
Abstract
In a sample of adults with asthma receiving care and medication in an outpatient pulmonary clinic, this study tested for statistical associations between social problem-solving styles, asthma control, and asthma-related quality of life. These variables were measured cross sectionally as a first step toward more systematic application of social problem-solving frameworks in asthma self-management training. Recruitment occurred during pulmonology clinic service hours. Forty-four adults with physician-confirmed diagnosis of asthma provided data including age, gender, height, weight, race, income, and comorbid conditions. The Asthma Control Questionnaire, the Mini Asthma Quality of Life Questionnaire (Short Form), and peak expiratory force measures offered multiple views of asthma health at the time of the study. Maladaptive coping (impulsive and careless problem-solving styles) based on transactional stress models of health were assessed with the Social Problem-Solving Inventory-Revised: Short Form. Controlling for variance associated with gender, age, and income, individuals reporting higher impulsive–careless scores exhibited significantly lower scores on asthma control (β = 0.70, p = 0.001, confidence interval (CI) [0.37–1.04]) and lower asthma-related quality of life (β = 0.79, p = 0.017, CI [0.15–1.42]). These findings suggest that specific maladaptive problem-solving styles may uniquely contribute to asthma health burdens. Because problem-solving coping strategies are both measureable and teachable, behavioral interventions aimed at facilitating adaptive coping and problem solving could positively affect patient’s asthma management and quality of life.
Introduction
Asthma is a largely uncontrolled chronic health condition with considerable financial, medical, and social burdens. Current public health estimates suggest that about 300 million people currently have asthma worldwide, and experts raise concern about the growing prevalence of asthma in the developing world. 1 From 2001 to 2009, asthma prevalence in the United States increased by 12.3%. 2 A considerable amount of research aimed at patient self-management skills has followed. Many clinics offer education about the nature of asthma and medication adherence training. Despite the efforts to enhance asthma education with nutrition and diet, 3,4 meditation and relaxation, 5 biofeedback, 6 and additional educational components, 7 most studies of complementary asthma programs show little to no benefit 7 and some negatively impacted asthma outcomes. 6,7 To bridge the gap between poorly and well-controlled asthma, others have implemented problem-solving components to intervention programs. 8,9 These programs assert that asthma-related behaviors such as taking medication daily, or carrying an inhaler, can be viewed as a stressor that could undermine effective asthma management.
Based on transactional stress models, 10 social problem-solving models are used to describe and teach the self-directed process of identifying and developing adaptive coping strategies for problems individuals may encounter in their daily life. More specifically, these models reflect the process whereby people direct their coping efforts at altering: (a) the nature of the situation such that it no longer represents a problem, (b) their maladaptive reactions to such problems, or (c) both the situation and the maladaptive coping response to the problem. 11 Rather than representing a singular type of coping behavior or activity, social problem solving is conceived as the multidimensional “meta-process” needed to effectively address the particular, and potentially unique, features of a given stressful situation. These processes include an individual’s tendency to react to problems with a positive or negative problem-solving orientation as well as engage in planned and rational or maladaptive coping strategies that involve impulsiveness–carelessness and avoidance behaviors. 11
The social problem-solving theoretical framework has predicted health status and psychological outcomes in terms of anxiety, 12,13 depression, 14 –16 psychological distress, 17 back pain, 18 cardiovascular health, and other chronic conditions. 19,20 It has also been useful in creating and informing new behavioral therapies such as “behavioral cardiology” that seek to reduce the patient’s risk for negative health outcomes by improving their ability to cope with stressful emotions and challenges. Now in the third-edition, Problem-Solving Therapy lays out a positive psychology and stress and coping approach to enhance adaptive coping as a way to avert exacerbations in chronic diseases. 11 However, social problem-solving psychometric measures based on the models described by Nezu et al. 11 have not been extensively applied to patients with asthma.
“Asthma control” is considered to be the most important measure of asthma health. 21 Well-controlled asthma is characterized by the minimization of symptoms, less bronchoconstriction, and minimal or no use of rescue medication. Asthma control is not an index of disease severity, but instead a measure of the most clinically relevant aspects of asthma control mentioned above. While asthma control is important, asthma-related quality of life, which represents the physical, emotional, environmental, occupational, and social effects resulting from asthma, is also relevant to health and well-being. 22 Previous research has shown that asthma control and asthma-related quality of life are somewhat independent constructs. 23 In other words, despite mild disease severity, some patients have a greatly reduced quality of life. It may be the case that asthma control and asthma-related quality of life are differentially related to social problem solving. Obtaining data on both measures of asthma health allow for analyses capable of discerning these sorts of effects.
