
Abstract
There has been a rise in the number of patients requiring long-term ventilation, both in the in-hospital and the out-of-hospital setting. Despite this, little is known about the subsequent clinical course of these patients following hospital discharge. The purpose of this study was to determine the frequency and management of respiratory incidents in patients with invasive out-of-hospital ventilation living in a nursing home allied to a weaning centre. We evaluated retrospectively the protocols that are used to monitor the patients over a period of 2 months. The average time from hospital discharge was 386 ± 330 days. Of the total 17 patients, 9 (53%) patients remained free from any respiratory incidents, while the remaining 8 (47%) patients were responsible for a total of 95 respiratory incidents. Patients that suffered respiratory incidents had been ventilated at home for an average of 194 days, while the others were receiving out-of-hospital ventilation for an average of 557 days. Desaturation (17), dyspnoea (17) and reduced general condition (10) were the most common respiratory incidents. Also, the use of an Ambu bag (bag valve mask; 17), request for a pneumologist review (12) and replacement of the tracheal cannula (7) were the most common interventions. Respiratory incidents are common in invasive home mechanical ventilation, and so home mechanical ventilation needed to be organized safely. Being allied to a weaning centre helps to organize invasive home mechanical ventilation in a safe manner over the long-term ventilation.
Keywords
Introduction
Patients requiring ventilation for more than 7 days are defined as prolonged weaning. 1 , 2 An estimated 55% of such patients can be successfully weaned from invasive ventilation, while 25% die and 20% remain dependent on either invasive or non-invasive ventilation (NIV). 3 In the recent years, the incidence of long-term ventilation appears to be on the rise. The Eurovent survey of 483 centres estimated the prevalence of home mechanical ventilation in 2005 to be 6.6/100,000 people with a wide variation between regions and countries. In total, 10–25% of the patients receiving home mechanical ventilation are ventilated via tracheostomy depending on the underlying disease. 3 , 4
Since 2005, the prevalence of prolonged and home mechanical ventilation has further increased. 5 The explanation for this rise in number involves the increasing age of patients, increasing severity of illness and an increase in patients with chronic lung disorders. Therefore, for example, the rate of successful weaning of patients in Italy has been shown to have fallen from 87 to 66% 6 between 1991 and 2006. Equally, the improvement in specialist care in combination with better accessibility to respiratory and weaning centres has also led to an augmented number of home mechanically ventilated patients. 7 It is expected that the incidence of mechanical ventilation projected to the year 2026 will be increased by about 80%, due in part to ageing baby boomers. 8
Despite the increasing prevalence of patients with invasive out-of-hospital ventilation, little has been published about the surroundings and medical support of these patients and the complications of long-term ventilation at home. It seems obvious that the environment of home mechanically ventilated patients will vary between countries, depending on local medical expertise and infrastructure as well as on differing social and health care systems. Nevertheless, there is no data describing these varying circumstances in detail and many questions remain: (1) How secure is life for patients with invasive out-of-hospital ventilation? (2) How many emergencies occur? (3) Are newly discharged patients more unstable than patients already established on a long-term ventilation therapy? (4) How often is readmission to hospital necessary? and (5) What kind of emergency treatments is needed out-of-hospital?
The aim of our study was to determine the frequency and severity of respiratory incidents and emergencies involving patients with invasive ventilation living in a nursing home allied to a weaning centre and to characterize how the emergencies are managed.
Methods
We examined invasively ventilated patients living in a nursing home (‘Haus Ahorn’, Solingen, Germany), which is a home for elderly people with a specialized division caring for ventilated patients. Each patient occupies a single room. Comparing this facility with an intensive care unit (ICU), there is no continuous invasive or non-invasive monitoring of the patients. However, each patient is equipped with a high-quality pulse oximeter with an in-built acoustic alarm (mostly OxiMax N560, Nellcor Puritan Bennett, Boulder, Colorado, USA), and in addition, the ventilator’s alarm is connected to the nurse call system.
The early shift is covered by six nurses, the late shift by five nurses and two nurses are present at night. At least 70% of the nurses are fully qualified, with the remainder comprising of auxiliary staff.
The home is located on the grounds of a weaning centre and pulmonary hospital (Bethanien Hospital, Solingen). The medical cover is supplied by general practitioners with the assistance of a weekly ward round by a pneumologist from the nearby weaning centre. Furthermore, doctors from the hospital provide emergency out-of-hours cover.
