
Abstract
Inherited neuromuscular disorders inevitably result in severe lung volume restriction associated with high morbidity and mortality. The aim of this retrospective study was to evaluate the long-term effects of the regular use of mechanical insufflation/exsufflation on the course of the vital capacity. This retrospective data analysis included 21 patients (16.1 ± 6.5 years) with neuromuscular disorders and severe lung volume restriction using nocturnal noninvasive ventilation. The patients were advised to regularly use the mechanical insufflation/exsufflation twice a day for 10 minutes applying sets of three insufflation/exsufflation breath via face mask irrespective of respiratory tract infection. Data on the course of vital capacity were collected 2 years prior and 2 years after the introduction of regular use of mechanical insufflation/exsufflation. Before the introduction of mechanical insufflation/exsufflation vital capacity decreased from 0.71 ± 0.38 L to 0.50 ± 0.24 L in the last year and from 0.88 ± 0.45 L to 0.71 ± 0.38 L in the next to last year. In the first year, after regular use of mechanical insufflation/exsufflation vital capacity significantly increased by 28% (from 0.50 L to 0.64 L)—after the second year the vital capacity increase remained stable (0.64 vs. 0.65 L). These data suggest that the regular use of mechanical insufflation/exsufflation improves vital capacity in patients with neuromuscular disorders and severe lung volume restriction.
Introduction
Respiratory muscles are commonly affected in inherited neuromuscular disorders (NMD). Respiratory muscle involvement results in muscular atrophy and muscular contractures with the consequence of limited movement of the thoracic cage. This progressive thoracic restriction causes a continuous decrease of vital capacity (VC). 1 The degree of lung volume restriction is the strongest predictor of mortality in NMD patients. 2 Besides this inspiratory muscle failure, progressive loss of lung volume and weakness of expiratory muscles result in cough insufficiency leading to impaired clearance of airway secretions, recurrent respiratory tract infection, and atelectasis. 3 Efficacy of cough is measured by cough peak flow (CPF) and considered to be insufficient below 270 L/min. Cough flows can be increased by mechanical insufflation techniques or by mechanical insufflation/exsufflation (MI-E). The introduction of a structured proactive management plan including the use of noninvasive ventilation (NIV) and assisted coughing techniques reduces morbidity and mortality of NMD patients. 1,3 –5
There is a small set of methods that might help to increase VC. Inspiratory muscle training is able to increase VC for a limited time. 6 However, up to date, there are no data supporting that physical training may influence the long-term loss of vital capacity in patients with NMD. 7 A recent study showed that for 22 patients with advanced Duchenne muscular dystrophy (DMD), regular use of a lung recruitment maneuver by air stacking via resuscitation bag is able to reduce annual decline of VC from 4.7% to 0.5% predicted. 8 The British Thoracic Society guidelines recommend the application of volume recruitment and deep lung insufflation techniques when the VC falls below 40% predicted, 9 but there are no data or clear recommendation whether the deep lung insufflation techniques should be used only to augment insufficient cough in situations with increased pulmonary secretions or additionally in the infection-free interval serving as internal physiotherapy. The addition of the mechanical exsufflation to a deep lung insufflation in the MI-E might further improve the mobility of the stiff thorax and help to clear retained airway secretions that reduce lung compliance. Therefore, we retrospectively analyzed whether the regular use of MI-E twice a day in the infection-free interval is able to slow down the annual decline of VC or even improve VC in patients with severe lung volume restriction.
Materials and methods
This retrospective data analysis was carried out on the basis of records of patients treated in the Departments of Pediatric Pulmonology and Pediatric Neurology of the University Hospital Essen in Germany. We included all patients that were put on or changed to MI-E between September 2009 and October 2012. All patients had severe lung volume restriction (VC <30% predicted), severe cough insufficiency with CPF < 160 L/minute and used nocturnal NIV. Of the 21 patients, 16 insufficiently used intermittent positive pressure breathing (IPPB) for mechanical assisted cough, 10 and five patients were naive to mechanical assisted cough. None of the patients needed intermittent suctioning or used bronchodilators/asthma medications routinely. No other systematic changes in the management (e.g. prophylactic antibiotics and improved nutrition) were initiated during the study period. None of the patients suffered from respiratory tract infection when spirometry was performed.
