
Abstract
Objectives
We aimed to evaluate fetal cerebral circulation using three-dimensional power Doppler (3DPD) vascular indices and to study their relationships with maternal lipid and glycaemic profiles.
Methods
Case–control study in women with and without gestational diabetes mellitus (GDM) at 28–32 weeks in which feto-maternal Doppler study and 3DPD cerebral vascularization indices (FI, VI and VFI) were determined. Maternal lipid and glycaemic profiles were also analysed. Both groups were compared and the correlations of the 3DPD indices with studied variables were analysed.
Results
There were significant differences between groups in cerebral FI (p= 0.02), mean maternal Uterine artery PI (p= 0.009) and glucose levels (p= 0.001), being higher in the GDM group. Significant negative correlations were found in GDM group between VFI and MCA PI (p = 0.02) and between VI and MCA PI (p= 0.01). In the GDM group we found a negative significant correlation between FI, VI, VFI and maternal glucose (r= −0.52, p<0.001; r= −0.32, p=0.03 and r= −0.36, p= 0.01, respectively).
Conclusions
Fetal cerebral FI values were higher in GDM pregnancies. All 3DPD vascular indices showed an inverse correlation with maternal glucose levels. These findings support the view that GDM may also represent a fetal vascular disorder influencing fetal neurodevelopment.
Keywords
Background
Gestational diabetes mellitus (GDM) is one of the most common medical complications of pregnancy. A greater prevalence of obesity and sedentary lifestyles during the last decades is increasing the prevalence of GDM among reproductive-aged women. The mean overall prevalence in Europe has been reported as 5.4% 1 and for the US as high as 7.6% of all pregnancies. 2
GDM is associated with a higher risk of short-term complications for mothers and newborns, including large for gestational age infants and macrosomia, preeclampsia, polyhydramnios, stillbirth, birth trauma, and increased neonatal morbidity. 3 However, in late years, we are becoming aware of long-term consequences associated with gestational diabetes that extend beyond the post-partum and neonatal periods. For the mother, gestational diabetes is a marker for the development of type 2 diabetes, metabolic syndrome, and cardiovascular morbidity later in life. 4 For the offspring may reflect the infant’s increased risk of developing childhood obesity, impaired glucose tolerance, metabolic syndrome and cardiovascular disease.4–6
Furthermore, although insults that occur in gestational diabetes are not associated with cerebral congenital abnormalities, the central nervous system (CNS) continues to develop through the third trimester and is still susceptible to subtle alterations, such as learning disabilities, that only become evident during the course of postnatal development. Neurodevelopmental studies on offspring of mothers with diabetes demonstrated lower scores of Bayley scales of Infant development and increased rate of gross and fine motor abnormalities, of attention deficit hyperactivity disorder, learning difficulties and possibly also autism spectrum disorder.7-10
The use of three-dimensional power Doppler (3DPD) is especially useful in the evaluation of brain vessels because of their small calibre, however, few studies have been conducted to assess 3DPD in fetal cerebral vascularization.11–13 Taking into account the previous observations of higher risk of neurodevelopmental impairment in the offspring of women with GDM, it would be of great interest to evaluate fetal cerebral circulation using 3DPD vascular indices and to relate with the conventional Doppler study and maternal lipid and glycaemic profiles.
Methods
This was a prospective and cross-sectional case–control study in pregnant women participating in a national research project about ambulatory blood pressure monitoring in women with gestational diabetes (PI16/00370). All women had an ultrasound examination between 28 and 32 weeks at the Division of Maternal-Fetal Medicine of the Obstetrics and Gynaecology Unit in Puerta del Mar University Hospital, Cádiz, Spain in 2017–2018. The study was approved by the ethical committee (CEI/20 December 2016) and was in accordance with the Declaration of Helsinki.
Inclusion criteria were the completion of glucose screening according to the two-step criteria of the National Diabetes Data Group that have been accepted by the Spanish Group of Diabetes in Pregnancy 14 and a signed consent form to participate in the study. The O'Sullivan’s test was used as an initial screening test (fasting blood glucose and 1 hour after administration of 50 g of glucose) and an oral glucose tolerance test (OGTT) as a confirmatory test (two or more pathological values in the determination of fasting blood glucose and 1, 2 and 3 h after administration of 100 g of glucose). Women with pathological results were included in the GDM group (n=56). Exclusion criteria were history of pregestational diabetes, hypertensive or thyroid disorders, multiple gestation and fetal anomaly. The control group consisted of physiologic pregnancies with normal glucose screening that were seen during the growth scan at 28–32 weeks and accepted to participate in the study (n=65). The management of GDM was the protocol recommended by the American Diabetes Association, 15 that is, to initiate medical nutrition therapy taking as therapeutic target a capillary glucose level of <95 mg/dL (5.27 mmol/L; fasting) and <140 mg/dL (7.76 mmol/L; 1 h postprandial). If these targets were not achieved after repeated assessments, insulin was initiated using NPH insulin and/or regular insulin.