We retrospectively evaluated the protocols used to monitor 17 invasively ventilated patients living at the nursing home over a 2-month period. The protocols contain 15 suspected emergency incidents in respiratory care. The protocols can be found in each living area, and every time an emergency occurs, the nursing staff are required to register the incident. If an emergency fulfils more than one criterion in the protocol, every applicable criterion is marked.
Analysis
The data were analyzed using non-parametric descriptive statistics. We report the frequency of incidents using bar charts. Time after hospital discharge and duration of ventilation as well as frequency of respiratory incidents in relation to the duration of ventilation are presented as box-and-whisker plot with the bottom and top of the box indicating the 25th and 75th percentile and a band near the middle of the box indicating the median (50th percentile). Non-parametric comparisons were performed using Mann–Whitney U test.
Results
During the observation period of 2 months, of the total 17 patients, 9 patients were free of any incidents, while the remaining 8 patients triggered all reported incidents. A total of 95 respiratory incidents were registered (Figure 1). Oxygen desaturation and reported dyspnoea were the most common incidents, followed by a reduced general state of health (Table 1). One patient died during the observation period although resuscitation was attempted. The death was unexpected and the cause remained uncertain.
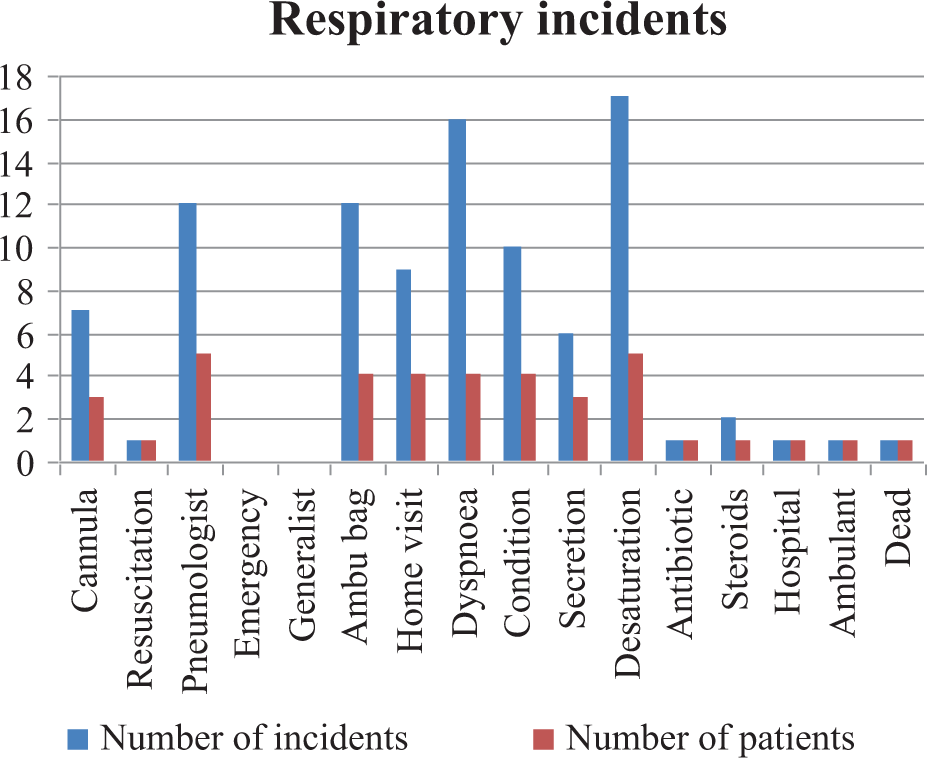
Frequency and character of respiratory incidents relating to patients. Eight of 17 patients had an incident (47%). Cannula: replacement of tracheal cannula; resuscitation: resuscitation of the patient; pneumologist: phone call to pneumologist of the nearby hospital; emergency: emergency call; generalist: call of a general practitioner; Ambu bag: use of an Ambu bag; home visit: unscheduled home visit of the patient by a doctor; dyspnoea: patient suffering from dyspnoea; condition: worsening of general condition; secretion: increase of tracheal secretion; desaturation: desaturation of 5% or more in relation to average saturation of the patient; antibiotic: use of antibiotics; steroids: use of steroids; hospital: hospital transfer; ambulant: transfer to emergency room (ambulant).
Frequency distribution of the most common respiratory incidents.a

aFor explanation of incidents refer to Figure 1.
