
Abstract
Background
Diabetes-related foot ulcers (DFUs), often complicated by peripheral arterial disease (PAD), remain a major therapeutic challenge. In patients unsuitable for revascularization, alternative treatments are essential. This study is the first to evaluate bipolar radiofrequency (RF) ablation as part of lumbar sympathetic block (LSB) for enhancing wound healing in DFU patients with critical limb ischemia.
Methods
This retrospective cohort study included 31 DFU patients with severe PAD who were not candidates for revascularization. Group 1 (n = 18) received LSB with bipolar RF plus medical care; Group 2 (n = 13) received medical care alone. Wound healing, amputation rates, pain scores (NRS, DN4), and complications were analyzed.
Results
Complete wound healing was significantly higher in Group 1 (55.5%) than in Group 2 (15.3%) (p = 0.031). Amputation was required in 23.1% of Group 2 patients, while none occurred in Group 1 (p = 0.063). Group 1 showed significant reductions in DN4 (p = 0.0057) and NRS (p = 0.0013) at 6 months. No complications related to LSB were observed.
Conclusions
LSB with bipolar RF ablation is a safe, potentially effective option for DFU patients with PAD not eligible for revascularization. It significantly improves wound healing and pain outcomes. Larger prospective studies are needed to confirm these results.
Keywords
Introduction
Diabetes-related foot ulcers/disease (DFUs), a severe complication of diabetes mellitus, are frequently associated with peripheral arterial disease (PAD).1–5 In patients with critical limb ischemia (CLI), these ulcers can progress to extensive tissue loss and pose a significant risk of amputation, severely diminishing quality of life.6–8 While peripheral bypass surgery and endovascular interventions are standard revascularization approaches, some patients are ineligible due to extensive vascular involvement, severe comorbidities, or both.9,10 This unmet clinical need underscores the importance of exploring alternative therapies to enhance blood flow and promote wound healing.
Lumbar sympathetic block (LSB) has emerged as a promising treatment option for CLI patients unsuitable for traditional revascularization.11,12 By inducing vasodilation of lower extremity arteries, LSB increases tissue perfusion, which may contribute to the healing of DFUs, particularly those with deep ulcerations and substantial tissue loss.13,14 Traditionally, LSB has been performed using monopolar radiofrequency ablation. However, recent advancements in pain management have seen the introduction of bipolar radiofrequency (RF) for various interventional pain procedures.15,16 According to our knowledge, this study represents the first reported use of bipolar RF ablation for lumbar sympathetic chain ablation in the treatment of DFUs (Figure 1). Bipolar RF ablation for lumbar sympathetic chain.
This study aimed to evaluate the efficacy of lumbar sympathetic chain ablation using bipolar RF in patients with severe PAD and DFUs characterized by severe ulceration and tissue loss. The treatment group received bipolar RF ablation in conjunction with antibiotics and antiplatelet therapy, while the control group received standard medical management alone. This article examines the use of bipolar RF lumbar sympathetic chain ablation as an alternative treatment for DFUs in patients who are not candidates for surgical or endovascular revascularization, discussing its potential to improve wound healing by augmenting blood flow.
Methods
Study design and ethical approval
This retrospective cohort study included patients with DFUs and severe peripheral arterial disease (PAD) treated at our tertiary care hospital between January 2022 and January 2024. Treatment decisions were determined by a multidisciplinary diabetic foot council comprising specialists in cardiovascular surgery, endocrinology, interventional radiology, internal medicine, infectious diseases, orthopedics, neurosurgeon and algology. The data collection and analysis protocol was approved by the Ethics Committee of Toros University (Approval No: 21.11.2024/181), and written informed consent was obtained from all patients. This standard consent covered both the risks and potential complications of the intervention as well as explicit permission for anonymized medical data to be used for scientific purposes. Therefore, no additional prospective consent was obtained specifically for this study.
Patient selection
Patients were selected by the multidisciplinary diabetic foot council. All participants underwent lower extremity arterial Doppler ultrasonography to assess the severity and location of PAD-related stenoses. Patients with occlusions distal to the ankle were excluded from consideration for surgical revascularization. Patients deemed at high surgical risk due to severe comorbidities were informed of surgical risks, and lumbar sympathetic chain ablation was offered to those who declined surgery due to these risks.
