
Abstract
Patients with chronic obstructive pulmonary disease (COPD) have extrapulmonary co-morbidities, such as cardiovascular disease, musculoskeletal wasting and neuropsychological conditions. To date, it remains unknown whether and to what extent COPD is associated with a higher prevalence of brain pathology. Therefore, the aim of this retrospective study was to compare the prevalence of neuropathological brain changes between deceased donors with and without COPD. Brain autopsy reports of age-matched donors with (n = 89) and without COPD (n = 89) from the Netherlands Brain Bank were assessed for demographics, cause of death, co-morbidities and brain pathology. The prevalence of degenerative brain changes was comparable for donors with and without COPD (50.6% vs. 61.8%, p > 0.05). Neoplastic brain changes were reported in a minority of the donors (5.6% vs. 10.1%, p > 0.05). After correction for cerebrovascular accident or cardiac cause of death and Charlson co-morbidity index score, the prevalence of vascular brain changes was higher among control versus COPD donors (27.0% vs. 11.2%, adjusted p = 0.013, odds ratio = 2.98). Brain autopsy reports of donors with and without COPD did not reveal differences in the presence of degenerative or neoplastic brain changes. Vascular brain changes were described more often in controls. Prospective studies including spirometry and structural and functional brain imaging should corroborate our findings.
Introduction
Chronic obstructive pulmonary disease (COPD) is characterized by chronic airflow limitation and extrapulmonary co-morbidities that may contribute to the severity of the disease. 1 Cardiovascular, musculoskeletal and also neuropsychological conditions are among the most prevalent extrapulmonary features. 2 Patients with COPD frequently have clinically significant, but often unrecognized, cognitive deficits, either globally or in specific cognitive domains. 3,4 Indeed, the incidence of cognitive impairment in patients with COPD varies in different studies from 12% to 88%. 5 Cognitive impairment is correlated with poor self-management skills, for example, improper use of medication, difficulties in dealing with co-morbidities and difficulty in handling guidelines. 6
Furthermore, neuropathologic changes may occur in COPD. It might be of great significance to map the presence of brain pathology since neuropathological brain changes may be a possible explanation for cognitive impairment in COPD. Studies using magnetic resonance imaging (MRI) suggested a relationship between COPD and neuropathological changes like reduction of regional grey matter volume, 7,8 reduced white matter integrity 7,9 and reduced hippocampal volume. 10 As pulmonary function deteriorates and the disease progresses, the risk of hypoxaemia and consequent hypoxia in the peripheral organs increases. 11 Consequently, decreased oxygen supply may cause neuronal damage in the brains of patients with COPD. 12 Frontal and parietal hypoperfusion 13 –15 and microstructural damage of white matter, such as severe periventricular white matter lesions might be correlated with cognitive impairment. 9,16 Indeed, Grant et al. showed a weak correlation between hypoxia and cognitive impairment in patients with COPD. 17 However, other authors did not find differences in brain structure between patients with COPD and controls using MRI and neurochemical imaging. 18
In order to unravel the discrepancy in the presence of brain pathology in patients with COPD, the aim of this study was to compare the prevalence of neuropathological brain changes between deceased patients with COPD and deceased controls without COPD, one-to-one matched for age, using brain autopsy reports. This study investigates the hypothesis that subjects with COPD have more brain pathology compared with subjects without COPD.
Methods
Study design
This retrospective cross-sectional, observational study has been conducted using the Netherlands Brain Bank (NBB; Netherlands Institute of Neuroscience, Amsterdam, the Netherlands). The NBB is a non-profit organization that collects human brain tissue of donors with a variety of neurological and psychiatric disorders and non-diseased donors. The brains of all subjects are neuropathologically investigated in a systematic way. In short, the brains were macroscopically examined and dissected depending on the clinical diagnosis and the actual applications of researchers. The brain tissue was either frozen or formalin fixed for 4 weeks. The formalin-fixed tissue was subdivided into cortex (frontal, temporal, parietal and occipital), hippocampus, locus coeruleus, substantia nigra, caudate nucleus, putamen, pallidum, insula, pons, cerebellum and medulla oblongata. These tissue specimens were embedded in paraffin, sectioned for histological or immunocytochemical stainings and used for microscopic examination by the pathologists of the NBB. 19
Study population
The computer program of the NBB selected 110 summaries of medical records of donors without dementia with a clinical diagnosis of COPD. Donors with Alzheimer’s disease, frontotemporal dementia, vascular dementia and other types of dementia were excluded. Other exclusion criteria were multiple sclerosis, Parkinson’s disease, progressive supranuclear palsy, schizophrenia and drug abuse. In total, 89 records (80.9%) had complete data on age, gender, cause of death and neuropathological information and were included in the current study. These were age matched with 89 summaries of medical records of donors without dementia and COPD. All patients provided pre-mortem consent for brain autopsy and use of brain material and clinical information for research purposes.
