
Abstract
Mental illnesses are frequent co-morbid conditions in chronic systemic diseases. High incidences of depression, anxiety and cognitive impairment complicate cardiovascular and metabolic disorders such as hypertension and diabetes mellitus. Lifestyle changes including regular exercise have been advocated to reduce blood pressure and improve glycaemic control. The purpose of this project was to evaluate the effect of physical training on the most prevalent corollary psychiatric problems in patients with chronic organic ailments. This longitudinal study assessed the mental health of hypertensive (age: 57 ± 8 years) and/or diabetic (age: 53 ± 8 years) patients using mini-mental state examination, Beck’s depression inventory, Beck’s anxiety inventory and self-reporting questionnaire-20 before and after a 3-month supervised resistance and aerobic exercise programme comprising structured physical activity three times a week. Clinically relevant improvement was observed in the Beck’s depression inventory and Beck’s anxiety inventory scores following the 12-week training (61%, p = 0.001, and 53%, p = 0.02, respectively). Even though statistically not significant (p = 0.398), the cognitive performance of this relatively young patient population also benefited from the programme. These results demonstrate positive effects of active lifestyle on non-psychotic mental disorders in patients with chronic systemic diseases, recommending exercise as an alternative treatment option.
Keywords
Introduction
Regular physical activity has been considered as one of the mainstream in treating systemic arterial hypertension (SAH) and diabetes mellitus (DM).1,2 Benefits such as better glycaemic and cardiorespiratory control, 3 increased insulin sensitivity, 4 improved lipid profile 5 and weight loss are well characterized. 6 Acute 7 and chronic 8 blood pressure lowering has also been linked to an active lifestyle.
In addition to physical and cardio-metabolic benefits, regular physical exercise can result in decreased depression and anxiety symptoms, 9 which may influence cognitive functions, probably by increased brain oxygenation due to a greater blood flow and perfusion, which directly influences cognition, regardless of age. 10
The prevalence of mental disorders such as anxiety and depression is greater in patients with DM compared with the general population. 11 Regular exercise plays an important role in controlling these disorders, and it can reduce levels of depression and anxiety by releasing neurotransmitters that activate specific cortical areas of the brain, acting in the mood. 12 However, it remains unclear in the literature which exercise type promotes a greater benefit to diabetics. Regarding patients with SAH, exercises can bring comparable benefits to anti-depressants, or even enhance their action, 13 as well as being an effective and practical treatment in reducing anxiety, 14 although some studies have found the results contradictory to the anxiolytic effects of exercise in animal models. 15 Thus, there is still controversy on the subject.
Hypertensive individuals are at risk of developing vascular dementia three times greater than normotensive individuals. This proportion increases to six times when the presence of SAH is associated with DM. 16 There are different models of exercise prescription. The most common ones are activities with aerobic characteristics, such as walking or running, 17 with interesting results about the effect on mental health in the diabetic population. However, the prescription of anaerobic activities is possible, such as resistance training (RT), which implies a completely different metabolic action than aerobic exercise. The results showing an association between an active lifestyle and mental disorder control are still scarce, as well as the effects of aerobic and resistance exercises in this population.
It is important to check the extent of the impact of the physical activity inclusion and compare if the exercise type prescribed in a systematic manner (aerobic or RT) has different impact amplitudes on mental health. This may guide the best way to prescribe exercises for this population. Thus, the objective of this study was to assess possible benefits of regular physical exercise on levels of anxiety, depression and cognitive impairment in diabetic and hypertensive patients belonging to a programme of supervised physical exercise, besides evaluating and comparing the results between programmes of aerobic and resistance exercises.
Material and methods
Study design
A descriptive, longitudinal type study, developed as part of the project ‘Global assessment of cardiovascular risk and mental state of patients assisted by the Viçosa Hiperdia Center after physical exercise program’, a partnership of the Federal University of Viçosa with Hiperdia Minas Program.
The study was conducted entirely at the premises of Hiperdia Center of the city of Viçosa, MG, consisting of a secondary health centre which has as a function the treatment of diabetics with glycosylated haemoglobin greater than or equal to 9% and patients with resistant hypertension. The study was approved by the Ethics in Research Committee of the Federal University of Viçosa, registered in Brazil Platform no. 33979214.3.0000.5153 protocol no. 832.149/2014.
Sample
Patient recruitment was done through analysis of medical records, where type 2 diabetic patients and resistant hypertension were selected. A phone call was made to these selected patients, where all the research procedures were clarified. If the subject agreed to participate, a first meeting in Hiperdia Center was scheduled for further information on the study procedures. The study began with a total of 21 patients, but 4 volunteers abandoned the research during the exercise routine for various reasons: financial difficulties to travel to Hiperdia, surgeries (umbilical hernia and cataract) and a cardiac ischaemia event. So the research ended with a sample of 17 patients, 8 patients with diabetes type 2 (DM2) and 9 resistant hypertensives (SAH), characterized by blood pressure that remains above the levels considered ideal, despite the concomitant use of three different classes of antihypertensive medications, one being necessarily diuretic. 18 All volunteers were participants in the supervised physical exercise programme of the Hiperdia Center in Viçosa, MG, for the registration and monitoring of resistant hypertensive and/or diabetic patients assisted by the Unified Health System (SUS) that meet Resolution SES no. 2.606 of 7 December 2010 which establishes the referral criteria for the Integrated Reference Centers Viva Vida and Hiperdia Minas.
