
Abstract
Background:
Increasing arterial stiffness is an important contributor to declining cardiovascular health in ageing. Changes in whole-body fuel metabolism could be related to alterations in arterial stiffness in ageing adults.
Methods:
Targeted high-performance liquid and gas chromatography mass spectrometry were used to measure 84 circulating metabolites in a group of community elderly adults (n = 141, 58% men; mean age = 70.6 ± 11.2 years) without cardiovascular disease. In basic and adjusted models, we correlated the measured metabolites to carotid–femoral pulse wave velocity assessed by applanation tonometry.
Results:
Age (β = 0.10, p < 0.0001), smoking status (β = 1.32, p = 0.02), dyslipidemia (β = 1.22, p = 0.01), central systolic blood pressure (β = 0.05, p < 0.0001), central mean arterial pressure (β = 0.04, p = 0.03) and central pulse pressure (β = 0.05, p < 0.0001) were significantly associated with pulse wave velocity. Amino acids such as histidine, methionine and valine correlated with pulse wave velocity. In multivariable models adjusted for clinical covariates, only Factor 5, comprising the medium- and long-chain dicarboxyl and hydroxyl acylcarnitines was independently associated with pulse wave velocity (β = 0.24, p = 0.015).
Conclusion:
An upstream metabolic perturbation comprising medium- and long-chain dicarboxyl and hydroxyl acylcarnitines, likely reflecting changes in cellular fatty acid oxidation, was associated with arterial stiffness among aged adults. This advances mechanistic understanding of arterial stiffness among aged adults before clinical disease.
Introduction
By 2030, approximately 20% of the world population will be aged 65 years or older. 1 This, coupled with the fact that cardiovascular disease (CVD) is a leading cause of death in older adults, 2 underscores the importance of gaining a better understanding of age-related CVD. Thus, the underlying mechanisms through which ageing exerts pathological changes in the cardiovascular system require further study. Although ageing is a physiological process, there are pathologic effects associated with older age which result in CVD. 2 Even in apparently healthy individuals, important changes occur in the cardiovascular system with advancing age, such as thickening and stiffening of the large arteries due to collagen and calcium deposition with loss of elastic fibres in the medial layer.2–4 These changes result in central arterial stiffening with ageing even in the absence of clinical hypertension. 5 Studies show that measures of arterial stiffening, such as aortic pulse wave velocity (PWV), increase multi-fold across the adult lifespan.6,7 Importantly, independent of the effects of blood pressure, PWV has been shown both in clinically healthy cohorts and in CVD cohorts to be a predictor of future cardiovascular events. 8 Certain traditional risk factors beyond ageing have been associated with arterial stiffness including insulin resistance/metabolic syndrome.9,10 Several studies have reported alterations in fuel-metabolism-related markers both in patients with clinically significant arterial stiffness10–12 and in subjects with subclinical changes in arterial stiffness.9,13–15 One interpretation is that arterial stiffening may drive metabolic changes through impairments in distal tissue perfusion. It is also possible that changes in fuel metabolism may be a driver of the process of arterial stiffening. The fact that metabolic alterations are detectable in patients with subclinical vascular changes suggests the latter may be true. Identification of a metabolomic signature that is associated with arterial stiffness in aged adults may therefore reveal both pathogenic mechanisms that lead to disease and markers that allow early identification of those at risk for progression to clinical disease. In this study, we hypothesized that changes in whole-body fuel metabolism are related to alterations in arterial stiffness in ageing adults. The aims of the study were to characterize the relationship between the metabolic profile of a group of community elderly patients without clinical CVD and clinical gold standard measure of arterial stiffness, aortic PWV.
Methods
The subjects were recruited from the Cardiac Aging Study (CAS), a prospective study initiated in 2014 that examines characteristics and determinants of cardiovascular function in elderly adults. CAS participants were recruited from the prospective, population-based cohort, The Singapore Chinese Health Study (SCHS) 16 and directly from the local community. The study sample consisted of men and women who participated in the baseline CAS 2014 examination who had no self-reported history of physician-diagnosed CVD (such as coronary heart disease), stroke or cancer. Informed consent was obtained from participants upon enrolment. The institutional review board of the National University of Singapore and the SingHealth Centralised Institutional Review Board had approved the study protocol.