Ultrasound Doppler assessment was performed in each patient including maternal mean uterine arteries (mUtA) and fetal umbilical and Middle Cerebral Artery (UA, MCA) pulsatility indices (PI). Cerebral-placental ratio (CPR, defined as MCA PI/UA PI) and cerebral-placental uterine ratio (CPUR, defined as the division of CPR by mUtA PI) were calculated accordingly.
The fetal head was scanned in its transverse plane at the level of the base of the skull. Power Doppler was activated to visualize the circle of Willis with a Pulse repetition frequency of 0.9 Hz. using a Voluson 730 Expert (GE Healthcare) equipment equipped with a 5-MHz transabdominal probe. Fetal head Power Doppler volumes were acquired and stored digitally for off-line analysis using 4D VIEW® software (GE Healthcare). This software contains the Virtual Organ Computer-aided AnaLysis (VOCAL), that was set automatically to generate a sphere volume, and then the 3DPD vascular indices (VI, FI, VFI) were calculated automatically by using the histogram (Figure 1). Three saved volumes for each patient were determined, and the mean of the three determinations for each vascular index was calculated. Transabdominal sonography was performed by one of two operators (FB and SPM). In 30 cases (15 controls and 15 GDM cases) both operators performed the scan to estimate the interobserver repeatability.
In the same visit, a venous blood plasma sample was obtained and froze at -20°C until these samples were analysed. Demographic, prenatal and delivery outcome data were reviewed and collected using electronic medical records.
Statistical analysis
Continuous numerical variables were described using means and standard deviations. Qualitative variables through numbers and proportions. The comparison between proportions was performed using the chi-square test and Fisher’s exact test if the observed numbers were less than 5. The distribution of the numerical variables was evaluated using a histogram and the Kolmogorov-Smirnov test. In the case of having a normal distribution, the correlation between variables was studied using Pearson’s correlation coefficient, and the differences between groups using the Student’s t-test. In the case of non-parametric variables, the coefficient of Spearman’s correlation coefficient was used and to compare groups of two, the U-Mann Whitney. The level of significance is previously established at 95% (p < .05). Limitations of the study were those derived from its design as it is a case-control study carried out in a single centre, without randomization and without being blind to any of the parts.
To demonstrate significant differences between both groups at 3D Power Doppler cerebral vascularization index (using FI), according to data from a previous study 11 carried out in IUGR fetuses, with an estimated standard deviation of 4.67 and a ‘minimum difference detected’ of 2.62. Using this data and accepting an alpha risk of 0.05 and a 1-beta power of 0.80 in a bilateral contrast, 50 subjects are required in each branch.
Results
Maternal demographic and clinical characteristics in women participating in the study.
