
Abstract
Patients with clinically stable chronic obstructive pulmonary disease (COPD) are physically inactive, and this inactivity appears to be an independent predictor of hospitalizations. To explore this relationship further, we compared physical activity of COPD patients assessed in 2008 to subsequent hospitalizations and mortality. Sixty adults with a history of cigarette smoking, a diagnosis of COPD, a forced expiratory volume in 1 second (FEV1)/forced vital capacity (FVC) of <0.70, and no recent exacerbation were studied. Physical activity was measured using a triaxial accelerometerworn on the waist for seven consecutive days and the vector magnitude units (VMUs) that are the sum of movements in three planes over each minute were recorded. Those patients with mean VMU < 170 (the median) were considered to be less physically active, and those with a 6-minute walk distance (6MWD) test of <350 m were considered to have lower functional exercise capacity. These two variables, along with age, gender, and a history of exacerbations in the preceding 12 months, FEV1, body mass index, and supplemental oxygen requirement, were related to subsequent all-cause and respiratory-related hospitalizations that occurred over the ensuing 53 ± 2 months. The mean age was 68 ± 11 years, 50% were male, and the FEV1 was 53 ± 19%. All-cause and respiratory-related hospitalizations occurred in 58 and 35%, respectively. A 6MWD < 350 m and VMU < 170 each significantly predicted subsequent all-cause and respiratory-related hospitalizations in univariate Cox proportional hazards analyses after controlling for previous exacerbations. Both 6MWD < 350 m and VMU < 170 counts remained in a multivariate model predicting respiratory-related hospitalization. These results indicate that both directly measured physical activity and functional exercise capacity are important predictors of hospitalization in COPD.
Keywords
Introduction
Patients with clinically stable chronic obstructive pulmonary disease (COPD) are physically inactive when compared with age-matched control subjects. For example, a study by Pitta et al. 1 demonstrated that COPD patients spent less time walking and standing and had less movement intensity during walking than healthy controls subjects. This low level of physical activity decreases even further following a hospitalization for a COPD exacerbation. 2 Physical inactivity in COPD is probably the result of multiple factors, including dyspnea associated with physical exertion, reduced ambulatory muscle mass, strength and aerobic capacity, reduced self-efficacy for walking, maladaptive behaviors such as sedentarism, and common comorbidities that may reduce activity, such as cardiac disease, peripheral vascular disease, or depression. 1,3–6
Although physical inactivity in COPD is associated with impaired health status, 7 more importantly, it appears to be a predictor of all-cause mortality and hospitalization independent of other severity variables. In one study by Waschki et al., 8 directly measured physical activity from a device worn on the arm was a stronger predictor of mortality over a 4-year period than traditional severity markers, including the forced expiratory volume in 1 second (FEV1) and 6-minute walk distance (6MWD). In another study by Garcia-Rio et al., 9 physical activity obtained from a triaxial accelerometer (RT-3) worn on the waist along with comorbidity and exercise endurance time during constant work rate testing were predictive of mortality. Furthermore, patients with higher physical activity were less likely to be subsequently hospitalized due to COPD exacerbations.
Patients with COPD frequently have prominent extrapulmonary manifestations and comorbid conditions that contribute to their overall disease burden. 10 Since hospitalizations in COPD are exceedingly important in driving up overall health care costs, more information regarding other factors influencing all-cause hospitalizations would also be useful. Accordingly, we measured physical activity in stable COPD patients using a triaxial motion detector worn at the waist and then related this to both all-cause as well as respiratory-related hospitalizations.
Methods
Aim of this study
The aim of this study is to determine whether directly measured physical activity is a significant predictor of all-cause and respiratory-related hospitalizations in COPD.
Patients
The study was approved by our institutions’ Institutional Review Board and informed, written consent was obtained from all patients. In 2008, patients were recruited from the pulmonary section for a study measuring physical activity. Inclusion criteria included adults with a clinical diagnosis of COPD, a 10+ pack-year history of cigarette smoking, and an FEV1/forced vital capacity (FVC) < 0.70 by spirometry. No specific airflow limitation criteria were required for study participation. All subjects had to be free from an exacerbation of COPD in the preceding 4 weeks. Patients residing in a skilled nursing facility, those actively participating in a pulmonary rehabilitation program, those with significant movement disorders, and those with disease severity or comorbidity that would preclude participation in this study were excluded.