All participants were examined and interviewed on one study visit by trained study coordinators. Participants completed a standardized form that included medical history and coronary risk factors. Hypertension was defined by current use of antihypertensive drugs or physician-diagnosed hypertension. Diabetes mellitus was defined by current use of anti-diabetic agents or physician-diagnosed diabetes mellitus. Dyslipidemia was defined by current use of lipid-lowering agents or physician-diagnosed dyslipidemia. Smoking history was defined as ever smokers (former or current smoking) or never smokers. Body mass index was calculated as weight in kilograms divided by the square of height in meters. Apart from excluding participants who had history of physician-diagnosed CVD, stroke or cancer, we excluded participants who had abnormal electrocardiograms (ECGs) or possible symptoms of heart disease. All clinical data were obtained on the same day as assessment of arterial stiffness and serum collection.
We performed arterial stiffness measurements in the daytime, in a quiet environment, at stable room temperature. Participants were studied in the supine position. We measured aortic PWV noninvasively using applanation tonometry (SphygmoCor system; AtCor Medical, Sydney, Australia). We measured the distance from the suprasternal notch to the carotid pulse and from the suprasternal notch to the femoral site on the same side. For each PWV measure, 10 s of carotid and 10 s of femoral arterial waveforms were recorded. The software computed the average time elapsed from the tip of the QRS (from sequential ECG) to the onset of the foot of the pressure wave at each site. PWV was calculated from the measurements of the pulse transit time and the distance travelled by the pulse between the two recording sites (measured on the surface of the body in meters) according to the following formula: PWV (m/s) = distance (m)/transit time (s). If the standard deviation (SD) was more than 10% of the PWV value, we repeated the study. PWV measures were made in duplicate; the mean value was reported.
Antecubital venous blood samples (20–30 mL) were taken from consenting participants in the morning; fasting was not required before blood collection. After collection, the blood samples were immediately placed on ice for transportation and were processed within 6 h to obtain serum samples, which were subsequently stored at −80°C.
Serum metabolomic profiling analysis was performed in the Duke-NUS Metabolomics Facility. Thawed serum samples (100 μL) were diluted with 800 µL methanol. After centrifugation of the mixture at 20,817 g for 10 min at 4°C, the supernatant fraction was collected and divided into two parts: one (100 μL) for acylcarnitine analysis and one (10 μL) for amino acid analysis. A pooled quality control (QC) sample was prepared by mixing equal amounts (10 μL) of each extracted serum sample. Measurement of acylcarnitine and amino acid panels was performed as previously described. 17 For free and total L-carnitine analysis, 10 µL of 250 µM d3-L-carnitine was added to 50 µL of plasma. A volume of 20 µL of the mixture was removed for protein precipitation and further dilution using an acidified methanol–water mixture (0.6% HCl in 80% MeOH). Free carnitine was estimated from the supernatant by analysing on an Agilent 6430 Triple Quadrupole LC/MS system and an Agilent XDB-C8 column (100 × 4.6 mm2; particle size = 1.8 µm; Agilent Technologies, CA, USA) kept at 30°C. Chromatography was performed by injecting 1 µ L of the supernatant and eluting by mobile phase A (0.1% formic acid in water) and mobile phase B (0.1% formic acid in acetonitrile) at a flow rate of 0.4ml/min.
The gradient was held at 95% A for 2 min, decreased to 10% A in 0.5 min, then held at 10% A for 0.3 min, finally re-equilibrated back to 95% A in 0.2 min, and held at 95% A for 2 min. Data acquisition and analysis were performed on an Agilent MassHunter Workstation B.06.00 Software. For total carnitine analysis, 10 µL of 1M KOH was added to the remaining d3-L-carnitine and plasma mixture. Hydrolysis was performed by incubating the mixture at 65°C for 15 min, followed by neutralizing with 12 µL 1M HCl. A volume of 20 µL of the supernatant was used for protein precipitation and dilution with acidified methanol–water mixture (0.6% HCl in 80% MeOH), followed by analysis with mass spectrometry as described above.
Clinical characteristics are presented as mean and SD for continuous data and frequency and percentage for categorical data. Linear regression was used to investigate the association between clinical characteristics and PWV.