Outcome measures
The following outcomes were obtained from the medical records: gender, age at death, cause of death, co-morbid conditions and neuropathological information. Cause of death (respiratory insufficiency, cardiac, cancer, cerebrovascular accident, pneumonia and others) and co-morbid conditions (according to the Charlson Co-morbidity Index) 20 were scored independently by two researchers (FAHMC, master of science in mental health and DJAJ, elderly care physician). Consensual classifications were automatically accepted. The researchers discussed discrepancies case-by-case until a consensual agreement was reached. Neuropathological reports were systematically studied by a pathologist with extensive expertise in autopsy neuropathology (JB). All reports were classified into normal brain (no brain pathologies) or brain pathology. The following brain pathologies were scored: vascular brain changes, degenerative brain changes (age-related degeneration and/or neurodegeneration) and neoplastic brain changes (Table 1).
Brain pathologies.
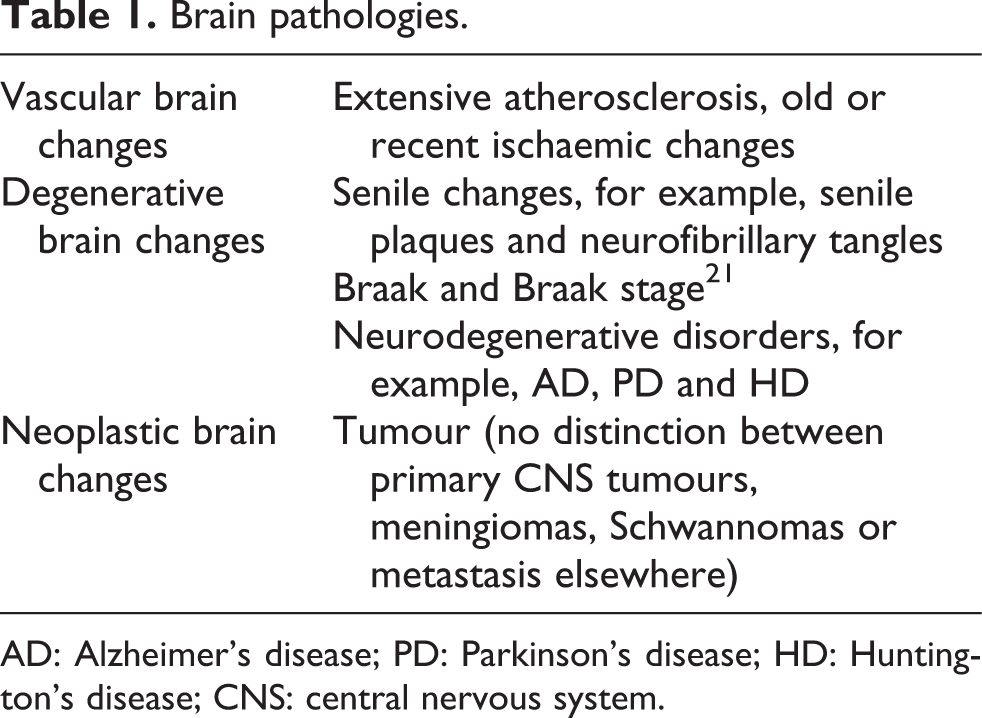
AD: Alzheimer’s disease; PD: Parkinson’s disease; HD: Huntington’s disease; CNS: central nervous system.
Statistics
Statistics were done using SPSS 17.0 (SPSS Inc., Chicago, Illinois, USA). Descriptive statistics were used to summarize the characteristics of the donors (age, gender, cause of death, co-morbidities and Charlson Co-morbidity Index score) and to present the various brain pathologies. Categorical variables are described as frequencies, whilst continuous variables were tested for normality and are presented as mean and standard deviation. Categorical variables were compared between donors with and without COPD using χ 2 tests. Continuous variables were compared between donors with and without COPD using an independent sample t-test. Binary logistic regression analysis was used to compare brain pathology between the two groups after correction for the following possible confounders that might be related with brain pathology: cardiac cause of death, cerebrovascular accident (CVA) as cause of death and Charlson Co-morbidity Index score. 22 –25 A priori, a two-sided level of significance has been set at p ≤ 0.05.