Baseline evaluation
Clinical information recorded included age, gender, body mass index (BMI), FEV1, expressed as percentage predicted, 6MWD, Medical Research Council (MRC) dyspnea rating (range 0–4, with 4 representing most dyspnea), respiratory medications, smoking status, the presence of comorbid conditions, and whether or not the patient had had an exacerbation of COPD in the preceding 12 months (by self-report). Physical activity was assessed over seven consecutive days using a RT-3 worn on the lateral position of the waist. This 2.3 oz activity monitor assesses movements in three planes using a piezoelectric sensor. Patients were instructed to wear this device while awake. The sum of movements over each minute in the three axes (vector magnitude units, VMUs) was recorded. Nonuse of the device was reduced using a computer algorithm created for this purpose. 11 Briefly, this involves utilization of a minute-by-minute decision tree to determine use versus nonuse. The device is considered to be worn on any particular minute if two of the following three criteria are met: (1) the VMU for that minute is >5; (2) at least 2 of the preceding 20 minutes have VMU > 5; and (3) at least 2 of the subsequent 20 minutes have VMU > 5.
Patients were divided into those with a 6MWD ≥ 350 m and those with a 6MWD < 350 m, since this threshold is useful in predicting mortality in COPD. 12 Since there is no established cutoff value for VMU that predicts outcome such as mortality or hospitalizations, we arbitrarily used the group median value of 170 counts/minute to separate those with higher and lower levels of physical activity.
Evaluation of hospitalization and mortality data
One investigator accessed our hospital’s database to determine hospitalizations and mortality occurring between study entry in 2008 and a subsequent analysis in 2012. Information included the dates of hospitalization and mortality, duration of hospitalization, and primary diagnosis for each hospital admission. Patients were also contacted by telephone to determine whether they were hospitalized outside our system; this information was added to the data, when necessary. A hospitalization was considered as respiratory related when, in the investigator’s interpretation, the discharge diagnosis was either COPD exacerbation or pneumonia.
Data analysis
Unless otherwise stated, clinical and disease severity data are presented as means ± SDs. The primary intent of our study was to determine whether directly measured physical activity predicts hospitalizations in COPD patients. The dependent variables were all-cause hospitalizations and respiratory-related hospitalizations over the interval from the baseline determination in 2008 to our analysis in 2012. Baseline clinical characteristics (age, gender, BMI, FEV1, 6MWD (dichotomized to above and below 350 m), and mean VMU per patient (dichotomized to above and below 170)) were related to all-cause and respiratory-related hospitalizations and mortality using Cox proportional hazards analyses. Since the history of exacerbations in the preceding 12 months has been demonstrated to be a significant predictor of frequent exacerbations, 13 it was included in all models as a covariate. Graphical depiction of hospitalization data are presented using Kaplan–Meier graphs. The value of p < 0.05 was considered significant.
Results
In total, 60 patients were studied, and their characteristics at baseline are given in Table 1. According to the Global Initiative for Chronic Obstructive Lung Disease (GOLD) 14 classification of severity of airflow limitation, 6 patients were in GOLD I, 29 were in GOLD II, 18 were in GOLD III, and 7 were in GOLD IV. Of these, 14% were current smokers, 76% reported one or more exacerbations in the year preceding study entry, and 40% reported two or more exacerbations over this time period. Diabetes was present in 28%, hypertension in 58%, a history of coronary artery disease in 24%, a history of congestive heart failure in 20%, and obstructive sleep apnea in 20%. Long-acting β agonist bronchodilators were used in 86%, long-acting anticholinergic bronchodilators in 75%, and inhaled corticosteroids in 76%.
Patient characteristics at baseline.

BMI: body mass index; FEV1: forced expiratory volume in 1 second; MRC: Medical Research Council; 6MWD: 6-minute walk distance; VMU: vector magnitude unit.
The duration of activity monitoring per patient, representing the time actually worn during waking hours, was 4895 ± 1428 minutes. There was no significant correlation between wear time and VMU. The mean 6MWD was 317 m (median = 329, range = 28–526 m.), and the mean VMU was 188 counts per minute (median = 170, range = 69–416 counts). Twenty-four patients (40%) had a mean 6MWD ≥ 350 m. The relationship between these two categorical variables is as follows: 6MWD ≥ 350 m and VMU > 170 counts: 19 patients; 6MWD ≥ 350 m and VMU < 170: 5 patients; 6MWD < 350 m and VMU ≥ 170: 12 patients; and 6MWD < 350 m and VMU < 170: 24 patients. Patients with VMU < 170 were older than those at or above that threshold: 72 ± 1.8 (standard error (SE)) versus 64 ± 1.8 years, respectively (p = 0.002), and had shorter 6MWD: 256 ± 16 (SE) versus 372 ± 16 m, respectively (p < 0.0001). There was no significant difference in FEV1 percentage predicted or BMI between higher and lower VMU categories: FEV1, 55 ± 17% versus 52 ± 20%, respectively (p = 0.53); BMI, 30 ± 6 kg/m2 versus 24 ± 7 kg/m2, respectively, (p = 0.46).