Metabolites with >25% of values below the lower limit of quantification were excluded from analysis (only C102 was excluded; hence, a total of 83 metabolites were analysed in the final sample). Two subjects who did not have free carnitine and total carnitine measured were inputted with a value of 1. Other missing metabolites were input with 0.01. We normalized the distributions of all metabolites by a logarithmic transformation.
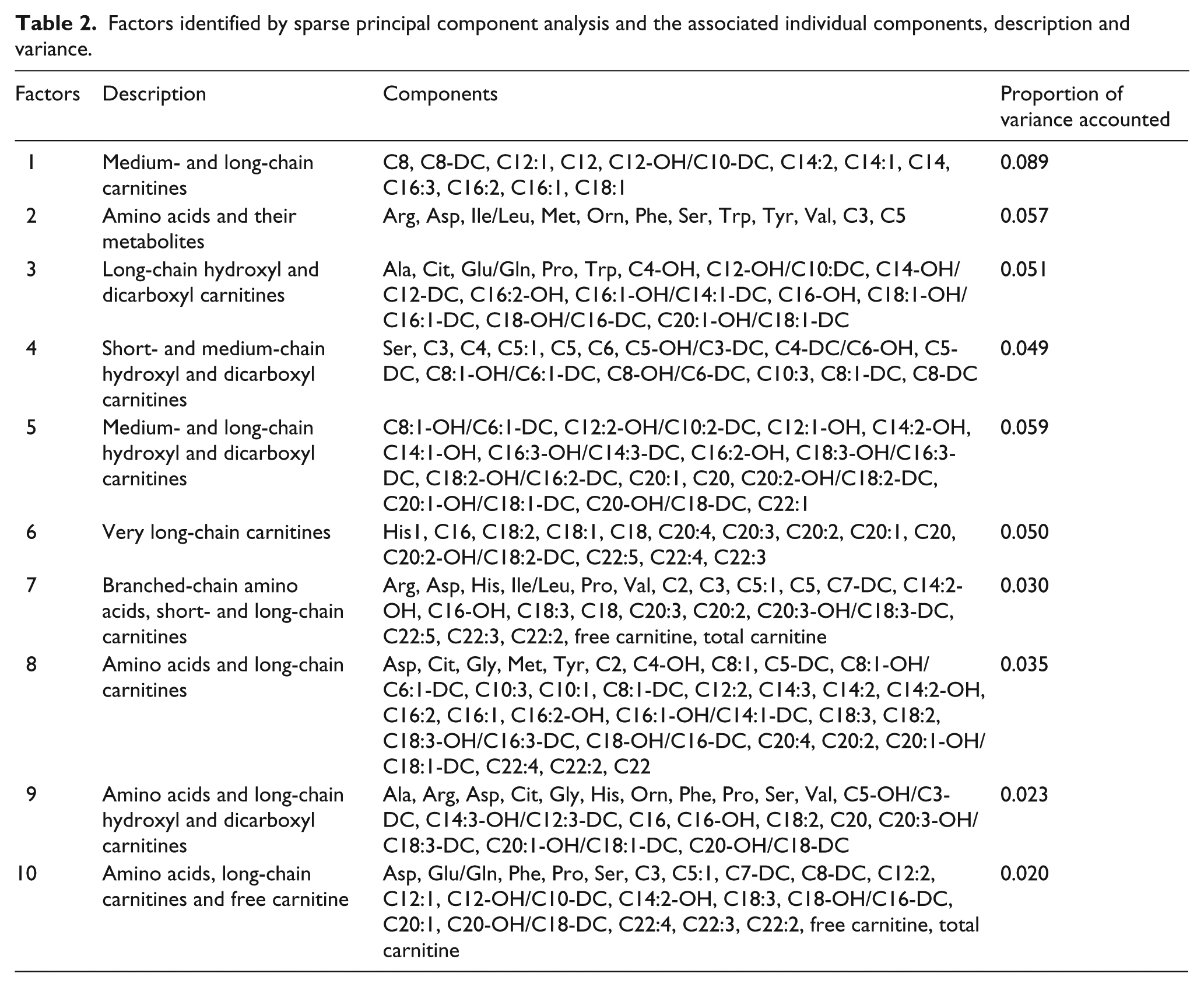
To identify metabolite correlations and reduce the dimensionality of correlated metabolites, we performed sparse principal component analysis (SPCA), which used a penalized matrix decomposition. 18 Comparing with the regular principal component analysis that suffers from the fact of a dense loading matrix from all variables, SPCA is capable of producing sparse loadings which makes it more biologically interpretable. Specifically, we set the orthogonality constraint on each component 18 and the number of components to be 10. We reported the description on each component and the proportion of variance accounted.
