
Abstract
Lung transplantation is a well-established treatment option for selected patients with end-stage lung disease, leading to improved survival and improved quality of life. The last 20 years have seen a steady growth in number of lung transplantation procedures performed worldwide. The increase in clinical activity has been associated with tremendous progress in the understanding of cellular and molecular processes that limit both short- and long-term outcomes. This review gives a comprehensive overview of the current status of lung transplantation for the referring physician. It demonstrates that careful selection of potential recipients, optimisation of their condition prior to transplant, use of carefully assessed donor organs, excellent surgery and meticulous long-term follow-up are all essential ingredients in determining a successful outcome.
Introduction
Lung transplantation is an established therapy for selected patients with a range of chronic end-stage lung diseases. After universally poor results in the early attempts of this procedure, advances in surgical technique and development of effective immunosuppression have led to substantially improved outcomes and an exponential growth in the number of lung transplantation procedures performed worldwide. 1 –3 Recently, however, further growth in lung transplantation as a therapeutic option has been curtailed by the limitation of adequate donor lungs. Numbers of potential recipients on waiting lists have also increased. 4 In the last decade, there have been initiatives to standardise lung transplant candidate referral and listing criteria to ensure fair and appropriate use of the donor lung resources. Simultaneously, multiple strategies have been employed to try to increase donor lung availability.
Survival after lung transplantation has now steadily improved with patients transplanted in the 2000–2008 international cohort, expecting a median survival of 5.7 years. 1 Median survival in experienced, high-volume lung transplant programmes is significantly better than this. However, long-term survival is still disappointing when compared with that achieved for other solid organ transplants, most significantly limited by the development of chronic allograft rejection, which is manifested clinically as bronchiolitis obliterans syndrome (BOS). 5,6 This review will give a comprehensive overview of the current status of lung transplantation aimed at the referring physician.
Indications for the referral of candidates for lung transplantation
Since 1998, the International Society for Heart and Lung Transplantation (ISHLT) has published guidelines to help physicians identify lung transplant candidates. 7 Due to the significant risks involved, it is essential that transplantation is not performed too early but reserved until life expectancy is limited and quality of life significantly affected. However, late referral for transplant may result in patients deteriorating too quickly or developing comorbid conditions, making the individual unlikely to survive to reach transplantation. A summary of the current ISHLT guidelines for the selection of lung transplant candidates is in Table 1.
Disease-specific guidelines for listing of lung transplant candidates (adapted from Orens et al., 2006) 9
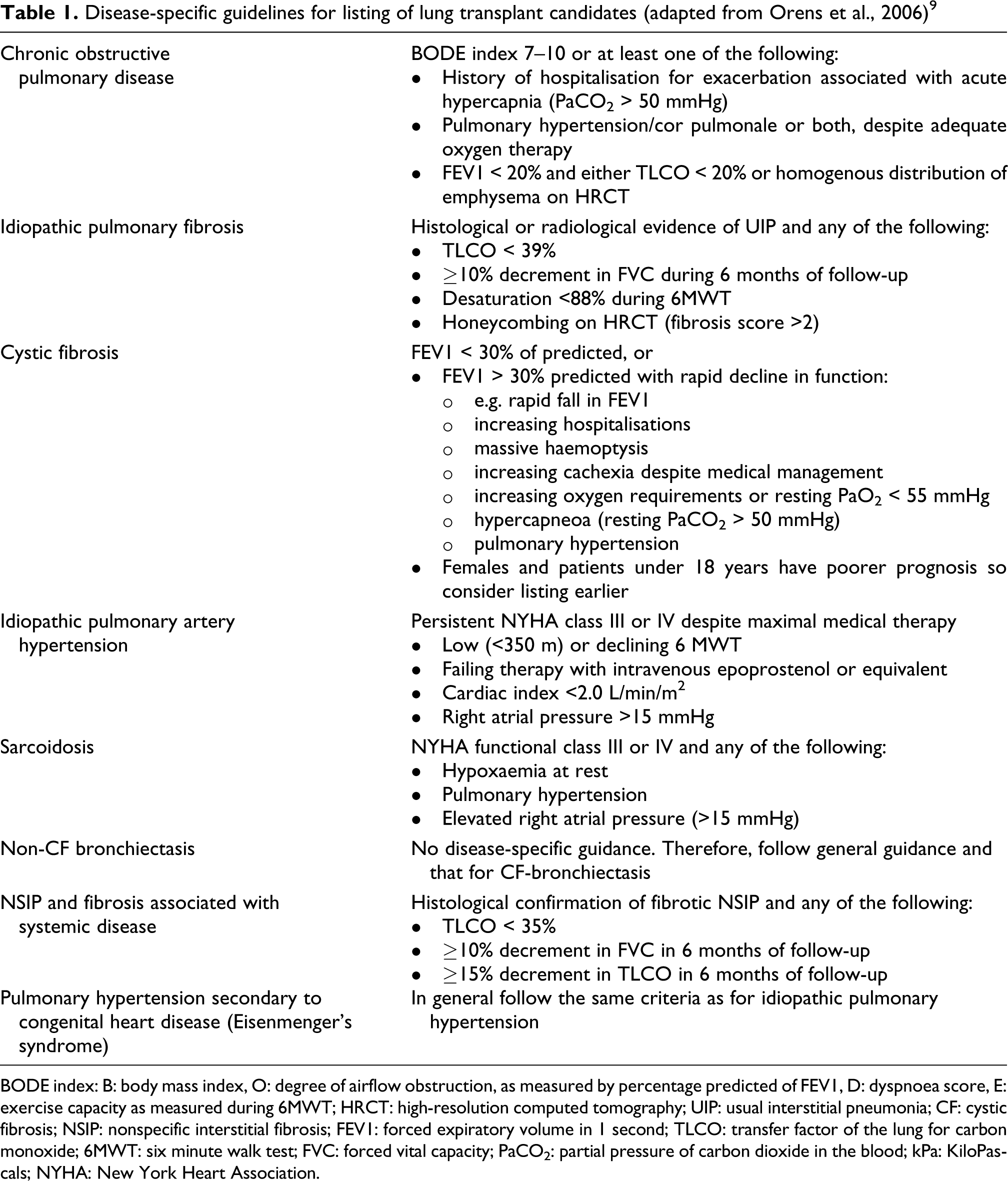
BODE index: B: body mass index, O: degree of airflow obstruction, as measured by percentage predicted of FEV1, D: dyspnoea score, E: exercise capacity as measured during 6MWT; HRCT: high-resolution computed tomography; UIP: usual interstitial pneumonia; CF: cystic fibrosis; NSIP: nonspecific interstitial fibrosis; FEV1: forced expiratory volume in 1 second; TLCO: transfer factor of the lung for carbon monoxide; 6MWT: six minute walk test; FVC: forced vital capacity; PaCO2: partial pressure of carbon dioxide in the blood; kPa: KiloPascals; NYHA: New York Heart Association.
