
Abstract
Body mass index (BMI) is an important prognostic measure in chronic obstructive pulmonary disease (COPD). However, its effects on pulmonary rehabilitation (PR) are unknown. This study aimed to evaluate the effectiveness of a walking-based PR programme across the BMI range and the impact of BMI on exercise performance and health status. A total of 601 patients with COPD completed a PR programme. The effects of BMI on exercise capacity (incremental and endurance shuttle walk tests (ISWT and ESWT)) and health status (chronic respiratory questionnaire (CRQ)) before and after PR were evaluated. 16% of patients were underweight, with 53% overweight or obese. At baseline, the obese had worse ISWT (−54 m ± 14 m; p = 0.001) despite a higher predicted forced expiratory volume in 1 s (7.4m ± 1.6%; p < 0.001). Patients in all BMI categories made clinically important improvements in ISWT distance: BMI <21, 62 m; 21–25, 59 m; 25–30, 59 m; >30, 65 m (p = < 0.001). All four domains of the CRQ increased above the level of clinical significance for all BMI categories (all p < 0.001). The majority of patients with COPD were overweight associated with a lower walking capacity. A walking-based PR programme was comparably effective across the BMI spectrum. Patients with COPD should be referred for standard PR, independent of BMI.
Introduction
Chronic obstructive pulmonary disease (COPD) is characterised by systemic features that are known to have a significant impact on mortality, morbidity and health care utilisation. 1 Previous studies are consistent in showing that underweight patients with COPD have a poorer prognosis and greater disability than those of normal weight. 1 –3 Conversely obesity, an increasingly prevalent problem worldwide, appears to confer a better prognosis in COPD. 4,5
Pulmonary rehabilitation (PR) incorporating progressive exercise training is an integral part of the management of COPD and has been demonstrated to improve the exercise performance and health-related quality of life (HRQOL). 2,3 However, uncertainty remains whether nutritional status (obesity or low body weight) influences the effectiveness of PR.
In obese patients, the response to exercise training may be dependent upon the modality used. Weight unsupported exercise (walking) is one of the commonest training modalities used. Potentially, the effect of carrying extra weight (akin to training with a rucksack) may limit the duration that obese individuals can sustain high intensity endurance training needed for physiological training adaptations to occur. Conversely, recent evidence has demonstrated that obesity was associated with higher peak performance compared to normal weight during incremental cycle ergometry by reducing dynamic hyperinflation. 4 A recent study reported that those in the obese category had lower walking capacity compared to normal weight and overweight patients with COPD but similar cycle endurance capacity. 4
On the other end of the body mass index (BMI) spectrum, patients with nutritional depletion have evidence of increased systemic inflammatory cytokines 6,7 and intramuscular catabolic mediators, 5 leading to the suggestion that these patients may respond less well to anabolic therapies such as exercise or nutritional supplementation. 8,9
The current international guidelines on PR (American Thoracic Society/European Respiratory Society (ATS/ERS)) highlight the prevalence and importance of cachexia and obesity in COPD. However, there is little evidence to guide the selection of patients for PR programmes based on nutritional status.
To date there has been no large-scale study determining the influence of BMI (across the full range of nutritional status) on the outcome of PR in COPD. This limits our understanding of whom should be referred to PR and whether different exercise strategies are needed for patients at either end of the BMI spectrum. We tested the null hypothesis that patients achieve similar clinical outcomes from a standard PR programme regardless of the baseline BMI. We compared clinical outcomes of PR (field exercise performance and health status) in patients with COPD stratified into established BMI categories. To place this comparison in context, we also report the distribution of patients referred for PR in these BMI categories and the association between BMI and other disease indices at baseline.
Methods
Study design
Data were obtained from a database of patients attending an outpatient PR programme (Glenfield Hospital, Leicester, UK). Local Research Ethics Committee approval was obtained to undertake an analysis of patient data held in the database. Patients were grouped into four different BMI categories (underweight <21 kg/m2, normal weight ≥21 to <25 kg/m2, overweight ≥25 to <30 kg/m2 and obese ≥30 kg/m2). The body-mass index, airflow obstruction, dyspnea, and exercise capacity index (BODE) definition of underweight (<21 kg/m2) was chosen as the cutoff, as it is predictive of mortality in COPD. 3 Subgroup analysis of extremes of BMI was performed (using World Health Organization criteria 6 ), which is defined as BMI < 18.5 kg/m2 for very underweight and ≥40 kg/m2 for extreme obesity.
Study population
Criteria for inclusion in the analysis were a clinical diagnosis of COPD, obstructive spirometry (global initiative for chronic obstructive lung disease stage ≥2) 1 and a recorded height and weight at baseline. Completion of the PR programme was defined as those who had an incremental shuttle walk test (ISWT) recorded after PR.