Results
The study cohort included 89 donors with COPD and 89 donors without COPD (Table 2). Respiratory insufficiency as cause of death was more prevalent in donors with COPD. Cancer and cardiac cause of death were more prevalent in control donors. The mean Charlson Co-morbidity Index score was significantly higher in COPD donors compared with the control donors.
Donor characteristics.a

COPD: chronic obstructive pulmonary disease; CVA: cerebrovascular accident; AIDS: acquired immune deficiency syndrome; HIV: human immunodeficiency virus.
aData reported as n (%) or mean (SD).
bIncluding for example septic syndrome, haematoma, haemorrhage and cachexia.
There was no difference in the prevalence of brain abnormalities between the donors with or without COPD (Table 3). The most frequently reported brain changes in both groups were degenerative changes, followed by vascular changes. Neoplastic brain changes were reported in a minority of the patients. Control donors had a higher prevalence of vascular brain changes. This remained significant after correction for a cardiac cause of death, CVA as cause of death and Charlson Co-morbidity Index.
Brain pathology.a

COPD: chronic obstructive pulmonary disease; CVA: cerebrovascular accident.
aData reported as n (%).
bBased on binary logistic regression analysis, adjusted for a cardiac cause of death, CVA as cause of death and Charlson Co-morbidity Index score.
Discussion
Key findings
The current retrospective study is the first to explore the presence of brain pathology in deceased donors with and without COPD. In both groups, only a minority had a normal brain. In contrast to our hypothesis, neuropathological brain changes did not occur more often in deceased donors with COPD. In fact, brain autopsy reports did not reveal a difference in the presence of degenerative or neoplastic brain changes between deceased donors with or without COPD. A statistically significant higher proportion of vascular brain changes was found among donors without COPD. However, the clinical relevance of this finding remains unknown.
The brain is a high oxygen-consuming organ, and although it constitutes only a small fraction (2.5%) of the total human body weight in adults, it accounts for about 20% of the body’s oxygen consumption. 26 A continuous oxygen supply is essential for proper functioning of the brain cells. 27 Earlier studies suggested that hypoxaemia may result in decreased oxygenation of the brain, 8 resulting in hypoxic stress. 26 Particularly during physical exercise, exacerbations and sleep, COPD patients were suggested to be at risk for prolonged periods of oxygen deprivation. 28 –30 Van Dijk et al. demonstrated that low oxygen saturation and COPD are associated with more severe white matter periventricular lesions, 16 independent of cardiac function, vascular risk factors and haemoglobin concentration, which might be related to reduced mental ability and reduced gait speed. 31 –33
As mentioned previously, other studies also showed structural brain abnormalities, for example, reduction of white matter integrity, grey matter and hippocampal volume, using MRI in patients with COPD. 7 –10 These pathologies are often been suggested to be induced by chronic hypoxaemia. In the study of Borson et al., however, no differences could be observed in brain structure between persons with COPD and controls using MRI. 18 Our study, using microscopical examination of brain tissue, confirmed the findings of Borson and colleagues. No significant difference in degenerative and neoplastic brain changes could be observed between both groups.
COPD patients might be protected against the ischaemic brain changes by increasing blood and oxygen supply to the brain. In fact, increased partial pressure of carbon dioxide and decreased partial pressure of oxygen lead to vasodilatation and increased cerebral blood flow. 34 Albayrak et al. demonstrated that total cerebral blood flow volume was increased in COPD patients due to vasodilatation of the bilateral internal carotid artery and vertebral artery, which are the main arteries supplying the brain. In a mouse brain study, during chronic hypoxia, significant vasodilation of the capillary diameter of intracortical microvasculature was observed, whilst the diameter of penetrating arterioles and emerging veins only demonstrated a tendency to enlarge. 35 This suggests that, within the brain, the capillaries are the main actors, which react to chronic hypoxia. Vogiatzis et al. showed that cerebral blood flow at the limit of exercise tolerance in COPD patients without resting hypoxaemia was maintained at significantly greater levels compared with resting conditions, whilst in healthy individuals cerebral blood flow declined towards baseline during exercise at the limit of tolerance. 36
Finally, hypoxia leads to lactate production. Previously, lactate was seen as a marker of brain hypoxia, and lactate was suggested to lead to toxicity of neuronal cells. However, a direct relationship between lactate and neuronal cell damage was not proved. 37 Moreover, Leverve suggested that lactate has a protective role rather than a detrimental role after brain ischemia. Indeed, lactate is used as an aerobic substrate used for cell recovery after hypoxia. 38 This may explain why this study did not show a relationship between brain changes and COPD.
