
Abstract
The unplanned transfer of patients from long-term acute care hospitals (LTACHs) back to acute facilities disrupts the continuity of care, delays recovery and increases the cost of care. This study was performed to better understand the unplanned transfer of patients with pulmonary disease. A retrospective analysis of data obtained for quality management in a cohort of patients admitted to an LTACH system over a 3-year period. Of the 3506 patients admitted with a pulmonary diagnosis studied, 414 (12%) underwent 526 unplanned transfers back to an acute facility after a median LTACH length of stay (LOS) of 45 days. Mechanical ventilation via tracheostomy was used in 259 (63%) patients admitted to the LTACH with a pulmonary diagnosis. The commonest reasons for unplanned transfers included acute respiratory failure, cardiac decompensation, gastrointestinal bleed and possible sepsis. Over 50% of patients had LOS at the LTACH between 4 and 30 days prior to the unplanned transfer. Patients with an LOS <3 days prior to transfer were more likely to be transferred around the weekend. In all, 32% of patients died within a median of 7 days of transfer back to the acute facility. Thirty-day mortality following unplanned transfer appeared independent of organ system involved, attending physician specialty/coverage status, nursing shift or transferring LTACH unit. Unplanned transfers disrupting continuity of care remain a significant problem in patients admitted to an LTACH with a pulmonary diagnosis and are associated with significant mortality. Strategies designed to reduce cardiopulmonary decompensation, gastrointestinal bleeding and possible sepsis in the LTACH along with additional strategies implemented throughout the health care continuum will be needed to reduce this problem.
Introduction
Patient readmission to an acute hospital facility following discharge to a long-term acute care hospital (LTACH) is an important quality of care issue as unplanned transfers are associated with significant morbidity, mortality and cost. LTACHs 1,2 enable referring acute care hospitals efficiently manage length of stay (LOS). An increasing number of patients are discharged to LTACHs for management of a pulmonary-related problem 1,3 such as an acute exacerbations of chronic pulmonary disease, tracheostomy management, weaning from invasive or noninvasive mechanical ventilation, pulmonary rehabilitation and end-of-life care. 4 The recovery trajectory of patients, due to an unanticipated escalation in medical care, is unpredictable and up to 23% of all patients admitted to LTACHs require an unplanned transfer back to an acute facility. 5 This study was undertaken to better understand the reasons for and outcomes of unplanned transfers of patients with pulmonary-related problems from an LTACH back to acute facilities.
Materials and methods
Study site
A retrospective observational cohort study performed at an LTACH system in Massachusetts comprised of a single 150-bed freestanding unit (Unit A) in southeastern Massachusetts (15 miles south of Boston) and two 20-bed satellite units co-located in Boston acute care hospitals (Unit B in a tertiary referral center and Unit C in a community acute care hospital). Comprehensive medical and rehabilitative care is delivered at the LTACH system to patients with complex medical diseases 6 with an average LOS of 25 days. There is focus on weaning from mechanical ventilation, noninvasive mechanical ventilation, management of multiple comorbidities and specialized wound care. Physical, occupational and speech therapy along with nutritional support are all available. Medical coverage is provided by either internists or pulmonary, critical care physicians, assisted by midlevel providers (physician assistants and nurse practitioners). A physician is available on-site at all times in Unit A. In Units B and C, a system of coverage is in place that utilizes either an on-site physician or the host hospital medical staff is available as needed to provide physician coverage during off-hours. A rapid response and code team is available at all sites. Routine subspecialty consultation is available. The LTACH is not staffed or equipped to manage patients who require intensive care unit (ICU) level of care (such as suspected new onset myocardial ischemia, hypotension requiring vasopressors, evaluation of new onset abdominal pain and acute blood loss requiring workup). Computed tomography (CT) scans or emergent subspecialty consultation (other than pulmonary and physical medicine and rehabilitation consultation) are also not available on-site.
