
Abstract
Obesity is a major burden on healthcare systems worldwide due to the association with numerous complications, arguably the most important of which are the development of type 2 diabetes and cardiovascular disease. Both are thought to develop from similar origins and occur at variable rates in obese individuals, including those with similar body mass indices. This phenomenon is likely a result of an increased susceptibility for the storage of excess fat in the wrong place, namely, ectopic fat surrounding the liver, pancreas and muscles. This triggers a concatenation of events leading to insulin resistance and inflammation which culminate in an increased atherothrombotic potential due to the dysfunction of vascular endothelial cells causing accelerated atherosclerotic plaque formation and a pro-thrombotic phenotype. The degree of weight loss following different interventions is well documented but it is less widely known what effect weight loss by various means has on the deleterious process mentioned above, in particular their effects on cardiovascular events. This review summarises the processes leading to increased vascular risk in obesity and examines the effects of currently available weight loss strategies on reversing these processes and how this translates to cardiovascular disease.
Introduction
Obesity is a major, global health problem and has been placed in the top three of social burdens caused by humans, just below smoking and war/acts of terrorism. It is now estimated that around 2.1 billion people worldwide (30% of the world’s population) are overweight or obese, which is associated with a reduced life expectancy, independently of factors such as smoking 1 and much of this increased mortality is due to cardiovascular disease (CVD). 2 This is, in part, due to a clustering of cardiovascular risk factors in obesity such as hypertension, dyslipidaemia and type 2 diabetes; however, obesity in itself can also be considered an independent risk factor for CVD. 3 The aim of this review is to provide an up-to-date brief overview of the mechanisms linking obesity with CVD and explore latest evidence related to modulation of vascular risk in overweight individuals. Pubmed was used to search for relevant articles using the following search terms: ‘obesity and cardiovascular disease’, ‘overweight and cardiovascular disease, ‘diet and cardiovascular disease’, ‘orlistat and cardiovascular disease’, ‘lorcaserin and cardiovascular disease’, ‘naltrexone/bupropion SR and cardiovascular disease’, ‘phentermine/topiramate ER and cardiovascular disease’, ‘GLP-1 and cardiovascular disease’ and ‘bariatric surgery and cardiovascular disease’.
Obesity, inflammation and atherosclerosis
Excess central adiposity, comprising both visceral and subcutaneous adipose tissue, creates a chronic, low grade inflammatory state which predisposes to insulin resistance and a pro-thrombotic phenotype4–6 and can directly affect cardiac structure and reduce left ventricular function. 7
The development of atherosclerotic plaques is a chronic inflammatory process triggered, in part, by endothelial cell (EC) dysfunction causing inflammatory cell infiltration and increased lipid deposition coupled with accelerated smooth muscle proliferation, culminating in the formation of the atheromatous lesion. EC dysfunction results in a reduction in the bioavailability of nitric oxide (NO) and subsequently increased platelet activation, 8 increased smooth muscle cell proliferation and increased expression of adhesion molecules. 9 This in turn leads to recruitment of inflammatory cells such as macrophages into the vessel wall, uptake of oxidised low-density lipoprotein (LDL) resulting in foam cell formation. These undergo fibrotic changes, secondary to the local inflammatory process mediated by various cytokines, thereby forming the atherosclerotic plaque.10–12 Obesity is associated with an inflammatory milieu, insulin resistance and a disordered haemostatic system, which are key mechanisms for increased risk of atherothrombotic events (Figure 1).