The most common interventions undertaken by the nursing staff were the use of an Ambu bag (n = 16) and the replacement of the tracheal cannula (n = 7), indicating that the respiratory incidents are the most severe problems in out-of-hospital invasively ventilated patients. Most of the emergencies were managed solely by the nursing staff, but in 13% of the cases, a doctor from the nearby hospital was called. It was not necessary to call the ambulance or public emergency doctor at any time.
Of the total 17 patients, 12 patients were long-term ventilated due to chronic obstructive pulmonary disease (COPD). The remaining five patients had a relevant neurological diagnosis leading to chronic hypercapnic failure (Table 2). The reported incidents occurred in patients with COPD (five patients) as well as in patients with neurological diagnosis (three patients).
Main diagnosis leading to chronic hypercapnic failure.

COPD: chronic obstructive pulmonary disease.
The average duration of ventilation at the beginning of the observation period was 490 ± 408 days (average ± SD) and the time from hospital discharge was 386 ± 330 days (Figure 2). Fifteen patients were ventilator dependent for 22–24 hours per day, while two patients were able to breathe spontaneously during the day.
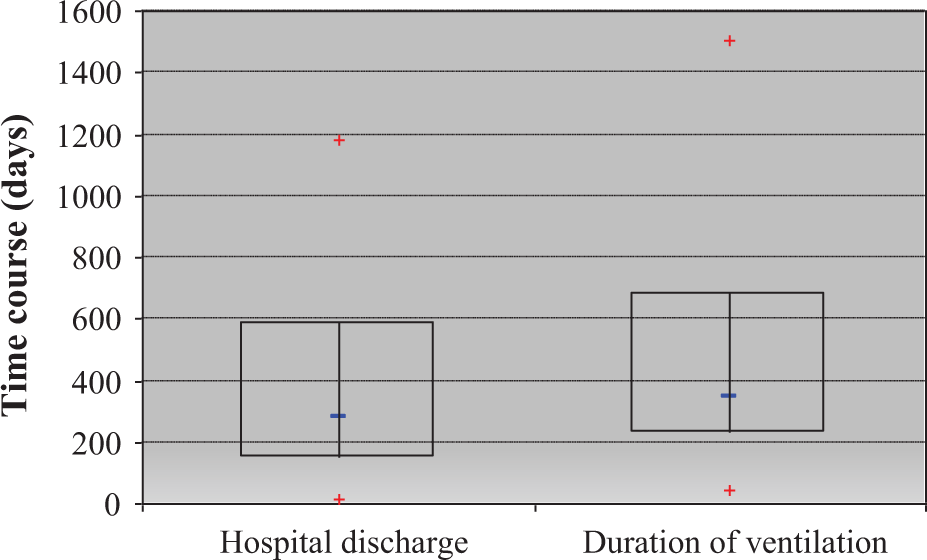
Box-and-whisker plot presenting the time after hospital discharge and the overall duration of ventilation since intubation. The median time since hospital discharge was 280 days (25%: 146 days; 75%: 588 days). Median duration of ventilation was 386 days (25%: 229 days; 75%: 686 days).
Those patients without any incidents were ventilated in the out-of-hospital setting for an average of 557 days. Patients experiencing respiratory incidents had been ventilated at home for an average of 194 days (Figure 3). This suggests that the early period following hospital discharge is more unstable with regard to the respiratory situation.
