
Abstract
This translational randomized and vehicle-controlled cross-over study was performed to assess the impact of haem arginate treatment on haem oxygenase-1 induction, endothelial function and insulin sensitivity in subjects with the metabolic syndrome (n = 14). Both treatment periods consisted of 5 days. Haem arginate or vehicle (
Keywords
Introduction
Haem oxygenase (HO) is the rate-limiting enzyme in the breakdown of haem into free iron, carbon monoxide and biliverdin. 1 Biliverdin is then rapidly converted into the anti-oxidant bilirubin by biliverdin reductase. An overwhelming amount of preclinical evidence on the anti-oxidant and anti-inflammatory effects of the inducible isoform HO-1 has fuelled speculations about the therapeutic use of HO-1 induction in human medicine. 2 As the metabolic syndrome (Met-S), type 2 diabetes mellitus and cardiovascular disease are all associated with the presence of oxidative stress and chronic low-grade inflammation,3–5 these conditions constitute an important area for research on the clinical use of HO-1 induction as a novel therapeutic strategy. Indeed, many preclinical experiments on HO-1 induction show promising results in models for Met-S and type 2 diabetes mellitus. 6 HO-1 induction ameliorates Met-S in obese mice, 7 improves insulin sensitivity in insulin-resistant rats, 8 reduces retroperitoneal adiposity and hyperglycaemia in Zucker diabetic fatty rats 9 and protects against endothelial dysfunction in high-fat-fed low-density lipoprotein (LDL)-receptor knockout mice. 10 Interestingly, recent data challenge the supposed beneficial role of HO-1 and conversely suggest that in obese settings HO-1 functioning may be disturbed and may even fuel insulin resistance. 11
Both haemin and haem arginate (HA) have been reported to induce HO-1 expression in healthy volunteers.12,13 Besides, short-term HA treatment has been demonstrated to ameliorate experimental ischaemia-reperfusion injury in healthy volunteers. 14 For the Met-S, type 2 diabetes mellitus or cardiovascular disease, translational data on the impact of HO-1 are currently lacking. We therefore aimed to induce HO-1 by a short-term HA treatment and subsequently assess its effect on insulin sensitivity and endothelial function in subjects suffering from the Met-S.
Materials and methods
Study population
Recruited subjects who met the Met-S criteria 15 were invited to an additional and more extensive screening visit. Participants had to be at least 18 and no older than 70 years of age and were not allowed to have a positive history of drug abuse, active smoking, type 2 diabetes or cardiovascular disease. In addition, subjects were prohibited from using vasoactive medication, statins, aspirin and anti-oxidant vitamin supplements, as these drugs could influence both HO-1 activity and endothelial function. Subjects with clinical evidence of cardiac or pulmonary disease or with biochemical evidence of renal or hepatic abnormalities (results exceeding twice the upper limit of normal range) were excluded. Finally, subjects with unconjugated hyperbilirubinaemia (total bilirubin level > 10 µmol/L) were excluded to avoid participation of subjects with the Gilbert syndrome. All subjects gave written informed consent prior to the first screening visit. The study protocol was approved by the local Medical Research Ethics Committee and consistent with the Declaration of Helsinki.