Severe cough insufficiency was defined as CPF < 160 L/minute in children older than 12 years. The threshold value for younger children might be lower as the standard values for CPF are lower in younger children. 11 Since 2010, all patients with severe cough insufficiency were trained using MI-E (Cough Assist, Phillips Respironics, Murryville, USA or NIPPY Clearway, B&D Electromedical, Statford-Upon-Avon, UK) with an individual determined inspiratory pressure (25.1 ± 5.3 (18–40) cmH2O) and expiratory pressure (−25.6 ± 5.7 (from −20 to −40) cmH2O). Unpublished data from our group show that the application of inspiratory pressures around 30 mbar results in the best increase of the insufflated volume and CPF. However, in this patient group, the settings of MI-E were established by patient comfort. The MI-E was applied using a face mask. All patients were advised to use MI-E twice a day for 10 minutes applying sets of three insufflation/exsufflations breaths to improve airway clearance independent of respiratory tract infection. This is similar to the published approach of four sets of five breaths in the respiratory management of spinal muscular atrophy. 12 All patients reported good adherence to the regular use of MI-E.
The VC was measured in the sitting patient wearing a noseclip with a handheld spirometer (ZAN 100, ZAN Meßgeräte, Obertulba, Germany) according to the American Thoracic Society criteria. 13 We retrospectively analyzed the course of VC 1 and 2 years before and after the introduction of MI-E, respectively. For each individual patient at least one pre-MI-E and one post-MI-E introduction data set was available.
The ethics committee of the University of Duisburg-Essen approved this retrospective data analysis.
Statistical analysis was performed using version 20 of the Statistical Package for Social Sciences statistics package (SPSS Inc., Chicago, Illinois, USA). Data are presented as mean and standard deviation. Comparisons between the time points were done using the paired t test. Longitudinal data were analyzed four times (between five separate time points). Therefore, we employed the Bonferroni adjustment for multiple testing and set the significance level to p < 0.05/4 = p < 0.0125.
Results
Between September 2009 and October 2012, 21 patients (DMD, spinal muscular atrophy, congenital myopathy without diaphragm weakness, and congenital muscular dystrophy with diaphragm weakness) started regular MI-E therapy as they showed progressive cough insufficiency and/or insufficient deep lung insufflation techniques. Patient characteristics starting with MI-E are presented in Table 1.
Patient characteristics.a

VC: vital capacity; M-I/E: mechanical insufflator/exsufflator.
aResults are presented as mean ± SD (range).
As pure lung volume restriction in the different NMD is similar, initially we analyzed all patients together. In the year before the introduction of MI-E, VC declined from 0.71 ± 0.38 L to 0.50 ± 0.24 L (p = 0.057) and from 0.88 ± 0.45 L to 0.71 ± 0.38 L (p = 0.02) in the next to last year. In the first year, after initiation of MI-E, VC significantly increased (0.50 L vs. 0.64 L, p = 0.002), which is an average relative increase by 28%. The VC increased in 18/21 patients, only three patients showed a small decline of VC (Figure 1). After the second year of regular use, this effect remained stable with a little further increase of VC from 0.64 to 0.65 L (Figure 1 and Table 2), which results from data of only six patients.
Course of VC before and after the initiation of mechanical insufflation/exsufflation.a

VC: vital capacity; M-I/E: mechanical insufflator/exsufflator.
aResults are presented as mean ± SD (range).
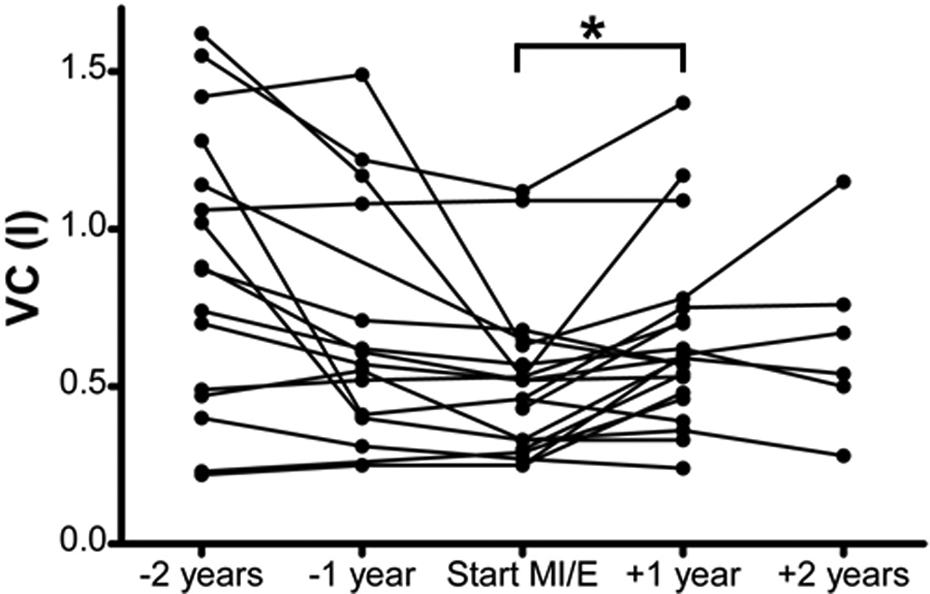
Course of VC before and after the initiation of mechanical insufflation/exsufflation. VC: vital capacity; M-I/E: mechanical insufflator/exsufflator.