Patients were admitted both from outpatient clinics and inpatient clinics; however, all procedures were performed during inpatient admission, and none were done on a day-case basis. As the procedures were performed by the Department of Algology, patients did not usually present directly but were most commonly referred by endocrinology, cardiovascular surgery, or plastic surgery specialists. All cases were systematically reviewed and approved by the multidisciplinary diabetic foot council prior to treatment allocation.
Inclusion criteria comprised patients with neuroischemic DFUs and severe PAD who were not candidates for surgical revascularization. Exclusion criteria included isolated neuropathic ulcers, traumatic ulcers, malignant ulcers, and ulcers with extensive necrosis due to uncontrolled infection. All eligible patients underwent arterial Doppler ultrasonography to evaluate revascularization potential, and surgical or endovascular bypass was considered in patients with proximal occlusive disease. Patients with distal occlusions or high surgical risk due to severe comorbidities were considered unsuitable for revascularization and were therefore evaluated for lumbar sympathetic chain ablation. Patient selection was conducted retrospectively by reviewing electronic hospital records and council reports, minimizing the risk of missing data.
Treatment groups
All patients recommended for lumbar sympathetic chain ablation by the diabetic foot council received detailed information regarding the procedure’s expected benefits and risks. Patients who consented to the ablation comprised Group 1 and received bipolar radiofrequency (RF) ablation combined with standard medical management. Patients who declined ablation formed the control group (Group (2) and received standard medical management alone. The main reasons for refusal were fear of interventional risks and unwillingness to discontinue antiplatelet therapy due to cardiac comorbidities. Standard medical management in both groups included antibiotics and antiplatelet agents.
Medical management
Standard medical management included wound care, offloading, glycemic control, antiplatelet therapy, and antibiotic treatment. All patients received regular wound debridement and dressing changes. Offloading was achieved through total contact casting or customized diabetic footwear, depending on ulcer location and severity. Glycemic control was optimized under endocrinology supervision, with insulin therapy when necessary.