As inclusion criteria, patients with DM2 and SAH, of both genders, over 18 years old, who do not practice routine and/or systematized exercise, were considered. The adopted exclusion criteria were as follows: type 1 diabetics, patients with peripheral artery disease, illicit drug users, congestive heart failure, decompensated pulmonary disease, symptomatic cardiac arrhythmia, orthopaedic or rheumatologic diseases that prevented the realization of the proposed exercises, symptomatic peripheral artery disease to exercise, acute cardiac ischaemia signs during exercise testing (ET) and symptomatic cardiac arrhythmia caused by ET. Also, individuals in use of anti-depressants or antianxiety medications were excluded.
At baseline, all participants were asked not to change their eating habits, not being prescribed any meal plan with calorie restriction. In addition, physicians were asked not to change the drug plan for any patient during the 12 weeks of training. All patients were informed about the methodology and the study’s objectives and they signed the Free and Informed Consent Term.
Data collection
Aiming for a possible diagnosis of cardiovascular disease, and further evaluation of symptoms consistent with arrhythmias and ischaemia induced by exercise, which are considered exclusion criteria, all patients were assessed by ET on ramp protocol, performed by a cardiologist in the centre itself, following the rules of the Brazilian Society of Cardiology guidelines 19 with the subsequent issue of medical opinion. Seeking the safety of volunteers, measurements of blood pressure were performed in all participants before the beginning of each exercise session, after 30 min of physical activity and 20 min after the end of each session. In these same periods, measurements of blood glucose in diabetic patients were conducted. Glucometer Roche Accu Chek Performa® (Mannheim, Germany, 2009) was used to measure the glucose, while for the blood pressure measurements we used the stethoscope and sphygmomanometer aneroid Premium (Wenzhou Instrument Co., China, 2014). Anthropometric procedures, used to collect data, were through body weight, using the Mercy® scale (LC 200 model, Brazil, 2010) ranging from 1 to 200 kg with 50 g of precision. Height was measured by stadiometer Welmy® (R110 model, Brazil, 2009) ranging from 0.8 to 2.00 m with 1 mm precision. Circumferences of waist, abdomen and hip were measured using retractable and flexible measuring tape Proximus® (Rio de Janeiro, Brazil, 2013) ranging from 0 to 200 cm with 1 mm precision. For measurements of skinfolds, the caliper Cescorf® Mitutoyo (Brazil) was used, with a reading amplitude of 88 mm and precision of 0.1 mm. The skinfolds were obtained using the equation suggested by Jackson and Pollock, 20 for men, and Jackson et al., 21 which used the sum of the following three skinfolds: chest, abdominal and medium femoral for men, and triceps, abdominal and medium femoral for women. For the conversion of body density (BD) in body fat percentage (BF %), the equation proposed by Siri 22 was used, using the sum of the skinfolds. The methodological procedures for the anthropometric records had the International Society for the Advancement of Kinanthropometry (ISAK) 23 recommendations as guidelines, being performed by two physical education professionals trained in this technique.
The evaluation of the mental state of the participants was performed by an experienced psychiatrist on the premises of the Hiperdia Center itself, with the following instruments: mini-mental state examination (MMSE), 24 Beck’s depression inventory (BDI), 25 Beck’s anxiety inventory (BAI) 26 and self-reporting questionnaire (SRQ-20). 27 The researcher instructed the patient to take into account the last week and the day the psychiatric evaluation was performed.
The MMSE is composed of questions that measure functions such as temporal and spatial orientation, attention and calculation, memory or recall and language. In our modified MMSE reflecting scholastic attainment, a minimum score of 20 points was considered for illiterate patients, 25 points for patients with 1–4 years of education, 26.5 points for 4–8 years, 28 points for 9–11 years and 29 points for more than 11 years.28,29
The BDI is a psychometric questionnaire of self-evaluation. The scale consists of 21 items that include attitudes and symptoms with intensity ranging from 0 to 3 and are intended to identify the presence of depressive indicators, considering various categories of symptoms, such as mood (sadness, loss of interest, crying and mood fluctuation), vegetative or somatic (weight loss, loss of appetite, sleep and fatigue), cognitive (guilt, hopelessness and suicidal thoughts), social (social withdrawal and inhibition) and motor (inhibition and agitation). 30 Participants who scored 0–9 points were considered with minimal depression, 10–16 mild, 17–29 moderate and 30–63 severe depression. 25
The BAI was used to assess the severity of anxiety symptoms using a scale of symptoms organized in 21 items, ranging from nothing, slightly, moderately and severely, expressed in anxiety symptoms, such as nervousness and tremors, and questions about palpitations, fear, feeling of suffocation and fainting, heat, numbness and others. A score between 0–7, 8–15, 16–25 and 26–63 represented minimal, mild, moderate and severe anxiety, respectively. 26
The SRQ-20 was used for tracking non-psychotic mental disorders in the evaluation of mental suffering. The instrument consists of 20 questions, and the answers are binary (yes/no). The final score was obtained by adding together the positive responses found in the test. Obtaining up to six positive responses led to no suspicion of mental disorder, and above seven positive responses mental disorder suspicion in relation to the last 30 days lived by the patient. 27
After this assessment step, the assessed patients initiated the supervised exercise routine. The exercises were prescribed individually respecting the limitations and potential of each patient identified in the initial assessments, and they followed the international guidelines proposed by the American College of Sport Medicine 31 and the American Diabetes Association (ADA) 32 for the diabetic population and the American College of Sports Medicine 33 for the hypertensive population.