Study population
The following inclusion criteria were used: (1) admission to Unit A, B or C from an acute facility between 1 January, 2005 through 31 December, 2007, (2) having a primary pulmonary diagnosis at the time of LTACH admission and (3) undergoing an unplanned transfer. The last date of follow-up was 31st December, 2009. The study was approved by the LTACH Institutional Review Board and the need for informed consent waived.
LTACH admission criteria
The LTACH uses the National Association of Long-Term Hospitals (NALTH)® screening criteria for admission of patients with pulmonary problems. In brief, these criteria include the following: mechanical ventilator dependence, ability to wean from mechanical ventilation, presence of comorbid diseases, prior episodes of prolonged mechanical ventilation, abnormal gas exchange, postsurgical respiratory compromise, need for respiratory care following weaning from mechanical ventilation or pneumonia with ongoing need for respiratory monitoring. The overall goal of the criteria is to identify patients likely to benefit from an average LOS of 25 days for management of complex pulmonary disease and multidisciplinary rehabilitation.
Definition of unplanned transfer
An unplanned transfer was defined as the transfer of a patient from LTACH to acute facility for either critical care or management of an escalating medical or surgical problem. Planned transfers were excluded.
Unplanned transfer data collection
All unplanned transfer data are recorded by the quality management department. The medical reasons for unplanned transfer were not predefined and were extracted from the medical record by a trained registered nurse. This database served as the primary data source. (We did not have access to the medical records in the referring acute facilities.) The following data were abstracted from the database and recorded in an Excel® spreadsheet: demographic and clinical information, LOS, all pertinent unplanned transfer data (e.g. diagnosis necessitating acute transfer back to acute facility, day of week, nursing shift and transferring provider), referring acute facility and final disposition of the transferred patient. The medical reason for each unplanned transfer was rechecked by two of the investigators (JG and AW). The 30-day mortality data were obtained from the LTACH medical record and the Social Security Death Index.
Statistical analysis
All data were imported into SAS (version 9.1, SAS Institute Inc., Cary, NC, USA). Categorical variables were compared using either χ 2 test or Fisher’s exact test. Continuous variables were analyzed using the Wilcoxon two-sample test. Statistical significance was assumed when p < 0.05.
Results
LTACH admission and discharge data