Antibiotic treatment was tailored according to the presence of bone involvement. In patients without osteomyelitis, a combination of intravenous (IV) ampicillin + sulbactam and oral ciprofloxacin or IV tigecycline + oral ciprofloxacin was administered for 2–3 weeks. In patients with osteomyelitis, a total of 12 weeks of treatment was administered: parenterally for the first 4 weeks and orally for 8 weeks. Teicoplanin + ciprofloxacin or daptomycin + ciprofloxacin was administered parenterally, while fusidic acid + ciprofloxacin was used orally. Drug selection was adjusted if side effects developed. Daptomycin was given at 10 mg/kg, teicoplanin at 10 mg/kg, tigecycline as a 100 mg loading dose followed by 50 mg every 12 h, fusidic acid at 500 mg three times daily, ciprofloxacin at 500 mg twice daily, and ampicillin/sulbactam at 100 mg/kg. These regimens were in line with current IDSA guidelines.
Procedure details
All procedures were performed during inpatient admission; none were carried out on a day-case basis. The fluoroscope C-arm was positioned to clearly visualize the L2 and L4 vertebrae, ensuring alignment of the superior endplates. The C-arm was then adjusted to an oblique view until the tip of the transverse process aligned with the anterior aspect of the vertebral body. Under local anesthesia at the planned entry point for each level (L2 and L4), two 21G RF cannulas with 15 cm length 10 mm active tips (TOP Neuropole® Needle, TOP Corporation, Tokyo, Japan) were introduced. At the L4 level, one cannula was advanced superior to the transverse process and the other inferior to it, both directed towards the anterior aspect of the vertebral body using oblique fluoroscopic guidance. At the L2 level, one cannula was advanced inferior to the transverse process, while the other was positioned just superior to the lower endplate, given that the sympathetic ganglion is predominantly situated within the lower third of the L2 vertebral body. The needles were brought into contact with the vertebra and carefully “walked along” the vertebral body to ensure proper placement, recognizing that major vessels lie ventral to the vertebral bodies. A lateral fluoroscopic image confirmed needle depth for each cannula, which was adjusted to maintain a position 3–5 mm dorsal to the most ventral aspect of the vertebral body. An anteroposterior (AP) view confirmed medial placement relative to the lateral vertebral line and at the level of the pedicle for each cannula (Figure 2). Fluoroscopy image of bipolar lumbar sympathetic RF.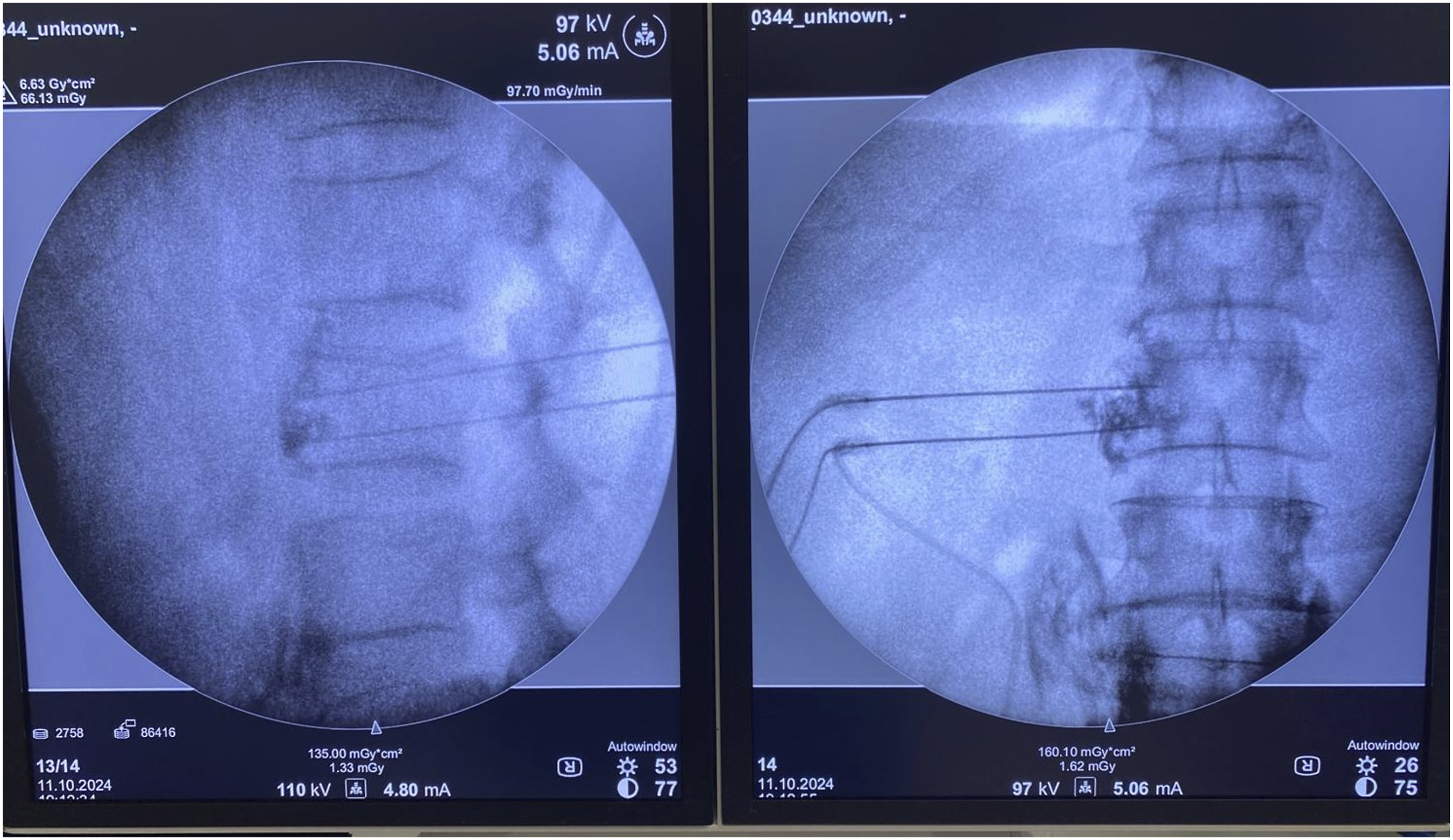
Once correct needle placement was confirmed by aspiration (negative for air, blood, or cerebrospinal fluid), 1 mL of contrast agent was injected to verify adequate flow and appropriate distribution, visualized as contrast covering the anterior vertebral body with superior and inferior spread across one adjacent vertebral level. Sensory stimulation was performed at 50 Hz and 0.5 V, and motor stimulation at 2 Hz and 2 V. In the absence of a response during both stimulations on both probes, local anesthetic was administered, and ablation was performed at 80°C for 90 s (RF device; TOP Lesion Generator TLG-10, Japan). This procedure was repeated at both the L2 and L4 vertebral levels.