Study participants underwent an intervention with physical exercise three times a week for 12 weeks. All training sessions were supervised by physical education professionals, assistants, physicians and nurses of the Hiperdia Center in Viçosa, MG. The training sessions took place in the morning period (7:00–11:00 a.m.) or afternoon (14:00–17:00 p.m.), according to the availability of study participants. In total, 36 sessions of physical exercises were held during 3 months of intervention, distributed in three sessions per week, where participants were free to choose the most appropriate days during the week to perform the routine proposed exercises. A 90% adherence to the programme was determined so that the results were valid.
Participants were randomly divided into two groups, corresponding to aerobic and resistance exercises. The group that corresponded to aerobic training (AT) consisted of nine patients (four hypertensives and five diabetics) and the RT group had eight patients (five hypertensives and three diabetics). Initially, seeking an appropriate physiological and motor adaptation, the duration of the main part of the sessions was 20 min, progressing to 30 min in the second week and to 40 min in the following week for the two intervention groups.
Training sessions for both groups started with a warm-up in a cycle ergometer for 10 min at an intensity of 50% of the maximum heart rate (MHR), estimated by the Tanaka et al. 34 equation MHR = 208 − (0.7 × age). The return to calm comprised exercises of active and passive stretching, lasting around 10 min, of the major muscle groups (quadriceps, hamstrings, large dorsal, chest, back). The average time to complete each exercise session was between 50 and 60 min after the third week.
The effort perception index (EPI) by the Borg scale 35 was used for both groups during exercise, because due to the patients’ low physical fitness and motor skills, the initial loads of each exercise were stipulated according to their effort perception, using the scale from 6 to 20 proposed by Borg 35 and, as improvements occur on the movement pattern and physical condition, the loads were adjusted. The scale values that were used were from 11 to 13, representing a moderate effort. Even with the load adjustments, the participants’ effort perception has always remained in the range from 11 to 13. We opted for the prescription and training load control in strength exercises from the perceived exertion due to low levels of physical fitness and motor coordination and to treat patients with high cardiovascular risk. Load testing or maximum repetitions would entail a non-consistent effort with health conditions of the participants, which would increase the risk of adverse events. Therefore, the training loads were adjusted to the extent that physical fitness and motor skills of the participants improved, but always taking into account the perceived exertion as moderate.
Participants of the resistance group followed a sequence of 10 exercises: neutral rowing, squats, lying dumbbell bench press, knee extension with shin pads, dumbbell shoulder press, dumbbell curls, bending knees with dumbbells, standing calf raises, cable rope overhead triceps extension and abdominal crunch. The circuit method with an interval of 15 s between exercises was used in the first 2 weeks in order to adapt the neural, joint and muscle systems, and the volunteers performed two sets of 15 repetitions. After this period, the training consisted of three sets of 12 repetitions. The loads were adjusted as improvements occurred in the motor and physical behaviours. The execution of the exercise repetitions was held continuously, controlled, with moderate speed and similar duration between the concentric and eccentric phases.
Aiming for an appropriate physiological and motor adaptation for the AT group, the duration of the main part of the sessions was initially 20 min the first week, 30 min the second week and 40 min from the subsequent week. The training was performed on a treadmill, exercise bikes, elliptical and upper body cycle ergometer. Initially, there was the intensity control proposal of training through the percentage of MHR estimated by Tanaka equation 33 with the establishment of 60% for the main part of the training. However, because some patients use adrenergic beta-blockers to control blood pressure, the scale of subjective effort perception, proposed by Borg, 35 was used for the control of training loads of these patients. For diabetic patients who did not have high blood pressure or did not use beta-blockers, the initial plan was maintained. Monitoring the heart rate (HR) was conducted through frequency meters of ergometers and controlled by the researchers responsible for the supervision of exercise sessions, controlled from the individual calculation of HR previously held. Regarding the use of EPI, the same RT group procedures were kept. After 12 weeks of inclusion in the proposed exercise programme, volunteers were reassessed using the same initial protocol.
Statistical analysis
Initially, the descriptive statistics of the sample was to obtain the means and standard deviations. The Shapiro–Wilk normality test was used. Then the paired T test and Wilcoxon test were used to compare pre- and post-training for parametric and non-parametric parameters, respectively. The χ2 and Fisher’s exact tests were used for dichotomous parameters when appropriate. The significance level was 5%. The data were analysed using SPSS statistics software. 20
Results
Table 1 presents characteristics of the sample. A higher prevalence of women (76%) was observed among the 17 patients compared to male members. Significant differences between the groups for age and education were not observed, and a high number of patients classified with obesity was noted, totalling almost half the sample (47%). The average adherence of 36 total sessions supervised proposal exercise was 95.1% and 91.9% for RT and AT groups, respectively.
Sample characterization of hypertensive and diabetic patients.