Study design
In a randomized order and with a wash-out period of at least 7 weeks in between, subjects received both a treatment with HA (Normosang®, Orphan Europe, France; 3 mg/kg with a maximum of 250 mg per dose) and a control treatment with equimolar amounts of
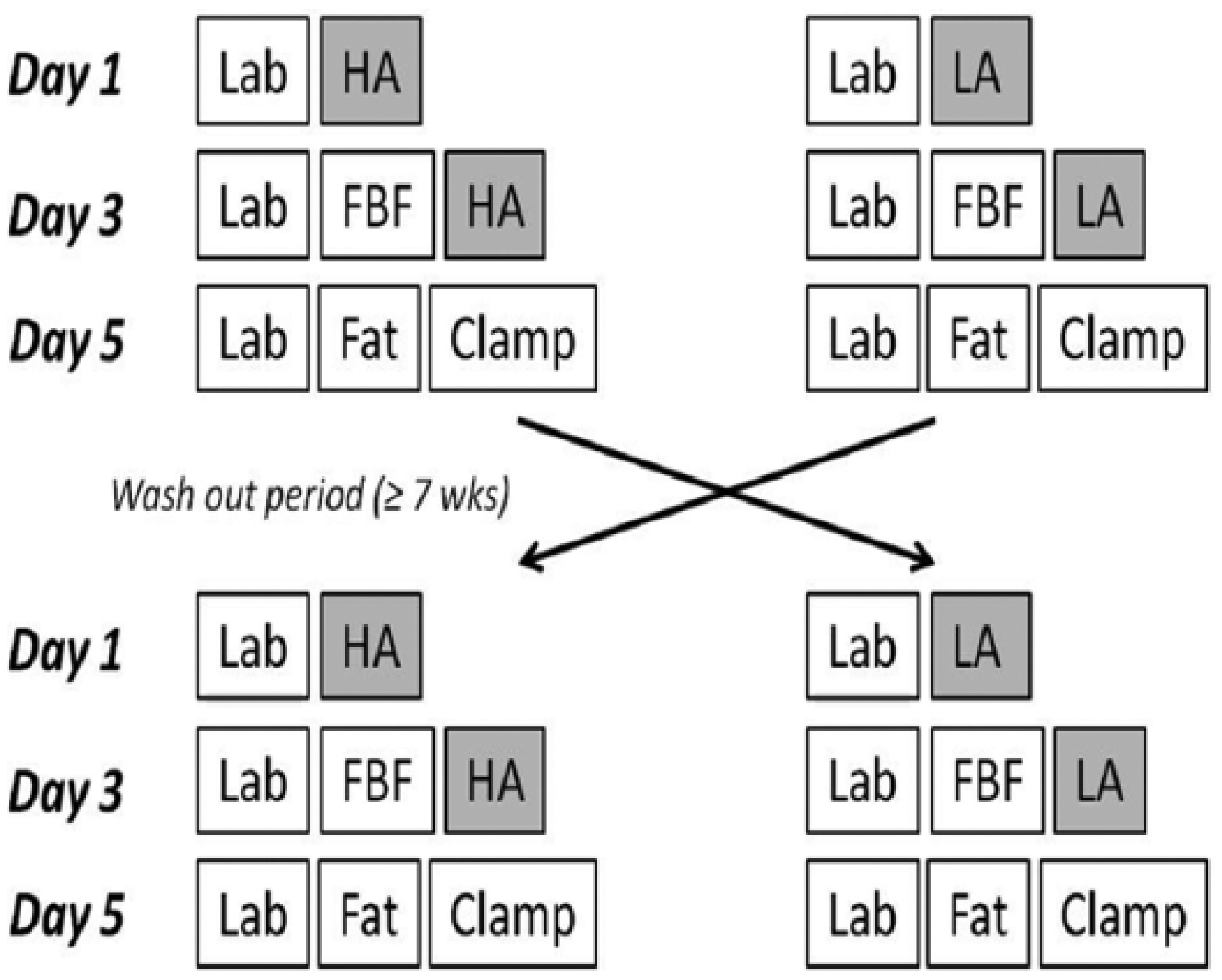
Study overview.
During all visits, venous blood was drawn. Haematological parameters were assessed using an ADVIA 120 Hemalog (Bayer Diagnostic, Tarrytown, NY, USA) and clinical chemistry parameters including bilirubin and ferritin were determined using an Aeroset (Abbott Laboratories, Abbott Park, IL, USA). In addition, plasma samples were stored at −80°C for additional measurements including the ferric reducing ability of plasma (FRAP) assay and plasma haem levels.
A subcutaneous fat biopsy was taken under local anaesthesia (2% lidocaine HCl) after an overnight fast. Adipose tissue was aspired from the lateral aspect of the hypogastrium, inferior to the umbilicus using a Hepafix Luer Lock syringe (Braun, Melsungen, Germany) and a 2.10 × 80 mm Braun Medical Sterican needle. The adipose tissue was washed using a 0.9% saline solution, snap frozen and stored at −80°C until further analysis.
Markers of the HO-1 system
HO-1 was determined on multiple levels including messenger RNA (mRNA) (peripheral blood and adipose tissue) and protein (plasma). In addition, we assessed plasma levels of the HO-1 substrate haem, the HO-1 activity product bilirubin and the iron scavenger ferritin. Finally, plasma anti-oxidant capacity was assessed by means of the FRAP assay.
For the isolation of total RNA from peripheral blood, we used the PAXgene Blood mRNA kit (Qiagen Benelux B.V., Venlo, The Netherlands). Samples were handled according to the manufacturer’s protocol. From adipose tissue, we extracted total RNA using TRIzol Reagent (Life Technologies Europe B.V., Bleiswijk, The Netherlands). RNA concentrations were determined using the NanoDrop 2000 Spectrophotometer (NanoDrop Products, Wilmington, DE, USA). Complementary DNA (cDNA) synthesis was performed using the iScript cDNA Synthesis kit (Bio-Rad Laboratories B.V., Veenendaal, The Netherlands). Real-time polymerase chain reaction (PCR) was performed using the iQ SYBR Green Supermix (Bio-Rad Laboratories B.V.) and the CFX Real-Time System and C1000 Thermal Cycler (Bio-Rad Laboratories B.V.). Expression of the HO-1 gene was normalized to acidic ribosomal phosphoprotein P0 (ARP) gene expression levels. Primer sequences were as follows: ARP, CACCATTGAAATCCTGAGTGATGT (sense), TGACAAGCCCAAAGGAGAAG (antisense); HO-1, TTTCAGAAGGGCCAGGTG (sense), AGACTGGGCTCTCCTTGTTG (antisense) (Biolegio B.V., Nijmegen, The Netherlands).
HO-1 protein content of plasma was determined using the Immuno Set HO-1 (human) ELISA development kit (Enzo Life Sciences BVBA, Antwerp, Belgium).