The time from the baseline determinations to the data analysis was 53 ± 2 months. Over this interval, 35 (58%) had been hospitalized at least once and 21 (35%) had been hospitalized for a respiratory cause at least once. Twenty-two patients had multiple all-cause hospitalizations over this interval and 14 had multiple respiratory hospitalizations.
Gender, BMI, MRC dyspnea, FEV1 percentage predicted, and GOLD classification did not predict hospitalization. A self-report history of an exacerbation in the preceding 12 months, present in 76%, did not significantly predict either all-cause or respiratory-related hospitalizations (p = 0.14 and 0.13, rrrespectively). Similarly, the history of two or more exacerbations in the preceding year was not predictive of subsequent hospitalizations (p = 0.06 for both all-cause and respiratory-related hospitalizations). The presence of diabetes, hypertension, obstructive sleep apnea, coronary artery disease, or the history of congestive heart failure did not predict hospitalizations. Similarly, there was no significant relationship between the use of any of the maintenance-inhaled medications for COPD and subsequent hospitalizations.
In univariate analyses, with the history of exacerbations (yes–no) included as a covariate, the following clinical variables were related to subsequent all-cause and respiratory-related hospitalizations: age, in years (hazard ratio (HR) 1.05, p = 0.01 and HR 1.06, p = 0.004, respectively); supplemental oxygen use (HR 2.9, p = 0.004 and HR 3.6, p = 0.006, respectively); 6MWD < 350 m (HR 3.7, p = 0.003 and HR 8.4, p = 0.004, respectively); and VMU < 170 (HR 2.9, p = 0.004 and HR 6.0, p = 0.001, respectively). Current smokers (n = 8) were at increased risk of all-cause hospitalization (HR 2.4, p = 0.04) but not for respiratory-related hospitalization. These results are listed in Table 2, while Kaplan–Meier survival curves depicting the effects of 6MWD and VMU on hospitalizations are given in Figure 1 and 2.
Significant predictors of hospitalization in univariate analyses.

6MWD: 6-minute walk distance; VMU: vector magnitude unit.
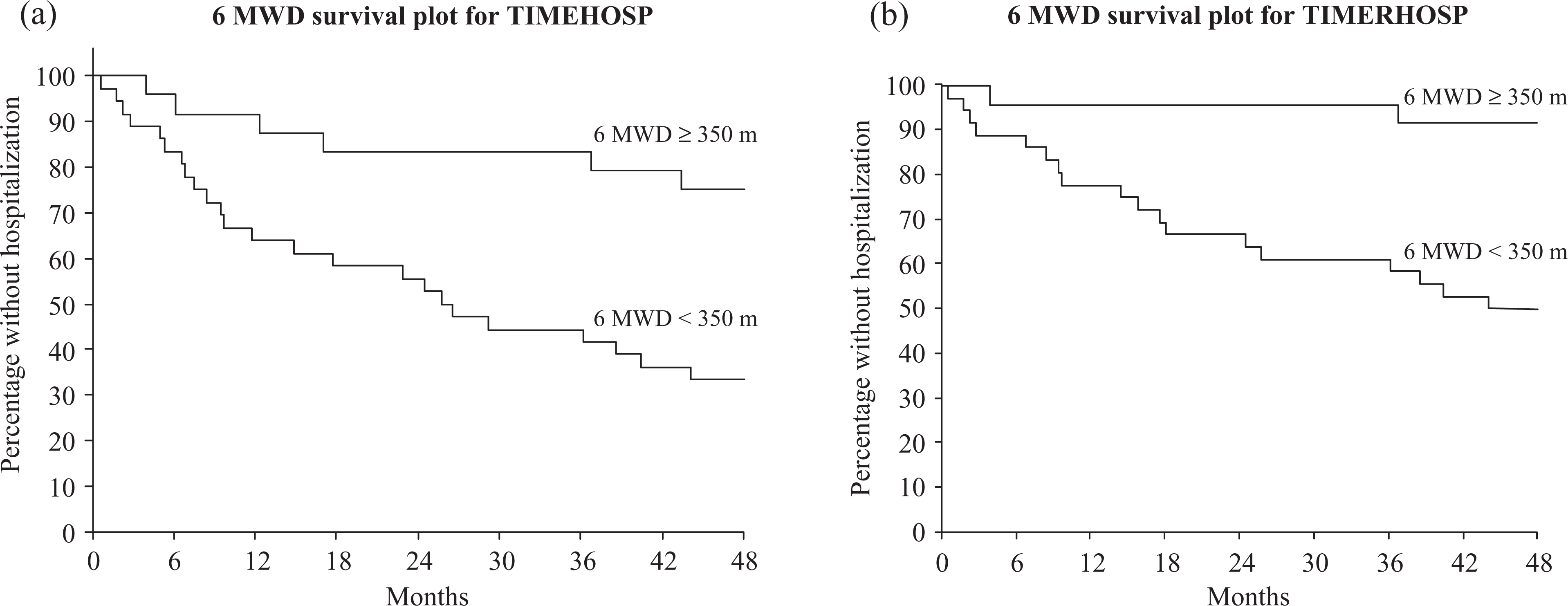
(a) Time to first all-cause hospitalization by 6MWD. (b) Time to first respiratory-related hospitalization by 6MWD. 6MWD: 6-minute walk distance.