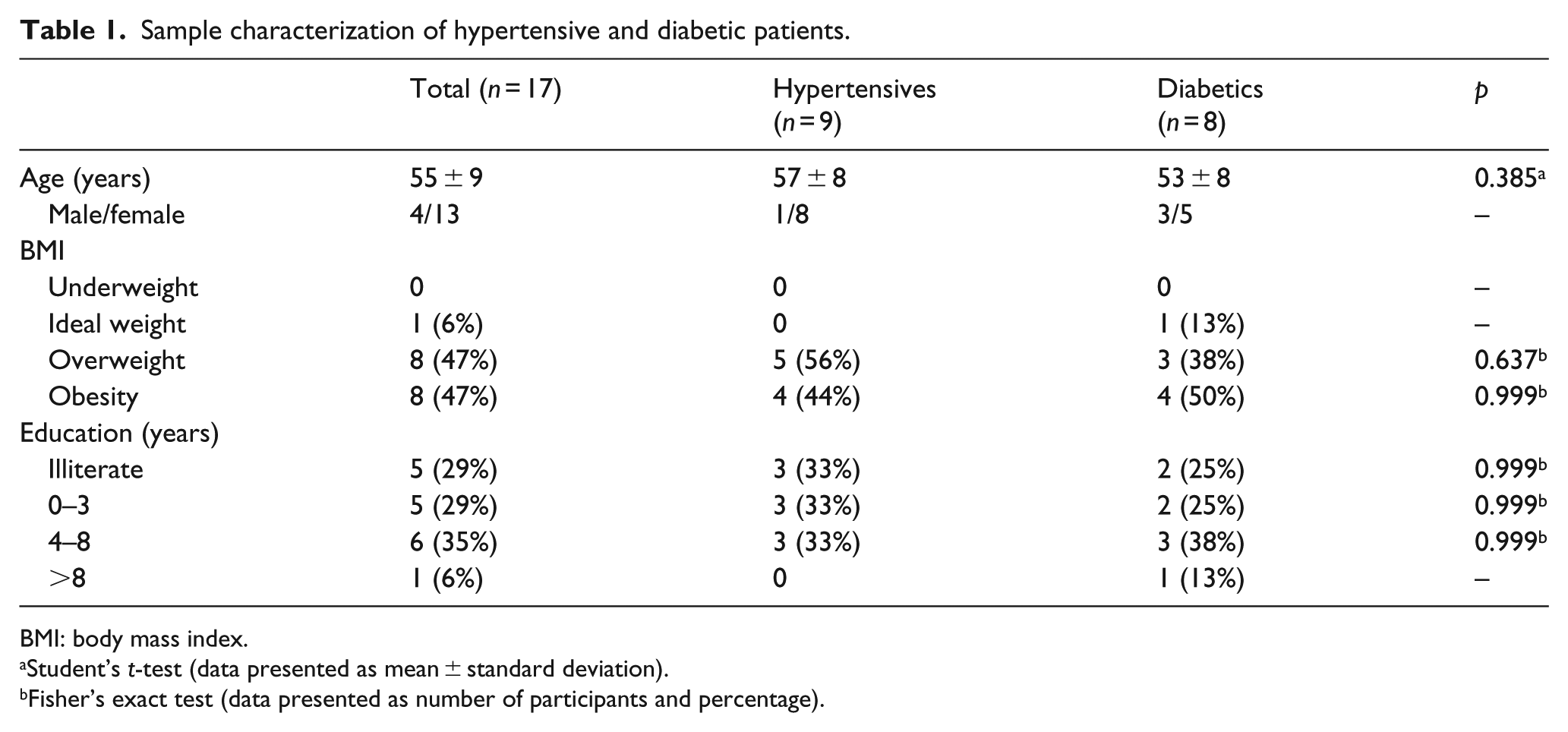
BMI: body mass index.
Student’s t-test (data presented as mean ± standard deviation).
Fisher’s exact test (data presented as number of participants and percentage).
Table 2 shows the mean and standard deviation of anthropometric parameters of diabetic and hypertensive patients, before and after intervention with exercises, and significant difference in both groups was not observed. The values considered high for abdominal circumference in patients of both diseases were observed, as well as waist–hip ratio and BF %. All study participants had waist circumference above the cutoff set by the World Health Organization (WHO), 36 which is above or equal to 94 cm for men and 80 cm for women, increasing cardiovascular risks. Regarding the waist–hip ratio, 75% of men showed values above 0.90, also established by WHO 36 as a limit value, since 54% of women had values above the cutoff value, which is 0.85. WHO 37 also states that fat percentages above 25% and 35% for men and women, respectively, indicate obesity status. Following this principle, the women in this study showed a high level of obesity, suggesting a further complicating factor in glycaemic and mental health control, as opposed to the sample of men.
Anthropometric parameters of participants before and at the end of a 12-week training.
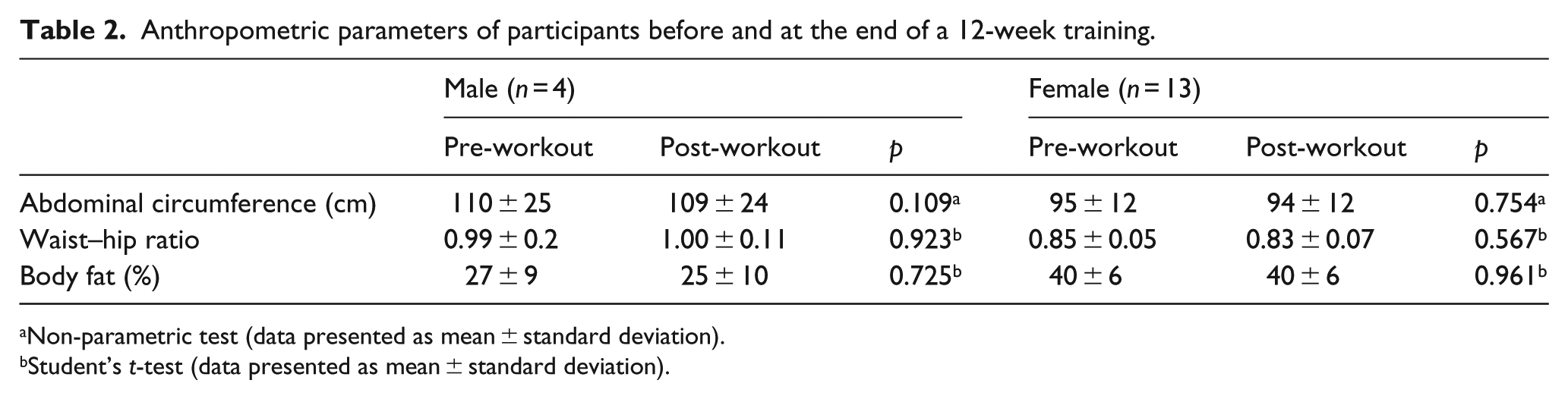
Non-parametric test (data presented as mean ± standard deviation).