This study examined possible statistical associations between social problem solving and individual’s asthma control and asthma-related quality of life as a first step toward a potential intervention component focused on improving the social problem solving of the patient. For this study, it was hypothesized that asthma medication-prescribed patients who reported engaging in more maladaptive social problem solving would also exhibit poorer asthma control and asthma-related quality of life.
Methods
Drexel University’s Office of Research Non-Medical and Medical Internal Review Boards approved all procedures (#1110000291). Potential participants were adults aged 18 and above, who previously received a primary diagnosis of asthma and were receiving care at Hahnemann University Hospital’s Division of Pulmonary and Critical Care Medicine outpatient clinic (Philadelphia, Pennsylvania, USA). Each day data from pulmonary physicians were collected for potential participants based on their medical records.. Patients with any level of asthma severity were invited to participate. However, patients with complex cases such as those patients with more than one respiratory diagnosis (e.g. comorbid chronic obstructive pulmonary disease plus and asthma) were excluded.
Social problem solving was measured cross sectionally using the Social Problem-Solving Inventory-Revised: Short Form (SPSI-R: S) developed by D’Zurilla et al. 24 The SPSI-R: S is a 25- item self-report questionnaire based on the validated SPSI-R 24 that assesses an individual’s tendency to engage in positive or negative problem orientations (two subscales) and adaptive (rational subscale) or maladaptive problem-solving styles (avoidant subscale and impulsive–carelessness subscale). The SPSI-R: S has good test–retest reliability across samples of adolescents, young adults, middle-aged adults, and elderly adults (r = .79) and has demonstrated strong structural, concurrent, and predictive validity. 24 Composite SPSI-R: S scores range from 0 to 20, with 20 representing the most adaptive social problem solving. SPSI-R: S subscale scores range from 0 to 4.
Asthma control was measured with the Asthma Control Questionnaire (ACQ) that includes assessment of the patient’s peak expiratory flow rate, a measure of lung function. Using nSpire Health “Pocket Peak Flow Meter” participants provided three peak expiratory force measures with time allowed in between for the patient to relax and regain normal breathing. The highest of the three peak expiratory force readings was compared against each patient’s predicted score. The ACQ has exhibited high reliability. In a 9-week validation study, patients whose asthma remained unchanged demonstrated an intraclass correlation coefficient of 0.90 across the two administrations of ACQ. 25 Asthma-related quality of life was assessed with the Mini-Asthma Quality of Life Questionnaire (AQOL) (Short Form). 22 This measure was found to exhibit an intraclass correlation coefficient of 0.83 in patients whose asthma remained unchanged. 22 Both asthma measures have scores that range from 0 to 7; 0 representing the worst asthma control and most impacted asthma-related quality of life and 7 being optimal control and least impacted asthma-related quality of life.
Statistical analysis
Patient characteristics
Around 5–25% of the patients in each clinic, depending on the day, were deemed to have a primary pulmonary diagnosis of chronic asthma without pulmonary comorbidities and were asked to participate. Over the course of 18 months, a total of approximately 70 participants were invited to participate. Of this, 21 patients declined due to lack of interest or time constraints as the most common reasons. Forty nine eligible and consenting volunteer participants completed the study assessments. The sample was largely female (82.5%) identifying as Black (55%), White (35%), Hispanic or Latino (5%), and Asian (2.5%) with age range from 20 to 78 years, mean age of 49.03, standard deviation (SD) of 14.68. Most participants (65%) lived in households making less than US$40,000 per year, and 20% reported being a current smoker. Descriptive data for the SPSI-R: S can be found in Table 1. In terms of asthma health, patients ranged from well controlled to poorly controlled asthma. The mean ACQ score was 1.92, SD = 1.2. The sample mini-AQOL (short form) mean was 4.45 and SD = 1.54.
SPSI-R: S, n = 39.

SD: standard deviation; SPSI-R: S: social problem-solving inventory-revised: short form.