To assess plasma haem levels, 20 µL pure dimethyl sulphoxide (DMSO) and subsequently 160 µL of a mixture of 250 µL HCl (37%) into 10 mL of acetone were added to 20 µL of plasma. After cooling on ice for 2 min, the sample was centrifuged. Next, the supernatant was analysed by reversed-phase high-performance liquid chromatography. The mobile phase comprised Solvent A (44% methanol, 56% 0.1 M ammonium phosphate buffer pH 3.4, v/v) and Solvent B (100% methanol, v/v) using the following gradient: Solvent B, 0% at t0 to 100% at 14 min; then isocratic to 15 min; down to 0% at 16 min and isocratic to 21 min. The ultraviolet (UV) detector was set at a wavelength of 400 nm. The gradient separation of haem was performed on a GraceSmart RP18 column, 150 × 4.6 mm i.d., 5 µm particle size at a column temperature of 60°C.
The FRAP assay was performed according to the method of Benzie and Strain. 16 FRAP values were obtained using a seven-point calibration curve of known amounts of Fe2+ and expressed in micromole Fe2+ per litre.
Endothelial function
Subjects were instructed to refrain from caffeinated foods and beverages on the day prior to the flow experiments. After overnight fasting, flow experiments were performed using venous occlusion plethysmography as described previously. 17 In brief, FBF was assessed during the successive administration of three increasing doses of acetylcholine (0.5, 2 and 8 µg/min/dL of forearm tissue) and nitroglycerine (0.25, 0.5 and 1.0 µg/min/dL).
Insulin sensitivity
Insulin sensitivity was measured by a 120-min hyperinsulinaemic euglycaemic clamp procedure. These experiments were also performed in the morning after overnight fasting with the subjects in supine position in a quiet temperature-controlled room. Glucose and insulin were administered in an antecubital vein. Insulin (Novorapid, NovoNordisk, Denmark; diluted in 0.9% saline to a concentration of 1 U/mL with the addition of 2 mL of the subject’s blood per 50 mL) was infused at a constant rate of 60 mU/min/m2 body surface area (360 pmol/min/m2). The plasma glucose level was monitored at 5-min intervals by sampling of arterialized blood from a cannulated vein on the dorsum of the controlateral hand, which was placed in a warm-air box. 18 Glucose concentrations were measured using a Biosen C_line GP+ (EKF-diagnostic, Barleben, Germany). Plasma glucose was clamped at a level of 5.0 mmol/L by variable infusion of a 20% glucose solution. Insulin sensitivity (M value) was calculated from the average glucose infusion rate (µmol/min) between 90 and 120 min of the euglycaemic clamp, divided by body weight (kg).
Statistical analyses
Statistical analysis was performed using the SPSS (version 16.0) and SAS (version 8.2) software package. Paired-samples t-test was used to compare Gaussian-distributed data. For analysis of the FBF measurements, the last five flows of each dose were used. Prior to analysis, logarithmic transformation was performed to obtain a Gaussian distribution. The flow data were then averaged per dose and subsequently analysed in a mixed linear model with random factor subjects and fixed factors treatment and dose. The log-transformed data used for statistical analysis are presented in Table 3. The data discussed in the text are medians instead of averages of the original flow data to approximate the effect of logarithmic transformation. Statistical significance was accepted at the 95% confidence level (p ⩽ 0.05).
Results
A summary of the screening, participation and drop out of subjects is provided in Figure 2. A total of 63 obese non-smoking subjects with a negative history of cardiovascular disease were recruited through local advertisements and gave written informed consent for participation. Of these 63, 16 subjects met the Met-S criteria as well as the additional criteria of our protocol. One of these subjects decided to withdraw informed consent prior to the actual enrolment in the cross-over study. Of the 15 subjects who did participate in the study, one experienced a severe headache several hours after the first administration of HA. Additional examinations including head computed tomography (CT) scan did not reveal any abnormality. Because of the severity of the headache, we nevertheless decided to refrain from the second infusion of HA and terminate the participation of this subject. The results of the remaining 14 subjects are presented.