To assess the association between the 10 SPCA factors and PWV, we performed the univariate linear regression. For each SPCA factor, we further performed multivariable linear regression adjusted for those significant clinical covariates (age, smoking, dyslipidemia and central systolic blood pressure (SBP)). In this analysis, since central mean arterial pressure (MAP) and central pulse pressure (PP) were highly correlated to central SBP (The Pearson correlation between central SBP and central MAP is 0.77 and 0.81 for central SBP and central PP), we only included central SBP into the multivariable model.
All statistical analyses were performed using STATA 13 (College Station, TX, USA), while the SPCA and correlation matrix heatmap showing pairwise correlations between metabolites and PWV were performed by R. For all analysis, a two-tailed p-value of <0.05 was considered significant.
Results
A total of 141 participants (mean age = 70.6 ± 11.2 years; 59 women) were included in this analysis. All of them completed metabolomic profiling. The majority of participants had vascular risk factors of hypertension (54.6%), dyslipidemia (50.4%) and diabetes mellitus (23.4%). The central systolic and diastolic blood pressures of the participants were 139 ± 18 mmHg and 76 ± 11 mmHg, respectively. Baseline clinical characteristics of the study sample are presented in Table 1.
Baseline clinical characteristics of study participants.
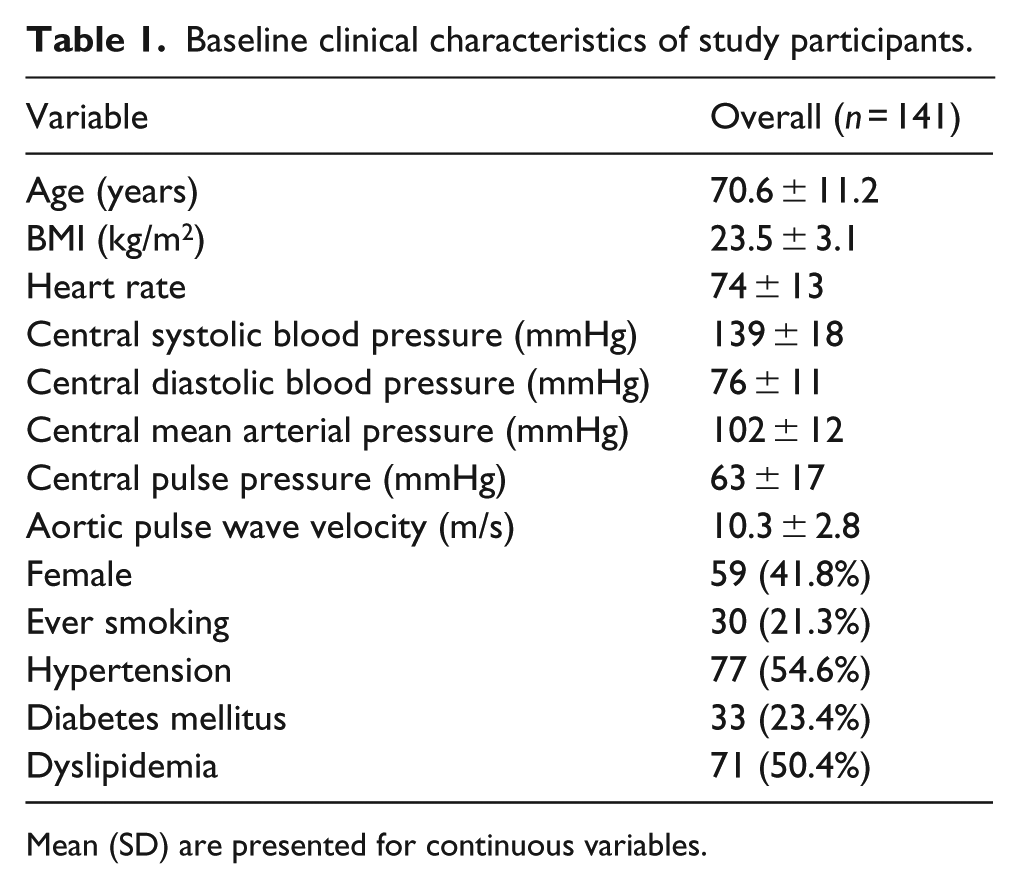
Mean (SD) are presented for continuous variables.