Student’s t-test (data presented as mean ± standard deviation).
Adding all the volunteers’ score, the values obtained with the MMSE totalled a score of 416 points before the intervention with exercises, averaging 24 points, with an increase to 430 points after the intervention, averaging 25 points (p = 0.398), totalling an increase of 3.3%. Thus, a slight improvement among patients was noted. Regarding the diseases studied, there was a slight increase achieved by the hypertensives (2.2%), the same to the diabetics (4.3%) according to the MMSE. Two patients achieved progress in classification, moving from classification ‘with’ cognitive impairment to ‘without’ cognitive impairment, both diabetics.
With regard to depressive parameters, we observed in the pre-tests the sum of 439 points, averaging 26 among the participants, causing a drop of 61% after physical exercise, totalling 170 points and averaging 10 (p = 0.001). Both diseases decreased in scores on the BDI questionnaire after supervised training, a total decrease of 64% in hypertensive patients and 59% in diabetics.
Significant results were also observed with regard to the improvement of anxiety symptoms. The average achieved by the participants after training with exercises was 10 points in the BAI, unlike the 21 observed before the intervention (p = 0.02). There was a decrease of 53% in the average score achieved after training with exercises, and the hypertensive reached a decrease of 55% and the diabetics 52%.
People with both diseases were classified on their average with moderate anxiety before starting the exercise routine. After 12 weeks of intervention with the proposed exercises, a score corresponding to a mild anxiety level was reached, according to the BAI questionnaire. The values observed in the BDI showed that before the studied population performed the proposed intervention, there was a predominance of moderate depression among the hypertensives and severe depression among the diabetics. Minimum depression levels were observed among the hypertensives and mild levels among the diabetics in the post-tests.
Table 3 shows in detail the cognitive status of patients before and after training with exercises, as well as their levels of anxiety and depression through the mean and standard deviation obtained for each group according to the score of each questionnaire used. A few changes were observed in what concerns the cognitive state after 12 weeks of physical exercises, with no significant differences in both groups.
Parameters of cognitive state and degrees of depression and anxiety in hypertensive and diabetic groups before and at the end of 12 weeks of physical exercises.
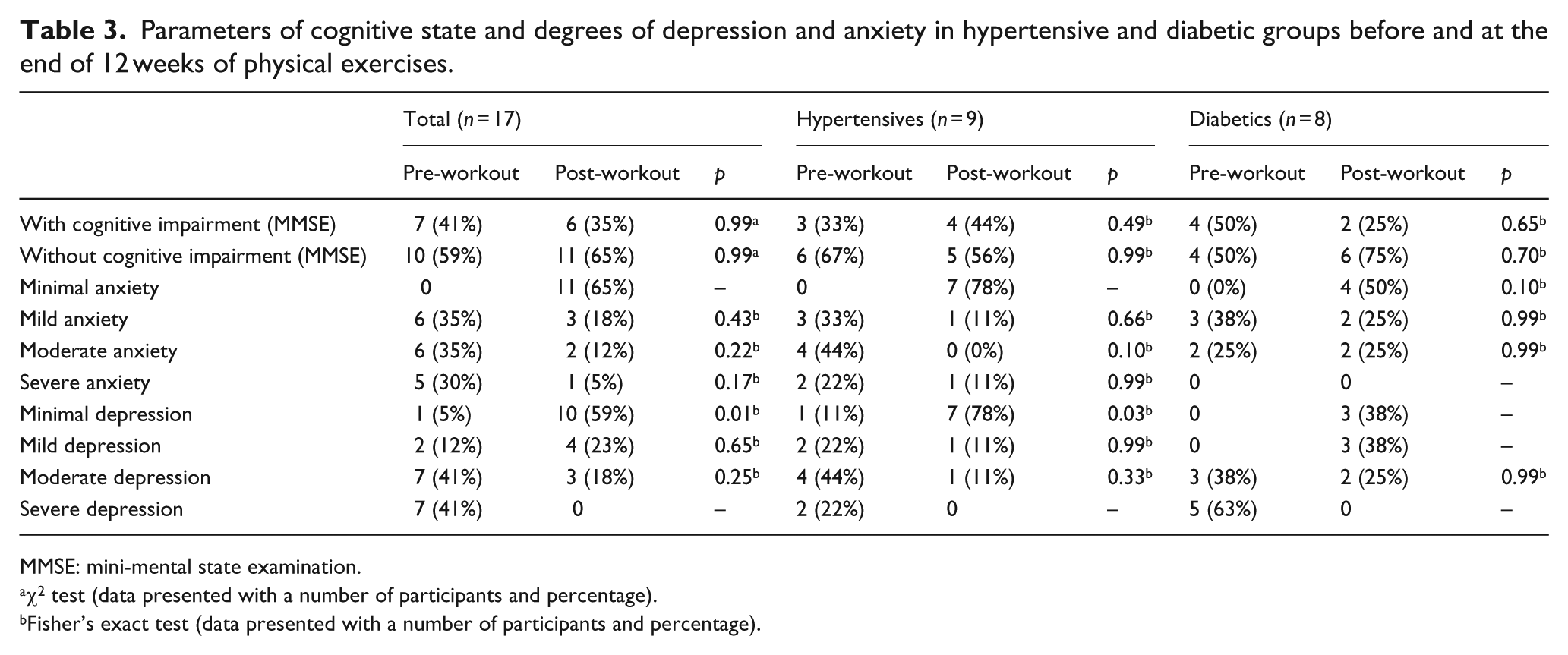
MMSE: mini-mental state examination.