General considerations in all patients referred for lung transplantation
Lung transplantation is reserved for those with chronic end-stage lung disease without the evidence of other significant end-organ dysfunction. 5 Referring physicians should ensure that the patients have received maximal medical therapy and yet show ongoing functional decline. Candidates should be functionally impaired (New York Heart Association class III or IV) but ideally still ambulatory; many centres set a minimum walk distance of 80 m to identify those who cannot tolerate the rigors of transplant surgery. The procedure is generally offered when the expected 2-year survival from the underlying disease falls to 50%. 8 At this point, the chances of surviving transplantation outweigh the risks of dying from the underlying disease, and given waiting times, may give patients the greatest overall pre-transplant survival while optimising chances of reaching transplantation. However, there are limitations to these criteria, including accuracy in predicting prognosis in individual patients and differences in waiting times for individuals dependent on numerous donor and recipient factors. Transplantation is rarely an option for acutely, critically ill patients, as universally these patients have poorer outcomes. 4 The absolute contraindications to lung transplantation are presented in Table 2.
Absolute contraindications to lung transplantation 9

Age
International criteria advocate age limit for transplantation to be 65 years for single-lung transplantation, 60 years for bilateral-lung transplantation and 55 years for heart–lung transplantation. 9 This is based on studies demonstrating worse outcomes in older patients. 10 Highly selected patients older than 65 years can undergo successful transplantation, but this is not an appropriate therapy for most patients in this category due to the presence of comorbidities. 11
Relative contraindications
Screening with coronary angiography is recommended in those at risk of coronary artery disease (candidates >50 years or those with identified risk factors). If coronary disease is identified and felt treatable with coronary artery stenting, then this may not automatically preclude transplantation. 12 Conditions including diabetes, hypertension and gastro-oesophageal reflux disease should also be optimised with specialist input where necessary. Careful attention should be paid to the resultant affect of these on renal function, left ventricular function and aspiration risk. 12
Nutrition
Obesity is associated with increased complications and difficulty with posttransplant rehabilitation, 13 and therefore most of the centres require body mass index (BMI) of <30 before active listing. Undernutrition is also associated with increased risk 14 ; efforts should be made to achieve a minimum BMI of 18.
Prior thoracic surgery and pleurodesis
Previous pleurodesis and thoracic surgery causing pleural adhesions make native lung removal at the time of transplantation more difficult and increase intraoperative bleeding risk. Experienced centres review cases on an individual basis. 9,15
Collagen vascular/connective tissue disease
These patients remain controversial due to the concerns that extrapulmonary manifestations of disease might increase the risks of complications, particularly the increased oesophageal dysmotility associated with scleroderma. However, several studies have shown that in selected patients with scleroderma, 1- and 2-year survival is comparable with other groups. 16 Such patients require very careful assessment.