On univariate analysis, age (β = 0.10, p < 0.0001), smoking status (β = 1.32, p = 0.02), dyslipidemia (β = 1.22, p = 0.01), central SBP (β = 0.05, p < 0.0001), central MAP (β = 0.04, p = 0.03) and central PP (β = 0.05, p ⩽ 0.0001) were significantly associated with PWV.
We analysed 83 metabolites comprising 65 acylcarnitine metabolites, 16 amino acid metabolites and 2 carnitine metabolites. The list of measured metabolites and their corresponding raw values are presented in Supplementary Tables S1–S4.
Correlations for the 83 metabolites were assessed using the Pearson correlation analysis with adjustment for age, smoking, dyslipidemia and central SBP (Figure 1). We observed positive correlations between amino acids histidine and PWV, and negative correlations between methionine, valine and PWV. For the acylcarnitine species, we observed positive correlations between C6, C16-OH, C18:1, C18:3-DC and PWV.
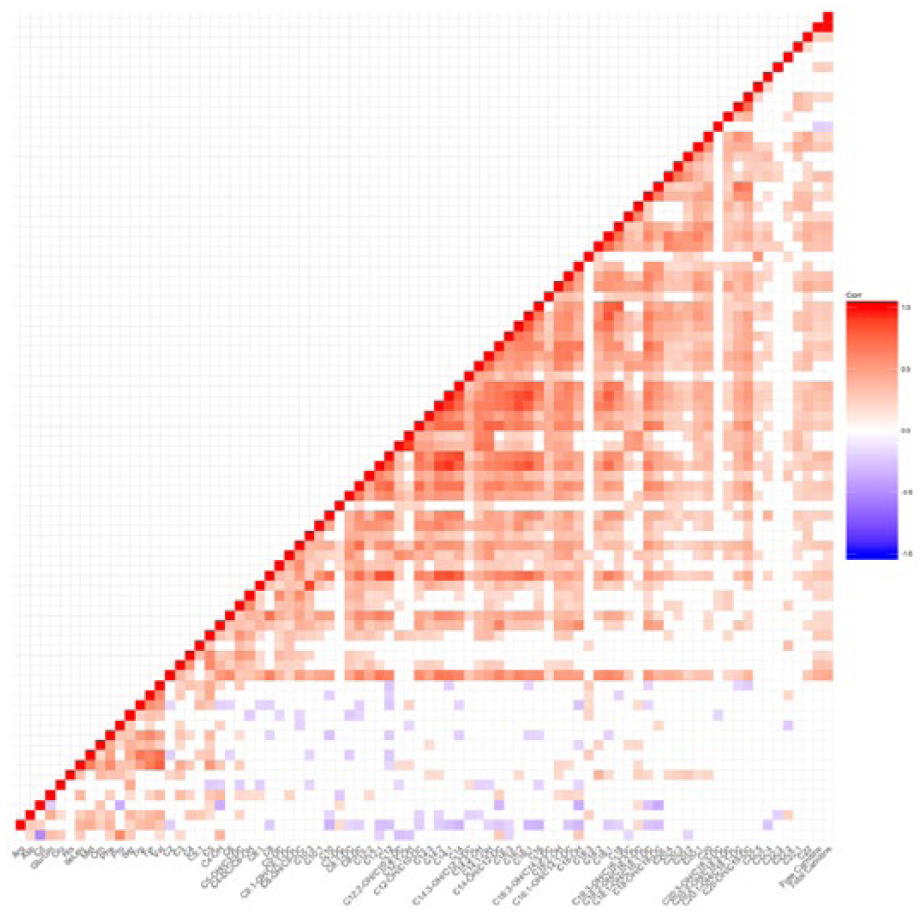
Correlation matrix heatmap.