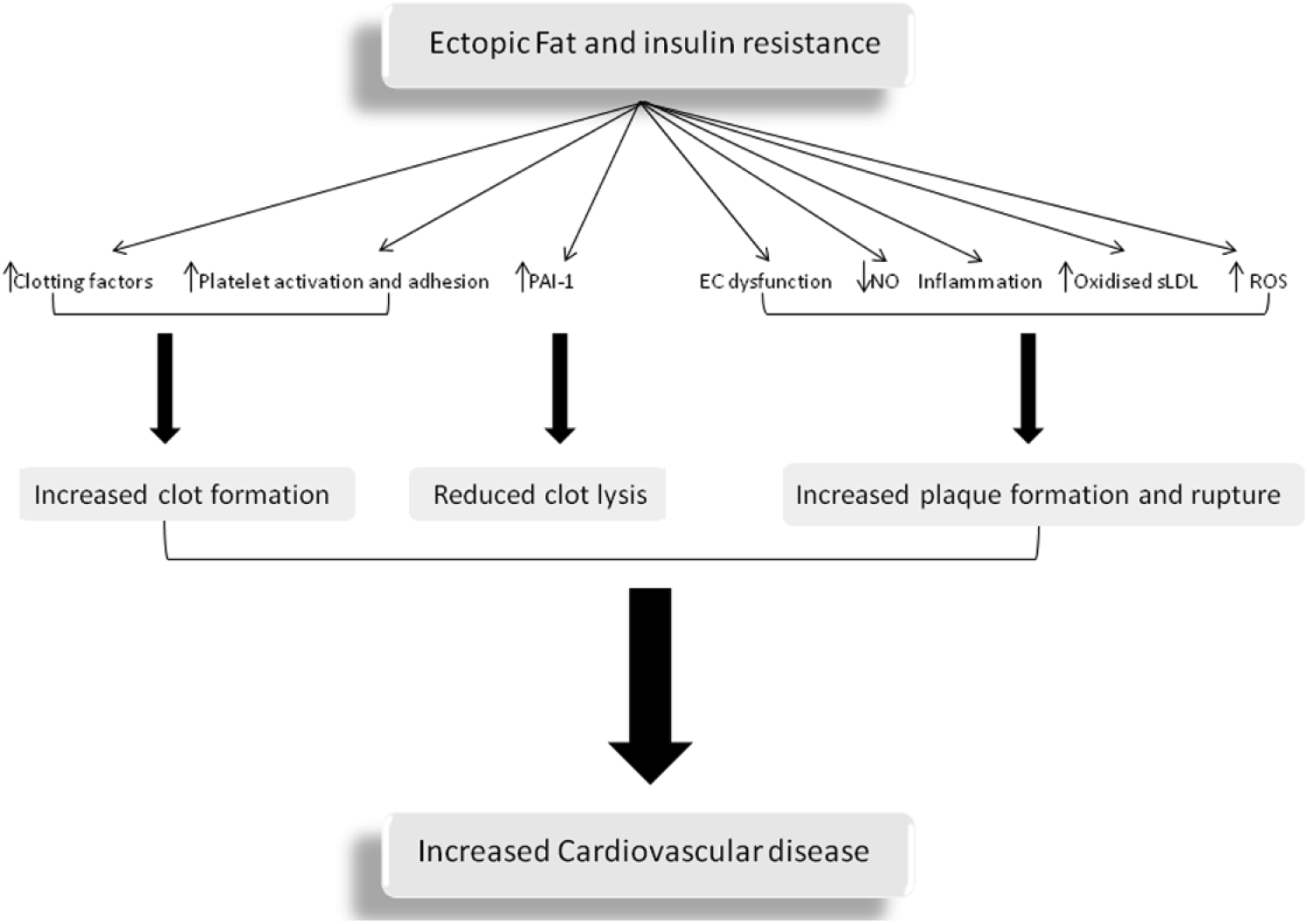
Summary of the contributing factors to cardiovascular disease in obesity. The presence of excess ectopic adipose tissue leads to the development of insulin resistance leading to endothelial cell (EC) dysfunction, reduced nitric oxide (NO) availability, increased oxidation of pro-atherogenic small LDL cholesterol, increased reactive oxygen species (ROS) and increased inflammatory cytokines such as IL-6 and TNF-α. These events lead to accelerated atherosclerotic plaque formation and increased susceptibility to plaque rupture. Concurrently, there is a pro-thrombotic environment triggered, leading to increased generation of clotting factors (tissue factor, fibrinogen, FVII and FVIII), increased platelet activation and adhesion and reduced clot lysis by increased production of the anti-fibrinolytic protein plasminogen activator inhibitor-1 (PAI-1).
It is not fully understood how inflammation is triggered within adipose tissue but what is clear is that hypertrophied adipocytes in obesity release a number of pro-inflammatory mediators including cytokines such as interleukin (IL)-6 and tumour necrosis factor alpha (TNF-α), adipokines such as leptin as well as retinol binding protein 4 (RBP4), complement C3, free fatty acids (FFAs) and monocyte chemoattractant protein-1 (MCP-1).13–15 This is turn results in increased recruitment of immune cells, predominantly macrophages, which once activated further drive this inflammation through the release of IL-6, IL-1β and TNF-α.16–18
Mechanisms for increased atherothrombosis in obesity
Atherosclerotic plaque formation
The presence of increased circulating leptin, IL-6 and TNF-α hastens atheromatous plaque formation by increased expression of chemoattractant proteins MCP-1 and vascular cell adhesion molecule-1 (VCAM-1) within ECs leading to increased macrophage infiltration and smooth muscle cell proliferation together with increased lipid deposition through reduced lipoprotein lipase activity.19,20 There is increased generation of mitochondrial reactive oxygen species (ROS), resulting in further EC dysfunction, due to reduced NO availability, which in turn increases the activity of the transcription factor NF-kB and expression of TNF-α and IL-6. 21 In addition, IL-6 induces the expression of C-reactive protein (CRP) in the liver, which is strongly associated with CVD and may contribute to atherosclerosis by increasing expression of adhesions molecules as above. 22 IL-6 also reduces the production of adiponectin from adipocytes which has potent anti-inflammatory and anti-atherogenic properties as it reduces the generation of ROS, increases NO production and reduces the activity of NF-κB, all of which help maintain EC function and limit the development of foam cells within arterial cell walls.
Insulin resistance frequently follows the development of inflammation associated with obesity and this has further deleterious effects on vascular ECs. Lipolysis within insulin sensitive adipose cells is finely balanced with energy requirements, but this is lost in insulin resistance causing increased lipolysis and release of FFA. Much of the pro-atherosclerotic effects of insulin resistance relate to the associated dyslipidaemia encompassing elevated triglycerides, low high-density lipoprotein (HDL) cholesterol and altered composition of LDL cholesterol. 23 Within insulin-resistant hepatocytes, there is increased production of triglyceride-rich very low–density lipoprotein (VLDL) which results in less removal of cholesterol from the vasculature as HDL metabolism is increased. Hepatic lipase and cholesterylester transfer protein (CETP) activity leads to greater numbers of small LDL particles which are more readily oxidised and infiltrated into the EC wall producing foam cells. Increased circulating FFA also contributes directly by reduced NO availability and increased ROS as described above.