Of the 3506 patients originally admitted from a referring acute facility with a pulmonary diagnosis, 414 (12%) subsequently required an unplanned transfer and comprised the study population. There were 526 unplanned transfers recorded in the cohort as some patients were transferred more than once. The median LTACH LOS prior to an unplanned transfer was 45 days. The unplanned transfer rate for all patients (any diagnosis) admitted to the LTACH was 22% and was 34% for those admitted without a pulmonary diagnosis.
Admission characteristics
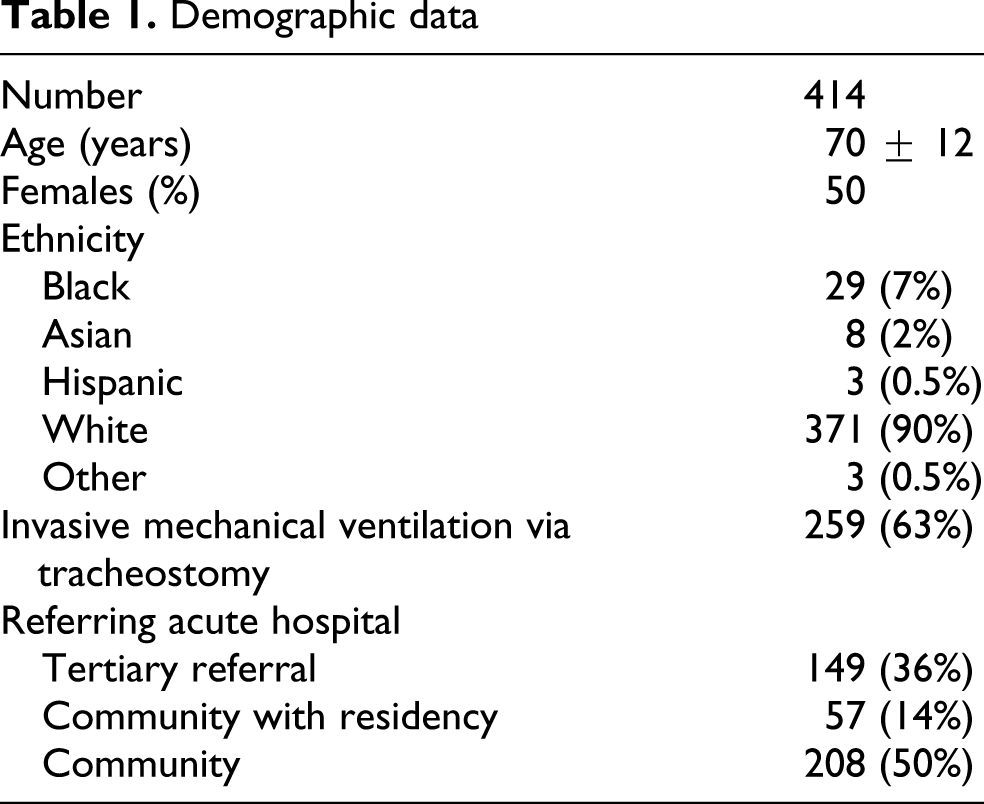
Demographic and patient characteristics of the study population are shown in Table 1 . The pulmonary diagnoses for patients admitted included pulmonary edema, chronic obstructive pulmonary disease (COPD), pneumonia, interstitial lung disease, pulmonary neoplasm and asthma.
Demographic data
Unplanned transfer data
Analysis of the LOS at the LTACH prior to the unplanned transfer showed 34 (6%) patients had LOS of 0–1 days; 66 (13%) had LOS of 2–3 days; 299 (57%) had LOS of 4–30 days and 127 (24 %) had an LOS of more than 31 days. Neither patient age (p = 0.7) nor gender (p = 0.6) varied according to LTACH LOS prior to unplanned transfer. An unplanned transfer following an LOS of 3 days or less was more likely to occur on a Thursday, Friday, Saturday or Sunday as compared with other days of the week (p = 0.003). Unplanned transfers occurred on all work shifts: day shift (7 a.m.–3 p.m.) 244 (46%), evening shift (3 p.m.–11 p.m.) 201 (38%) and night shift (11 p.m.–7 a.m.) 80 (15%). The majority of patients were receiving their care under the direction of either an academic (146, 28%) or private (323, 61%) pulmonary/critical care physician. A minority of patients were receiving their care under the direction of an internist (57, 10%). The patient’s care was directed by either their designated attending physician (280, 53%) or by a covering or ‘moonlighting’ physician (246, 47%) at the time of the unplanned transfer. LTACH LOS prior to unplanned transfer did not vary significantly with work shift at time of transfer, specialty of attending physician or category of discharging physician (data not shown).
Medical reason for the unplanned transfer
The medical diagnoses triggering an unplanned transfer are listed in Table 2 . An acute change in pulmonary status was the most frequent cause of an unplanned transfer, accounting for 37% of the transfers, following any LOS. Of the 194 patients, 167 transferred for a change in respiratory status had acute respiratory failure. The other most common medical reasons for transfer to acute care were evaluation of myocardial ischemia, arrhythmia, cardiopulmonary arrest, gastrointestinal bleed, acute abdomen, fever workup, change in mental status, seizure and acute renal failure. The organ system not change significantly with LOS at the LTACH (Table 3 ).