SPCA identified 10 metabolite factors clustering in biologically related groupings (Table 2). At univariate analysis, Factors 1, 4 and 5 were associated with PWV (Table 2). Generally, these three factors increased with PWV (β = 0.18, p = 0.037; β = 0.28, p = 0.015; β = 0.31, p = 0.004). After adjustments for clinical covariates such as age, smoking, dyslipidemia and central SBP, only Factor 5 (medium- and long-chain dicarboxyl/hydroxyl acylcarnitines) remained independently associated with PWV (β = 0.24, p = 0.015) (Table 3).
Factors identified by sparse principal component analysis and the associated individual components, description and variance.
Univariable and multivariable association of metabolomic factors with pulse wave velocity.
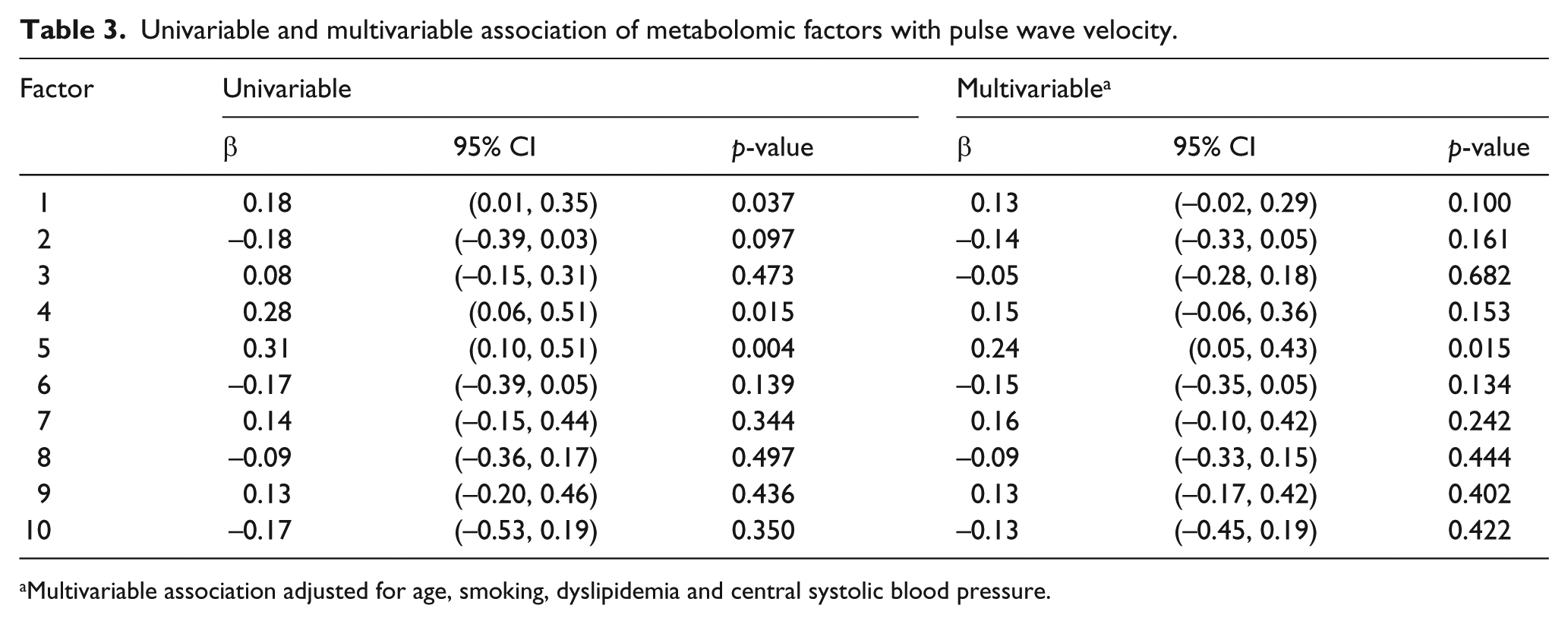
Multivariable association adjusted for age, smoking, dyslipidemia and central systolic blood pressure.