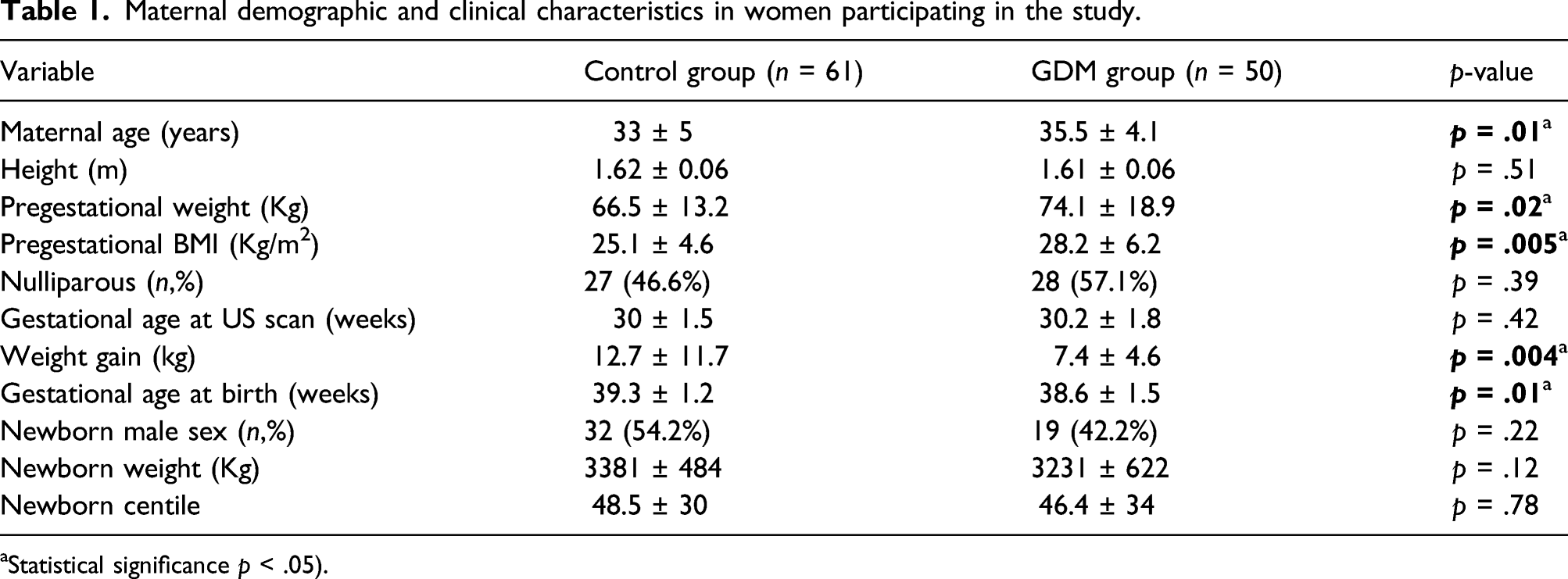
aStatistical significance p < .05).
Biochemical parameters in maternal blood and Doppler and 3D Power Doppler ultrasound parameters.
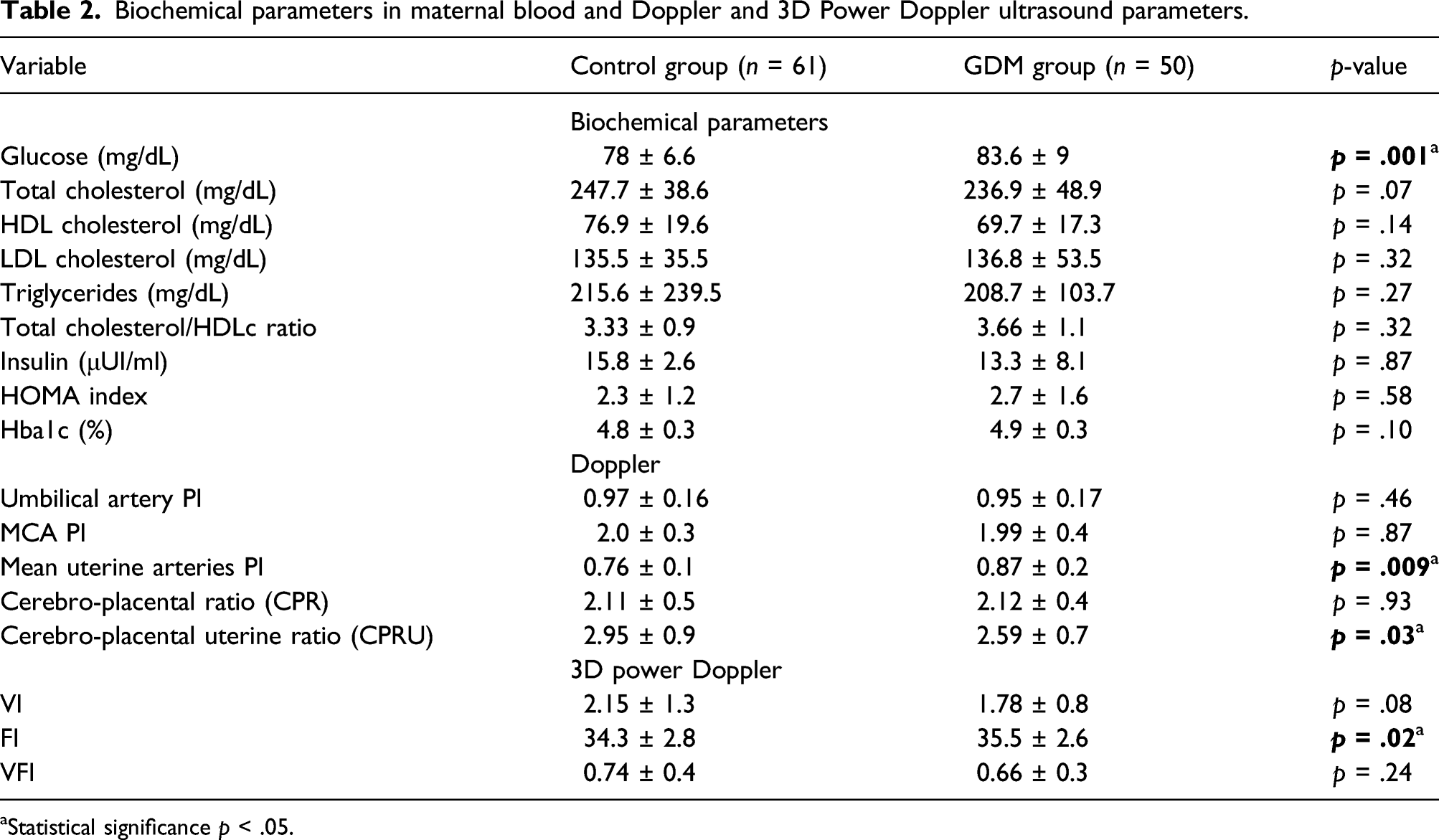
aStatistical significance p < .05.