Osteoporosis
Significant osteoporosis may be a relative contraindication to transplantation due to the risk of painful and debilitating vertebral fractures postoperatively. All patients should be screened with bone densitometry and treatment initiated where appropriate. 17
Current use of corticosteroids
All attempts to discontinue or reduce the daily dose of prednisolone to ≤20 mg should be made, particularly if found to have little impact on disease decline. Attention should be paid to steroid-associated morbidity, especially obesity, osteoporosis and diabetes. 9
Colonisation with pan-resistant organisms, non-tuberculous mycobacteria or fungi
Chronic colonisation of the airway is a feature of cystic fibrosis (CF) and other septic lung diseases. Although patients with CF with pan-resistant strains of pseudomonas have lower 1- and 5-year survival rates compared with other patients with CF, they are comparable with other patient groups. 8 The issue of pretransplantation infection with Burkholderia cepacia complex (BCC) is discussed in the Cystic Fibrosis section of disease-specific guidelines for transplantation. Colonisation with nontuberculous mycobacteria is not an absolute contraindication. Careful consideration should be given to whether it is appropriate to attempt eradication with medical treatment prior to active listing for transplantation. One case series suggested a perioperative mortality of 45% in patients with fungal infection who have developed mycetomas, due to soiling of the pleural space at surgery. Therefore, a cautious approach to these patients is appropriate. 18
Preformed circulating antibodies
Donor-specific antibodies in the recipient circulation are associated with accelerated chronic graft dysfunction and worse long-term survival. 19 It can be difficult to find suitable donors for recipients with high levels of circulating preformed antibodies to human leukocyte antigens (HLAs), resulting in prolonged waiting times.
Disease-specific considerations for lung transplantation listing
Chronic obstructive pulmonary disease (COPD) and α1-antitrypsin deficiency account for nearly half of all the patients undergoing lung transplantation. 20 Other causes include idiopathic pulmonary fibrosis ((IPF) 19%), CF (17%) and idiopathic pulmonary hypertension (<5%). Other indications including non-CF bronchiectasis and sarcoidosis account for a few percentage of all lung transplantations. 20 The latest ISHLT disease-specific guidelines are summarised in Table 1. However, much contention surrounds estimates of prognosis in disease-specific cohorts, and these may have further limitation in application to individual patients. 21,22 Therefore, not all patients who meet the criteria require immediate listing for transplantation and, conversely, patients outside the criteria but who are declining rapidly may warrant listing. 22,23
Chronic obstructive pulmonary disease
All medical management should be optimised including long-term oxygen therapy, nutrition and pulmonary rehabilitation prior to referral. 7 Prolonged survival is possible in patients with severe airflow obstruction and therefore predicting prognosis and timing of transplantation referral can be challenging. 24 –26 Recent studies show the body mass, airway obstruction, dyspnoea and exercise capacity (BODE) index to be superior to forced expiratory volume in 1 second (FEV1) at predicting mortality in COPD. 27 However, its application to the population being considered for lung transplantation is not yet verified. 28
Idiopathic pulmonary fibrosis
Histological confirmation of usual interstitial pneumonia (UIP) on biopsy and radiological features of IPF on high-resolution computed tomography (HRCT) with significant honeycombing and fibrosis is associated with poorer prognosis. 29,30 Baseline TLCO (Transfer factor of the Lung for Carbon Monoxide) < 39% combined with HRCT fibrotic scores was shown to be the best predictor of a 2-year mortality. 31 The Newcastle group demonstrated that a more rapid rate of disease progression was associated with higher mortality while awaiting transplantation. 32 This suggests that the rate of decline may be a better indicator for referral and listing than absolute values of Total Lung Capacity or TLCO. This patient group has the highest mortality rate while on the transplant waiting list, and this has led to recommendation by the ISHLT that patients with typical UIP should be referred for transplantation at the time of diagnosis. 9,33 The intention is not to list all patients immediately but to allow close follow-up and sufficient time to address potential barriers.
Nonspecific interstitial fibrosis
A pathological or radiographic pattern of nonspecific interstitial fibrosis (NSIP) is usually associated with markedly better prognosis than UIP, with some reports indicating median survival times of 5–8 years. 34 However, it is likely that this represents a heterogeneous group. Those with predominantly fibrotic features are likely to have a poorer prognosis. Those patients with NSIP with a TLCO of <35% predicted and/or a decrease in a TLCO of >15% over 6 months have a median survival of 2 years, 35 closely resembling UIP. Therefore, physicians should not be falsely reassured by a histological diagnosis of NSIP, if there is a clinical evidence of decline.
