
Abstract
Eosinophilic asthma phenotype predicts good response to corticosteroids and associates to asthmatic exacerbations. Sputum induction by hypertonic saline (HS) inhalation is technically demanding. Bronchial hyperresponsiveness (BHR) to osmotic agents indirectly mirrors active airway inflammation. We compared the safety and ability of HS and mannitol to induce sputum and measure BHR. We evaluated the stability of inflammatory phenotypes. We studied 35 non-smoking asthmatics randomized to undergo HS and mannitol challenges on 2 days 1 week apart. Sputum was sampled for cell analysis and phenotyped as eosinophilic (≥3% eosinophils) and non-eosinophilic (<3%) asthma. Nineteen subjects had BHR to mannitol and nine of them also had BHR to HS. Drops in forced expiratory volume in 1 s were higher from HS challenge than from mannitol challenge. Adequate sputum samples were obtained from 80% subjects (68% mannitol and 71% HS). Eosinophils and macrophages from both challenges correlated. Neutrophils were higher in sputum from HS. Ninety percent samples were equally phenotyped with HS and mannitol. Fractional exhaled nitric oxide, sputum eosinophils and BHR correlated in both challenges. HS and mannitol showed similar capacity to produce valuable sputum samples. BHR to both osmotic stimuli partially resembled airway eosinophilic inflammation but mannitol was more sensitive than HS to assess BHR. Eosinophilic phenotype remained stable in most patients with both stimuli.
Introduction
Induced sputum (IS) technique by hypertonic saline (HS) inhalation has been widely validated. It allows us to identify airway inflammatory phenotypes and to detect patients who will (or will not) benefit from inhaled corticosteroids (ICS) 1 or from the novel antibody-based treatments. 2 Further, eosinophilic asthma phenotype is also related to a higher rate of asthma exacerbations. 3 However, IS is a demanding technical procedure that requires time, trained staff and patients’ collaboration, which precludes it from being widely used in clinical practice. Another practical limitation that derives from the use of HS is that the delivery of a wet aerosol via an ultrasonic nebulizer requires to be made at a lung function setting. Similar to other osmotic stimuli, HS eases expectoration by hydrating airway secretions. To prevent the bronchial narrowing that some subjects experience as a result of HS inhalation, patients are pretreated with albuterol before undergoing sputum induction.
The identification of bronchial hyperresponsiveness (BHR) to osmotic stimulus is consistent with active airway inflammation responsive to corticosteroids and mast cells stabilizing agents. 4 Dry powder mannitol, commercially available, provides a simpler and portable method of osmotic challenge. The safety and efficacy of mannitol and HS challenges to assess BHR 5 have shown similar results. However, mannitol has also demonstrated the ability to induce good-quality sputum samples. 6
In this study, we have tested the combined capacity of both HS and mannitol to simultaneously induce sputum and measure BHR in asthma patients not pretreated with albuterol. We have studied the safety of the technique, compared the results obtained with both challenge agents and tested the stability of the inflammatory phenotype from both challenges.
Methods
We recruited 35 adult, non-smoking and stable asthma patients who consecutively visited our Allergy Department. They were informed and gave written consent to participate in the study. The protocol had the approval of the review board of our hospital. Asthma diagnosis was made according to the Spanish Guidelines for Asthma Management. 7 During the last month, patients had not suffered from asthma exacerbations, respiratory infections and had not changed their anti-asthmatic medications.
On two separate days, patients underwent either the HS challenge or the mannitol challenge. Tests were performed 1 week apart and in random order. Before each visit, patients withheld their anti-asthmatic medications, for example, long-acting β2 agonist for 12 hours and short-acting β2 agonist for 6 hours. Prechallenge, fractional exhaled nitric oxide (FENO) by NIOX MINO® (Aerocrine AB, Sweden) and forced spirometry were performed. Every lung function test was performed with the same MasterScreen Pneumo spirometer (Jaeger, Germany) in accordance with the international guidelines 8 and reference values of Stanojevic et al. 9 Forced expiratory volume in 1 second (FEV1) values ≥70% predicted normal were required to start challenges. During each challenge, one sputum sample was also collected.