Pulmonary rehabilitation
The programme comprised 7 weeks of physical training combined with multidisciplinary education, including a 1-h session on generic dietary advice. 7 Individuals were referred to a dietician for specific advice if found to be underweight. Patients attended two supervised sessions per week and daily home training (walking). The exercise programme entailed principally aerobic (walking) training. The walking speed was set at the equivalent of 85% VO2 peak derived from baseline ISWT and duration progressed throughout the programme.
Outcome measures
The following baseline data were collected at first assessment: age, gender, BMI (weight (kg)/height (m) 2 ), spirometry (ERS/ATS standards 10 ), resting heart rate and SpO2, Medical Research Council dyspnoea grade, smoking history and use of supplemental oxygen.
Exercise performance was assessed using ISWT and endurance shuttle walk test (ESWT). 11,12 Peak oxygen consumption (peak VO2) directly measured on the ISWT has been demonstrated to be linearly related to peak VO2 during laboratory incremental treadmill walking in COPD. 8 A minimally clinical important difference (MCID) in ISWT has been identified as 48 m. 9 The ESWT is a field walking test, with the constant speed set at the equivalent of 85% of the predicted peak VO2 derived from the ISWT distance. All patients underwent a familiarisation ISWT prior to assessment.
HRQOL was assessed using the self-reported chronic respiratory questionnaire 13 (CRQ-SR). The clinically important difference for each CRQ domain has previously been defined as 0.5 units. 14
Statistical analysis
Analyses were carried out using SPSS statistics (version 18, Chicago). Characteristics between PR completers and noncompleters were compared using independent t tests for continuous data and chi squared test for categorical data. Baseline characteristics between groups were compared using analysis of variance, with Bonferroni post hoc comparisons. Correlations between baseline characteristics were calculated using Pearson correlation coefficient. Following PR, within group changes were compared using paired t tests and Wilcoxon signed-rank for normal and nonnormally distributed data, respectively. Differences in exercise performance and health status between BMI categories were compared using Kruskal-Wallis analysis, correcting for baseline score (e.g. baseline ISWT, forced expiratory volume in 1 s (FEV1) percent predicted and gender). A comparison of responders and nonresponders (assessed by achieving MCID for ISWT) was analysed using chi squared test. BMI, as a continuous variable, was tested against changes in performance by multivariate regression, corrected for baseline score, FEV1 percent predicted, age and gender. The pattern of relationship between BMI and ISWT was further investigated by a locally weighted scatter plot smoother, producing Loess curves based on least squares fits.
Results
940 patients fulfilling the inclusion criteria were identified from the database, of which 601 attended a post-rehabilitation assessment (i.e. designated to have completed the programme), allowing the measurement of the ISWT, ESWT and CRQ following the intervention. There was no significant difference in BMI between patients who completed PR and noncompleters (26.4 kg/m2 (SD 5.9) vs. 26.2 kg/m 2 (SD 6.0); p = 0.703). The numbers in each BMI category are shown in Figure 1. Of all, 16% were underweight, 31% normal weight, 28% overweight and 25% obese.

Flow chart of the study.
Baseline characteristics of completers, including baseline exercise performance and health status of the four groups are shown in Table 1. There were significant correlations between BMI and FEV1 percentage predicted (coefficient 0.260; p < 0.001) and ISWT distance (coefficient −0.134; p = 0.001). The obese population, compared with normal weight, had significantly worse ISWT (−54 ± 14 m; p = 0.001) despite a higher FEV1 (7.4 ± 1.6%; p < 0.001).
Baseline characteristics of patients within BMI groups who successfully completed a pulmonary rehabilitation programme a

FEV1: forced expiratory volume in 1 s; IQR: interquartile range; LTOT: long-term oxygen therapy; ISWT: incremental shuttle walk test; ESWT: endurance shuttle walk test; CRQ: chronic respiratory questionnaire; MRC: Medical Research Council.
aBaseline exercise performance and health status data are also shown.
b p < 0.05.
Exercise performance
The mean (95% confidence interval) changes in ISWT and ESWT for the whole cohort were 61 (55–67) m and 408 (375–441) s, respectively. Changes in exercise performance in the different BMI categories are shown in Figure 2. There were clinically meaningful improvements in all measures of exercise performance (p < 0.001 for all BMI groups). There was no difference between the change in exercise performance between the different BMI groups for ISWT (p = 0.883) or ESWT (p = 0.224).

Changes in exercise performance in the different body mass index (BMI) categories based on (a) incremental shuttle walk test (ISWT) and (b) endurance shuttle walk test (ESWT). The dotted line at 48 m for ISWT indicates the minimally clinical important difference (MCID) for improvement in performance. Error bars show ±1 SE.