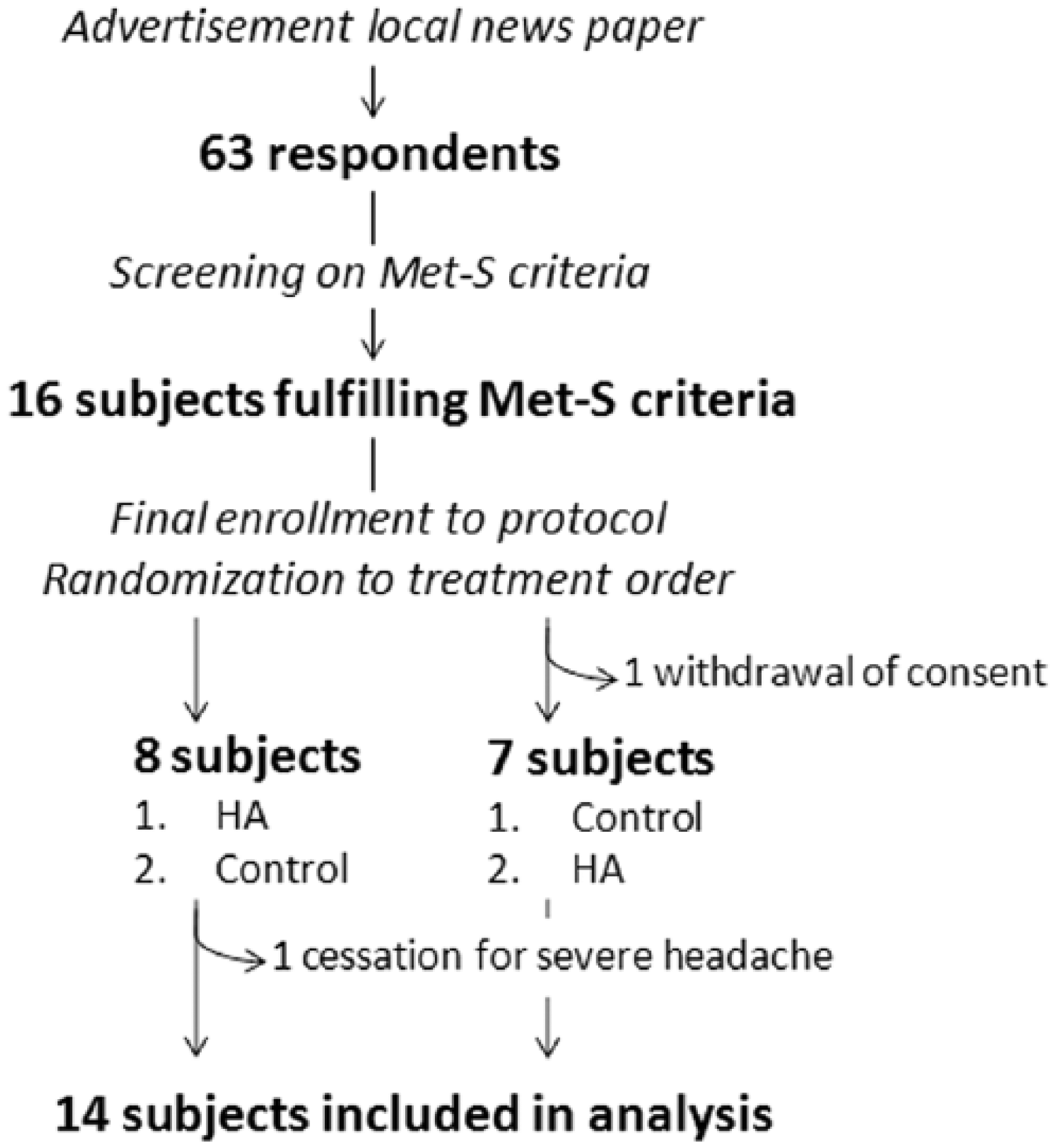
Diagram illustrating the screening, participation and drop out of subjects.
Subject characteristics
Characteristics of the final study population are shown in Table 1. This population consisted of eight males and six females with an average age of 50.4 years and an average body mass index of 34.6 kg/m2. All subjects met the Met-S criteria with regard to elevated waist circumference and hypertension. 15 Three of 14 subjects demonstrated an elevated plasma level of fasting glucose. Two subjects were using corticosteroids chronically for psoriasis (topical application) and chronic obstructive pulmonary disease (inhalation), respectively. In both subjects, no dose adjustments were made during participation. A third subject was using small amounts of topical corticosteroids for eczema during the first day of his HA treatment. None of the remaining subjects suffered from active (auto)inflammatory disease during participation. Three subjects were using non-steroidal anti-inflammatory drugs on demand for musculoskeletal pain and on our request refrained from taking these drugs during the experiments.
Characteristics of study population (n = 14).
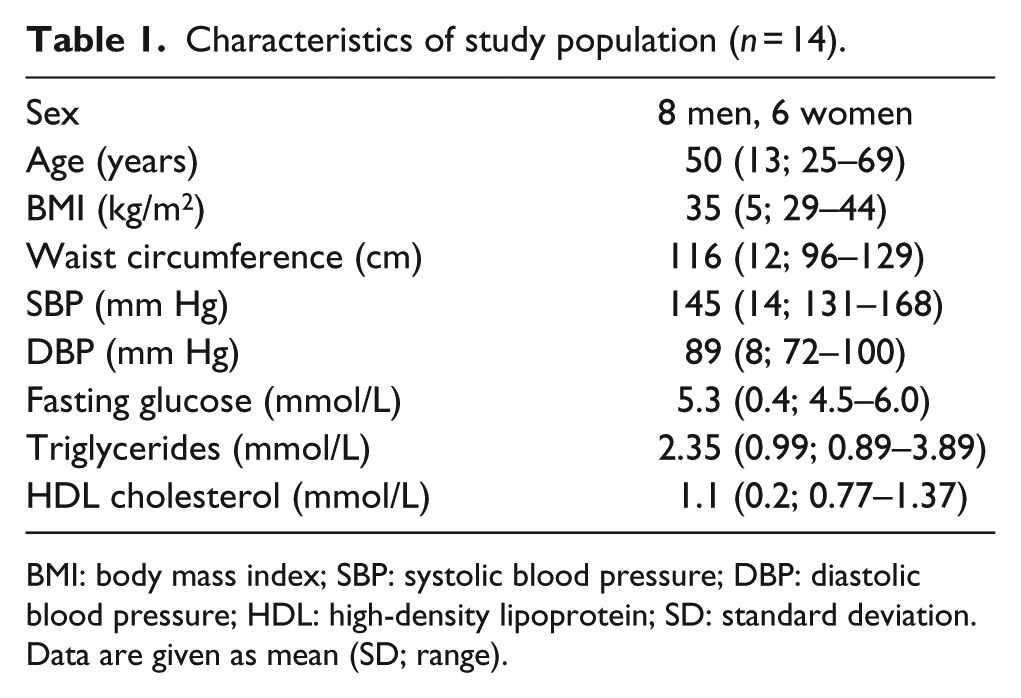
BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; HDL: high-density lipoprotein; SD: standard deviation.