Discussion
In this study, we used a targeted, quantitative metabolomic profiling approach in a community cohort of aged adults to identify a group of circulating metabolites that were significantly associated with arterial stiffness, independent of standard clinical risk factors.
The current wealth of literature pertaining to metabolomics in CVD is largely focused on symptomatic cohorts with clinical CVD.19–22 While there are community-based studies that have looked at the association between metabolomic signatures and CVD and function,23,24 few have studied the elderly. The study by Rizza et al. 25 looked at a high-risk cohort of elderly subjects in which over half of the participants had documented coronary artery disease or stroke. Rizza et al. found a distinct signature comprising medium- and long-chain acylcarnitines that predicted major adverse cardiac events in this high-risk elderly population. This finding suggests that mitochondrial beta-oxidation pathways are linked to increased cardiovascular risk.
Our results demonstrate an association between medium- and long-chain dicarboxyl/hydroxyl acylcarnitines and arterial stiffness in elderly subjects. The dicarboxyl acylcarnitines are generated via the omega-oxidation pathway which is initiated in the endoplasmic reticulum 26 followed by further processing in the peroxisome27,28 and then likely continuing on in the mitochondria (Figure 2). Hydroxyl carnitines are derived from peroxisomal alpha-oxidation of branched-chain fatty acids. Thus, elevation of these medium- and long-chain dicarboxyl and hydroxyl acylcarnitines potentially represents the disturbances in endoplasmic reticulum, peroxisome and/or mitochondrial function. 29 Disturbances in fuel oxidation pathways have been previously linked to arterial disease. Zagura et al. 11 used PWV to study male subjects with symptomatic peripheral arterial disease. They found a signature comprising lactate, carnitine and amino acids that were associated with PWV in their cohort. The group measured a subset of the acylcarnitines included in our study and did not find any association between acylcarnitines and PWV. The patients in the study differed from our study population with regard to age (mean age of 66 years vs 70.6 for our study) and the fact that their study patients suffered from symptomatic occlusive arterial disease. In a study of patients with established CVD, disturbances in the dicarboxyl/hydroxyl acylcarnitine pathway were able to predict incident cardiovascular events. 22 The metabolomic pattern reported in this study closely overlaps our findings and lends support to the notion that alterations in metabolism, arterial stiffness and overt cardiovascular events represent a continuum of pathologic changes which may have special relevance in the ageing population. Although more data from aged cohorts similar to ours are needed to confirm our results, the accumulation of acylcarnitines and other fuel metabolism intermediates observed in all of the studies may be indicative of mitochondrial dysfunction and/or defects in cellular fatty acid oxidation as an important driver and marker of ageing-associated CVD.