The mean improvement in all BMI groups was greater than the clinically significant 48 m. There was no difference in the proportion of patients achieving a 48-m improvement in the different BMI groups (underweight 60.8%, normal weight 55.1%, overweight 57.8% and obese 57.5%; p = 0.833).
Exercise performance and BMI as continuous variables were also compared. Multivariate regression showed no relationship between changes in exercise performance and BMI (ISWT: p = 0.676, ESWT: p = 0.207). Regression curves (Figure 3) demonstrated a lower baseline ISWT at the extremes of BMI but similar absolute improvement in ISWT. For endurance performance, exercise times were similar across BMI categories at baseline. Although the magnitude of the improvement in ESWT performance was greater in the normal weight group, this was not statistically significant.
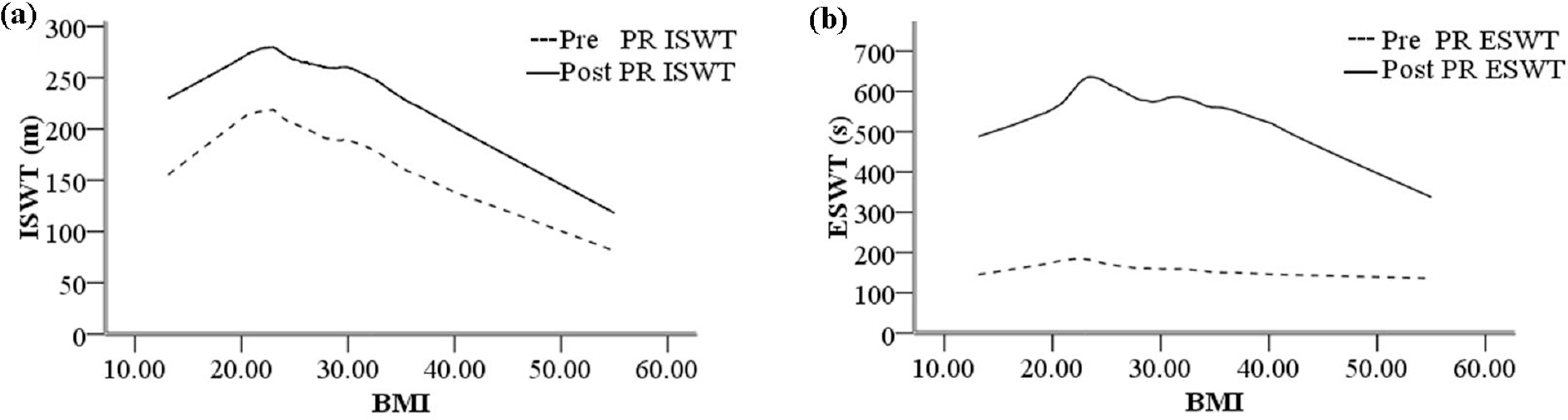
Graphs showing Loess regression curves pre- and post-pulmonary rehabilitation for (a) incremental shuttle walk test (ISWT) and (b) endurance shuttle walk test (ESWT).
Health-related quality of life
Mean CRQ score significantly improved in all four domains following the PR programme (p < 0.001 in all groups for each domain). Each of the BMI groups significantly improved the CRQ score, comparably. No significant difference in the proportion of patients achieving the clinically important change was seen in any domain (Table 2). Multivariate regression demonstrated no relationship between changes in the different domains of the CRQ and BMI category (dypnoea p = 0.390, fatigue p = 0.543, emotion p = 0.792, mastery p = 0.968).
Changes in exercise performance using incremental shuttle walk test (ISWT), endurance shuttle walk test (ESWT) and health status (CRQ-SR) domains in different BMI groups a

aSignificant clinical improvement also shown as percent of total patients in each group.
Extremes of BMI
A total of 33 very underweight (BMI < 18.5 kg/m2) and 15 extremely obese (BMI >40 kg/m2) patients were identified. Baseline ISWT was lower in the very underweight group compared with the less underweight group (176 m vs. 225 m; p = 0.043) and between the extreme obese and obese group (122 m vs. 185 m; p = 0.004). There were no differences in ESWT time or baseline health status scores.
Mean (SD) exercise performance improved significantly in both very underweight (ISWT: 73 (64) m, ESWT: 427 (411) s) and extremely obese (ISWT 49 (49) m ESWT 338 (320) s), with no difference compared with other BMI groups (ISWT: p = 0.657, ESWT: p = 0.525). Post hoc analysis comparing very underweight with extreme obesity also demonstrated no significant difference between groups (ISWT: p = 0.241, ESWT: p = 0.712). HRQOL showed improvement in all domains of BMI categories except the extreme obese group. In the extreme obese group no improvement was seen in the fatigue domain (0.29 ± 0.26; p = 0.290), a trend towards improvement in the emotion and mastery domains (0.51 ± 0.28; p = 0.054 and 0.52 ± 0.24; p = 0.094, respectively) but an improvement in dyspnoea (0.94 ± 0.28 p = 0.008).