Data are given as mean (SD; range).
Markers of the HO-1 system
The outcome on the different markers of HO-1 induction is shown in Table 2. Apart from baseline, these measures were determined 48 h after the first dose and 48 h after the second dose of both HA and control. The data discussed concern the data following HA treatment compared to the data following control treatment at the same time point. The plasma haem levels were elevated significantly after HA infusion compared to control. On HO-1 mRNA level, fat biopsies demonstrated a significant but modest increase (1.27 fold increase in mRNA level, p = 0.03) after HA treatment, whereas no difference on mRNA levels was observed in the peripheral blood. On HO-1 protein level, the HO-1 plasma level increased upon the first HA infusion. Upon the second infusion, no difference was found. On the level of HO-effector molecules, plasma ferritin levels increased after both HA infusions, but plasma bilirubin levels remained unaffected. Finally, HA infusion did not alter the anti-oxidant capacity of plasma as measured by the FRAP assay.
Impact of haem arginate compared to control treatment at Day 3 (48 h after the first dose) and Day 5 (48 h after the second dose) on primary endpoints and markers of HO-1 induction.
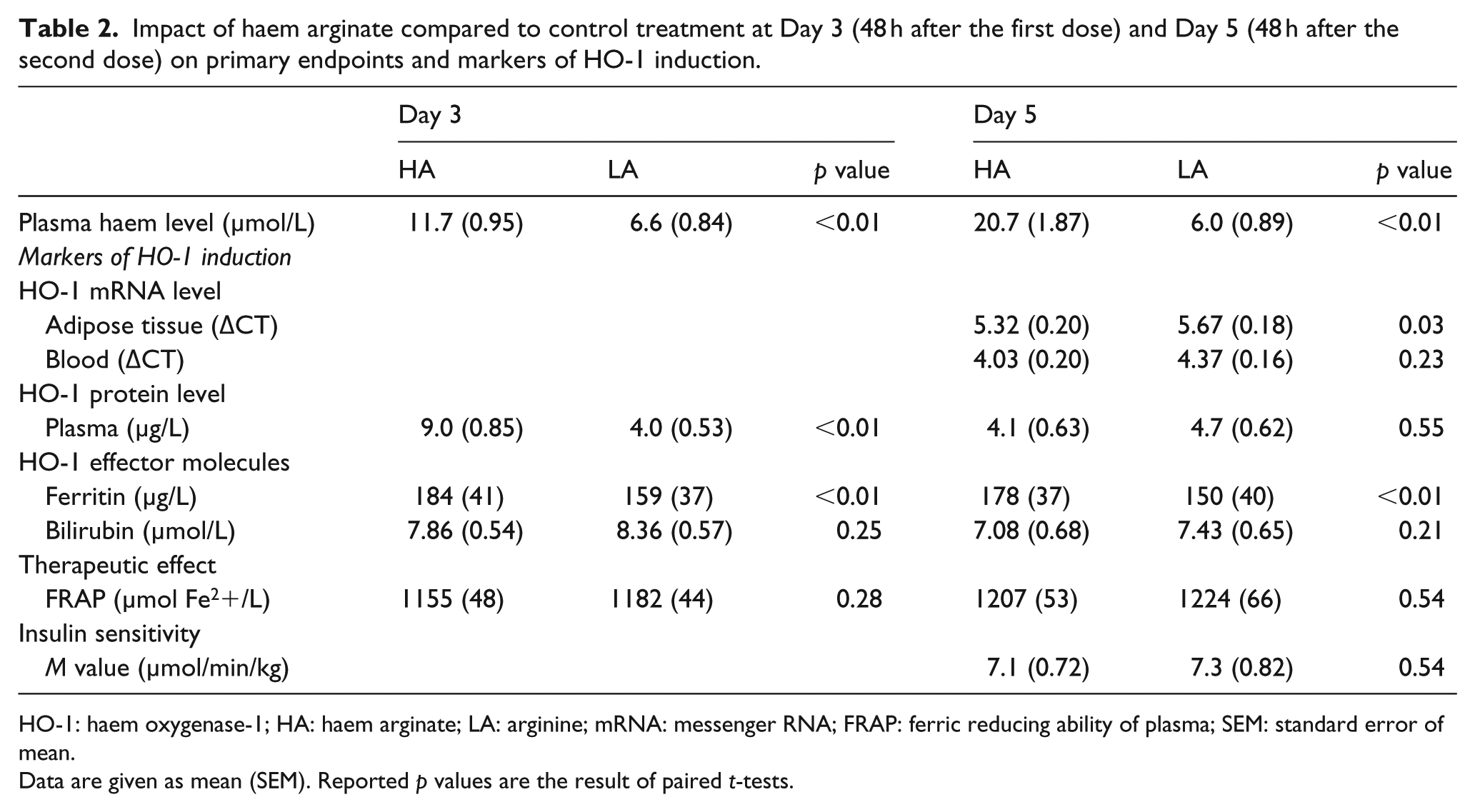
HO-1: haem oxygenase-1; HA: haem arginate; LA: arginine; mRNA: messenger RNA; FRAP: ferric reducing ability of plasma; SEM: standard error of mean.
