
Abstract
Lifestyle-induced weight loss studies in patients with obstructive sleep apnoea syndrome (OSAS) have revealed that at least 10% loss of their initial weight may correct or at least improve the symptoms of the syndrome. 1,2 Obese individuals are encouraged to lose 5–10% of their weight to improve OSAS but data supporting this recommendation are limited, particularly in moderate to severe cases. Whether a 5–10% weight loss range is more beneficial in moderate and/or severe OSAS compared with less weight loss (<5%) is the main focus of this study.
We present additional data from a previous study
3
after pooling the patients’ data and subdividing them into three categories according to the weight changes recorded at the 6-month follow-up: 0–4.9% (lowest), 5–9.9% (intermediate) and
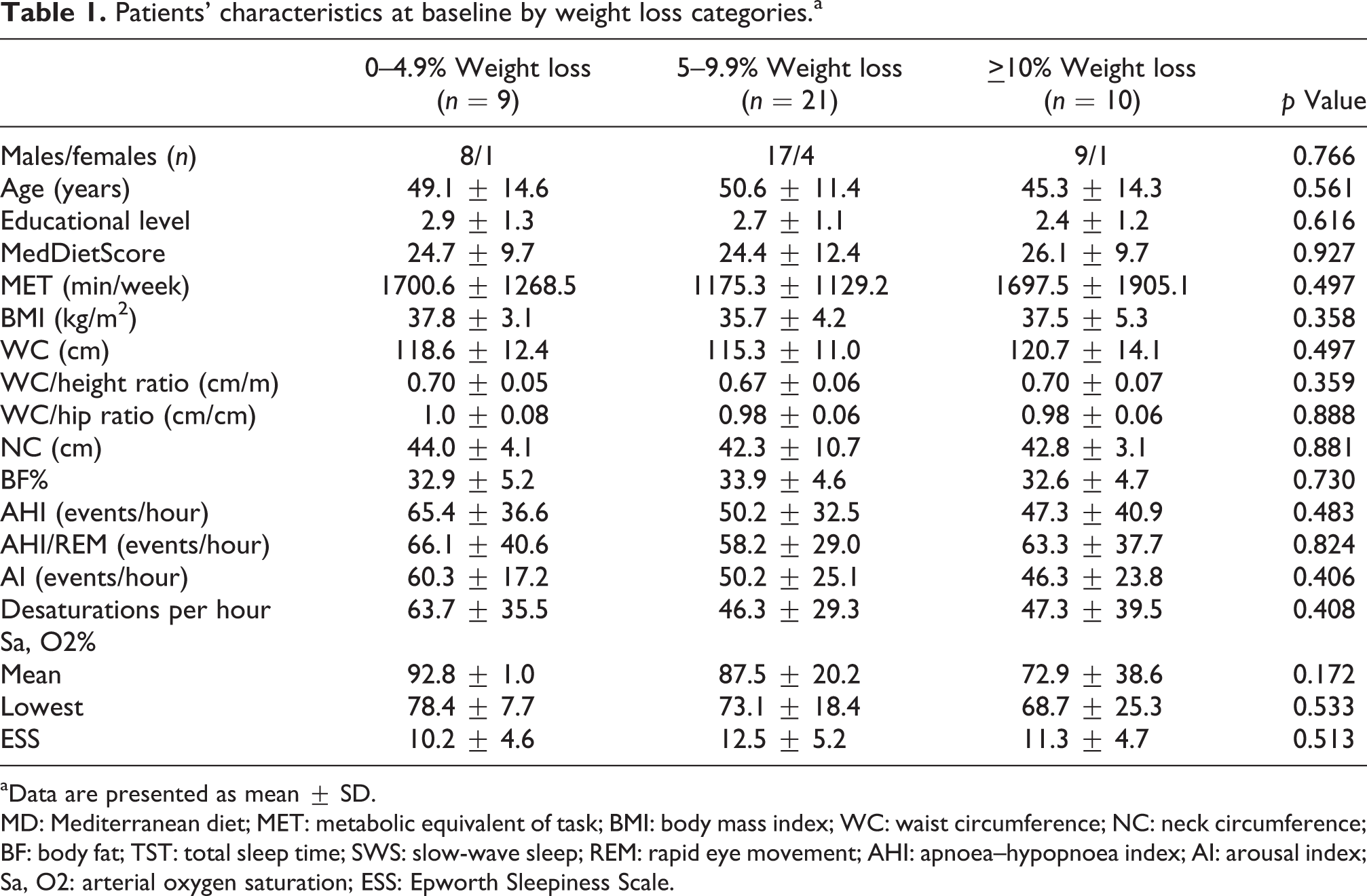
There were no significant differences (p > 0.05) among the weight loss categories concerning the baseline characteristics (Table 1). The highest category showed a greater improvement in apnoea-hypopnoea index during rapid eye movement (AHI/REM) and the lowest oxygen saturation compared with the lowest (p < 0.05; Table 2). The latter OSAS parameter also improved significantly more in the highest category than in the intermediate (p < 0.05). The comparison between the lowest and intermediate category did not reveal any significant differences concerning changes in OSAS severity indices (p > 0.05).