Thrombosis
Obesity is associated with a pro-thrombotic state and relates to increased plasma levels or activity of numerous coagulation factors and fibrinolytic proteins24,25 which is largely a consequence of the inflammatory, insulin-resistant state described. Following tissue injury, clot formation is initiated by tissue factor (TF) on the surface of damaged ECs. A cascade of enzymatic reactions ensues that activate a number of coagulation factors (F), ultimately resulting in the generation of thrombin, which has two important functions, first converting soluble fibrinogen to insoluble fibrin and second activating FXIII, which stabilises the fibrin clot through cross linking of fibrin fibres. The process is regulated by the fibrinolytic pathway, which is activated upon fibrin formation, and helps localise clot formation and initiates clot lysis through the actions of plasmin 26 (Figure 2).
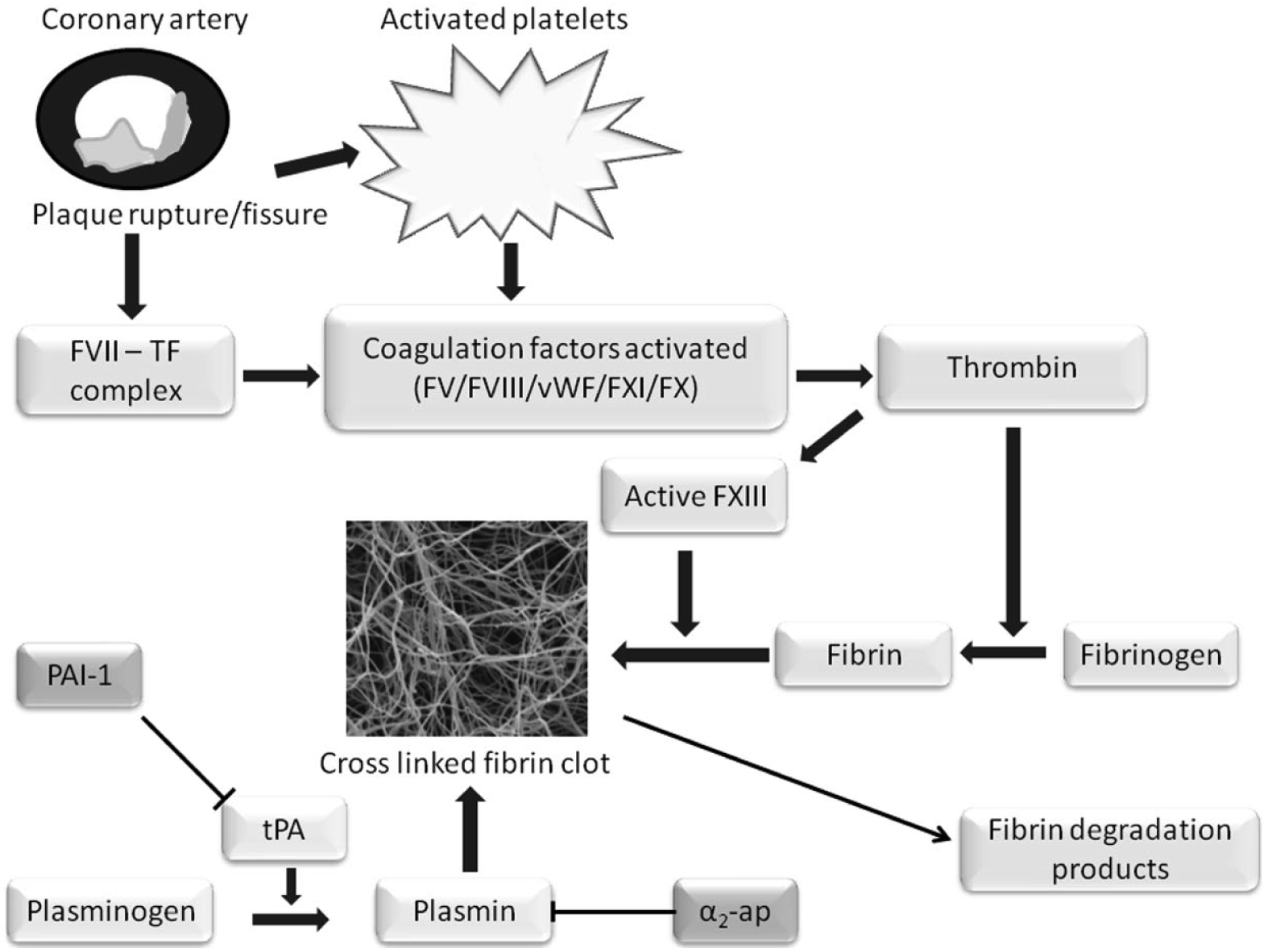
Simplified illustration of fibrin clot formation and fibrinolysis. Following plaque rupture or fissure, a TF/FVII complex is formed and platelets are activated. This results in the activation of numerous coagulation factors and ultimately the conversion of prothrombin to thrombin, which converts soluble fibrinogen to fibrin. A network of fibrin fibres is formed which is stabilised by the actions of FXIII, cross linking the fibres. Clot lysis occurs following the conversion of plasminogen to plasmin by tissue plasminogen activator (tPA) which generates fibrin degradation products. Fibrinolysis is regulated by plasminogen activator inhibitor-1 (PAI-1) which inhibits tPA and α2-antiplasmin (α2-ap) which inhibits plasmin activity.