Diagnoses prompting unplanned transfers
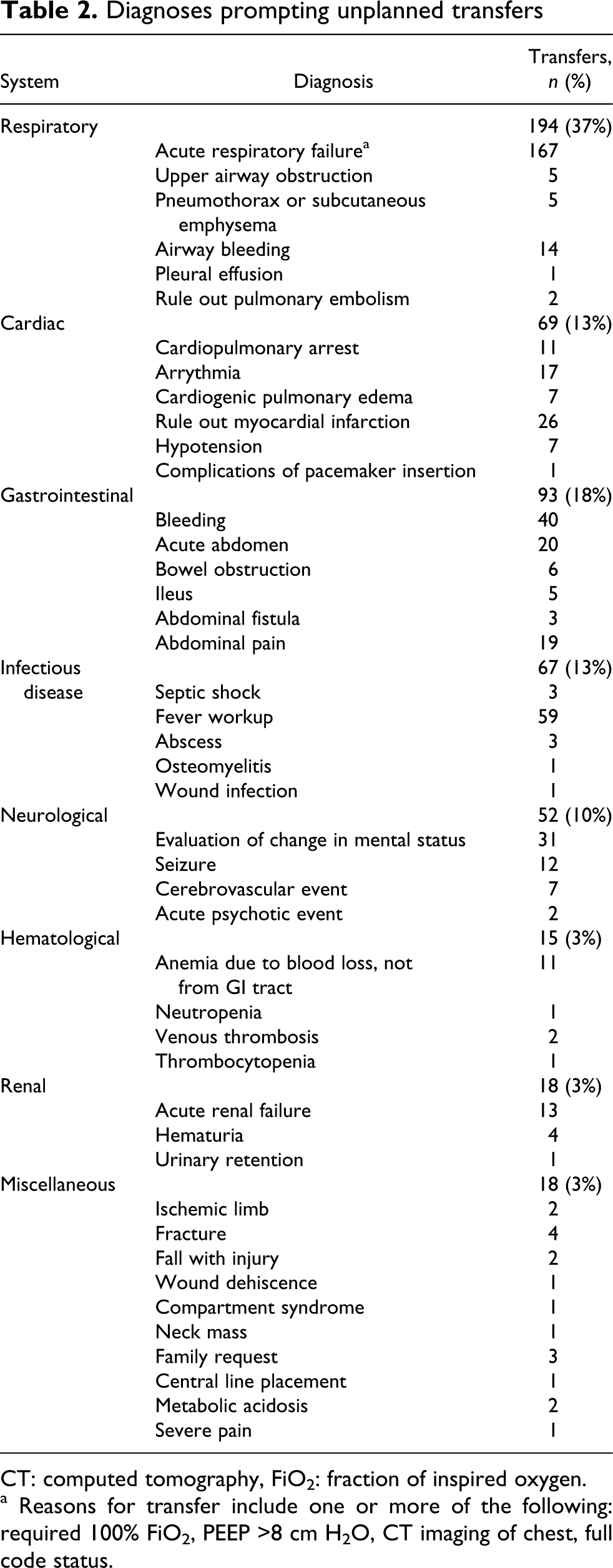
CT: computed tomography, FiO2: fraction of inspired oxygen.
a Reasons for transfer include one or more of the following: required 100% FiO2, PEEP >8 cm H2O, CT imaging of chest, full code status.
Comparison of organ system involvement at the time of unplanned transfer according to LTACH length of stay

LTACHs: long-term acute care hospitals.
Mortality following unplanned transfers
The 30-day mortality rate following unplanned transfer was 32% (133/414) and was independent of LTACH LOS (Table 4 ). The median time to death following unplanned transfer was less than 7 days for any LTACH LOS. The 30-day mortality rate following unplanned transfer did not vary with organ system involved at the time of transfer (Table 5 ), category of acute hospital that originally referred the patient to the LTACH (tertiary referral center: 46/149 [31%]; community hospital with residency program: 17/57 [30%]; community hospital: 71/208 [34%], p = 0.79) or number of unplanned transfers per patient (one unplanned transfer: 103/332 [31%]; two unplanned transfers: 21/62 [34%]; three or more unplanned transfers: 9/20 [45%], p = 0.41), the LTACH unit, the nursing shift or attending physician specialty/coverage status (Table 6 ).