HS challenge and sputum collection
HS at 5% was administered with an ultrasonic nebulizer (ULTRA-NEB 2000; DeVilbiss, Somerset, Pennsylvania, USA) adapted to a two-way valve (Hans-Rudolph, inc., Shawnee, Kansas, USA) as described. 10 HS was administered in increasing time periods of 0.5, 1, 2, 4 and 8 minutes (total inhalation time: 15.5 minutes). After each inhalation period, patients were asked to cough and expectorate if possible. Spirometry was made at baseline and 1 minute after each inhalation period. The test was stopped when a drop in FEV1 ≥ 15% from baseline was recorded or the last inhalation period was completed.
The greatest FEV1 fall from baseline was recorded and the slope of the dose–response (DRS) curve calculated by dividing the %fall in FEV1 by the amount of HS inhaled (HS-DRS). 10
Mannitol challenge and sputum collection
Dry powder mannitol was administered as recommended (Osmohaler, Aldo-Unión, Barcelona, Spain). Firstly, an empty capsule was inhaled and FEV1 was measured. FEV1 change ≤5% from baseline was required to start the test. Mannitol at 5, 10, 20, 40, 80, 160, 160 and 160 mg was administered. After each inhalation, patients were asked to cough and expectorate if possible. Three minutes after each capsule inhalation, FEV1 was recorded. The test was completed when a drop in FEV1 ≥ 15% from baseline was recorded or the total mannitol cumulative dose (635 mg) was given.
The PC15 mannitol was defined as the concentration of mannitol that induced a FEV1 fall of 15%. The mannitol DRS was calculated by dividing the %fall in FEV1 by the cumulative dose of mannitol inhaled. We used the DRS to HS and mannitol to compare both challenge tests.
Sputum analysis
Sputum samples, obtained from HS and mannitol, were processed as described 11,12 and blindly evaluated. Samples were deemed adequate for cytological analysis when macrophages were observed and squamous cell contamination was under 20%. Percentage counts of macrophages, eosinophils, neutrophils, mast cells and lymphocytes were made over a total count of 400 cells.
Statistical analysis
Patients were phenotyped according to sputum inflammatory cells as eosinophilic (≥3% eosinophils), neutrophilic (≥60% neutrophils), mixed (≥3% eosinophils and ≥60% neutrophils) and paucigranulocytic (<3% eosinophils and <60% neutrophils). 13 Patients with ≥3% sputum eosinophils were further grouped as eosinophilic asthma.
Statistical Package for the Social Sciences programme was used. Phenotype classifications between HS and mannitol sputum induction were analysed by the chi-square test. The Mann–Whitney test was used to compare differences between the HS and the mannitol results regarding sputum cell counts and lung function. Paired analysis of cases grouped according to the use or not of ICS was studied by Wilcoxon’s rank test. The Spearman correlation rank coefficient was used. p < 0.05 was considered significant.
Results
All patients completed HS challenge and mannitol challenge tests. Their features are shown in Table 1.
Demographic characteristics from patients in the global sample and according to their capacity to produce (sputum+) or not (sputum−) an adequate sputum sample.

ns: not significant; ICS: inhaled corticosteroid; FEV1: forced expiratory volume in 1 second; FENO: fractional exhaled nitric oxide: IQR: interquartile rate.
aResults are expressed as median and IQR.