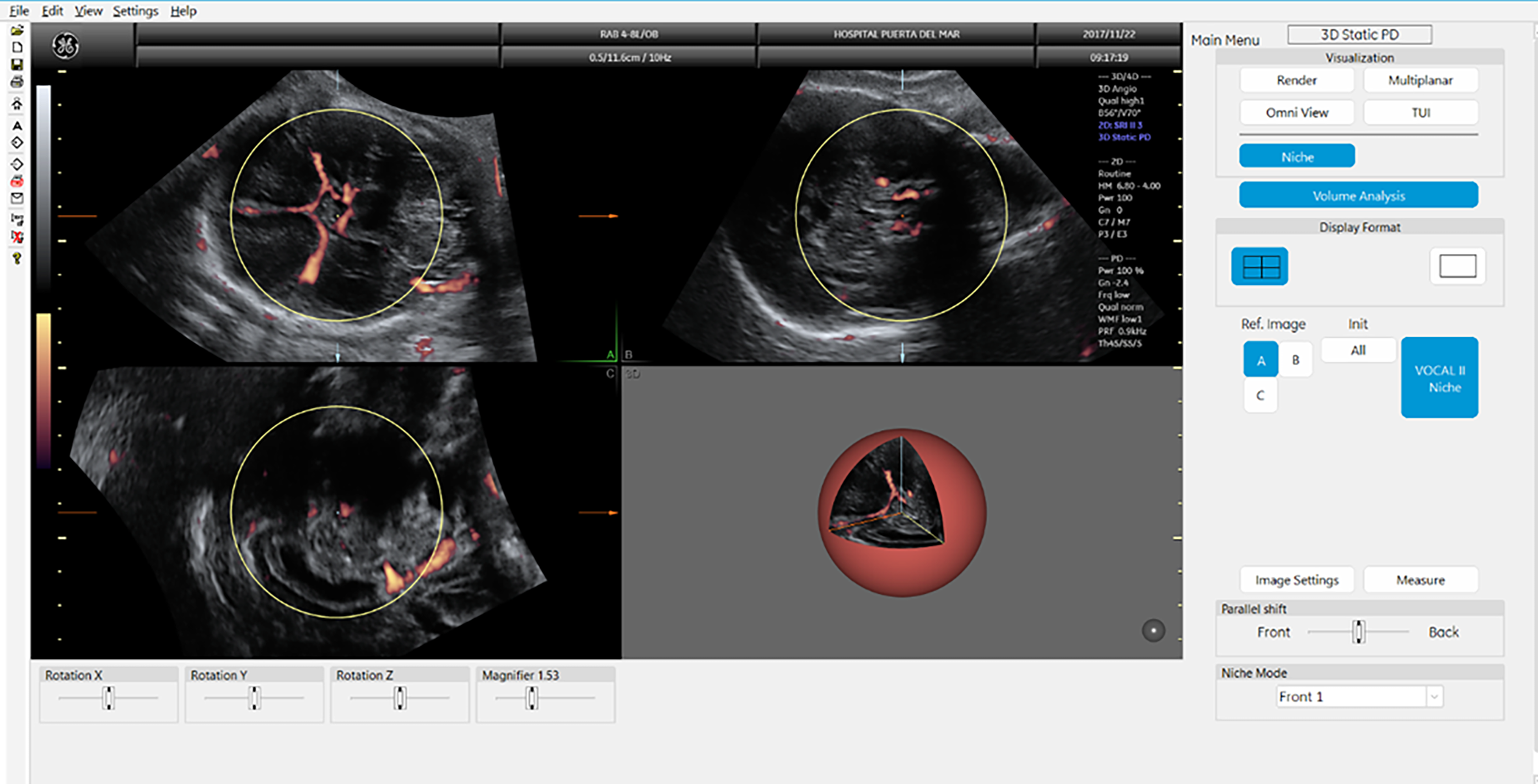
The fetal head 3DPD volume acquisition using VOCAL was set automatically to generate a sphere volume. 3DPD vascular indices were calculated automatically off-line by using the histogram facility. 3DPD: three-dimensional power Doppler.