Procedural success was confirmed by an increase in ipsilateral leg temperature within minutes following ablation.
Follow-up and outcome measures
Patients were followed for at least 12 months, with regular visits at 1, 2, 3, 6, and 12 months post-procedure. Follow-up assessments included clinical examination, wound size measurement, and evaluation of wound healing. Pain scores, infection control, and potential side effects were also monitored and documented. Wound diameter was tracked using a tracing method. A sterile acetate sheet was placed over the wound, and the wound borders were marked. After carefully cutting along the marked borders, the wound area was photographed with a smartphone and subsequently analyzed using ImageJ® software, which is capable of calculating irregular wound areas. To minimize measurement error, all ImageJ results were cross-validated by placing the acetate sheet on graph paper (0.25 cm2 per square) and manually counting the enclosed squares.
Data collection and analysis
Data on demographics, comorbidities, ulcer characteristics, treatment, and follow-up outcomes were collected retrospectively. Numeric Rating Scale (NRS) and Douleur Neuropathique 4 Questions (DN4) scores were recorded before and after the procedure to assess treatment effects on pain. Wound areas at follow-up, wound closure (epithelialization), and the need for amputation were recorded. Statistical comparisons were performed between the treatment and control groups.
Results
Patient selection and participation
Between January 2022 and January 2024, 176 patients were evaluated by the multidisciplinary diabetic foot council. Based on the council’s recommendations. • 65 patients were deemed suitable for peripheral bypass surgery, • 80 patients were directed to endovascular treatment and excluded from the study.
31 patients who were not candidates for surgical or endovascular treatment were recommended for sympathetic chain ablation. After thorough explanation of the procedure’s benefits and risks. • 18 patients consented to lumbar sympathetic blockade and received combined sympathetic blockade with medical treatment (Group 1). • 13 patients declined the procedure and received standard medical therapy alone (Group 2).
Demographic and clinical characteristics
The mean patient age was 60.16 ± 11.89 years (range: 35–81). No significant difference in age was observed between Group 1 and Group 2 (p = 0.2368). Six patients (19.35%) were female, and 25 (80.64%) were male, with no significant difference in sex distribution between the groups (p = 0.6768). The mean duration of diabetes at the time of treatment was 15.60 ± 8.53 years (range: 3–34), with no significant difference between the groups (p = 0.2542).
Baseline laboratory and wound characteristics were also comparable between groups. The mean HbA1c was 8.11 ± 1.97 (range: 5.6–12.6) in the RF group and 7.76 ± 1.45 (range: 5.5–10.3) in the medical group (p = 0.4354). Mean estimated GFR was 76 ± 20.31 (range: 31–106) in the RF group and 89 ± 26.51 (range: 11–118) in the medical group, showing a statistically significant difference (p = 0.0238). The mean wound area at enrolment was 22 ± 22.42 cm2 (range: 2–89) in the RF group and 27.07 ± 22.73 cm2 (range: 4–74) in the medical group, with no significant difference (p = 0.3370).
Prior to treatment, 4 patients were classified as Wagner stage II, 14 as stage III, 10 as stage IV, and 3 as stage V. No patients were classified as Wagner stage I. No significant differences in wound Wagner staging were observed between the groups (p = 0.8761).
Thirteen patients (41.9%) had positive wound cultures, and 7 (22.58%) had positive blood cultures before treatment. No significant differences were found between the groups for wound culture or blood culture positivity (p = 0.6858 and p = 0.9952, respectively).
Preoperative clinical and demographic characteristics of patient.

aStudent t-test.
bFisher Exact Test.
cMann Whitney-U.
dChi Square Test.
Treatment outcomes
Wound healing rates
In Group 1 (lumbar sympathetic chain ablation), 10 patients (55.55%) achieved complete wound healing, 7 (38.88%) experienced partial healing, and 1 (5.55%) showed no improvement (Figure 3(a)–(c)). In Group 2 (medical therapy alone), 2 patients (15.38%) achieved complete wound healing, 6 (46.15%) experienced partial healing, and 5 (38.46%) showed no improvement. Lumbar sympathetic ablation was associated with a significantly higher rate of complete wound healing compared to medical therapy alone (Fisher’s exact p = 0.032; OR = 5.68, 95% CI: 1.10–29.28; RR = 3.09, 95% CI: 0.94–10.21). (Table 2). Wound healing after bipolar lumbar sympathetic RF. Comparison of wound healing and amputation outcomes between groups during follow-up. aFisher Exact Test.