χ2 test (data presented with a number of participants and percentage).
Fisher’s exact test (data presented with a number of participants and percentage).
Referring to the number of patients achieving minimal anxiety levels after the end of the 12-week intervention with exercises, an increase of 65% was observed, with a migration of patients with moderate and severe anxiety to the minimum anxiety, reaching a clinically satisfactory result. As in anxiety, a sharp decline was observed in depressive symptoms. This is because 82% of the total sample had levels of depression, from moderate to severe, in the pre-tests. After the exercise inclusion in the sample routine, this percentage was limited to 18%, with an attenuation of depression levels to minimum depression state, reaching 59% of the studied population, and these beneficial effects of physical exercise were evident in both diseases.
According to the SRQ-20 questionnaire, 88% of participants were classified ‘with suspicion of common mental disorder’ before the intervention with exercise. After intervention, this quota was reduced to 12% (p = 0.001). In the hypertensive group, seven patients (78%) were suspected of common mental disorders before the exercise programme, dropping to two patients (22%) after the intervention (p = 0.05), while six diabetics (75%) were classified as ‘no suspicion of common mental disorder’ after 12 weeks of performing the proposed exercises, an opposite scenario to what was found before the intervention, when eight patients (100%) were suspected of common mental disorder (p = 0.006).
Regardless of the exercise mode, a significant decrease was observed in the levels of anxiety and depression in hypertensives and diabetics, as it can be seen in Figure 1 through the mean and standard deviation achieved in the instruments used, revealing that both aerobic and resistance exercises were beneficial for mental health patients. Significant improvements in cognition were not found in both groups.
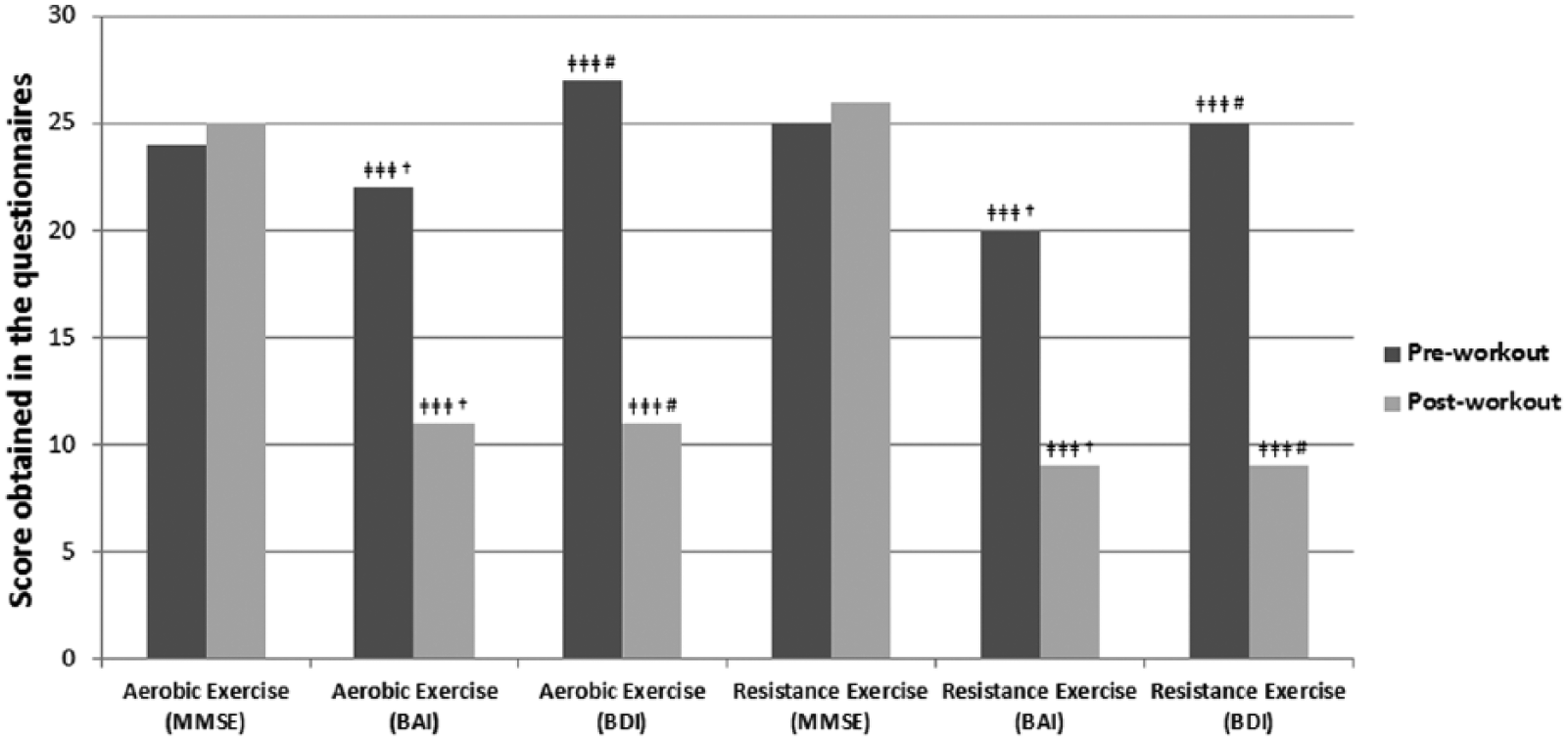
Evolution of depression, anxiety and cognitive levels of aerobic and resistance training groups before and at the end of the 12-week supervised training.