Data are given as mean (SEM). Reported p values are the result of paired t-tests.
Adverse events
Headache was reported during HA treatment in seven cases and during control treatment in five cases. Nearly all subjects reported their headache upon the first but not the second infusion of either HA or control. Only one subject experienced headache upon both the first and second infusions of control treatment. In time, two cases of headache were closely related to the administration of HA. In one of these cases, participation was ended for the severity of the headache. The other subject continued participation and did not experience headache upon the second infusion of HA. Besides, phlebitis was noted after HA infusion in three cases and after the control infusion in a single case.
Vascular and metabolic effects
The results of the FBF experiments are depicted in Table 3. Baseline flow after control treatment was comparable to baseline flow after HA treatment (2.2 and 2.4 mL/min/dL tissue in the intervention arm and 1.8 and 2.2/mL/min/dL in the control arm, respectively). During the FBF experiments, the mean arterial blood pressure was not significantly influenced by HA treatment compared to control (103 mm Hg versus 108 mm Hg, respectively, non-significant). Intra-arterial infusion of acetylcholine induced an increase in FBF at all three doses after both control and HA treatment. The extent of this response was not affected by pretreatment with HA. On average, a non-significant increase of 11% [95% confidence interval (CI): −10% to 36%] was observed in the response to the three doses of acetylcholine. At the highest dose of acetylcholine, 8 µg/min/dL, FBF amounted to median levels of 20.3 and 23.5 mL/min/dL following control and HA, respectively.
Forearm blood flow data after logarithmic transformation.
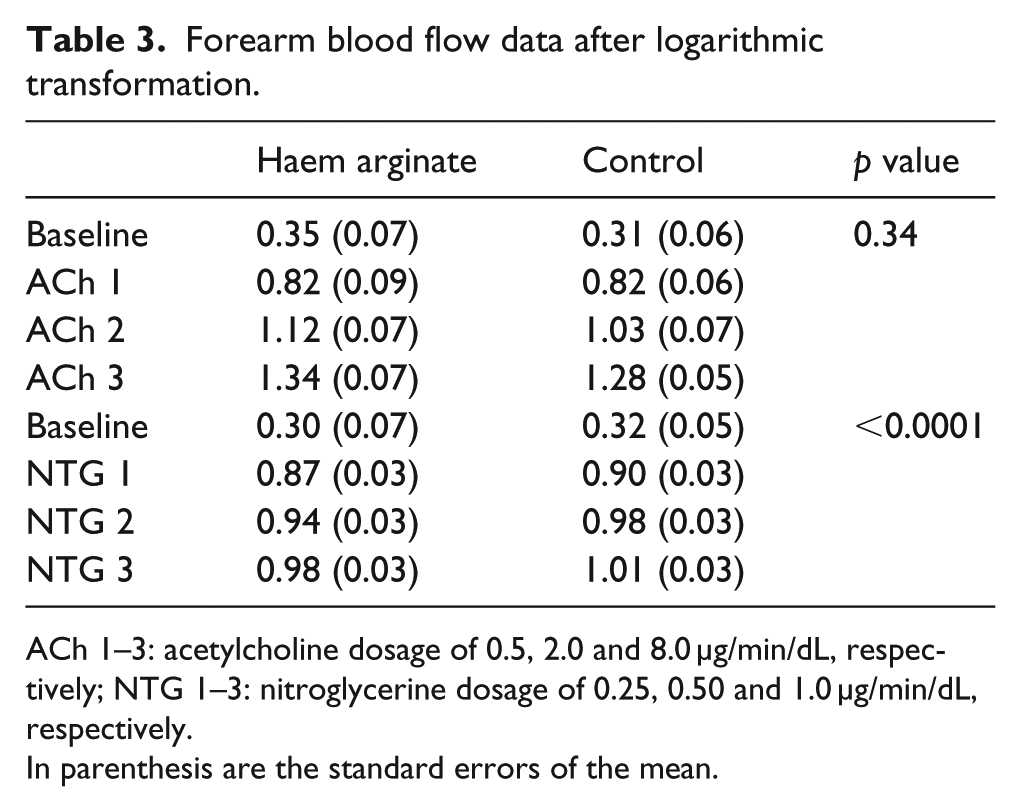
ACh 1–3: acetylcholine dosage of 0.5, 2.0 and 8.0 µg/min/dL, respectively; NTG 1–3: nitroglycerine dosage of 0.25, 0.50 and 1.0 µg/min/dL, respectively.
In parenthesis are the standard errors of the mean.