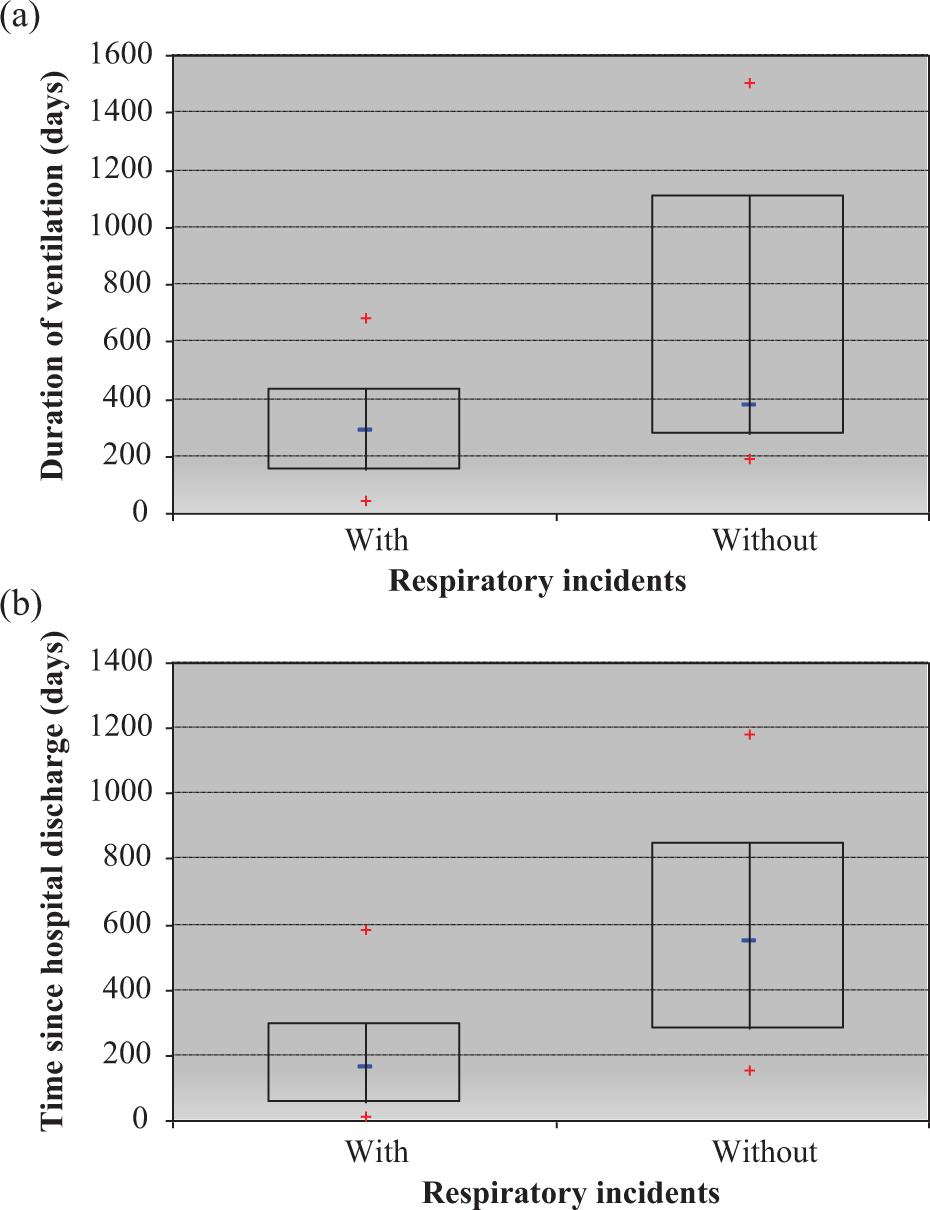
(a) Box-and-whisker plot presenting the frequency of respiratory incidents in relation to the duration of ventilation. Patients with respiratory incidents had been ventilated for 284 days (25%: 145 days; 75%: 431 days) and without incidents had been ventilated for 373 days (25%: 269 days; 75%: 1107 days; p = 0.015). (b) The plot presents the time since hospital discharge. Patients with incidents had been discharged 160 days ago (25%: 51 days; 75%: 295 days), and those without incidents had been discharged 549 days ago (25%: 278 days; 75%: 845 days; p = 0.167).
The health and ventilatory status of two patients improved gradually during the observation period. One patient was thus transferred to the weaning centre and subsequently successfully weaned. Another patient was weaned by way of gradual extension of the spontaneous breathing time before a trial decannulation was carried out. This was performed at the nursing home itself, because the patient did not wish to be readmitted to the hospital.
Discussion
Our study examines for the first time the frequency and management of critical incidents in invasive home mechanical ventilation. Summarizing the results of the study, half of the patients experienced severe incidents during an observation period of 2 months. For those patients who experienced respiratory incidents, this may be calculated as 5.9 incidents per month. These findings indicate that it is imperative to organize the out-of-hospital ventilation in a safe manner regarding the medical cover (doctors and nursing staff) and the supply of appropriate medical equipment for each patient.
Critical illness and treatment at an ICU influences not only the short-term course of patients but also the long-term outcomes. The prognosis after treatment at an ICU remains poor, with the cumulative mortality over the first year after treatment ranging from 26 to 63%. The reported 5-year mortality ranges from 40 to 58%, 9 with an increased mortality of patients with respiratory failure. 10 Moreover, invasive ventilation during ICU stay worsens prognosis with regard to the short-term outcome as well as to long-term survival. 11 Although there is no published data in this field, it can be assumed that the prognosis of patients with ongoing invasive ventilation after hospital discharge would be even worse due to respiratory problems and emergencies.