Discussion
The main findings of this study were the reduction in depression and anxiety symptoms of both hypertensive and diabetic patients after a 12-week intervention of supervised exercises. A decrease in the number of patients with probably positive screening of non-psychotic mental disorder was also noted, where anxiety and depressive symptoms are also investigated in the SRQ-20 scale. In addition, both the aerobic and resistance exercise groups had results with similar improvements. There is evidence that this study was the first to evaluate cognitive impairment, depression, anxiety and non-psychotic mental disorders in hypertensive and diabetic patients after intervention of an exercise programme consisting of aerobic or resistance activities. As there is no difference between the exercise types in improving mental disorder levels in the population studied, alternative forms of regular physical activity insertion can be used in training methodologies.
Resistant hypertensive and type 2 diabetic patients belonging to the sample studied had high body mass index (BMI) index and fat percentage as well as waist circumference and waist–hip ratio above what is recommended by the WHO 36 (Tables 1 and 2). The incidence of DM is associated with increased waist–hip ratio and peripheral lipoatrophy. Thus, abnormal distribution of adipose tissue, particularly visceral, is closely related to the incidence of DM. 38 Depression and anxiety are the most common mental disorders associated with overweight. 39 This association between depression and obesity can also be explained by the attitude of society towards obese individuals, leading some people to lose confidence and self-esteem. 40 Matini et al. 39 observed in their study that the higher the BMI, the greater the levels of psychiatric disorders in a population of 67 morbidly obese patients, with a mean age of 36 years and BMI of 48.8 kg/m2. Weight gain may also be accelerated by the use of antipsychotic medication, leading to DM, or patients with this syndrome who use this class of medication to lose control over this disease. 41 As food intake was not controlled in this study, it may explain, in part, the lack of improvement in anthropometric levels of the sample. Nevertheless, exercise has been consolidated as an extremely important instrument in combating obesity, along with oriented nutritional education. Resistance exercise of low to moderate intensity showed no benefits on the anthropometric parameters, yet was effective on mental disorders. Thus, it can be used in these individuals, as they are easy for people who find it difficult to join in more intense activities. 42
SAH may favour anxiety and depression states in their patients, as noted in the study of Mushtaq and Najam, 43 which detected a combination of these psychiatric symptoms in 137 hypertensive patients, 77 men and 60 women with a mean age of 43 years, compared to a control group. As noted in this study, exercise can have a positive effect on depression (Table 3). Data corroborate the findings of Zarshenas et al., 44 where 41 women with a mean age of 26 years showed a significant reduction in the levels of depression after intervention of 4 weeks of aerobic exercise compared to the control group matched for age, education and marital status. The duration of the exercises was 30–35 min in the main part of the sessions, with a 60%–80% of MHR. It is noteworthy that considerable uncertainty about the optimal workout duration and frequency to obtain satisfactory results still occurs. 45
In addition to depression, there are evidences that suggest positive effects of physical exercise also on anxiety parameters, corroborating the findings of this study (Table 3). Aidar et al. 46 concluded that after a 12-week intervention of RT with 48 h of rest between sessions and durations of 45–60 min in 13 individuals with a mean age of 52 years affected by stroke, large reductions in anxiety levels occurred compared to the control group of a similar age.
In diabetic patients, the depression symptoms are strongly associated with the disease, but little is known about anxiety. 47 In this study, both psychiatric disorders showed high prevalence in diabetics before supervised exercise intervention. After the set period of intervention, clinically favourable results were observed in this study (Table 3). Broadly in line with our findings, Gallagher et al. 48 observed that depressive symptoms were halved in patients with diabetes and cardiovascular disease who made life-style changes including both exercise and healthier diet. In a cross-sectional study, Saleh et al. 49 observed in 500 patients with DM type 2, aged more than 25 years, that 80% of patients who performed less than 45 min of exercise per week, in other words, who did not adhere to a regular exercise routine, had depressive and anxiety symptoms. The regular exercise programme can increase self-esteem, mood, well-being feeling and positive effects on body image, reducing the physiological effects of stress. 50
Data observed using the MMSE showed no beneficial effects on cognitive aspects evaluated by this questionnaire (Table 4). The MMSE was chosen by its high validity, reliability and easy application. Despite its recommendation for the elderly, it has been increasingly used in adults. 51 Research has shown that cognitive function can be benefited by physical exercise. Furthermore, studies have been proving that physically active people have a delay in cognitive decline, 52 as noted in the study of Dupuy et al., 10 when 22 women with a mean age of 24 years and 36 women with a mean age of 62 years were submitted to a maximal progressive test and performed the Stroop cognitive test in the meantime. The results showed that the higher the cardiorespiratory fitness of these women, the higher their performance on cognitive tests. The lack of improvement in cognitive status may be partly due to the characteristics of the prescribed activities, which are repetitive. It is possible that activities such dance and mini games require more from the cognitive process, resulting in greater benefits.