Relationships between 3DPD vascular indices and Doppler ultrasound parameters
Relationships between three-dimensional power Doppler vascular indices and Doppler and biochemical parameters.
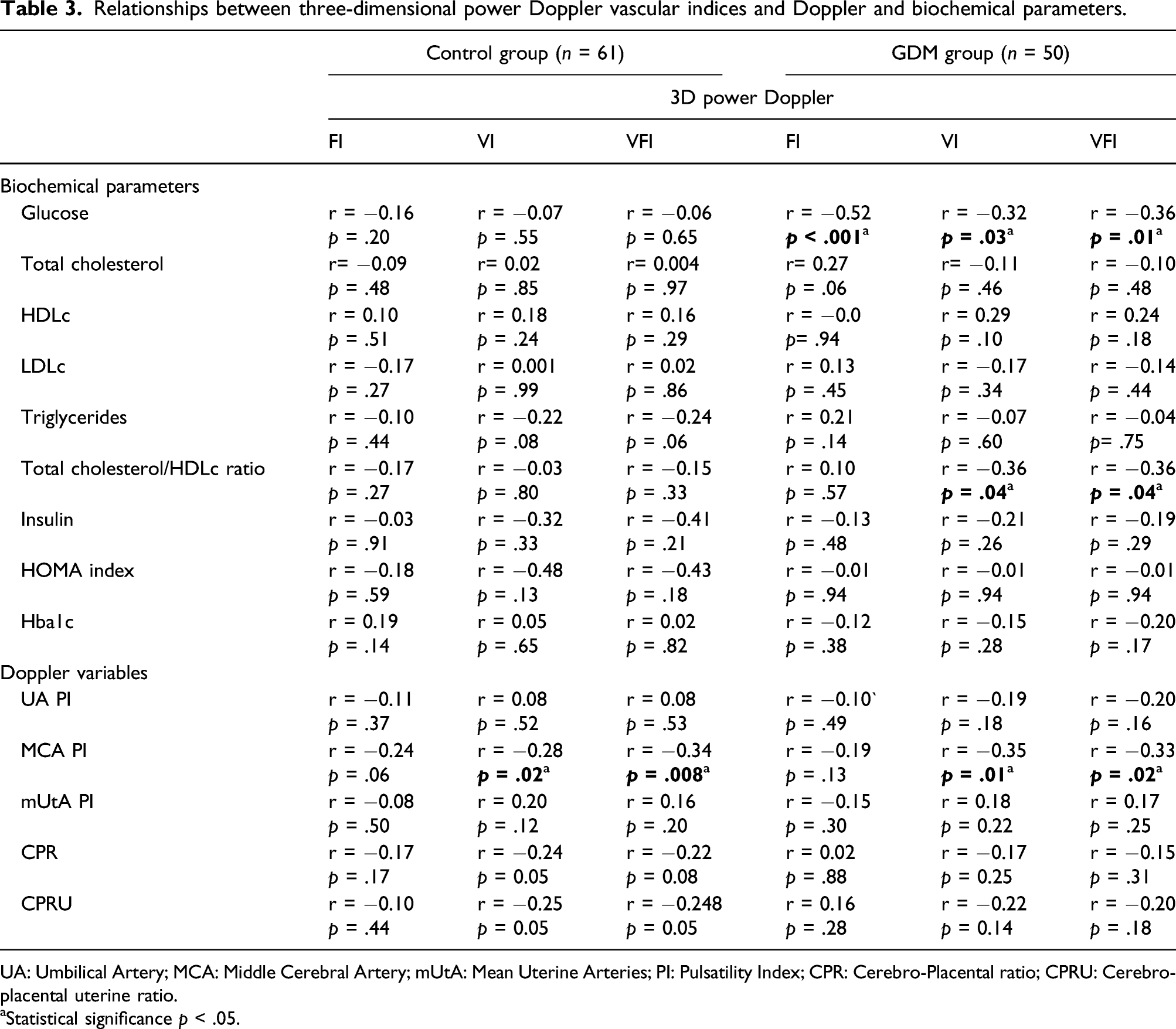
UA: Umbilical Artery; MCA: Middle Cerebral Artery; mUtA: Mean Uterine Arteries; PI: Pulsatility Index; CPR: Cerebro-Placental ratio; CPRU: Cerebro-placental uterine ratio.