Cystic fibrosis
Patients with CF often suffer from chronic colonisation of the airways with pan-resistant organisms, the commonest being Pseudomonas aeruginosa. Studies have demonstrated 1- and 5-year survival rates of 87% and 58%, respectively, in patients with CF with pan-resistant organisms versus 97% and 86%, respectively, in those without pan-resistant strains. 36 However, these survival rates are comparable with other non-CF groups undergoing lung transplantation. In relation to pretransplantation infection with BCC, many centres described notable decrease in 1-year survival, that is, around 50–67%. 37,38 Further subgroup analysis revealed that excess mortality appears to relate specifically to Burkholderia cenocepacia infection. Most transplant centres worldwide consider infection with this subtype of BCC a contraindication, but will consider those with other strains of BCC. 39,40
Non-CF bronchiectasis
Patients with severe bronchiectasis are a heterogeneous group, and little is known regarding the factors predicting prognosis. Attention should be paid to the characterisation of colonising organisms, particularly atypical mycobacteria, when referring for transplantation. Transplant centres have generally followed similar criteria as for CF-bronchiectasis when listing for transplantation. 7
Sarcoidosis
Studies suggest that those with symptomatic breathlessness (NYHA class III and IV), an FVC (Forced Vital Capacity) < 50% predicted and/or FEV1 <40% predicted, have a poorer prognosis and therefore suggested these as prompting referral for transplantation. 8 In contrast, other studies identified elevated pulmonary artery pressure, hypoxaemia and elevated right atrial pressure (>15 mmHg) as predictors of short-term mortality. 41 The current sarcoidosis-specific referral guidelines (Table 1) take into account both sets of findings. 9,42 Care must be taken to exclude significant extrapulmonary manifestations of sarcoidosis.
Idiopathic pulmonary artery hypertension
With the introduction of long-term pulmonary vasodilator and other targeted therapies, transplantation for idiopathic pulmonary artery hypertension (iPAH) has fallen from approximately 10.6% for all thoracic transplantations in 1990 to 3.6% in 2001. 8 The widespread use of these medications has revolutionised management, and 5-year survival of patients treated with IV epoprostenol is now around 55% compared with 28% of historical controls. 43,44 However, not all patients respond similarly, and those that remain in functional class III or IV despite maximal medical treatment have a 3-year mortality of only 33% compared with 88% for those in class I or II. 45
Secondary pulmonary hypertension and Eisenmenger’s syndrome
Pulmonary hypertension occurs secondary to multiple conditions including thromboembolic disease and collagen vascular disease. In general, these patients have poorer prognoses, and the same criteria as for iPAH should be used for transplantation referral. Overall, patients with Eisenmenger’s syndrome tolerate similar levels of pulmonary artery hypertension but with better cardiac function translating into improved overall survival. 46
Combined lung and other organ transplantation
In some multisystem disorders, patients may present with multiple organ failure and may be considered for multiorgan transplantation, predominantly lung–liver transplants in selected patients with advanced CF. In general, patients must meet all the criteria for each organ transplant. 44
Criteria for identifying suitable donor lungs
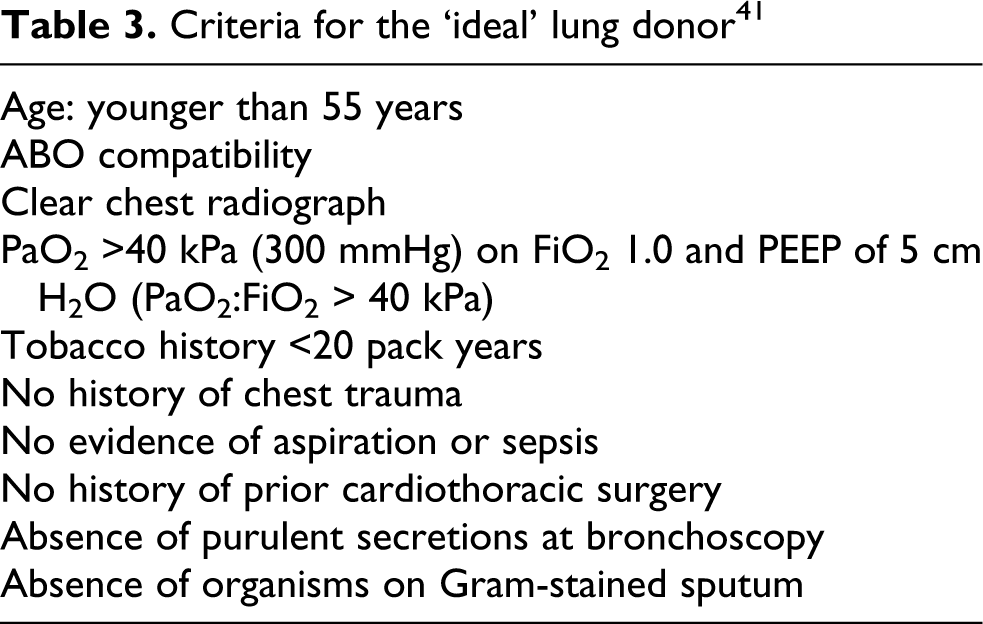
There is an ever-increasing gap between suitable donor lungs and the number of recipients requiring lung transplantation. 47 In the United Kingdom, 14% of lung transplant candidates die while awaiting transplantation, while a further 11% are removed due to deterioration. 48 The critical factor is a shortage of appropriate lung donors. Despite the significant need, only 24% of multiorgan donors in the United Kingdom are used as lung donors. 48 Reasons cited include the relatively strict criteria for acceptable lung donors as summarised in Table 3. These criteria were developed as best practice but are not evidence based. Therefore, a number of initiatives have been developed with the aim to extend the donor pool, which are discussed below. 49,50
Criteria for the ‘ideal’ lung donor 41
Accepting ‘marginal’ or less than ideal donors