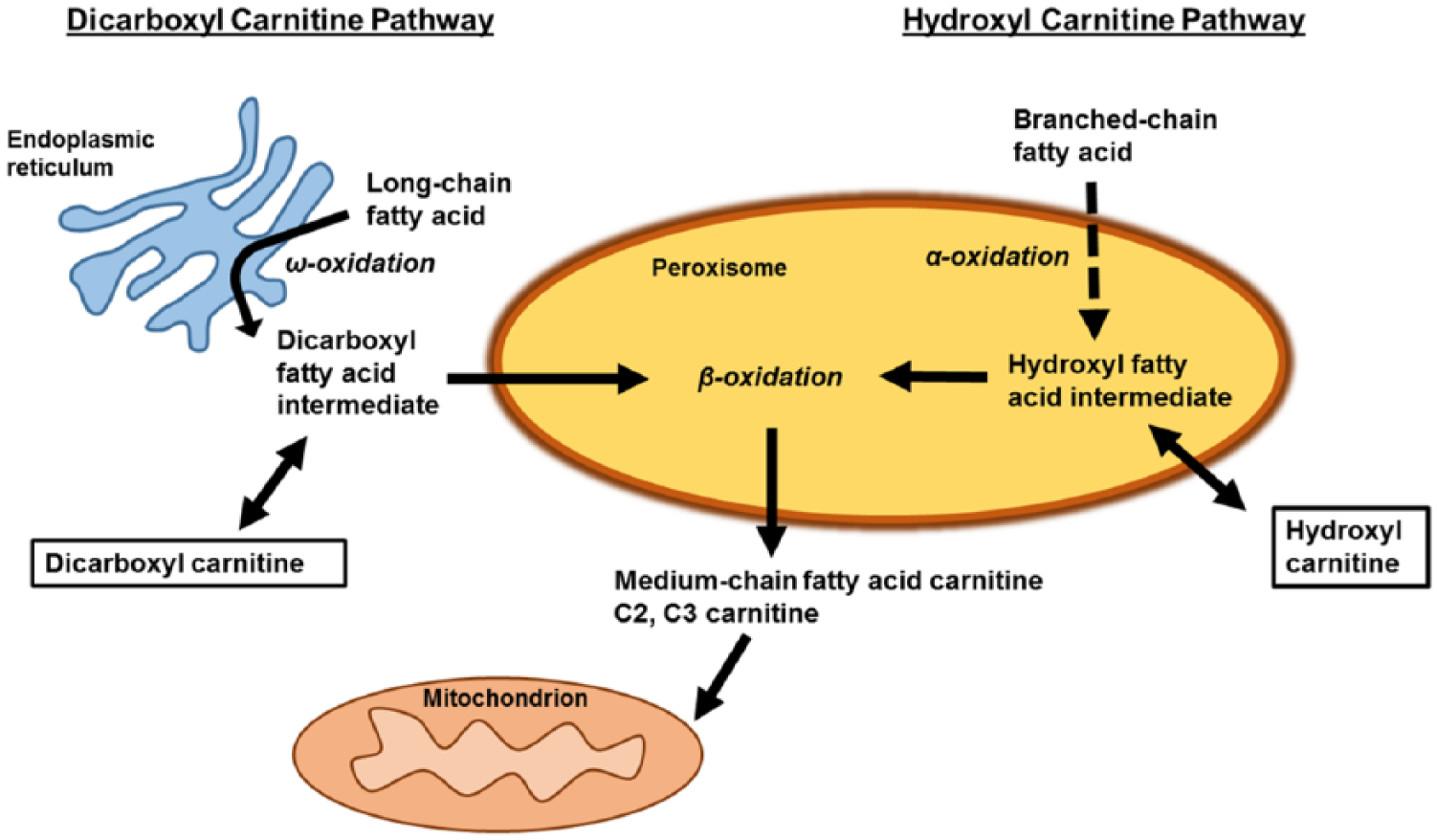
Pathway for production of dicarboxyl and hydroxyl carnitines.
Our results emphasize the need for identification of metabolomic signature profiles in particular cohorts. Metabolomics has the potential to identify new pathophysiological pathways, assist in finer risk-stratification and personalized cardiovascular care, 30 particularly in the growing ranks of the elderly. Our study design is cross-sectional and hence we cannot infer causal relationship between arterial stiffness and metabolites. The serum samples were obtained in a non-fasting state which may potentially introduce analytic differences in post-absorptive states between the subjects studied. As a community-based driven study, we acknowledge challenges in getting subjects to fast in order to participate in these studies. Future studies comprising fasting samples may provide additional insights as to the effect of fasting on similar analyses. Sample size was relatively small although we were able to identify statistically significant associations within the group. Future longitudinal follow-up in a larger cohort may provide greater power as well as further insights as to causality. One advantage of our study was the prospective collection of blood samples at the same time as the cardiovascular measurements.
A circulating metabolomic profile comprising medium- and long-chain dicarboxyl and hydroxyl acylcarnitines, likely reflecting changes in cellular fatty acid oxidation, is independently associated with arterial stiffness among aged adults without clinical CVD, and independent of known risk factors including elevated blood pressure. Our results indicate that an upstream metabolic perturbation is detectable in aged adults. These findings may be useful to advance mechanistic understanding of arterial stiffness among aged adults before clinical disease.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The Cardiac Aging Study has received funding support from the National Medical Research Council of Singapore (NMRC/TA/0031/2015 and NMRC/OFIRG/0018/2016)), Hong Leong Foundation and Edwards Lifesciences. Participants from the Singapore Chinese Health Study were supported by the United States National Institutes of Health (NIH R01 CA144034) and UM1 CA182876. The funder had no role in the design and conduct of the study; collection; management, analysis and interpretation of the data; and preparation, review or approval of the manuscript.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.