Amputation rates
No patients in Group 1 (0%) required amputation. In Group 2, 3 patients (23.07%) required amputation. This difference in amputation rates between the groups was not statistically significant (Fisher’s exact p = 0.064; OR = 0.08, 95% CI: 0.004–1.73; RR = 0.11, 95% CI: 0.006–1.88). (Table 2).
Complication
No complications, including neurological deficits, local infections, or hematomas, were observed in any of the patients who underwent sympathetic chain ablation.
Pain score
DN4 score
- Group 1 (Sympathetic Chain Ablation): The DN4 score decreased from 3.72 ± 1.93 before the treatment to 2.5 ± 1.33 after 6 months, showing a significant reduction in neuropahtic pain (p = 0.0057). Comparison of pain scores between groups during follow-up. aMann Whitney U. bWilcoxon Sign Test.

NRS Score. - Group 1 (Sympathetic Chain Ablation): The NRS score decreased from 4.61 ± 2.85 before the treatment to 1.77 ± 1.62 after 6 months (p = 0.0013), showing a significant improvement in pain levels. - Group 2 (Medical Treatment): No significant change in the NRS scores was observed (p = 0.197). (Table 3)
Discussion
DFUs, frequently associated with peripheral arterial disease (PAD), represent a significant complication of diabetes mellitus. In patients unsuitable for surgical revascularization, these treatment-resistant wounds, often accompanied by infection and tissue loss, not only increase the risk of amputation and severely impair quality of life, 17 but also significantly elevate the risk of mortality 18 This necessitates the exploration of alternative therapeutic strategies. Lumbar sympathetic blockade (LSB) has emerged as a promising option for DFU patients with critical limb ischemia (CLI) who are not candidates for surgical or endovascular interventions.19,20 This study investigated the contribution of bipolar radiofrequency (RF) ablation, a novel approach in this context, to DFU healing. This study is the first in the literature to investigate the use of bipolar RF ablation in lumbar sympathetic block for patients with DFU, aiming to assess its contribution to wound healing in cases of critical limb ischemia.
Our study demonstrated a significantly higher rate of complete wound healing in the group receiving LSB with bipolar RF ablation (55%) compared to the medical treatment group (15%) (p = 0.031). This finding aligns with existing literature suggesting that LSB promotes healing by enhancing blood flow in the treatment of DFUs. Improved circulation and increased tissue oxygenation are proposed mechanisms by which LSB accelerates wound healing.
While our study showed a trend towards reduced amputation rates in the LSB group (0%) compared to the medical treatment group (23%), this difference did not reach statistical significance (p = 0.063). This lack of statistical significance may be attributable to the relatively small sample size. Larger studies are needed to further investigate the impact of LSB on amputation rates. It is hypothesized that LSB reduces the need for amputation by improving blood flow and tissue oxygenation, factors known to influence amputation risk. The positive impact of LSB on patient quality of life, through pain reduction and improved functional status, is well documented in the literature. However, in our study, no statistically significant difference was observed between the groups in terms of NRS and DN4 scores; this may be attributed to the fact that the primary aim of the study was to assess the contribution of LSB to wound healing rather than pain management. It should also be emphasized that non-significant P values in a study of this size cannot be taken as evidence of no difference. The wide 95% confidence intervals observed in our outcomes reflect the uncertainty inherent in our limited cohort and highlight the need for larger, adequately powered prospective studies to confirm these findings.