Intra-arterial infusion of nitroglycerine induced an increase of FBF at all dosages. Pretreatment with HA led to a significant diminution of the vasodilator response to nitroglycerine when compared to control. On average, a significant decrease of −7% (95% CI: −11% to −3%) was observed in response to the three doses of nitroglycerine. At the highest dose of nitroglycerine, 1.0 µg/min/dL, FBF amounted to median levels of 10.6 and 9.7 mL/min/dL following control and HA treatment, respectively.
Regarding insulin sensitivity, no difference was observed (Table 2). The average M values after treatment with HA and control mounted to 7.1 and 7.3 µmol/min/kg, respectively (non-significant). Post hoc analysis yielded similar findings for a subgroup with the highest insulin resistance (the seven subjects with the lowest M values after control treatment) and a subgroup with the most prominent HO-1 induction (the seven subjects with the highest increase in HO-1 mRNA level in the adipose tissue).
Discussion
This is the first translational study to evaluate the impact of HA administration on HO-1 induction, insulin sensitivity and endothelial function in subjects suffering from the Met-S. For years, an accumulation of preclinical data strongly suggested therapeutic benefit of HO-1 induction for both insulin resistance and endothelial dysfunction. 2
In contrast to the observed efficacy of HO-1 induction by chronic HA treatment in preclinical experiments, short-term HA treatment in human subjects suffering from the Met-S did not improve insulin sensitivity and endothelial function compared to control treatment with
HO-1 in metabolic disease
Noteworthy, the dogma of metabolic protection by HO-1 has been challenged recently. 11 Insulin-resistant obese subjects demonstrate increased HO-1 expression in liver and visceral fat compartments compared to insulin-sensitive obese subjects. In addition, hepatocyte HO-1 appears to promote insulin resistance in genetic gain- and loss-of-function models, and macrophage HO-1 knockout mice appear to be protected against metabolic disease upon a high-fat diet. Finally, cellular assays support a pro-inflammatory role for HO-1 in the development of metabolic disease. This discrepancy with previous preclinical studies on HO-1 induction is striking and urges to a re-evaluation of data and further research. One of the explanations put forward is the limited specificity of metalloprotoporphyrins used for HO-1 induction including cobalt protoporphyrin (CoPP), haem and haemin.11,19 As a result, the net positive effects of metalloprotoporphyrins reported from preclinical experiments may be related to other mechanisms than HO-1 induction per se. However, this theory seems inconsistent with the observed abrogation of protection by metalloprotoporphyrins when HO activity is co-inhibited. 8 Moreover, it does not explain the observed beneficial effects of HO-effector molecules like bilirubin in models of the Met-S and diabetes.17,20 An alternate explanation is a possible dysregulation of the HO-1 system by factors involved in the Met-S, causing a switch from the well-known anti-inflammatory profile to the recently recognized pro-inflammatory role. 21 Underlying mechanisms are to be clarified and might include a differential induction by pathological stimuli, alterations in posttranslational regulation or changes in the subcellular translocation of HO-1. 21 In conclusion, HO-1 appears to act as a double-edged sword having both protective and injurious effects in the development of the Met-S.
Study design
Our experiments are among the first studies to the therapeutic efficacy of HO-1 induction in human disease. Consequently, little is known of the optimal design of translational experiments on the supposed beneficial impact of HO-1 induction in man. As a result, we cannot exclude that either the observed low level or the duration of HO-1 induction obtained by our short-term HA treatment is insufficient in view of the lack of therapeutic efficacy.
The short-term design of our experiments originated from promising data provided by two papers demonstrating significant experimental HO-1 induction in healthy volunteers.12,13 Significant increases in HO-1 mRNA plasma level, HO-1 protein plasma level and ex vivo HO activity in leukocytes were reported 48 h after a single bolus infusion of either HA 13 or haemin. 12 The HA dosage applied in our study (3 mg/kg) equals the highest of three HA dosages applied in the first study and the single haemin dosage applied in the second study. Endothelial function and insulin sensitivity, our main outcome parameters, were assessed 48 h after the administration of HA, parallel to the reported HO-1 induction in both studies. Suggesting effectiveness of short-term HA treatment in human translational models on the therapeutic value of HO-1 induction, others have demonstrated an amelioration of ischaemia-reperfusion injury in healthy volunteers 24 h after a single dosage of HA of only 1 mg/kg. 14 For insulin sensitivity however, it should be noted that a chronic treatment with HO-1 inducers for 4–8 weeks was used in animal experiments demonstrating an improvement of glucose metabolism.7–9,22 Likewise, a long-term experiment might have been more effective in subjects suffering from the Met-S. In clinical practice, however, HA is registered for short-term use only with a maximum of 4 days for acute porphyria attacks. 23 Chronic once-weekly use has been reported in individual porphyria cases, 23 but no data are available on the extent of HO-1 induction associated with a chronic once-weekly HA treatment regimen in man. Finally, chronic weekly HA treatment is associated with serious vascular side effects involving the disappearance of the superficial venous system and the need of an indwelling venous access. 23 Although more promising based on preclinical experiments, we therefore felt that it was inappropriate to perform a long-term experiment and overleap a short-term design with less safety concerns and proven efficacy in terms of HO-1 induction.