In forward stepwise multivariate testing, in which age, gender, smoking status, FEV1 percentage predicted, oxygen supplementation, history or exacerbations in the preceding year, and 6MWD and VMU were included as potential factors predicting hospitalization; 6MWD < 350 m and oxygen supplementation requirement remained in the model predicting all-cause hospitalization, while 6MWD < 350 m and VMU < 170 counts remained in the model predicting respiratory-related hospitalization. These results are summarized in Table 1.
Predictors of hospitalization in multivariate testing.
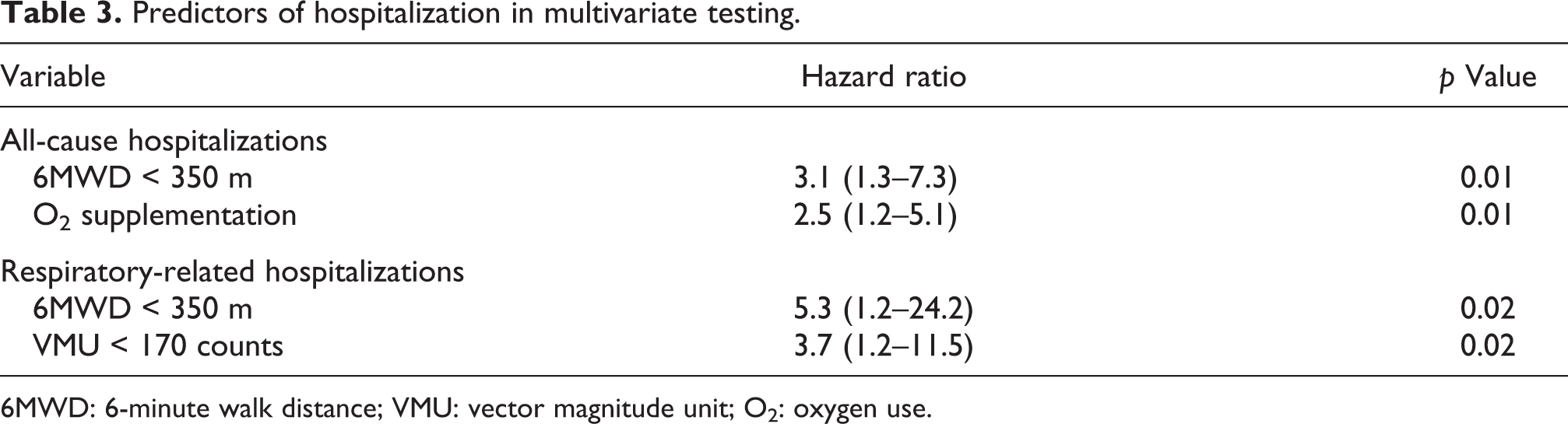
6MWD: 6-minute walk distance; VMU: vector magnitude unit; O2: oxygen use.

(a) Time to first all-cause hospitalization by VMUs. (b) Time to first respiratory-related hospitalization by VMUs. VMUs: vector magnitude units.
Eight patients (13%) died during the follow-up period. This represents a mortality rate of 2.5% per 100 patients per year. All eight patients who died had 6MWD < 350 m. VMU < 170 was not significantly related to mortality (p = 0.11).
Discussion
The results from our study suggest that functional exercise capacity and physical activity are both predictive of all-cause and respiratory-related hospitalizations in patients with COPD. These two variables not only predicted all-cause hospitalization in univariate testing, they both remained in the model in the multivariate analysis for respiratory-related hospitalizations. This underscores the need to consider these two variables as separate constructs. The patient’s exercise capacity measured in the laboratory and his/her physical activity in the home and community settings appear to be independently predictive of respiratory-related hospitalizations.