Some centres accept donors who do not fulfil 1 or 2 of the ideal criteria. Many centres are willing to use donors aged up to 60 years, if they otherwise fulfil the criteria. 51 Several case series have shown acceptance of chest x-ray abnormalities including ‘minor atelectasis’, with no adverse effect on outcomes. 52,53 Several case series have shown no adverse events when accepting donors with a smoking history slightly greater than 20 pack-years. 52 However, no long-term data have been presented and there is a concern about cancer transmission risk. 54,55 In practice, the risk associated with the use of any specific donor has to be weighed against the risk of not receiving a donor lung at all and dying while on the waiting list. 50 This has led to efforts to assess the individual risk adversity of patients listed for lung transplantation to fully inform them of the risks of accepting lungs from donors with particular features but also the possible consequences of excluding them as well.
Aggressive medical management of donor
Many donors are excluded based on the failure to meet the PaO2:FiO2 (Partial pressure of Oxygen in the Blood : Fraction of Inspired Oxygen) criteria. However, the lungs are susceptible to interstitial oedema particularly in the context of brainstem death and many feel these changes are reversible, making the underlying lung suitable for transplantation. Straznicka et al.
56
described the management of 27 unacceptable donors with a mean Pa
Donation after circulatory death
Donation after circulatory death (DCD) occurs in donors who undergo cardiac arrest on cessation of futile life supporting treatment. 57 After 5 minutes, the lungs are reintubated, appropriate organs removed and prepared for transplantation. DCD is only performed on donors who meet conventional criteria. Numbers receiving donation by DCD remain small, but evidence from the North American UNOS database suggested that patients had an overall 2-year survival of 87% after DCD (similar to conventional donation after brainstem death). 58
Ex vivo lung perfusion
Ex vivo lung perfusion (EVLP) involves slow perfusion of isolated ex vivo donor lungs with a physiological extracellular electrolyte solution designed to give oncotic pressure to maintain flow through the organ, without developing pulmonary oedema. 59 This can be performed for several hours before the lungs are reevaluated by measuring gas exchange while mimicking conditions of ventilation. EVLP has been used to improve the function of marginal donors and to assess the function in DCD lungs. A recent case series with results from 23 donors undergoing 4 h of EVLP showed no significant difference in 72-h primary graft dysfunction (PGD), length of intensive care unit/hospital stay or 30-day mortality. 60
Medical management while awaiting lung transplantation
Medical management while awaiting lung transplantation is an important factor in survival to transplantation. This involves active treatment to keep the disease stable and reassessment to ensure that their disease, treatments or comorbidities do not alter significantly to change the risks associated with transplantation. In general, studies recommend review by the patients’ local physician at least every 3 months. 5 Common aspects of management include review of medical treatments to ensure benefit is outweighing potential toxicity, judicious use of antibiotics and steroids, monitoring nutrition and renal function. Those with CF, bronchiectasis and long-standing colonisation require quarterly assessment of their organisms to ensure tailored antimicrobials are still appropriate and that there is no emergence of atypical organisms. 61 If the patient deteriorates to such an extent that they would be unlikely to survive a transplant operation, then this needs to be recognised. Similarly, being accepted on to a transplant waiting list should not preclude appropriate palliation of patient’s symptoms while waiting.
Options for transplantation
Lung transplant procedures include single-lung, bilateral-lung and combined heart–lung transplantation. Lobar transplants from living donors are performed in some centres and may be unilateral but are normally bilateral (lobes donated from two living donors) and are applicable to smaller recipients. 62,63 Two lungs can be removed from most donors, but there are situations in which one is damaged irretrievably while the other is usable. The decision on which procedure to perform depends upon the pretransplant diagnosis.