Mortality (30 days) following unplanned transfer according to LTACH length of stay a

a p = 0.425.
b % deaths/unplanned transfers.
c Median, 25th and 75th percentiles.
Mortality rate following unplanned transfer by organ system involvementa

LTACHs: long-term acute care hospitals.
a p = 0.37.
Mortality following unplanned transfer according to site, timing and care oversight

LTACHs: long-term acute care hospitals.
Discussion
In this study, we report on the problem of unplanned transfers of patients with pulmonary disease, from an LTACH system back to acute facilities. The study outlines the movement of this patient population through the health care continuum, describes the medical complexity of this patient population and begins to explore the relationship between LTACH LOS and outcome following unplanned transfer.
A small number of patients required an unplanned transfer within 24 h of arrival at the LTACH. This study also demonstrated an increase in unplanned transfers toward the end of the work week. These observations raise two questions: the suitability of the patient for transfer from the acute facility and secondly the ability of the LTACH to care for their medical needs.
Two sets of admitting criteria (NALTH® and McKesson Corporation®) have been developed to help identify those patients suitable for transfer to an LTACH for further care. In theory, patients with pulmonary disease with or without the need for mechanical ventilation who meet the LTACH admitting criteria have recovered to the point of hemodynamic stability but continue to have significant pulmonary, medical and rehabilitative needs. The recent trend toward earlier tracheostomy placement in intubated patients 7 may reflect pressure on acute facilities to stabilize and discharge patients from the ICU to an LTACH or step down unit.
The majority of the unplanned transfers occurred after an LOS at the LTACH of more than 3 days and reflects the difficulty in predicting medical stability and subsequent recovery as well as the potential for ongoing medical complications in patients with prolonged medical illness. The significance of the apparent increase in unplanned transfers on Thursday–Sunday as compared with Monday–Wednesday for some patients with a short LOS is unclear. The LTACH by definition has less resources than the referring acute care facility but operate on the assumption that patients have attained a sufficient level of stability to have their complex respiratory needs met. The patient-to-medical provider ratio is higher at night and at the weekend, and we suspect that this factor contributes to a percentage of unplanned transfers. The freestanding LTACH does not have an intensive care or high-dependency unit resulting in patients who may need closer observation during a period of escalating medical needs being transferred to a local ICU. For example, patients with worsening respiratory failure require high intensity continuous invasive or noninvasive mechanical ventilation, 100% fraction of inspired oxygen (FiO2), rising positive end expiratory pressure (PEEP) needs and thus need closer hemodynamic monitoring and are a full code are appropriately transferred to an ICU setting. The two satellite LTACH units co-located within acute care hospitals have the ability to rapidly transfer patients to the ICU of host hospitals.
The need for acute facilities to have critical care beds available for expected weekend emergencies or scheduled surgeries after the weekend may in part explain an increase in LTACH admissions as the week advances with a pattern of unplanned transfers occurring 2–3 days later. More research is needed to determine whether the acute hospital LOS and patient severity of illness at the time of discharge inform the unplanned transfer rate from the LTACH.
Medical coverage in hospitals differs during off-hours such as nights and weekends. Despite adequate communication and sign off, a covering physician may never be as familiar with a patient’s complex medical situation as the attending physician. We speculated that as a result the outcomes of patients transferred by the attending physician might differ from the outcomes of patients transferred by covering physicians. Our results indicate that neither LTACH LOS prior to nor mortality following unplanned transfer varied with either the physician attending or coverage status. These data suggest that factors other than the skill level of the physician caring for the patient determine mortality following an unplanned transfer. Examples of other factors that may influence mortality following transfer include the severity of illness, the level of services available at the LTACH and patient and referring facility preferences of care in the event of deterioration in the patient’s condition.