The impact of HA treatment on markers of HO-1 induction observed in our subjects is limited. It is currently unclear, however, whether the extent of HO-1 induction observed in translational studies relates to the intended clinical effect of treatment with metalloprotoporphyrins. Besides, the selection of appropriate markers of HO-1 induction is complicated by the differential impact of HO-1 activity on various tissues. As stated, HO-1 activity in the liver and in visceral fat has been shown to aggravate instead of ameliorate the Met-S. 11 Finally, we have recently demonstrated that HO-1 induction by lipopolysaccharide in human cells differs from that in widely used experimental animal models. 24 Potential inter-species differences and cell-type-specific responses therefore necessitate caution in the adoption of markers of HO-1 induction from animal to human experiments. In search for an appropriate marker of HO-1 induction and for the central role of adipose tissue in the Met-S, 4 we included the measurement of HO-1 mRNA in subcutaneous adipose tissue. However, the relevance of this marker too is challenged by recent data demonstrating that overexpression of HO-1 in adipocytes does not protect against insulin resistance. 25
Elevated haem levels
Assessing endothelial function, we observed an unexpected reduced response to nitroglycerine 48 h after HA infusion. In theory, this reduced response might be related to changes in blood pressure. In animal experiments, lowering of blood pressure upon chronic HO-1 induction has been reported in obese mice. 7 However, we did not observe significant changes in blood pressure after short-term HA treatment compared to control. In addition, baseline blood flow was unaltered by HA treatment. In our opinion, the reduced response to nitroglycerine is more likely related to the elevated plasma levels of haem (11.7 µmol/L on average) at the time we performed forearm plethysmography. The haem levels found at this point of time, 48 h after the first administration of HA, correspond to haem levels reported by others. 13 Although long-term dosing of nitroglycerine involves complex effects, 26 short-term high dosing as used in our study is associated with the release of nitric oxide (NO). 27 Whereas HO-1 induction is expected to increase the bioavailability of NO, 28 elevated haem levels have been demonstrated to trigger the opposite by scavenging NO. 29 In fact, haem levels exceeding 6 µmol/L have been demonstrated to lower the vasodilator response to sodium nitroprusside, an NO donor, by as much as 80%. 29 In addition, excess of haem is associated with increased oxidative and inflammatory stress and endothelial activation in mouse models of haemolytic diseases.30,31 Scavenging of free haem by the administration of haemopexin markedly attenuates the observed endothelial toxicity induced by haem. 30 In contrast to our design, animal experiments on HO-1 induction in a model of endothelial dysfunction involved a pretreatment HA without exposure to haem during the subsequent in vitro assessment of endothelial function. 10 As for the vasodilator response to nitroglycerine, the elevated haem levels may have masked a beneficial impact of HA treatment on the NO-dependent vasodilator response to acetylcholine, our marker of endothelial function. Likewise, the pro-inflammatory and pro-oxidant effects of haem 31 may have counteracted a beneficial impact of HO-1 induction on insulin resistance. In our opinion, our data on nitroglycerine therefore reveal an important and general message with regard to the possible adverse effects of elevated haem levels upon the use of HA for translational studies on HO-1 induction. The pharmacokinetics of intravenously administered HA have been published in the past 32 and should be addressed specifically during the design of future experiments.
Side effects
We observed several well-known side effects of HA, including headache and phlebitis, despite the adherence to the instructions of the manufacturer. Both side effects were reported previously by others.12–14 Notably, headache was also observed during control treatment and occurred almost exclusively upon the first infusion of HA and control, prior to the assessment of FBF. Therefore, alternative causes including abstinence from caffeine must be considered. 33 Phlebitis has been associated with both haemin and HA. 23 For the use of haemin, others have been able to avoid phlebitis through the dilution in albumin instead of saline. 12 Future research should determine whether this strategy suits for HA and affects the efficacy of HA.
Limitations
Limitations of the study include the lack of a healthy control group in our protocol. As a result, we cannot substantiate the assumed presence of impaired insulin sensitivity and endothelial dysfunction in our Met-S population at baseline. Second, our study population was characterized by a certain degree of diversity in terms of gender and age. Despite the use of a cross-over design, gender- or age-related differences in therapeutic efficacy of HO-1 induction within our study population may have flattened the results. Finally, our control treatment consisted of equimolar amounts of
In conclusion, short-term HA treatment only marginally induces HO-1 expression and does not improve insulin sensitivity or endothelial function in subjects suffering from the Met-S. This is in contrast to the promising results from preclinical studies. Novel studies should unravel the various mechanisms by which HO-1 activity and metalloporphyrins affect Met-S. In addition, chronic once-weekly HA regimens should be examined for their potency to induce HO-1 and subsequently their efficacy on clinical endpoints. Finally, the design of translational experiments should be calculated on the delicate balance associated with the use of HA and strive for a dosage that is sufficiently high to achieve clinical efficacy and at the same time sufficiently low to avoid elevated haem levels by the time endpoints are assessed.
Footnotes
Acknowledgements
The authors are very grateful to Marielle Verstegen, Anja Rasing-Hoogveld and Karin Saini, whose assistance during the forearm blood flow experiments was essential. Trial registry no. NTR2472.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This work was supported by the Dutch Diabetes Research Foundation (grant no. 2006.00.055) and the Dutch Burns Foundation (grant no. 09.110).