Patients’ characteristics at baseline by weight loss categories.a
aData are presented as mean ± SD.
MD: Mediterranean diet; MET: metabolic equivalent of task; BMI: body mass index; WC: waist circumference; NC: neck circumference; BF: body fat; TST: total sleep time; SWS: slow-wave sleep; REM: rapid eye movement; AHI: apnoea–hypopnoea index; AI: arousal index; Sa, O2: arterial oxygen saturation; ESS: Epworth Sleepiness Scale.
Comparison of changes in patient characteristics by weight loss categories.a
MD: Mediterranean diet; MET: metabolic equivalent of task; BMI: body mass index; WC: waist circumference; NC: neck circumference; BF: body fat; TST: total sleep time; SWS: slow-wave sleep; REM: rapid eye movement; AHI: apnoea–hypopnoea index; AI: arousal index; SaO2: arterial oxygen saturation; ANOVA: analysis of variance.
aData are presented as mean ± SD. The following parameters were log-transformed: DMedDietScore, DMET, DBMI, DWC/hip ratio, DAHI, Desaturations, and DSaO2% (mean, lowest).
b p Value derived from one-way ANOVA, using the Bonferroni rule to correct for type I error in the post-hoc multiple comparisons between weight groups (with the identical superscript lettersc, d, edenoting significant differences between groups).
c,d p Value < 0.05 “0–4.9% Weight loss” category vs. “5–9.9% Weight loss” category.
d,e p Value < 0.05 “5–9.9% Weight loss” category vs. “>10% Weight loss” category.
c,e p Value < 0.05 “0–4.9% Weight loss” category vs. “>10% Weight loss” category.
In the present study, the OSAS parameters with a remarkable difference in their change between different weight loss categories were AHI/REM and lowest arterial oxygen saturation. These are promising findings in OSAS treatment, because compared with non-rapid eye movement (REM) sleep, during REM sleep there is an increase in the duration of apnoea episodes 4 and the lowest oxygen saturation has been independently associated with several metabolic and inflammatory risks. 5
The significant difference in the change in AHI/REM between the lowest and highest category coexisted with notable differences in the change of waist circumference (WC) and WC/height ratio. Patients with the highest weight loss reduced AHI/REM more than the others possibly because of the greater reduction in abdominal fat and the associated mechanical load. 6,7 The differences between the aforementioned categories in body changes can be attributed to the adherence concerning prescribed diets and exercise programs. 8
Another finding of this study is that in the lowest category, an increase in apnoea-hypopnoea index (AHI) during REM sleep was recorded despite reductions in abdominal and body fat. Decreases in AHI following exercise training have been found to be independent of weight changes; 9 the inverse may have occurred in the current study, since AHI/REM increased in parallel with a decrease in physical activity level. A decrease in fatigue resistance of the diaphragm, 10 the main inspiratory muscle during REM sleep, caused by a reduction of physical activity, may explain these observations.
Regarding the notable increase in the lowest arterial oxygen saturation in the highest category compared with the lowest, this can be attributed to the significant difference in the change in AHI/REM and in the reduction of fat deposits around the abdomen possibly resulting in a greater improvement of rib cage expansion and thus of breathing during sleep. The latter mechanism could also explain the difference in the change in oxygen saturation between the intermediate and highest category.
The absence of any difference in the change of OSAS indices between the intermediate and lowest category indicates the quantitative effect of the diet/physical activity changes; there seems to be multiparametric threshold, limiting the effect of WC on the aforementioned OSAS indices. A lack of difference in the change of AHI/REM was also observed between the intermediate and highest category, despite the differences in the change in WC. Although it must be studied further, it may be that the changes in WC and WC/height ratio may have a greater effect on AHI/REM via a greater improvement in the associated mechanical load compared with the WC.