Atherosclerosis is expected to be associated with smoking and COPD. 39 Several authors demonstrated increased intima-media thickness, an early phase of atherosclerosis, in COPD patients. In our study, more extensive atherosclerosis was found in the brain of control donors. However, the cause of this discrepancy is unknown. Future studies should explore this issue.
In analogy with cardiac ischaemic preconditioning, characterized by brief, repetitive periods of ischaemia reducing the size of a subsequent myocardial infarction, 40 COPD might also lead to brain ischaemic preconditioning. 41 Recently, Thompson et al. described that ischaemic brain preconditioning leads to an ischaemic-tolerant epigenetic profile. 42 Ischaemic preconditioning might also induce a reduction in the vascular changes like atherosclerosis or ischaemic lesions in the COPD brain as observed in this study. Biochemical and molecular biological techniques with fresh brain tissue samples that allow measurement of enzyme activity, (epi)genetic status and expression of cell death proteins, inflammatory cytokines and growth factors might be used in the future to further analyse brain differences between both groups.
The pathologies described in the autopsy reports such as age-related brain- and neurodegeneration and neoplastic brain changes are evenly distributed between the deceased COPD and control donors. These data suggest that COPD is not the main contributor in the onset of these brain pathologies.
Although evidence has been found for a relationship between neuropathologic alterations and cognitive impairment in COPD, 9,13 –16 the results of this study do not show a higher prevalence of neuropathologic brain changes in COPD. Other previously hypothesized etiologic factors for cognitive impairment in patients with COPD are smoking, inflammation, atherosclerosis and also decreased physical activity, exacerbations and co-morbid conditions such as obstructive sleep apnoea syndrome and major depressive disorders. Future studies should explore brain abnormalities using structural and functional brain MRI scans along with the investigation of cognitive functioning in patients with and without COPD.
Limitations
A first potential limitation is the retrospective nature of this study with pathological records only. Data collection was dependent on the availability and accuracy of the medical records. No information was available about the lung function, including severity of COPD (i.e. Global Initiative for Chronic Obstructive Lung Disease grading). Therefore, it was unknown whether and to what extent the diagnosis of COPD was confirmed by spirometry. Moreover, the amount of structural brain changes and areas affected in the brain were not consistently described in the medical records and therefore could not be explored in this study. Furthermore, the present study could not explore the causal relationship between impaired lung function and brain pathology. Also data about cognitive functioning, educational level, intelligence, sleep apnoea, smoking history, hypoxaemia, alcohol consumption, medication and long-term oxygen therapy were incomplete or unavailable. Because of the poor characterization of the COPD patients it was impossible to explore the relationship between COPD and the presence of structural brain changes after correction for clinical characteristics such as severity of airflow limitation or hypoxaemia. Second, the donor sample may have been distorted by selection bias, involving persons motivated to make their brain available for brain autopsy. These persons may not be generalizable to the whole population. 43 Furthermore, this may explain the deviated distribution of causes of death in this study sample compared with the previously described COPD literature. 44
Conclusions
The presence of brain pathologies did not differ between deceased persons with and without COPD. Interestingly, vascular brain changes were described more often in the brain autopsy reports of controls. However, the clinical relevance of this finding remains unknown. Longitudinal prospective studies should explore brain abnormalities using structural and functional brain MRI scans along with the investigation of pulmonary function and cognitive functioning in patients with COPD and age-matched controls without COPD.
Footnotes
Acknowledgements
The authors thank The Netherlands Brain Bank, Amsterdam, the Netherlands, for providing the medical records.
Conflict of interest
All authors of this article declare that there is no financial or moral conflict of interest that would bias the impartiality of this work
Funding
The research work was financially supported by a funding from The Weijerhorst Foundation, Maastricht, the Netherlands.