aStatistical significance p < .05.
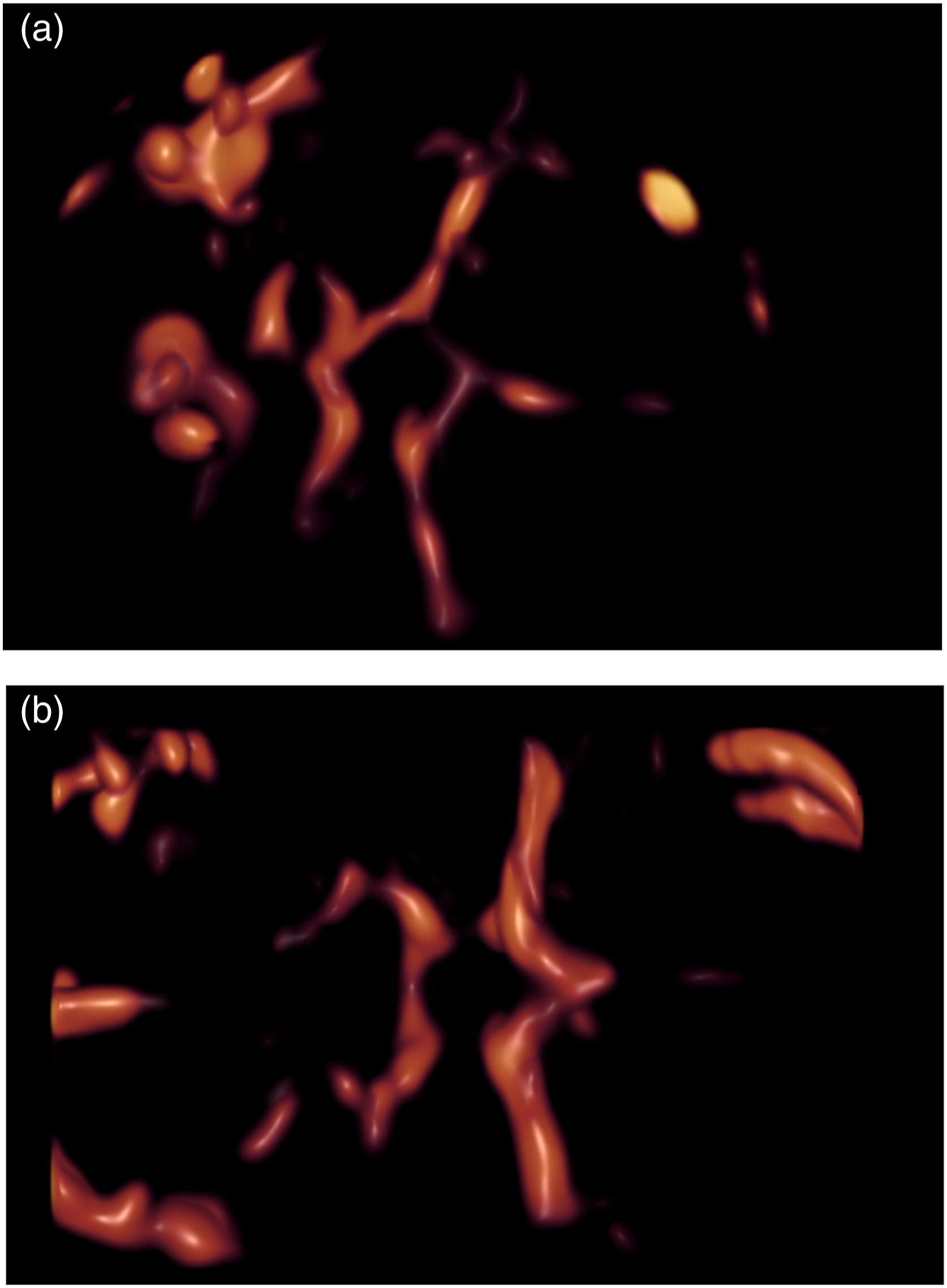
Fetal cerebral three-dimensional power Doppler volume images including the circle of Willis in control (A) and GDM pregnancies (B).