Subgroup analysis of the VC course before and after the introduction of MI-E in the groups DMD, spinal muscular atrophy, congenital myopathy without diaphragm weakness, and congenital muscular dystrophy with diaphragm weakness showed no significant change of VC after regular use of MI-E was initiated. However, all groups showed tendencies toward an improvement of VC one year after MI-E therapy was started. In DMD, VC increased from 0.48 ± 0.15 L to 0.59 ± 0.25 L, in spinal muscular atrophy, VC increased from 0.34 ± 0.13 L to 0.52 ± 0.20 L, in congenital myopathy without diaphragm weakness, VC increased from 0.54 ± 0.39 L to 0.79 ± 0.43 L and in congenital muscular dystrophy with diaphragm weakness VC increased from 0.62 ± 0.33 L to 0.71 ± 0.26 L.
Discussion
We report for the first time on the improvement of VC in patients with advanced NMD after the introduction of the regular use of MI-E independent of respiratory tract infection. The increase of VC was obvious in all subgroups analyzed (DMD, spinal muscular atrophy, congenital myopathy without diaphragm weakness, and congenital muscular dystrophy with diaphragm weakness), however, did not reach statistical significance within limited subgroups.
Importantly, the individually determined inspiratory and expiratory pressures applied by MI-E in our study were significantly lower than the recommendations for other groups 14 and no side effects were observed. Current guidelines recommend the use of MI-E to improve clearance of airway secretions, but recommendations with respect to frequency or intensity are not given. 1,9 Thus, most patients use their MI-E mainly in situations of respiratory tract infections. We advised our patients with insufficient cough and severe lung volume restriction to use MI-E at least twice a day for 10 minutes irrespective of the presence of respiratory tract infection. Two factors might contribute to the 28% increase of VC in our cohort of NMD patients:
First MI-E serves as “internal” physiotherapy releasing contractures and adhesions of the thoracic cage in accordance to the therapy of limb contractures. 15 Second especially the mechanical exsufflation in the MI-E maneuver might clear microatelectasis and augment reduced lung compliance reported to be present in NMD with severe lung volume restriction. 16,17 The release of microatelectasis might be especially due to the mobilization of airway secretions by the application of exsufflation. A recent report showed that deep lung insufflation maneuvers improve ventilation inhomogeneity in patients with NMD, 18 supporting the hypothesis that MI-E improves lung compliance and microatelectasis. Especially microatelectasis and reduced lung compliance might be more susceptible to MI-E than deep lung insufflation alone, resulting in an increase of VC by 28% in our cohort compared to the reduction of VC decline (0.5% vs. 4.7% predicted per year) using deep lung insufflation alone presented by McKim et al. 8 Furthermore, in the McKim et al. study, the VC at the initiation of deep lung insufflation was twice higher than the VC in our DMD cohort. There are some data showing that the VC is not significantly influenced by a single session of MI-E. 19,20 Thus the increase of VC presented in our study is a long-term effect, supporting the hypothesis that the release of thoracic cage contractures might be the main factor for the improvement of VC. Unfortunately, we did not measure VC or other physiologic parameters closer than 3 months after the introduction of the regular twice daily use of the MI-E.
Limitations of the study
The presented data result from a retrospective study, where data set in parts are incomplete. Finally, we are not able to differentiate whether the increase of VC in our cohort is the result of the deep lung insufflation (within the MI-E maneuver) alone or really due to the addition of the exsufflation maneuver with the MI-E. However, all patients using deep lung insufflation techniques prior entering this study used the IPPB technique only to improve cough during respiratory tract infections. In 2009, we started advising patients to use hyperinsufflation or MI-E regularly twice daily.
Conclusion
Here we report for the first time that an intervention slows down the decline and even improves VC in patients with NMD. It is known so far that the continuous use of NIV and MI-E reduces hospitalizations 21 and mortality 5 in DMD patients. This effect might at least partly be due to an increase or stabilization of the VC decline. If the regular use of MI-E in earlier stages of NMD resulting in severe lung volume restriction has positive effects regarding mortality, morbidity, or quality of life, it remains to be determined in prospective trials.
Footnotes
Conflict of interest
The authors declared no conflicts of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.