Safety and BHR assessment
Positive challenges were recorded in 9 (25%) subjects from HS and in 19 (54%) from mannitol. All patients who reacted to HS also reacted to mannitol. Whilst both tests were well tolerated, cough-induced mannitol caused more subjective discomfort (data not provided). The airway narrowing that was induced with both agents was easily reverted with albuterol. Challenge-induced falls in FEV1 ≥25% happened in two subjects, namely, one from HS (36%) and the other one from mannitol (27%). HS challenge median FEV1 fall was lower than mannitol challenge median FEV1 fall (5.5% [interquartile rate (IQR): 4.0–18.0] vs. 16.5% [16–19.3], p = 0.025). When paired results for patients who reacted to both mannitol and HS were compared, the maximal fall in FEV1 values was greater in HS challenge (20.5% [18.9–22.0]) than in mannitol challenge (19.3% [15.5–20.0], p = 0.01).
HS challenge and mannitol challenge correlated in both FEV1 maximal fall and DRS (Figure 1).

Correlations between HS challenge and mannitol challenge in terms of maximum FEV1 fall (a) and DRS curve (b). HS: hypertonic saline: FEV1: forced expiratory volume in 1 second; DRS: dose–response slope.
Sputum cytological characteristics
Adequate IS samples were obtained from 25 (71%) patients during HS challenge and from 23 (68%) during mannitol challenge. Adequate sputum samples with both stimuli were obtained from 20 (57%) patients. In 7 (20%) subjects, it was not possible to obtain good sputum samples with either the HS or mannitol stimuli. There were no differences between patients regarding the collection of adequate sputum samples, although a trend towards higher atopy and ICS use was observed among those who produced adequate sputum samples (Table 1).
Table 2 shows differential cell counts of sputum samples obtained from HS and mannitol. Neutrophil percentages were significantly higher in sputum from HS. We observed correlation between HS- and mannitol challenge eosinophils and macrophages (Figure 2) but not neutrophils or non-squamous total cell numbers.
Cellular components of the sputum samples obtained from HS and mannitol.a
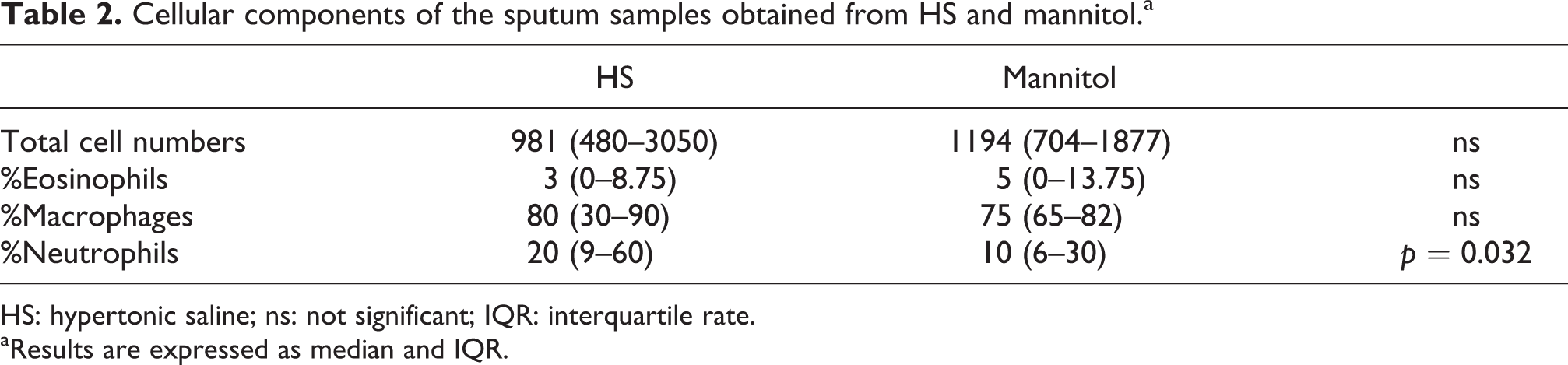
HS: hypertonic saline; ns: not significant; IQR: interquartile rate.
aResults are expressed as median and IQR.

