived disease control was observed earlier in Trinidad 11 and elsewhere. 13,14 Uncontrolled asthmatics who are unaware of their disease status are apt to delay reporting of symptoms and are at increased risk of exacerbations 15 making them more likely to make ED or unscheduled clinic visits. It is equally important for patients to realistically recognize their level of disease control, as it is for health professionals to not rely solely on patients’ perceptions so that appropriate and timely adjustment of therapy can be made. 16 Lack of asthma control is a predictor of future exacerbations that would sustain uncontrolled disease. 1 Disagreement between measured and perceived control puts patients at risk of being under-treated, suffering disease exacerbations, and influences self-management of asthma and attention to the warning signs of exacerbations.
We believe the rate of PEFR > 80% in 40.50% of subjects is most likely due to newer approaches in the chest clinics after the guidelines were implemented. There is an enhanced doctor-to-patient ratio, spirometry evaluation is scheduled at the patients’ first visit, and patient education has been introduced. Nonetheless asthma management remains suboptimally controlled in these clinics at which difficult-to-treat asthma patients are referred. These large clinics in the public health system function with limited resources, and the ideal access to peak flow meters and required technical assistance are not available. The clinics are situated in the most densely populated (87.45%) areas of the country (2011 Population and Housing Census Preliminary Count, Central Statistical Office, Ministry of Planning and the Economy, Republic of Trinidad and Tobago.) that have high attendance, are very crowded and where patient non-compliance for the scheduled three monthly follow-up visits is a frequent occurrence. Patients attending here are generally less educated, from a lower socio-economic stratum and often have to buy their own peak flow meters, which may explain why they do not have peak flow diaries nor use their action plans. Given the sizeable clinic attendance, the availability of a single spirometer and irregular technical assistance, routine spirometry is not an option, and this evaluation is often done by senior doctors using their personal instruments. Because guidelines serve as a standard of care subject to local limitations, they may not address the problems of developing countries, 17 such as the issues of availability of drugs, devices and resources, hence regular monitoring of outcomes with appropriate action is a step towards better asthma control.
Absolute and predicted PEF values were significantly lower in uncontrolled asthmatics. Olaguibel et al. 14 reported the mean forced expiratory volume in 1 second was significantly lower in uncontrolled patients compared with those with controlled or partially controlled disease. Co-morbidity, a predictor of uncontrolled asthma 18 and a confounder of asthma control, 19 was present in two-thirds of patients and significantly associated with uncontrolled asthma and reduced per cent predicted PEFR. Recognizing and addressing co-morbid conditions can avoid a burden on the patient and the health care system. We failed to find an association between obesity and asthma control, adding to literature with evidence both for and against an obesity–asthma morbidity link. Nevertheless, the significant association between obesity and poor asthma control observed in epidemiologic studies in adults and children 20,21 is an alert for the large proportion (44.2%) of our patients with a BMI ≥30 kg/m2 in whom asthma was uncontrolled. Asthma control, severity and response to therapy are negatively affected by overweight in both early and late onset obese asthmatics. 22 Clinicians should target weight loss for asthmatics with obesity.
A large proportion of patients believed they had to live with their asthma symptoms, despite being burdened by hospitalizations and visits to the ED. This belief encourages satisfaction with and low expectations of disease control and in fact is associated with high morbidity. 7,23 In the Living and Breathing Study, 23 when 58% of patients who were satisfied with the level of their asthma management were presented with what they should ideally expect from appropriate disease management in international guidelines, the proportion reduced to 33%. Patients believe frequent symptoms, exacerbations, limitation of routine activity and lifestyles are the expected outcome of having asthma and perceive they have controlled disease, even if they experience significant limitations in leisure and work activities. 24
Despite having seen a PEF meter, being instructed on inhaler technique and knowing the warning signs of an exacerbation, a paltry percentage of patients kept an asthma diary or checked lung function at home, an observation supported by other authors. 25
Limitations
As children were not included in the study, information on disease control in them is not available. The study was done in chest clinics and does not inform on asthma control in the community. Peak flow evaluations done by the researchers used the predicted values as an estimate of control in the absence of personal best. A previous study 11 of uncontrolled disease utilized tools that had different criteria from the guidelines, so that true comparisons cannot be made.
Conclusions
Subsequent to implementation of the revised Caribbean guidelines, asthma control in Trinidad’s chest clinics continues to be below optimal. A disconnect between patients’ knowledge and understanding of asthma was present, which suggests an increased focus on patient education should be put into practice. The challenge for caregivers is to reinforce and encourage adherence to the asthma management guidelines. Even though physicians may be aware of the guidelines, continuing medical education could lead to improved implementation. Through patient education initiatives, patients would be better able to understand their disease and its assessment and have realistic therapeutic expectations of their asthma. Frequent assessments of patient understanding, followed by relevant remedial measures are recommended.
Footnotes
Acknowledgements
Giovanni Maharaj, Karishma Davi and Jason Jogie assisted with data collection.
Authors’ Note
SB, DG, SB and AM performed the research study and did data entry. SS contributed to the study design and protocol and supervised data collection. TAS analyzed the data and assisted with manuscript preparation. LMPP designed the study, supervised the research and wrote the article. All authors read the final manuscript.
Conflict of interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.