Fibrinogen levels are increased in obese individuals, most likely due to increased hepatic production resulting from enhanced IL-6 production. 27 Hyperfibrinogenaemia is associated with CVD and ex vivo generates a compact clot structure that is more resistant to fibrinolysis. 28 Increased plasma levels of other coagulation factors such as factors VII and VIII also occur in obesity, which is linked to coronary artery disease (CAD). Moreover, pro-inflammatory cytokines are responsible for increased hepatic and adipose release of the anti-fibrinolytic agent plasminogen activator inhibitor 1 (PAI-1) and TF.29–31 TF initiates the development of the insoluble fibrin clot and is known to be elevated in patients with CAD. PAI-1 is a key anti-fibrinolytic protein and elevated levels are associated with CVD due to diminished clot lysis. 27 Finally, the adipokine leptin has also been implicated in the increased thrombosis potential by increasing the expression of TF from monocytes and also EC in coronary arteries. 32
Platelet activation, another important factor in the development of atherothrombosis, is increased in obesity, thus enhancing clot formation.32,33 Platelets have a wide variety of surface receptors and secrete numerous molecules linked to inflammation 34 and thus numerous abnormalities associated with obesity contribute to increased platelet aggregation, including reduced NO production, reduced adiponectin secretion and insulin resistance within the platelet. Platelet anti-aggregating actions are provided by NO and prostaglandin I2, which is enhanced by insulin receptor signalling and consequently is lost in insulin-resistant obesity. Insulin also inhibits the release of platelet TF, and thus this mechanism is lost in insulin resistance. Moreover, elevated circulating IL-6, TNF-α and leptin also have a deleterious effect by increasing platelet activation. 32
Effects of weight loss on vascular risk and the differential effect of various management strategies
The reversal of the above processes through weight loss theoretically should lead to a reduction in CVD. Population-wide weight loss has been demonstrated to improve CVD mortality, as observed during the Cuban economic crisis of the early to mid 1990s during which time the average weight of the population fell by 4–5 kg with a resultant decline in CVD mortality. 35 However, reduction in vascular risk by weight loss can vary according to the method applied, and the degree of vascular protection differs considerably between individuals by mechanisms that are only partially understood.
Diet and lifestyle
Weight loss and surrogate cardiovascular markers
A number of studies have explored a wide range of diets and lifestyle interventions, including low carbohydrate, low fat, glycaemic index and Mediterranean style diets with or without increasing physical activity. Full details of the effects of such interventions on cardiovascular risk in patients with and without diabetes can be found elsewhere 36 and a brief summary of the main findings is provided here. The amount of weight loss obtained by diet and lifestyle interventions in clinical trials is generally between 3% and 10%, with greater deficits seen in the short term. This weight loss is often associated with improvements in cardiovascular risk factors such as lipid profile (reduced triglycerides and total cholesterol and elevated HDL cholesterol) and blood pressure. This degree of weight loss resulting from dietary and lifestyle changes has been linked with amelioration of the inflammatory state with reduced plasma levels of CRP, IL-6, leptin and C3, and an improvement in insulin resistance. 37 Adherence to a Mediterranean style diet also appears to be anti-atherogenic by reducing oxidation of LDL cholesterol and improving insulin sensitivity and endothelial function. The mechanisms are not wholly understood but are likely to be independent of weight loss and relate to the dampening of the pro-inflammatory state due to the macronutrients that constitute the Mediterranean diet.38,39 Severe caloric restriction with a very low–calorie diet (VLCD), typically around 600 kcal/day, can also improve insulin sensitivity. 40 Improvements have also been noted to coagulation parameters following lifestyle interventions, with reduced plasma levels of PAI-1and fibrinogen after mean weight loss of 7%–10% which resulted in improved fibrinolysis of fibrin clots ex vivo. 41
Cardiovascular outcomes
The question that arises: do these changes in surrogate cardiovascular markers translate clinically into improved outcome?
The use of a Mediterranean style diet appears the most fruitful with a reduction in cardiovascular events in primary and secondary prevention studies of obese participants with and without diabetes.42,43 The recent randomised controlled trial of intensive lifestyle intervention in type 2 diabetes mellitus (T2DM), LOOK AHEAD, failed to demonstrate improvement in CVD outcomes (a composite of death from CVD causes, nonfatal myocardial infarction, nonfatal stroke or hospitalisation for angina, occurring in 15.7% and 16.3% of participants in the intensive and control arms) after a mean follow-up period of 9.6 years compared to control despite achieving weight loss of 6% and 3.5%, respectively, by the end of the trial. 44 Improvements were noted in HbA1c, blood pressure and diabetes remission in the intervention arm over control and suggest that changes to diet composition, such as a Mediterranean style diet, confers additional CVD benefits over and above calorie restriction as described above. Other factors that may account for the lack of improvements in CVD outcomes are that improvements in cardiovascular risk factors, such as HbA1c, blood pressure and waist circumference, in the intervention group gradually diminished over the course of the study and suggest a return to the deleterious inflammatory, insulin-resistant state over time (markers of inflammation and insulin resistance were not measured). An explanation may also lie with the Da Qing Diabetes Prevention programme that only demonstrated significant reduction in CVD events in the intervention group 23 years after a 6-year intensive lifestyle programme and so beneficial effects on CVD may take time to come to fruition post-intervention. 45 Levels of LDL cholesterol were also higher in the LOOK AHEAD intervention group compared to control and may have contributed to increased atherosclerotic plaque formation. The cohorts were also all at relatively high risk of developing CVD at the outset and the ubiquitous use of medications such as statins and antihypertensive agents, for example, in the both arms may account for the reduced incidence of CVD events overall.