The medical complexity of our patient population is similar to that reported by Scheinhorn et al. in the subgroup of pulmonary patients who require prolonged mechanical ventilation. 8,9 A range of medical problems triggered an unplanned transfer with no clear temporal pattern of organ system failure. The most common problem triggering an unplanned transfer of a pulmonary patient back to an acute facility following any LOS at the LTACH was a deterioration in their pulmonary status and may reflect the unpredictable recovery pattern of patients with pulmonary disease. Cardiac disease was the second most common reason for an unplanned transfer.
Delirium and other less well-defined milder forms of delirium have been reported to occur in 7–20% of patients admitted to a respiratory step down unit 10 and in 5% of patients undergoing prolonged mechanical ventilation in LTACHs. 9 Treating and preventing delirium both in patients in acute care facilities before they are moved to an LTACH and in the LTACH may reduce both unplanned transfers and mortality. 11,12 Patients with renal failure needing dialysis are comanaged with consulting nephrologists at the LTACH. However, renal replacement therapy is usually initiated in an acute facility.
Thus, there is a wide range of medical and surgical complications driving the unplanned transfer process from LTACHs back to acute facilities. This pattern of readmission following discharge to an LTACH is reminiscent of prior studies showing that patients discharged from an ICU to a floor bed have a significant readmission rate. 13–16
The cost of medical care at the end of life has been receiving more attention and up to 40% of Medicare decedent expenditure occurs in the last month of life. 17 We found that up to 25% of patients died following transfer to the acute facility regardless of LTACH LOS prior to transfer, timing of transfer, the unit making the transfer, organ system involved and specialty and coverage status of the physician. The use of acute facility resources for patients approaching the end-of-life at the LTACH may be an example of ‘supply-sensitive care.’ 18 Tools to better identify patients in whom restorative care, in any care setting, has failed and death is likely within 1–2 weeks, along with strategies to help align family expectations with the clinical reality of the patient’s condition, such as a palliative care program, may reduce futile unplanned transfers back to acute facilities in the final stages of illness. 17
The unplanned transfers have a number of possible explanations. First, the criteria being used to screen pulmonary patients for LTACH admission may be unable to identify patients at high risk of unplanned transfer. LTACHs are referral centers for patients with pulmonary disease and complex medical problems and a significant unplanned transfer rate might be an unavoidable consequence of this care model. Second, it might be an indicator of patients either being transferred from an acute facility prematurely due to financial pressures 1,19,20 or third being transferred to an LTACH that is not equipped to meet patient needs. 15 By examining the discharge destination of all patients referred to the LTACH system, our data show that over 67% of patients are successfully discharged to home or a skilled nursing facility, suggesting the LTACH is an effective care model for the majority of referred patients. More work is needed to distinguish between patient-related and process of care-related factors that contribute to the unplanned transfer rate from LTACHs.
The study has some limitations. This is a single-center study and may not reflect practice in other LTACHs. The geographic area of study has a concentration of both acute facilities, which may encourage unplanned transfers and other LTACHs which, through competition, may encourage premature patient acceptance to an LTACH in the first place. Hand off communication between acute facilities and the LTACH system was not addressed. 21,22 We did not address those patients admitted with complex medical problems (but without a pulmonary diagnosis) that in fact had a higher unplanned transfer rate. Access to clinical data from referring hospitals, along with measures of severity of illness and functional status on arrival at the LTACH would have been useful to better stratify the unplanned transfers from the LTACH. Strategies are needed to reduce unplanned transfers back to acute facilities for patients with pulmonary disease being cared for in the LTACH setting. Further studies focused on patients transferred within 24 h of LTACH arrival and those close to the end of life may help reduce unplanned transfers from the LTACH back to an acute facility.
Footnotes
Acknowledgments
We thank Lawrence Hotes, MD, Norma Terrin, PhD, Mary Beth Urquhart, RN, MBA, for providing helpful discussions. Dr White had full access to all the data in the study and takes full responsibility for the integrity of the data and accuracy of the analysis.
Study was funded by and performed at the Rose Kalman Research Center at New England Sinai Hospital.
The authors declared no conflicts of interest.