Descriptive statistics (e.g. means, ranges, skewness, and kurtosis) were generated for the total sample, those taking medication, and those not. These preliminary analyses of distributional properties were performed to determine whether outliers were present and if variance stabilizing or normalizing transformations should be applied. These preliminary analyses indicated that one observation was an outlier in terms of their asthma measures. Data for this observation were removed from analyses. To ensure that the sample represented a group of more severe asthma patients reporting asthma-specific medication use, cases were excluded from analysis if they reported that they did not use asthma medication (n = 2) or had missing data for this variable (n = 3). Data from the final sample of 44 participants were entered into SAS version 12.1 for analyses.
Preliminary analysis
Preliminary analyses of demographic associations to asthma control indicated that age, gender, and household income were potentially important covariates for modeling asthma health for both ACQ (age β = 0.03, 95% confidence interval (CI): 0.015–0.051, p = 0.001; gender β = −1.01, 95% CI: −0.012–2.028, p = 0.053; income β = 0.11, 95% CI: −0.064–0.291, p = 0.204) and mini-AQOL (short form) (age β = 0.05, 95% CI: 0.024–0.076, p = 0.001; gender β = 1.24, 95% CI: −0.084–2.556, p = 0.066; income β = 0.12, 95% CI: −0.127–0.368, p = 0.328). While these variables did not account for statistically significant amounts of variance in ACQ and mini-AQOL (short form) age, gender, and income have been repeatedly identified in previous literature as important factors when examining self-management processes 26 –28 ; so these variables were included in the primary multivariate models.
Results
Direct entry linear regression models were used to control for demographic variables (age, gender, and income) and estimate the unique contribution of social problem solving to asthma health. Of the 5 subscales, impulsive–careless problem-solving style emerged as a statistically significant predictor of asthma control (β = 0.70, p = 0.001, CI [0.37–1.04]) with higher scores on the impulsive–careless subscale related to lower scores on asthma control (Table 2). Higher impulsive–careless problem-solving scores also predicted lower asthma-related quality of life (β = 0.79, p = 0.017, CI [0.15–1.42]; Table 3).
SPSI-R: S, gender, age, and income predicting ACQ, n = 39.
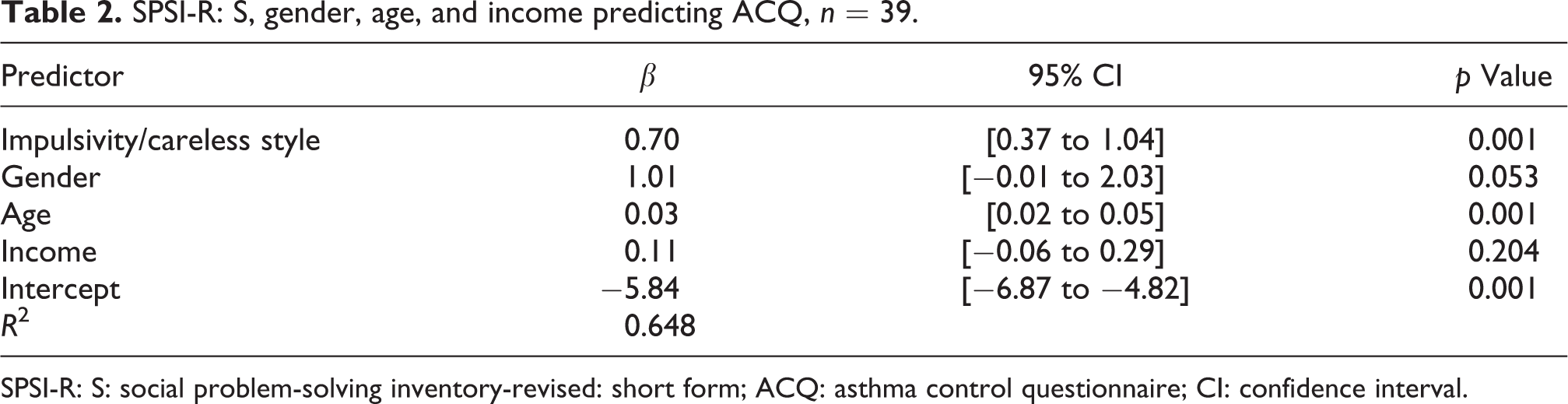
SPSI-R: S: social problem-solving inventory-revised: short form; ACQ: asthma control questionnaire; CI: confidence interval.
SPSI-R: S, gender, age, and income predicting AQOL-mini, n = 39.

SPSI-R: S: social problem-solving inventory-revised: short form; AQOL: asthma quality of life questionnaire; CI: confidence interval.