The important role of exercise in weight management is increasingly understood in terms of improving CVD risk. 46 Alone, exercise is unlikely to achieve clinical meaningful weight loss, unless it is high intensity exercise and as such patient education is important to ensure realistic goals are set and aid compliance. 47 To complicate matters, cardiorespiratory fitness is associated with improved CVD mortality, with lower rates observed in overweight fit individuals compared to healthy weight, unfit individuals. 48 Physical activity in conjunction with dietary adjustments appears to have greater beneficial effects on weight, fat mass, blood pressure and insulin sensitivity 49 than either in isolation and thus it is important that diet and physical activity are discussed as a single intervention. Therefore, the scientific, and social, obsessions with weight reduction alone is not enough to reduce CV risk, at least in the medium term, and a ‘package of changes’ is required to achieve meaningful reduction in vascular risk.
Pharmacotherapy
In clinical practice, supplementing dietary and lifestyle modifications with pharmacotherapy in order to achieve clinically meaningful weight loss is a common and popular scenario. In Europe, there are three anti-obesity drugs approved for use, namely, orlistat, liraglutide and naltrexone/bupropion combination, although only orlistat can currently be prescribed in the United Kingdom. Two further agents are approved in the United States, lorcaserin and combination phentermine/topiramate ER.
Weight loss and surrogate cardiovascular markers
Orlistat
Orlistat is a lipase inhibitor that reduces fat absorption by 30%, necessitating reduced fat intake by patients in order to avoid gastrointestinal side effects. The use of this medication in addition to calorie restriction and increased physical activity achieved around 3% greater weight loss than placebo in 1640 patients after 4 years, with favourable effects on CVD risk factors such as reduction in blood pressure, total cholesterol, LDL cholesterol, triglycerides, fasting glucose and increased HDL levels. 50 Short-term use appears to have a beneficial effect on systemic inflammation with reduced plasma CRP levels and increased levels of the anti-inflammatory adipokine, adiponectin. Insulin resistance is also improved as is the progression to T2DM in obese individuals with pre-diabetes.50,51 There is also evidence that orlistat treatment is associated with an improvement in endothelial function, 52 platelet activation 53 and lower levels of PAI-1. 50 Despite these promising findings, there have been no trials to date demonstrating improved CVD outcomes with the use of this agent.
Naltrexone/bupropion SR
The combination medication naltrexone/bupropion SR appears to cause weight loss via its effect on pro-opiomelanocortin cells (POMC) in the hypothalamus. Bupropion, a dopamine and noradrenaline reuptake inhibitor, is thought to increase the anorectic effects of POMC neurons, while naltrexone, an opioid receptor antagonist, blocks the auto-inhibition of these neurons. 54 Compared to placebo (n = 752, weight loss 1.3%), there is around 5% greater weight loss with naltrexone/bupropion SR (n = 992, weight loss 6.4%) at the highest dose after 1 year,55,56 which increases to weight loss of 9.3% (n = 482) at 1 year when combined with intensive behaviour modification (placebo 5.1%, n = 132). 57 There were small but statistically significant improvements in plasma levels of hsCRP, triglcyerides, HDL and insulin resistance but a neutral effect on LDL cholesterol and blood pressure.55,56 It would be expected that blood pressure in particular would improve with this degree of weight loss and thus detrimental vascular effects of this drug need to be evaluated. No data regarding its effect on thrombosis or other inflammatory markers are available and no data regarding cardiovascular outcomes.