Correlations between samples obtained with HS and with mannitol: eosinophils (a) and macrophages (b). HS: hypertonic saline.
We recorded eosinophilic phenotype in 14 (56%) samples from HS challenge and 15 (65%) from mannitol challenge, mixed phenotype in 5 (20%) and 1 (4.3%) samples and paucigranulocytic phenotype in 5 (20%) and 7 (30.4%) samples, respectively. Only one (4%) neutrophilic phenotype was observed and it occurred in the HS challenge. The chi-square test for independent variables applied to asthma phenotypes obtained with HS and mannitol was significant (p < 0.001).
No changes in the inflammatory phenotype were observed in 13 out of the 20 (65%) patients with whom adequate sputum samples were obtained in both HS and mannitol (8 eosinophilic and 5 paucigranulocytic). Of the remaining seven paired cases, five mixed phenotypes from HS challenge shifted to eosinophilic pattern from mannitol. One paucigranulocytic pattern and one eosinophilic pattern from HS challenge, respectively, shifted to mixed and paucigranulocytic phenotypes from mannitol challenge. When grouped just as eosinophilic or non-eosinophilic asthma, the phenotype remained stable in 90% of the patients.
Correlations between BHR and inflammatory markers as assessed by both, HS and mannitol challenges Correlations between FENO, cytological analysis and BHR from HS challenge:
FENO correlated to baseline FEV1 (p = 0.007, r = 0.45), DRS curve (p = 0.048, r = 0.27), HS-induced maximal FEV1 fall (p = 0.013, r = 0.33) and sputum eosinophils (p = 0.002, r = 0.38). The fall in FEV1 values correlated to sputum total cell numbers (p = 0.007, r = 0.59).
Among eosinophilic asthma patients, the fall in FEV1 correlated with eosinophil percentage (p = 0.045, r = 0.46). Such association disappeared in non-eosinophilic asthma, where the fall in FEV1 correlated to neutrophils (p < 0.001, r = 0.58). Correlations between FENO, cytological analysis and BHR from mannitol challenge:
FENO correlated to DRS curve (p < 0.001, r = 0.47), PC15 (p = 0.014, r = −0.39), mannitol-induced maximal FEV1 fall (p = 0.001, r = 0.58) and sputum eosinophils (p < 0.001, r = 0.51).
Mannitol-PC15 values inversely correlated to sputum eosinophils (Figure 3) and remained in eosinophilic asthma (p = 0.025, r = −0.60) and non-eosinophilic asthma (p < 0.001, r = −0.84).

Correlation mannitol-PC15 values and eosinophils in sputum from mannitol.
Discussion
It is becoming evident that asthma is a polyhedral disease presented as different phenotypes of therapeutic response. Among them, eosinophilic phenotype (sputum eosinophils ≥3%) is considered a marker of good response to ICS 1 and antibody-based therapies. 2 Further, eosinophilic asthma patients are more likely to suffer from asthma exacerbations. 3 Therefore, sputum analysis should be taken into account in the evaluation of patients with asthma-like symptoms, especially before indicating anti-inflammatory, long-lasting or immuno-modulator treatments. However, this is not always possible due to the demanding features of the technique, some of them derived from the delivery system of the HS solution and also from the fact that not every subject is able to produce good quality sputum samples. Good correlations have been observed between sputum eosinophils and FENO but the adoption of cut-off points of FENO values corresponding to 3% sputum eosinophilia is troublesome. 14 In our respiratory laboratory, FENO <21 ppb very likely ruled out sputum eosinophilia among ICS naive patients. However, the negative predictive value of such cut-off value was dramatically reduced when patients on ICS were evaluated. 15
We compared the ability of both HS and mannitol challenge to produce sputum and measure BHR. As reported, 5 although patients were not pretreated with β-agonists, both challenges were well tolerated. Two subjects had fall in FEV1 values greater than 25% (36% with HS and 27% with mannitol) that were rapidly reverted by albuterol inhalation. In contrast to the similar response rates reported, 5,6 in our study, mannitol challenge had a higher sensitivity than HS challenge to detect BHR. Moreover, all patients with BHR to HS also responded to mannitol. It might be thought that asthma stability required in our study and the different level of respiratory tract deposition for each osmotic stimulus might account for that. Nevertheless, we observed a good degree of relationship between lung functional markers from HS and mannitol challenges giving internal consistency to both tests.