Single-lung transplantation can only be performed if the contralateral lung can be left in the recipient, that is, in the absence of contralateral sepsis. Single-lung transplantation is ideal for restrictive lung disease as both ventilation and perfusion are directed towards the transplanted lung and gives excellent functional outcomes and improved survival. 6
Septic lung disease (e.g. CF) means the native lung cannot be left in place; all the infected lung tissue should be removed. The standard choice would be bilateral-lung transplantation, but heart–lung transplantation with domino donation of the recipient’s heart is used in some centres, for which the outcome is equally good. 6,64 Using domino procedure minimised donor heart wastage, but there is a disadvantage to the pulmonary recipient, who receives a denervated organ which is prone to accelerated graft coronary disease. 6,64
COPD is the commonest indication for lung transplant worldwide; both single-lung and bilateral-lung transplantation can be considered. 1 Bilateral-lung transplant is required when the contralateral lung may be a source of infection (e.g. from colonisation of bullae by Aspergillus). 65 Most centres now favour bilateral-lung transplantation in COPD due to enhanced survival and functional capacity when compared with single-lung transplantation. 65,66 Single-lung transplantation is now rarely performed in COPD due to native lung hyperinflation and mediastinal shift towards the transplanted lung, which can limit transplanted lung function. 66 Avoiding an open surgical procedure by performing bronchoscopic lung volume reduction surgery (LVRS) in advanced COPD may reduce overall complications and include candidates with more severe disease or cardiovascular issues prohibiting an open thoracotomy. 67 LVRS generally offers less functional benefit than transplantation, but is significantly less morbid, and can offer some functional benefit without the need for transplantation. 67
For pulmonary vascular disease, heart–lung transplantation is performed if there is irreparable congenital heart disease, left ventricular dysfunction or significant coronary disease. If the heart can be retained, bilateral-lung transplantation can be performed. 68 Single-lung transplantation is rarely performed due to higher early mortality, worse functional result and the risk of a severe ventilation–perfusion mismatch, if obliterative bronchiolitis develops in the transplanted lung. 68
Postoperative management
Immediate complications: Primary Graft Dysfunction
Primary Graft Dysfunction (PGD) is a clinical diagnosis defined as a significant impairment of oxygenation together with diffuse radiological infiltrates consistent with pulmonary oedema in the lung allograft within the first 72 h posttransplant.
69
PGD is a form of acute lung injury similar to adult respiratory distress syndrome. Diagnosis requires exclusion of other causes including hyperacute rejection, venous anastomotic obstruction, cardiogenic oedema and pneumonia.
70
PGD is the primary cause of morbidity and mortality in the immediate postoperative period posttransplant.
71
Impaired lung function and an increased risk of developing chronic rejection are associated with severe PGD. The reported incidence is 12–15%, accounting for 30% of all 30-day mortalities.
72
Histologically, diffused alveolar damage and alveolar oedema are seen, with eventual development of hyaline membrane and endothelial cell detachment. PGD severity is graded based on the Pa
Early complications: Acute Cellular Rejection
Acute cellular rejection (ACR) following lung transplantation is defined histologically by perivascular or peribronchiolar mononuclear inflammation. 80 ACR is thought to be due to the alloreactive T-cells responding to donor antigen. 81 However, humoral rejection also occurs, which is characterised by the presence of antibody to donor HLA. 81 Also, environmental stimuli, including pulmonary infections, interact directly with the lung allograft and contribute to the development of rejection. 80 ACR can present any time after the first week and is commonly seen in the first year posttransplant. 80 ACR affects up to 40% of patients in the first month posttransplant, and its incidence markedly declines after 6 months. 1 ACR presents with nonspecific symptoms such as fever, cough and dyspnoea and may be associated with infiltrates or pleural effusions on chest x-ray. Hypoxia and decline in spirometry may occur. 82 Ground-glass opacities, septal thickening and pleural effusions on chest computed tomography (CT) suggest acute rejection. 83 Transbronchial biopsy is required for a firm diagnosis. 84 Rejection may be clinically silent and up to 20% of cases are discovered unexpectedly during surveillance biopsies, which are commonly employed in the first year posttransplant. 85 ISHLT grading of acute rejection is from A0 (no evidence of rejection) to A4 (severe acute rejection). 86 Early acute rejection is treated with pulsed IV methylprednisolone followed by an augmented dose of oral corticosteroids tapered over 1 month. 80 Most patients respond rapidly with improvements seen as early as 24 h after the treatment is commenced. Acute rejection occurring after the first month can be treated adequately with augmented oral corticosteroids. 80 Treatment of refractory or recurrent rejection is more challenging. Repeating the pulsed steroids and altering the baseline immunosuppressive regimen, such as switching calcineurin inhibitors, or substituting azathioprine with mycophenolate mofetil (MMF) represent some of the options. 87 More aggressive therapy includes the use of cytolytic agents, including polyclonal antithymocyte globulin and anti-interleukin (IL)-2 receptor antagonists. 88 The frequency and severity of acute rejection episodes are recognised as predisposing to chronic allograft rejection, the main cause of late mortality. 80
Antibody-mediated allograft rejection is increasingly recognised in lung transplantation. 89 With the development of improved antibody detection techniques, donor-specific antibodies have been implicated in lung, renal and heart transplantation. 90 Treatment options for humoral rejection include intravenous immunoglobulin, plasmapheresis or rituximab. 80 The role of C4d complement immunostaining in lung capillary beds has been postulated as a marker of antibody-mediated rejection. 91 However, the prognostic relevance of this marker remains unproven as yet.