Mental state of hypertensive and diabetic patients before and at the end of the 12-week supervised training.
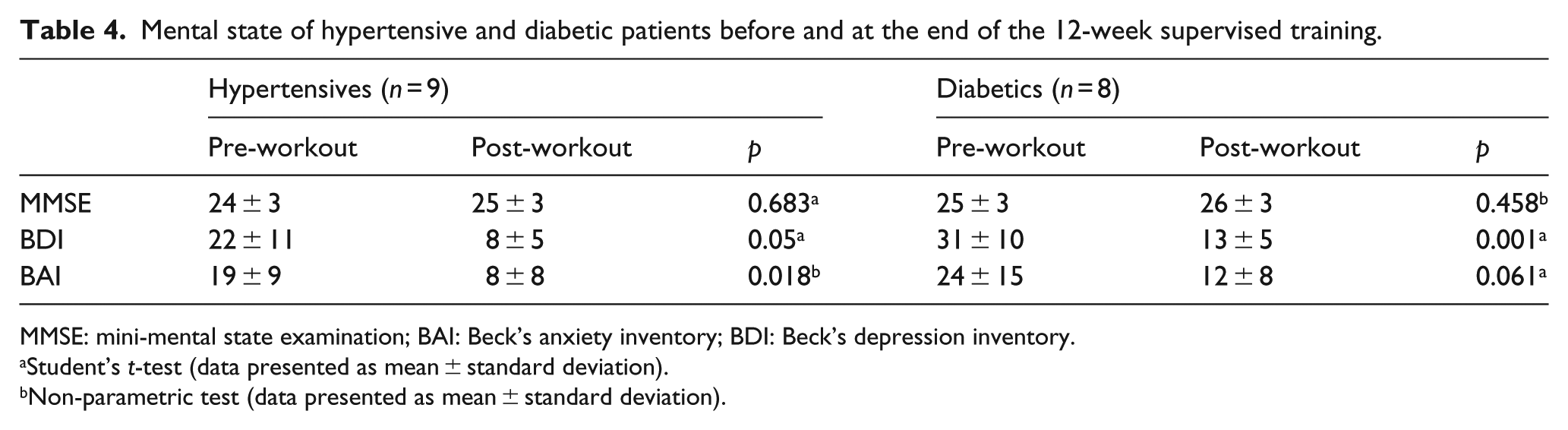
MMSE: mini-mental state examination; BAI: Beck’s anxiety inventory; BDI: Beck’s depression inventory.
Student’s t-test (data presented as mean ± standard deviation).
Non-parametric test (data presented as mean ± standard deviation).
Regarding the SRQ-20 questionnaire, this instrument was used for its wide tracking capability of common mental disorders symptoms, such as depressive–anxious mood, somatic symptoms, vital energy decrease and depressive thoughts, being necessary to emphasize that this instrument seeks a screening of non-psychotic psychiatric disorders, such as anxiety, depression and other mental disorders, and is widely used to diagnose suspicion of common mental disorders. Before the intervention with exercise, mental health levels tracked by the three instruments were worrying, and these mental disorders were alleviated after the intervention period, with both resistance and aerobic exercises. Thus, the improvements observed by the SRQ-20 corroborate the findings on BDI and BAI questionnaires (Table 4).
Study limitations
Only screening instruments were used in this study, which do not replace the medical interview for an accurate diagnosis. In addition, one of the inclusion criteria in the study was the condition of participation in the physical exercise programme at the Hiperdia Center. This led to a limited sample size, since not all the diabetic and hypertensive patients assisted at the Center can perform the training, but only those that are recommended by the physician after a rigorous evaluation. The non-inclusion of a control group may also be considered as a limitation of the study. This was the great difficulty encountered in recruiting patients for participation in the study.
Conclusion
This study showed positive interference of exercise on the mental health of patients with hypertension and diabetes type 2. Significant improvements on depression and anxiety status in both disorders were found after 12 weeks of supervised exercise intervention as well as great improvements in states of possible suspicion of non-psychotic mental disorder. On the other hand, improvements on cognitive status of hypertensive and diabetic patients after the intervention with physical exercise were not found. Benefits to mental health were found in the groups who performed aerobic and resistance exercises, leading us to believe that regardless of the performed mode, exercise is beneficial to the mental health of hypertensives and diabetics and clearly shows the importance of supervised physical exercise in the full health treatment of hypertensives and diabetics, which can benefit in the treatment adherence and maintenance of a good underlying disease control, even in a short training period of 12 weeks of activities.
Footnotes
Acknowledgements
J.C.B.M. is a productivity grant beneficiary of the National Council for Scientific and Technological Development (CNPq). R.B.T. is a Master’s Grant Program beneficiary of the Higher Education Personnel Improvement Coordination. T.A.S.M. is a fellow of scientific research of the Support Foundation for Research of Minas Gerais (FAPEMIG). This article is part of the Master’s dissertation of Robson Bonoto Teixeira by the Federal University of Viçosa (UFV).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
This study was supported by the Support Foundation for Research of Minas Gerais – FAPEMIG.