Radofrequency energy and its thermal effects on tissues have long been utilized in modern medicine. One widely used technique is monopolar RF, which employs a grounding pad. Factors such as needle thickness, active tip length, targeted tissue, and target temperature significantly influence the size of the lesion created. As distance from the electrode increases, the generated energy and resulting temperature decrease exponentially. 21 The size of the lesion created is a critical factor determining procedural success. The inconsistent success rates observed with monopolar RF have prompted researchers to explore alternative methods. Bipolar RF, which has recently gained popularity due to its reported superior efficacy, uses two electrodes placed directly into the target tissue. RF current passes between these two electrodes without the need for grounding pads, minimizing energy loss and enabling larger ablation volumes. While monopolar RF produces ellipsoidal lesions, bipolar RF generates rectangular lesions. Additionally, lesions created by bipolar RF are considerably larger compared to those produced by monopolar RF. 22 Due to these characteristics, bipolar RF is more likely to capture the nerve even in cases of anatomical variations. Given the essential need for wound healing in our patient group, we preferred bipolar RF. Multiple studies indicate that LSB increases lower extremity blood flow 13 and it has also been utilized for diabetic neuropathy and DFUs. LSB not only improves blood flow through vasodilation but also by reducing inflammatory cytokines such as norepinephrine, serotonin, beta-endorphin, and substance-P. 23 Therefore, we consider LSB particularly important in managing DFUs. In our patient population, who experienced prolonged diminished quality of life, we found it more appropriate to directly utilize bipolar RF, which is believed to be more effective, rather than repeatedly attempting less effective interventions.
Importantly, the risk of complications is higher when lumbar sympathetic blockade (LSB) is performed with neurolytic agents compared to radiofrequency (RF) ablation. 24 However, in our study and other reports in the literature, placing two needles instead of one during RF thermocoagulation did not increase the risk of complications. 25 Therefore, applying bipolar RF in LSB may represent a good alternative to neurolytic blockade.
In our study, no neurological deficits, local infections, or hematomas were observed in any patient undergoing LSB with bipolar RF. This finding supports the safety of the procedure and aligns with previous studies reporting low complication rates for LSB. 26 Although rare complications such as nerve injury or bleeding have been reported,27–29 often related to specific application techniques, our results suggest that LSB with bipolar RF can be a safe and effective treatment option in appropriately selected patients, with minimal risk of complications.
Another important point concerns patient preference in treatment selection. While the main reasons for refusing ablation were fear of interventional risks and reluctance to discontinue antiplatelet therapy due to cardiac comorbidities, other factors may also have influenced patient decisions. These include socioeconomic barriers, concerns about the novelty of the technique, partial symptomatic relief with conventional therapy, psychological reluctance toward invasive procedures, and logistic challenges such as accessibility to specialized centers. Such factors, though not systematically recorded in our study, may have contributed to the composition of the control group and should be considered when interpreting our findings.
This study has limitations, including its retrospective design and relatively small sample size, which warrant confirmation of our findings in larger, prospective studies. The lack of long-term follow-up also limits our ability to draw definitive conclusions about the long-term effects of this treatment. In addition, objective perfusion measures such as ABI and pedal acceleration time were not systematically recorded, as these assessments were not part of our routine clinical protocol. TcPO2 was also unavailable in our institution due to local technical limitations. Therefore, comparability of tissue perfusion between groups could not be confirmed with standardized parameters. Moreover, the Wagner classification was used to describe ulcer severity, although more contemporary systems such as SINBAD or WIfI may provide a more comprehensive assessment of prognosis. In addition, the confidence intervals for our main outcomes were wide, reflecting the uncertainty around the point estimates. This further underscores that our results should be interpreted with caution and validated in larger studies. Moreover, despite comparable baseline characteristics between groups, the retrospective and non-randomized design inevitably introduces the possibility of unmeasured confounding and inherent group differences that may have influenced the outcomes. However, to our knowledge, this study is the first to investigate the effects of LSB on DFUs using bipolar RF ablation. This innovative approach represents a significant contribution to the literature and may serve as a foundation for future research. The direct comparison of LSB with standard medical therapy and the detailed monitoring of complication rates are key strengths of this study.
Conclusion
Bipolar RF lumbar sympathetic chain ablation significantly improved wound healing in patients with DFUs and severe PAD who were not candidates for surgical or endovascular revascularization. Compared to standard medical therapy alone, this procedure was associated with higher complete wound healing rates and reduced neuropathic pain, without complications. These findings suggest that bipolar RF ablation may serve as a safe and effective alternative treatment for DFUs in high-risk patients. Nevertheless, our findings should be considered preliminary, and a prospective pilot randomized controlled trial (RCT) would represent the most appropriate next step before moving toward a larger, adequately powered RCT.
Footnotes
Ethical Consideration
Toros University ethical board approved this retrospective study at 21.11.2024 (181 number).
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.