Lorcaserin
Lorcaserin leads to centrally induced reduction in food intake via its agonistic effects on serotonin 2C receptors and was approved for use as an anti-obesity medication in the United States by the Food and Drug Administration (FDA) in 2012. Although mean weight loss in 1595 patients compared to placebo at 1 year is modest, at around 3.6%, significantly more subjects achieve >5% weight loss compared to placebo (45% vs 20%) and 22.6% achieve >10% weight loss compared to 7.7% for placebo. In addition to weight loss, there are encouraging effects on CVD risk factors along with improvements in inflammation, insulin resistance and thrombotic potential. Compared to placebo, lorcaserin significantly improves blood pressure and dyslipidaemia associated with obesity, 58 or at least reduces the amount of medication required to adequately control these parameters. 59 Treatment also significantly reduces plasma levels of hsCRP, fibrinogen and insulin resistance as measured by homeostatic model assessment-insulin resistance (HOMA-IR) compared to placebo. 58 No data are available regarding CVD improvements and indeed post-marketing trials are currently ongoing in the United States to demonstrate its long-term cardiovascular safety following withdrawal of other anti-obesity medication such as sibutramine. 60
Phentermine/topiramate ER
This combination compound utilises lower dosages for both individual drugs thus minimising the respective adverse effects and increasing the amount of weight loss, although the exact mechanism for weight loss is not fully understood. Like lorcaserin, it is only approved in the United States for the medical treatment of obesity. The mean weight loss for the highest dose (phentermine 15 mg plus topiramate ER 92 mg) is around 10% compared to 1%–2% for placebo at 1 year, which is maintained up to 2 years.61,62 Greater numbers also achieved >5% and 10% weight loss (687/981, 70% and 467/981, 48%, respectively, at year 2) compared to placebo (204/979, 21% and 72/979, 7%, respectively). Phentermine/topiramate ER is also associated with significant improvements in blood pressure and lipid abnormalities compared to placebo, but there is little evidence of its direct effect on inflammation, insulin resistance and thrombosis. Fasting glucose and insulin levels are significantly reduced in non-diabetes obese patients and its use appears to reduce the progression to T2DM in high-risk individuals. 62 There is no evidence that phentermine/topiramate ER improves cardiovascular outcomes and indeed global use of this medication is limited due to concerns regarding its long-term cardiovascular safety due to the actions of phentermine. Cardiovascular outcome studies attempting to elucidate these outcomes are in progress. 60
Glucagon-like peptide 1 receptor agonists
Several glucagon-like peptide 1 receptor agonists (GLP-1 RA) have been developed for use in T2DM and their beneficial effects on weight, in addition to glycaemic control, are widely accepted. Of those currently in use for T2DM, liraglutide has also recently received approval in Europe and the United States for use in chronic weight management in individuals without diabetes. The Liraglutide Effect and Action in Diabetes (LEAD) trials demonstrated its positive effect on weight, blood pressure, glucose homeostasis, fasting lipids and β-cell function as monotherapy or in combination with other hypoglycaemic agents in diabetes. 63 Subsequent studies using a higher dose (3 mg/day dose) in 2487 obese patients without diabetes also demonstrated impressive results after 56 weeks.64,65 Liraglutide at 3 mg/day produced weight loss of (mean ± standard deviation (SD)) 8.4 ± 7.3 kg compared with 2.8 ± 6.5 kg in placebo-treated individuals, with significantly achieving >5% and >10% weight loss (63.2% vs 27.1% and 33.1% vs 10.6%, respectively). There were fewer cases of diabetes diagnosed along with similar improvements in CVD biomarkers as in the LEAD trials. In addition to its beneficial effects on classic CVD risk factors such as body mass index (BMI), blood pressure, dyslipidaemia and hyperglycaemia in clinical trials, GLP-1 RA have been shown in vitro and in numerous animal models to have anti-atherogenic and anti-inflammatory effects.66–69 Plasma levels of leptin, TNF-α, CRP and PAI-1 have been shown to be reduced in some but not all studies.64,65,68,70 The GLP-1 RA class of agent therefore appears to positively affect the three processes that are known to contribute to the development of atherothrombosis in obesity and thus may advocate their early use in the treatment of obesity in the presence and absence of diabetes. Moreover, there is emerging evidence that this class of agent may also offer a degree of cardio protection by other mechanisms when administered during acute myocardial infarction. Intravenous and subcutaneous administration of exenatide during acute revascularisation procedures appear to reduce the size of infarct and preserve left ventricular function.71,72
Cardiovascular outcomes
There is also the suggestion that the beneficial effects of GLP-1 RA on cardiovascular risk markers may be translated to improvements in cardiovascular outcome with fewer major adverse cardiovascular events compared to comparators noted in retrospective analysis of pooled data.73,74 The Liraglutide Effect and Action in Diabetes: Evaluation of cardiovascular outcome results (LEADER) trial published in June 2016 reported a 22% reduction in cardiovascular deaths in the liraglutide group compared to placebo (hazard ratio (HR), 0.78; 95% confidence interval (CI), 0.66–0.97; p = 0.007) and included patients with and without established CVD. Mean weight loss in the treatment group compared to placebo was modest at around 3 kg and may relate to the fact that around 28% of the liraglutide group were commenced on some form of insulin therapy during the trial. 75 Extending these results to a non-diabetes cohort may be problematic but these are certainly encouraging results.
Bariatric surgery
Weight loss and surrogate cardiovascular markers
Of all the weight loss treatment strategies available, bariatric surgery delivers the greatest amount of weight loss, which is maintained long term. Average weight loss following Roux-en-Y gastric bypass (RYGB) is approximately 30%, and although some degree of weight regain occurs, results from 2010 patients in the Swedish Obese Subjects (SOS) study group suggest around 18% weight loss at 20 years post-operatively. 76 Surgery is also associated with significant improvements in CVD risk factors with reduced rates of dyslipidaemia and hypertension and corresponding improvement in CVD risk scores.77,78 A greater proportion of the weight is lost from the visceral compartment with associated reductions noted in liver enzymes and inflammatory markers, including IL-6, CRP and adipokines such as leptin and C3. Unsurprisingly, insulin sensitivity is also improved 79 and remission of diabetes is believed to be around 70%–80% at 2 years and 30% at 15 years.76,80 The incidence of diabetes is also greatly reduced following surgery compared to the control group at 15 years. 79 The pro-thrombotic environment associated with obesity is also ameliorated with lower plasma levels of fibrinogen and PAI-1 post-operatively, 81 which corresponds to a reduction in the fibrinolysis rates of ex vivo fibrin clots 82 and a reduction in platelet activation in some patients. 83
Cardiovascular outcomes
In contrast to many other weight management therapies, the cumulative effect of these changes post-bariatric surgery translates into long-term cardiovascular benefits with fewer cardiovascular events noted in the SOS study. After a mean follow-up period of 14.7 years, there were 28 cardiovascular deaths and 199 cardiovascular events in the surgery group compared to 49 and 234, respectively, in the control group (adjusted HR, 0.47; 95% CI, 0.29–0.76 and 0.67; 95% CI, 0.54–0.83, respectively, following multivariate adjustment for baseline conditions). 84 A similar reduction in myocardial infarction incidence was noted when patients with diabetes were analysed separately. 79 There is ongoing debate as to the most efficacious surgical procedure, with general consensus that RYGB produces greater weight loss and improvements in comorbid conditions than laparoscopic adjustable bands (LAGB) and vertical sleeve gastrecotomy. 85 There is evidence, however, that LAGB can achieve similar long-term results to RYGB if patients are given appropriate peri-operative care along with long-term follow-up in specialist centres. 86 Despite this multitude of positive effects on the main protagonists of atherothrombosis and benefit on CVD, weight loss surgery is not the panacea of treatment for obesity. Although 90-day mortality is respectable at around 0.2%,76,79 it is important to consider other long-term sequelae such as nutritional deficiencies, hypoglycaemia, osteoporosis, psychiatric issues and the potential need for plastic surgery to remove excess skin. Therefore, a multidisciplinary approach to patient and surgical selection is vital to achieve the aim of improved well-being and reduced CVD in a cost-effective manner.