Early complications: infection
Infectious complications remain a major cause of morbidity and mortality in lung transplant recipients. The increased susceptibility of the pulmonary allograft to infection is due to its direct contact with microbes by inhalation, concurrent immunosuppression and impaired clearance mechanisms. 92
Resistant and nosocomial causes of bacterial pneumonias, especially Staphylococcus and Pseudomonas, are prevalent because of frequent antibiotic use and hospitalisations. The Newcastle group has shown an association between de novo Pseudomonas colonisation and BOS development. 93 B. cenocepacia infection carries a high risk of severe sepsis. 94 Mycobacterium tuberculosis infection may occur due to reactivation, transmission by transplantation or nosocomial infection. 92
Cytomegalovirus (CMV) frequently presents in the first 4 months of posttransplantation. 95 CMV predisposes to secondary bacterial/fungal infection and is a risk factor for BOS. 96 All seropositive recipients are at risk, whereas seronegative recipients transplanted with a seropositive donor lung are at the highest risk of developing infection. 95 Manifestations of CMV infection range from asymptomatic to severe invasive disease, starting with pneumonitis and later disseminating. 97 A rising viral titre on polymerase chain reaction is diagnostic. 92 Treatment is usually with ganciclovir or valganciclovir and anti-CMV immunoglobulin. 98
Reactivation of Epstein-Barr virus (EBV) occurs in a significant number of patients posttransplant, and EBV is the major risk factor for the development of posttransplant lymphoproliferative disease (PTLD), which has an incidence of 1–20%. 99 PTLD is a heterogeneous group of lymphoproliferative disorders ranging from reactive polyclonal hyperplasias to aggressive non-Hodgkin’s lymphomas. 99 Chest CT may show infiltrates, adenopathy or masses. 100 Treatment involves decreasing immunosuppression and starting ganciclovir/valganciclovir. 101 Rituximab may be indicated if the lymphoproliferative cells are CD20 positive on histology. 100 The liver and the bowel are also common sites for PTLD development. 97 Any patients with lung transplantation presenting with persistent weight loss and unexplained abdominal symptoms must be investigated to exclude this possibility.
Aspergillus and Candida cause 80% of fungal infections in patients with lung transplant. 97 Aspergillus can cause colonisation, infections of the bronchial anastomosis and tracheobronchial tree, invasive pneumonias and disseminated disease. 102 Treatment is with amphotericin or voriconazole and surgical resection of affected areas in refractory cases. 102 Chest CT scan, bronchoscopy and Aspergillus galactomannan assay may aid diagnosis. 103
Pretransplant immunisation is performed for influenza, 2009 influenza A (H1N1), Streptococcus pneumonia, tetanus and hepatitis B. 97 Routine postsurgical broad-spectrum antibiotic prophylaxis targeting cultures from donor lungs or known positive recipient cultures is performed. CMV prophylaxis with ganciclovir or valganciclovir is administered to patients at risk, with data showing that a 12-month prophylactic regimen is superior to shorter-duration regimens. 104 Cotrimoxazole prophylaxis can prevent Pneumocystis pneumonia, with effects against Toxoplasma, Nocardia and Listeria. Antifungal prophylaxis in the form of aerosolised amphotericin-B immediately postoperative, and itraconazole or voriconazole for 1–12 months postoperative is commonly used. 105
Immunosuppression
Optimal immunosuppression is required to maintain a long-term graft survival and keep the balance between infection and rejection. Immunosuppression therapies target multiple immune pathways to decrease both acute and chronic allograft rejection. 106 The required high load of immunosuppressants adds a cumulative risk of nephrotoxicity, bone marrow depression and malignancy. 106
Induction immunosuppressive agents are used in some centres to deplete the recipient immune system in the immediate posttransplant period to decrease early interaction between the recipient immune cells and donor allograft antigens to prevent acute rejection. 107,108 Induction therapy consists of a brief regimen of intravenous antilymphocytic agents including polyclonal anti-T-cell preparations (antithymocyte globulin) and monoclonal antibodies, aimed at lymphocyte surface molecules including CD3 (OKT3), IL-2R/CD25 (basiliximab, daclizumab) or CD52 (alemtuzumab). 107 OKT3 prevents T-cell activation. Daclizumab and basiliximab inhibit T-cell proliferation and differentiation. Alemtuzumab causes leukocyte depletion.