Relationships between 3D vascular indices and the analytical parameters
In the GDM group we found a negative significant correlation between 3D vascularization indices (FI, VI and VFI) and maternal glucose (r = −0.52, p < .001; r = −0.32, p = .03 and r = −0.36, p= 0.01, respectively) (Figure 3), however such correlation was not found in the control group. We also found significant negative correlations in the GDM group between VI and VFI with total cholesterol/HDLc ratio (r= −0.36, p = .04 and r = −0.36, p = .04, respectively). (Table 3) Scatterplot of MCA PI in relation to VFI (3A) and VI (3B) in the GDM group. Scatterplot of maternal glucose (mg/dL) in relation to FI (3C), VI (3D) and VFI (3E) in the GDM group. GDM: gestational diabetes mellitus; MCA: Middle Cerebral Artery.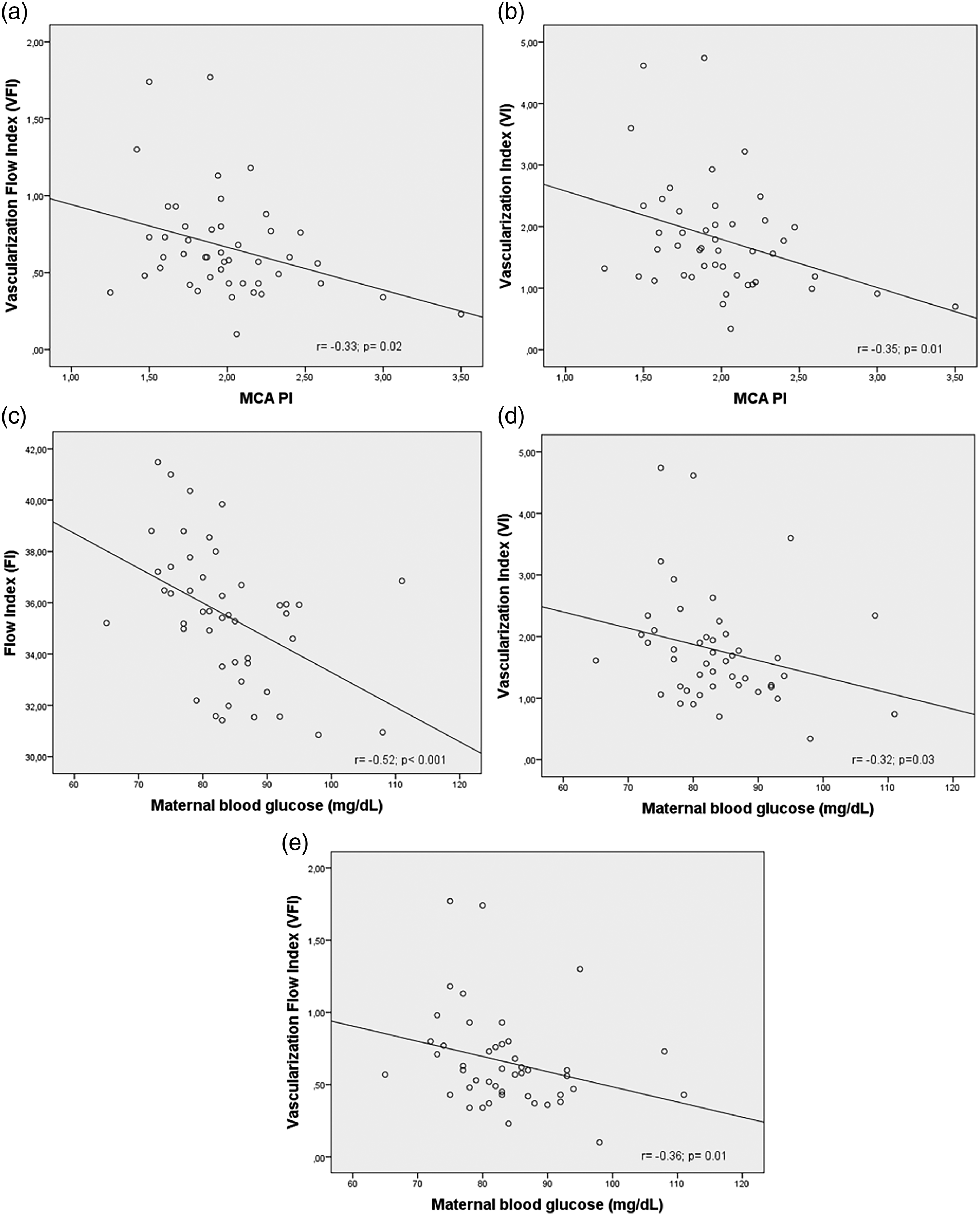
Discussion
In this study, we have evaluated the state of fetal cerebral vascularization using vascular indices obtained with 3DPD in a sample of women with and without gestational diabetes.