Discussion
On the face of it, weight loss by lifestyle and dietary changes, medication or surgery reduces systemic and local inflammation, improves insulin sensitivity and ameliorates the pro-thrombotic environment, but with mixed, and inconsistent effects on cardiovascular outcomes (Table 1). The reasons for the varied results observed in clinical trials are unclear, but serve as a reminder of the numerous physiological interactions involved in the development of CVD and its amelioration. The ‘obesity paradox’ may offer some explanation and illustrates the heterogeneous nature of CVD in obesity. Several studies have reported a reduction in coronary heart disease mortality in overweight and obese (class I) subjects compared to normal weight individuals.87–89 These results highlight the inadequacy of BMI as a measure of metabolic dysfunction associated with obesity and does not provide information regarding body composition, fat distribution and cardiorespiratory fitness. There is a strong link between low lean body mass and CVD,90,91 increased visceral and abdominal subcutaneous adipose tissue and CVD 92 along with poor cardiorespiratory fitness and CVD.46,93 If waist to hip ratio is used instead of BMI, there is a graded increased in the rate of myocardial infarction 94 and therefore this may be a better combined maker of obesity/CV risk.
Summary of the effects of weight loss interventions on weight, inflammation, coagulation and cardiovascular disease.
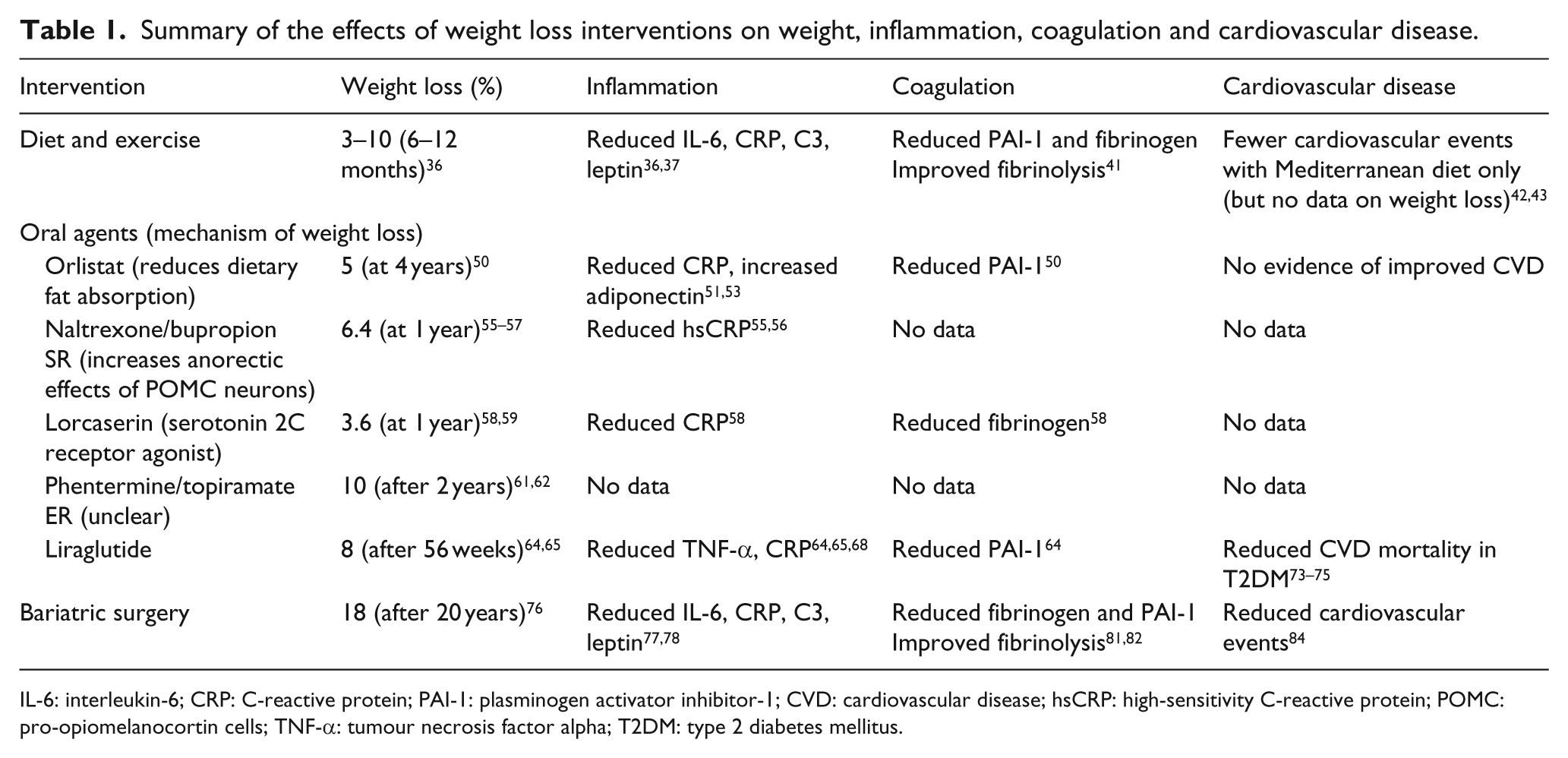
IL-6: interleukin-6; CRP: C-reactive protein; PAI-1: plasminogen activator inhibitor-1; CVD: cardiovascular disease; hsCRP: high-sensitivity C-reactive protein; POMC: pro-opiomelanocortin cells; TNF-α: tumour necrosis factor alpha; T2DM: type 2 diabetes mellitus.