Discussion
This study demonstrates that a walking-based PR programme is effective in improving clinical outcomes, across the BMI spectrum. As such patients of all body composition should be referred to a PR programme. In addition, obese patients present to PR with poorer exercise performance at baseline, despite better preserved lung function compared with normal weight patients. In very underweight patients both lung function and performance are worse at baseline, compared with normal weight patients.
This is the first study with a sufficiently large sample to compare PR outcomes across a full range of nutritional status, including the very underweight and extreme obesity. The results support the enrolment of patients with COPD to standard PR regardless of baseline BMI. Our data support previous studies that have also shown benefits in different BMI groups 15,16 but have been limited in the range of BMI categories studied.
The appreciation that nutritional depletion has a significant impact on morbidity and mortality in COPD has focused attention on the mechanisms and therapies in this subpopulation. However, our data show this to be only 5.5% of the PR cohort, whereas obesity is a more prevalent abnormality of body composition. Moreover, patients in the overweight groups had reduced exercise capacity despite relatively better preserved lung function and hence are more likely to be referred to PR. Whilst carrying extra weight is likely to be the predominant reason for the reduced ISWT performance, other comorbid disease may also contribute such as osteoarthritis and heart disease. Our observations are therefore of practical importance to PR programmes, suggesting that modifications of exercise programmes, such as water-based exercise, may not be needed.
Our findings are in keeping with those of Ramachandran et al., who noted reduced walking performance with obesity in COPD compared to normal weight. 15 In contrast, Ora et al. reported increased exercise capacity with cycling in obesity and COPD due to reduced dynamic hyperinflation. 18 These differences may be due to the modality of exercise used between weight supported (cycling) and weight unsupported (walking) exercise. A recent publication supports reduced walking performance in obese COPD but similar cycling performance. 4
In the underweight categories, poorer baseline exercise performance was seen only in the more severe underweight group (BMI < 18.5). This subgroup may represent a cohort of patients with more severe muscle wasting, which has previously been demonstrated to be associated with lower exercise capacity. 17 The association of muscle wasting with systemic inflammation and an intramuscular catabolic response could limit the training response in this cohort although recent mechanistic study suggests that cachectic patients retain the potential for skeletal muscle remodelling. 19 Our current study provides evidence that these patients are able to make comparable gains in walking capacity following high-intensity endurance training to normal weight patients.
BMI had no effect on improvement following PR in health status, except in the subgroup of extreme obesity. Improvements in all domains were seen, with similar proportions achieving the MCID for the CRQ-SR following PR. The effects of extreme obesity need to be interpreted carefully due to small numbers, but this group appeared not to improve in the fatigue domain. The lack of improvement in the fatigue domain may reflect the wider impact of obesity, possibly including unrecognised obstructive sleep apnoea and obesity hypoventilation.
This study did not measure weight following PR and so cannot investigate its effect on weight. Previous studies have shown modest gains in weight in the underweight population 20,21 ; to date the effect of PR on weight in the obese population has not been explored.
We acknowledge limitations to the interpretation of our data. This study was a retrospective analysis of an established PR database. However, data capture was prospectively recorded throughout the delivery of the PR service allowing a large number of patients to be included. Completers were limited to those with a recorded ISWT measurement after PR, rather than the number of sessions attended leading to a higher proportion of noncompleters than typically observed. BMI, rather than fat-free mass, was measured, and significant muscle wasting may be present in patients with COPD of normal or increased BMI, 22 and therefore we cannot determine whether alterations in lean or fat mass might have affected our observations.
Whilst we have demonstrated an equivalent effect of a walking-based PR programme across the BMI groups, we have not investigated the effects of resistance training or interval training across the BMI spectrum. Although the current walking (weight carrying)-based programme achieved important clinical changes in exercise performance in the obese population, it is not known whether weight supported exercise (cycling) could achieve superior results and requires further investigation.
In conclusion, this study demonstrates that walking-based PR provides benefits across the BMI spectrum and highlights the prevalence of obesity in patients with COPD. BMI should not be a criteria restricting access to rehabilitation services for patients with COPD.
Footnotes
Acknowledgements
The authors acknowledge all the members of the pulmonary rehabilitation department at Glenfield Hospital. The views expressed in this article are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.
This report/article presents independent research commissioned by the National Institute for Health Research (NIHR).