The capacity of HS and mannitol to induce sputum showed similar results and the quality of the samples given by eosinophil and macrophage rates showed good correlation. We observed a trend towards higher non-squamous total cells in samples from mannitol and significantly more neutrophils in samples from HS. Wood et al. 6 also observed higher neutrophil rates, although not statistically significant, in sputum from HS. They attributed such differences to the differential composition of IS according to the duration of the inhalation technique. 16 In sequential sputum sample analysis, earlier samples exhibited higher eosinophil and neutrophil rates whereas later samples exhibited higher macrophage rates. Authors concluded that such differences could be due to the different airway compartments sampled, for example, proximal airways rich in eosinophils and neutrophils would be sampled during the first minutes and smaller airways rich in macrophages would be sampled after 12 minutes of inhalation. 16 We conclude that the greater neutrophil rates observed in our study are not likely due to the inhalation time since most patients needed the maximum HS-nebulization time (15.5 minutes). Alternatively, it is possible that mannitol is sampling more peripheral airways than HS, since the size particle of mannitol dry powder is <3.6 µm whereas HS was delivered by an ultrasonic nebulizer at high output. This fact could explain a more proximal deposition of HS and, consequently, the higher neutrophil counts from HS challenge.
Clinical relevance of sputum cell analysis mainly lies in identifying the asthma phenotype that allows for predicting the individualized therapeutic response. We required asthma stability, at the baseline and between challenges that were conducted 1 week apart. The inflammatory phenotype assessed by both challenges was consistent in 65% of the cases. However, changes were mainly due to the higher neutrophil percentages observed in sputum from HS compared with sputum from mannitol. Furthermore, five out of the seven changes in inflammatory phenotypes were eosinophilic patterns from mannitol that shifted to mixed phenotypes from HS. Therefore, mannitol and HS agreed in classifying asthma as eosinophilic or non-eosinophilic in 90% of the subjects.
It is thought that BHR to osmotic agents mirrors active bronchial inflammation and, thus, indirectly supports sputum cytology. 4 This feature can be interesting in cases where it is not possible to obtain adequate sputum samples (in our study, it happened in 20% of the patients). Moreover, we observed an inverse relationship between mannitol-PC15 values and sputum eosinophilia that was kept when patients were grouped according their eosinophilic phenotype. Correlations were weaker or inconsistent among sputum eosinophilia and HS challenge. This can be explained because the scarce number of subjects that had a positive response to HS challenge did not allow to express results in terms of HS-PC15 values. Moreover, most patients underwent the maximum HS-nebulization time (15.5 minutes), which also hampered the discriminative capacity of HS-DRS values.
To resume, in our study, mannitol and HS behave similarly at sputum induction, but mannitol has higher sensitivity to detect BHR and better correlates to sputum eosinophilia. Moreover, mannitol, commercially available as dry powder, solves some of the technical problems of HS-sputum induction. As it only requires spirometry, it can be performed outside of clinical settings. Further it allows an easier quantification of response in terms of PC15 that allows comparison of sequential challenges, intra- or inter-subject. It might also provide indirect information about airway eosinophilic inflammation, particularly useful in subjects from whom it is not possible to obtain a quality sputum sample. It is worthy to emphasize that in most patients the eosinophilic phenotype determined by sputum remained stable for at least 1 week even when different osmotic stimuli were utilized.
Footnotes
Conflict of interest
The authors declared no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.