Other than some dietary trials, studies examining the effect of weight loss on CVD have not clearly examined the effect on primary and secondary prevention separately. Surgical trials such as the SOS largely contain patients with no prior history of CVD and the reduction in CVD was linked to baseline fasting insulin levels and not BMI. Another study suggests that those with the highest pre-operative cardiovascular risk appear to gain the most in terms of reduced CVD following surgery,95,96 although it is likely that is weight loss per se that induces the benefits rather than a specific intervention. Future studies of weight loss medications containing patients at high risk of, but without established CVD, may provide useful information regarding their true effect on CVD prevention. However, such studies are often difficult to undertake due to greater numbers of patients needed to demonstrate an effect. Minor improvements in inflammatory markers and insulin resistance have been seen with agents that block cytokine action or transcription97–102 and suggest that other, unknown, factors play a more important role. 103 Further evidence of alternate pathways may be seen by the dramatic, positive effect of the sodium glucose co-transporter 2 inhibitor (SGLT2i), empagliflozin on CVD outcomes in T2DM 104 and again illustrates that despite advances in knowledge, there are still unknowns with regard to CVD. Significant reductions in weight are also observed with SGLT2i and as such they may play a role in weight loss for simple obesity and promising results have been seen in animal studies 105 with clinical trials in progress. Although impressive, the degree of weight loss observed with SGLT2i may not be as great as expected given the degree of calories lost in the urine due to glycosuria. Explanations for this observation may relate to increases in glucagon levels and appetite with SGLT2i 106 and thus combining their use with a GLP-1 RA may potentiate against these adverse effects and enhance the desired weight effects of SGLT2i. Such trials are currently underway and given the apparent positive effect of both class of agent individually on CVD may lead to an exciting management option in obese individuals.
Conclusion
The processes that lead to CVD in obesity are multiple, complex and only partly understood, although the evidence base is ever increasing. What is known is that excess ectopic adiposity leads to IR within hepatocytes, myocytes and pancreatic β cells which exacerbate the inflammatory and pro-thrombotic milieu, producing a perfect storm for the development of atherothrombosis and CVD. Weight loss strategies resulting in around 10% weight loss have positive effects on this pro-atherothrombotic state by dampening inflammation, improving insulin sensitivity and reducing thrombosis potential, in addition to improvements in other classical cardiovascular risk factors such as hypertension, hyperglycaemia and dyslipidaemia.
As with the treatment of diabetes, successful weight management requires an individualised approach to achieve clinically meaningful weight loss (and subsequent maintenance) thus improving cardiometabolic dysfunction and quality of life. The mainstay of treatment should encompass achievable physical activity to increase cardiorespiratory fitness, dietary changes encompassing a Mediterranean style diet and reduced portion size. Progression to pharmacotherapy will be required in many case and of the medical options currently available, GLP-1 RA, as an adjunct to diet and physical activity, appear to offer the most benefit in terms of weight loss, increased insulin sensitivity and amelioration of pro-thrombotic factors culminating in reduced incidence of CVD. Combining GLP-1 RA with SGLT2i in patients without diabetes may also be a therapeutic option in the future.
For many, it will be more appropriate to escalate treatment to bariatric surgery following dietary and lifestyle changes, and there is an argument for changing the criteria for bariatric surgery with less focus on BMI and more towards identifying those with metabolic derangement due to increased proportions of visceral adiposity for example. Bariatric surgery is the intervention associated with the greatest degree of weight loss, and which importantly can be maintained in the long term, with subsequent improvement in CVD. It may be short-sighted however to concentrate solely on CVD as a criteria for surgery as this may ignore the detrimental effects of obesity on cancer risk, arthritis, mental health and quality of life. Until more efficacious weight loss medications are commonly available in the United Kingdom, the only way to significantly improve the health of patients already afflicted with obesity and its complications is to increase the amount of bariatric surgery that is performed, procedures which are relatively safe, with proven long-term health benefits and positive health economics. 107
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.