Maintenance immunosuppressive therapy is based on a triple regimen composed of a calcineurin inhibitor (ciclosporine or tacrolimus), an antimetabolite (azathioprine or MMF) and corticosteroids. 109 Mammalian target of rapamycin (mTOR) inhibitors, for example, sirolimus and everolimus, may replace the calcineurin inhibitor or antimetabolite. 109 A randomised multicenter study showed that BOS-free lung transplant recipients had significantly smaller decline in FEV1 and experienced fewer acute rejections when treated with everolimus compared with azathoprine. 110 Everolimus has been shown to give a significant survival benefit compared to those treated with MMF. 111
Cyclosporine and tacrolimus inhibit calcineurin, thereby decreasing IL-2 production and reducing T-cell activation/proliferation. Azathioprine and MMF are antimetabolites, which deplete lymphocytes. Sirolimus and everolimus are mTOR inhibitors, which arrest T-cell growth. Corticosteroids suppress prostaglandin synthesis, reduce histamine/bradykinin release, decrease vascular permeability and downregulate cytokines. 112
Large-airway complications
Bronchial stenosis is the commonest airway complication and is seen within 2–9 months of posttransplantation. 113 It may be asymptomatic or present with declining expiratory flows, stridor, dyspnoea, cough or postobstructive pneumonia. 113 Flexible bronchoscopy is required for diagnosis. Management is with endoscopic balloon bronchoplasty and stent placement, if it recurs. 114
Exophytic granulation tissue can cause significant airway obstruction. Concurrent infection with Aspergillus makes it refractory to therapy and increases morbidity. 88 Debridement by cryotherapy, laser vaporisation or argon plasma coagulation can be effective in these circumstances. 88 In single-lung recipients, the native lung can be the source of pulmonary complications including neoplasms, infections and recurrence of primary disease. 113
Late complications: Bronchiolitis Obliterans Syndrome
Long term survival following lung transplantation is relatively poor compared to other solid-organ transplants being restricted to a mean of 5 years, mainly due to the development of Bronchiolitis Obliterans Syndrome (BOS). 1 BOS, which has a prevalence of 40–50% at 5 years posttransplantation, is the clinical manifestation of chronic allograft rejection, characterised by progressive, irreversible decrease in lung function as measured by the FEV1 from a stable posttransplant baseline value. 115 Staging of the disease (BOS level 0–3) depends on the magnitude of FEV1 reduction. 116 BOS is characterised histologically as obliterative bronchiolitis, with inflammation and fibrosis in small- and medium-sized airways causing airflow obstruction. 115 The clinical course of BOS is variable, with a median time from transplantation to diagnosis of 16–20 months and a median survival after onset of 3–4 years. 115 The pathogenesis of BOS is believed to be initiated by repeated epithelial injury from both alloimmune and nonalloimmune mechanisms, leading to a final common pathway of airway remodelling. 117 Damage and failure to reestablish an intact airway epithelium following injury is thought to contribute to irregular repair and airway remodelling. 117 Risk factors for BOS include ACR, PGD, respiratory infections, HLA mismatching and gastro-oesophageal reflux disease. 118 BOS is variable in its clinical presentation; initial symptoms are often nonspecific. As the disease progresses, patients develop exertional dyspnoea, cough and wheezing and can suffer frequent respiratory tract infections. 115
Most therapies work by an anti-inflammatory rather than antifibrotic effect, therefore early detection and prevention of BOS is emphasised. Augmentation of immunosuppression with antilymphocyte antibodies, cyclophosphamide, methotrexate, extracorporeal phototherapy and total lymphoid irradiation has shown only limited success. 117 These therapies may slow progression, but do not reverse disease, and can increase infection risk. Also, mTOR inhibitors have been used to stabilise lung function in BOS. 117 The macrolide antibiotic azithromycin has immunomodulatory effects; it has been shown to prevent BOS development and improve FEV1 in some patients with established BOS. 119 Gastroesophageal reflux disease has been implicated in the aetiology of BOS, and intervention with early gastric fundoplication may offer some protection. 120 Retransplantation for advanced BOS can be successfully performed, but the lack of donor organs means that this option is limited to few selected patients. 117
Future developments
Two studies have reported a novel technique in a rat model describing the in vitro regeneration of lungs which had been decellularised and their subsequent successful transplantation. 121,122 This is one of the initial steps in the ultimate goal of generating fully functional human lungs in vitro, which would solve the problems of donor lung shortage and tolerance.
Conclusions
Lung transplantation offers a realistic treatment option for improved survival and improved quality of life for selected patients with end-stage lung disease. The last 20 years has seen tremendous progress in improving outcomes and understanding of the cellular and molecular processes that limit outcomes. Careful selection of potential recipients, optimisation of their condition prior to transplant, use of carefully assessed donor organs and meticulous long-term follow-up are all essential ingredients in addition to excellent surgery in determining a successful outcome. New developments in donor lung optimisation may see that the availability of this therapy increases, thus allowing more of those who are suitable candidates to benefit in the future.
Footnotes
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.