Discussion
This study hypothesized that greater impulsive and careless social problem-solving style, as measured by the SPSI-R: S, would be associated with (1) poorer asthma control and (2) more negatively affected asthma-related quality of life. Both hypotheses were supported in the hypothesized directions and at a statistically significant level. Even when variance in asthma associated with gender, age, and income was controlled for impulsive and careless problem-solving styles accounted for a significant proportion of variance of both asthma control and quality of life.
Research similar to the presented study and studies of applications aimed at improving social problem solving or coping with chronic illness do exist. One study of pediatric asthma used social problem-solving measures to identify potential vulnerabilities in the family’s ability to manage asthma. However, the study did not carry out statistical analyses relating specific types or levels of maladaptive problem solving with asthma morbidity. 8 Studies of adult asthma found that variables similar to social problem-solving components (e.g. avoiding asthma) were related to quality of life. 29,30 In children with asthma, analyses indicated that avoidant coping with asthma mediated the relationship between emotional competence and quality of life. 31 At this time, high-quality intervention studies aimed at enhancing adaptive social problem solving and reducing maladaptive coping to improve asthma are limited. A home-based coping with asthma psychosocial intervention delivered by a nurse receiving psychological supervision did not result in better outcomes in comparison with routine care. 32 However, the intervention did not measure baseline levels of maladaptive coping nor did the report indicate explicitly which cognitive behavioral approaches were applied. Obviously without baseline measures, the study could not determine whether or not potential deficits in coping were remedied.
Another trial compared improvements in asthma and cognitive–behavioral problem solving in two groups (1) children attending the routine summer camp and (2) the camp + problem-solving training that targeted constructs very similar to those in social problem solving. 33 Again, there was no difference between the two groups in terms of asthma outcomes. The findings of these trials speak to the need for (1) research such as the work presented here that identifies the most relevant types of coping deficits, (2) individualized cognitive–behavioral assessment to identify patients with room for improvement in coping, and (3) intervention studies to conduct pre- and post-intervention measures in order to determine if the intervention impacts variables of interest (e.g. social problem solving) and actual asthma outcomes.
While it was not a study of asthma, one randomized control trial testing the effectiveness of coping-based interventions versus a wait-control group for atopic dermatitis yielded measured improvements in adaptive coping and the atopic condition itself. 34 Further, a recent review of coping skills training programs for diabetes found that such programs are effective means of improving health outcomes. 35 Overall, it appears there is value to coping-focused interventions, but they ought to be directed at patient’s individual deficits. Such interventions should also test for changes in stress and coping skills and asthma-related physiologic and quality of life variables.
Each asthma patient has their own risk factors and protective factors including social support, economics and health care access, education, understanding of the disease and the roles of medication, ability to control environmental triggers, and beliefs about one’s ability to manage asthma. Social problem solving, being a meta-process, can impact all of these. The advantage of interventions aimed at improving social problem solving is the potential to positively impact asthma (or health in general) along multiple pathways: social, behavioral, and physiological. In addition, this research focused on social problem solving because of its history of high predictive and descriptive power in health outcomes, as well as the aptitude for clinical translation. Not only can strengths and weaknesses in social problem solving be measured adaptive social problem solving can be taught to anyone and the benefits apply to health behaviors such as asthma management and all other challenges in life.
Results from this study suggest that patients’ social problem solving is a key contributor to asthma control and asthma-related quality of life. As such, the presented research lays the foundation for asthma health training modules that measure social problem solving and facilitate the development of adaptive social problem solving. These modules would include components to increase positive problem orientation and promote adaptive problem-solving styles. Patients and families would be counseled to view stressors, including health care visits and medication adherence challenges, as good opportunities to maintain well-controlled asthma. Further, in light of these findings, the importance of not avoiding life’s problems, particularly asthma, should be emphasized. Future research should further extrapolate the extent to which social problem-solving interventions can actually improve social problem solving and relieve asthma through changes in adherence, environmental triggers management, and asthma-related physiologic outcomes.
Footnotes
Acknowledgment
Author Sean McCormick acknowledges the coauthors Dr Christine Nezu, Dr Arthur Nezu, Dr Michael Sherman, Dr Adam Davey, and Dr Bradley Collins and also the Hahnemann Hospital Pulmonary Clinic fellows, residents, and staff for logistic support.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.