A major limitation of our study is its relatively small sample size of 60 patients and our multivariate analyses testing multiple (eight) baseline variables as predictors of hospitalization. Because of this, our results should be interpreted with caution, and firm conclusions would need confirmation from testing a larger cohort study.
The frequency of exacerbations (by self-report) in our patients was high: 76% reported one or more and 40% reported two or more in the 12 months before study entry. This is considerably higher than the 47 and 29%, respectively, reported in a large, longitudinal study of COPD. 13 This difference may reflect the selection bias – referral to a pulmonary specialist in our sample may have been more likely in the patient with frequent exacerbations – or may reflect inaccuracy in self-reported exacerbations. We did not verify this history with record documentation. Of interest, neither the history of one or more exacerbations in the year preceding recruitment nor two or more over this were related to subsequent hospitalization in our study.
Although it is not clear whether increasing exercise capacity or physical activity in COPD patients through pharmacologic or nonpharmacologic interventions will reduce subsequent health-care utilization, it does support attempts to address both problems. For instance, goals of pulmonary rehabilitation should include both increasing exercise performance and physical activity.
Steele and colleagues, using an earlier version of the activity monitor in stable COPD patients, demonstrated a mean daily VMU ranging from 80 to 115, depending on whether or not patients were participating in pulmonary rehabilitation on the days of testing. Our mean VMU of 188 is higher, possibly because we eliminated nonuse of the device, thereby decreasing the number of minutes per day with false zero or near zero counts from the analysis. Our mean VMU is closer to the value of 208 reported by Garcia-Rio et al. in their earlier study. 9
Dichotomizing the 6MWD using a 350-m threshold seems reasonable based on a study by Cote et al. 12 Of the 1379 COPD patients followed for 55 ± 29 months, mortality was 66% of those with a 6MWD < 350 m and 31% in those above this threshold. In contrast, a clinically meaningful threshold value for dichotomizing VMU, if it exists, has not yet been defined. Therefore, we utilized the median value, 170 counts per minute, as an arbitrary threshold. In a similar fashion, Garcia-Rio et al., 9 who used the same type of device as ours in their prospective study comparing activity to outcome in 173 COPD patients, categorized VMU into quartiles for their analysis. Our smaller sample size precluded the creation of more than two groups for analysis.
Recent studies have demonstrated a relationship between questionnaire-rated physical activity and outcome. An analysis of 2386 individuals who met criteria for COPD in the Copenhagen City Heart Study disclosed that a very low level of self-reported physical activity at the baseline evaluation was associated with the highest risk of hospitalization for COPD over the ensuing 12 years. Furthermore, self-reported physical inactivity predicted a higher all-cause and respiratory mortality over this time period. 15 In another study, those patients hospitalized for a COPD exacerbation were more likely to be readmitted if they reported lower levels of physical activity. 16
The study by Garcia-Rio et al., 9 similar to ours in design, had similar results. They measured physical activity using the same type of RT-3 worn at the waist in 173 patients (91% male) over 65 ± 26 months. In their study, physical inactivity was predictive of shorter time to first COPD hospitalization and greater hospitalization risk. Our study had a greater percentage of female participation, although the FEV1 percentage predicted and 6MWD values were remarkably very close to theirs. Our study extends their findings by also demonstrating the relation between physical activity and all-cause hospitalizations as well as respiratory-related hospitalizations.
The demonstration that the timed walk distance in our patients was related to mortality—all eight deaths were in patients with 6MWD < 350 m—has been demonstrated before. 17,18 Lower performance on the externally paced incremental shuttle walk test has also been demonstrated to be predictive of mortality in COPD patients participating in pulmonary rehabilitation. 19 Our finding that VMU was not significantly predictive of mortality (p = 0.11) may have been due to the relatively small number of subjects and the relatively low mortality rate in our study. The study by Garcia-Rio et al., with its larger sample size, did indeed show a significant relationship in this outcome area.
In summary, our study provides further evidence that lower levels of directly measured physical activity are predictive of increased all-cause and respiratory-related hospitalizations in COPD in univariate analyses. Since both physical activity and functional exercise capacity remained in our multivariate model predicting respiratory-related hospitalization, it appears that both act independently in predicting this health-care outcome. This knowledge may expand our clinical approach to COPD toward exploring ways to translate gains in exercising capacity realized from pharmacologic and nonpharmacologic interventions into increases in physical activity at the home and in the community settings.
Footnotes
Acknowledgement
The authors wish to thank Dr Bimalin Lahiri, MD, Chief, Pulmonary and Critical Care, St Francis Hospital and Medical Center, Hartford, Connecticut, USA, for his support in this research study.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.