The GDM group presented higher maternal age, weight and pre-pregnancy BMI compared to control pregnancies. These findings can be explained since these characteristics are well-known risk factors for developing gestational diabetes mellitus. The GDM group also presented higher glucose maternal levels, as a reflection of the presence of this pathology in pregnancy.
Women with GDM showed higher mUtA PI values which could result in a decreased uterine blood flow. In the same line, a previous study in GDM 16 showed a direct relationship between the pro-inflammatory state and the lipidic profile with mUtA PI. Recently, a new parameter, the Cerebro-placental-uterine ratio (CPUR), has been proposed by MacDonald et al. 17 to detect more cases of fetal growth restriction. It is calculated by dividing the CPR by mean UtA PI. We have found lower CPRU values in GDM cases and may be of clinical interest in the identification of fetuses at risk of poorer neonatal outcomes, as has been previously proposed for Cerebro-placental ratio. 18
Concerning data of 3DPD cerebral vascularization indices, the flow index (FI) represents the mean intensity of the Power Doppler signal of all the existing coloured voxels and the vascularization index (VI) the proportion of coloured voxels with respect to the total voxel (expressed as a percentage). 19 In the GDM group, we have found a higher cerebral blood supply (higher FI) without an increase in the number of vessels (VI) in the area of the circle of Willis that the conventional MCA PI Doppler study failed to detect. This finding could mean a mild increase in the fetal cerebral circulation, which in these cases do not imply an authentic redistribution phenomenon, but that could be related to the poorer neurological outcomes previously reported.7–9,20,21 In the same line we also found a negative correlation between VI and VFI with MCA PI, so the lower MCA PI, the higher the cerebral blood flow as indicated by increased 3D vascularization indices. A study evaluating 3DPD indices in intrauterine growth-restricted fetuses (IUGR) 11 found a significant increase in blood flow (FI) and in the number of vessels (VI), possibly in response to angiogenesis processes resulting from hypoxia. The vascular flow Index (VFI) is the mathematical result of multiplying VI and FI and dividing it by 100. 19 This index did not show any outstanding results.
We found significant negative correlations between the three vascular indices and maternal blood glucose levels in the GDM group. This finding support the view that high glucose levels may cause some kind of subtle damage leading to an altered fetal cerebral vascularization.
The contour mode in the VOCAL software was set automatically to generate a spherical volume to ease a standard method useful in clinical practice. However, this technique also has its limitations, given that we assumed we left a part of the cerebral circulation out of our measurements, that is sensible to fetal movements and position and that is difficult to obtain in cases with increased maternal adiposity. This is the reason why we were not able to obtain valid 3DPD volumes in 10 of 121 studied fetuses (8.2%).
In conclusion, we have found that in GDM, fetuses present a higher cerebral blood flow (FI) without an increase in the number of vessels (VI), that conventional Doppler study (MCA PI) was not capable to detect. Finally, all 3DPD vascular indices showed an inverse relationship with maternal glucose levels. These findings support the view that GDM may also represent a fetal vascular disorder influencing fetal neurodevelopment. We hypothesize that maternal hyperglycaemia may represent a deleterious effect on fetal brain vascularization. Optimal metabolic control of women with gestational diabetes may help to decrease the potentially pernicious effect of hyperglycaemia on these fetuses.
Further studies of 3DPD vascular indices may provide interesting data for the clinical management of gestational diabetes, since may lead to better identification of fetuses at increased risk of poorer neurological outcomes that may benefit from obstetric intervention.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the Carlos III Health Institute (PI16/00370) to C. López-Tinoco and F. Bugatto.