The patients that are at a high risk of long-term ventilation (longer than 7 days) and those with COPD are disproportionally represented. 12 In a German study of 2008, the overall weaning success rate in 38 weaning centres was 66.4%. 13 In general, about 50–70% of the patient with long-term ventilation may be weaned from invasive ventilation. The use of NIV facilitates weaning, especially in patients with COPD. 14 In fact, 70% of the patients in our study with continued invasive ventilation were suffering from COPD as the underlying disease. Thus, in part, the description of the respiratory incidents reflects the problems and symptoms of severe COPD.
Our study was conducted at a specialized home for ventilated patients. Although the general medical cover is supplied by a general practitioner, the patients are reviewed weekly by a pneumologist, and a nearby pneumology centre may be contacted in case of emergency. This concept is also known as the ‘Solinger Concept’ and denotes the integration of intensive respiratory medicine (e.g. weaning centre) with out-of-hospital invasive ventilation. The German guidelines of ventilation for the treatment of chronic respiratory failure recommend this kind of cooperation of home mechanically ventilated patients to a weaning centre. 15 Concepts such as the Solinger Concept contribute to the stability of the ventilated patients.
Additionally, medical supply and monitoring considerably influences the outcome of patients with out-of-hospital ventilation. In our study, the routine use of a pulse oximeter facilitated a quick and appropriate response by the home care staff. Oxygen desaturation points largely to an acute respiratory problem, which enables correct interventions (e.g. use of Ambu bag and replacement of cannula) by the nursing staff. Similarly, maintained oxygen saturation may either suggest other reasons for the reduced general state (e.g. cardiac problems) or may provide reassurance and thus avoid unnecessary emergency calls. This is an important point not only concerning the health status of the patient but also the costs involved in out-of-hospital ventilation. Readmission of an invasively ventilated patient to hospital is one of the most expensive interventions. Calculations of assurances in Germany (AOK Nordrhein/ Hamburg and TKK) demonstrate a reduction in cost by more than 40% through the reduction in the readmission rate. As seen in our study, the acute measures taken by the staff avoided the need for an emergency transfer to hospital. There was only one patient transferred to hospital, as a planned admission to complete the weaning process that was started out-of-hospital.
The patients in this study had all been ventilated out-of-hospital for a relatively long period (median of approximately 9 months), and most of the patients were highly ventilator dependent. There are two lessons that can be learned by the distribution of respiratory incidents seen in our study sample, with events occurring in patients who had been discharged on average 6 months ago versus no events occurring in patients who had been discharged on average 18 months ago. First, the early period following hospital discharge seems to be less stable and more likely to result in serious respiratory events. The reasons for this include the less intensive medical care and monitoring compared with an ICU but also the fact that a proportion of these patients are in a generally poor condition upon hospital discharge and experience a further decline in health status thereafter. Second, we demonstrate that it is possible to manage patients with out-of-hospital ventilation for lengthy periods without any respiratory incidents at all. Paradoxically, it seems that the clinical course becomes less problematic and safer in the long-term. One reason for this may be that those patients who are unstable and in poor general condition die during the first months after hospital discharge, which leaves a group of patients who are less severely ill and therefore experience fewer critical respiratory events.
In Germany, there is a good infrastructure of specialized nursing services providing care for ventilated patients. If out-of-hospital care of invasive ventilation can be well organized and becomes routine, the question may be asked whether long-term out-of-hospital ventilation should be regarded not only as the result of weaning failure but also as a medical alternative for patients with chronic respiratory failure who either do not accept or improve with NIV (‘chronic NIV failure’) and remain in a poor general condition. For these patients, invasive ventilation may be a therapeutic option. But if invasive ventilation is to become a viable treatment option for chronic respiratory failure in specific cases and is not simply characterized as the result of weaning failure, we need to have more detailed information about the further clinical course of the patients subsequent to hospital and intensive care discharge.
Conclusions
The conclusion of this study is that invasive out-of-hospital ventilation needs to be organized safely because respiratory incidents are to be expected and common, occurring in 50% of the examined patients over a 2-month period. Specific expertise consisting of specialist nursing and a key ventilator expert providing consultant support is needed. However, we have shown that these incidents can be managed in the community setting, largely by nursing staff. The alliance with a weaning centre and coordination of patient care thus helps to organize invasive home mechanical ventilation in a safe manner over the long-term. Guidelines for home mechanical ventilation assist those who look after invasively ventilated patients. 15
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.