
Abstract
Little is known about the epidemiology of metabolic syndrome in urban areas of China. To estimate the prevalence of MetS and identify its cardiovascular-related factors in men and women, a representative sample of 15,477 urban adults aged 18–74 years in Northeast China was selected from 2009 to 2010. The diagnosis of metabolic syndrome was based on criteria set by the National Cholesterol Education Program/Adult Treatment Panel. The overall prevalence of metabolic syndrome was 27.4% (men 27.9% and women 26.8%). Multivariable logistic regression analysis revealed that a higher education level and a higher family income were associated with a higher prevalence of metabolic syndrome in men, but associated with lower prevalence of metabolic syndrome among women. Higher physical activity was associated with a decreased prevalence of metabolic syndrome in men (adjusted odds ratios (aORs) = 0.88, 95% confidence interval (CI): 0.79–0.99), but associated with an increased prevalence of metabolic syndrome in women (aOR = 1.14, 95% CI: 1.00–1.29). Compared with rice as the major staple food, cooked wheaten foods were associated with lower adjusted odds for metabolic syndrome both in men (aOR = 0.72, 95% CI: 0.58–0.90) and in women (aOR = 0.72, 95% CI: 0.56–0.92). In conclusion, metabolic syndrome is highly prevalent in urban areas of China, and there is heterogeneity by sex in the relationships between risk factors and metabolic syndrome prevalence.
Introduction
Metabolic syndrome (MetS) is a clustering of several metabolic factors, including obesity, high levels of triglycerides, low levels of high-density lipoprotein cholesterol, elevated serum levels of fasting glucose and hypertension. Substantial data indicate that MetS increases the risk for atherosclerotic cardiovascular disease (ASCVD)1–3 and diabetes mellitus,4–6 which are major contributors to morbidity and mortality all over the world, including China. 7 It was observed that individuals with MetS had a higher probability (odds ratio (OR) = 2.13) of developing occlusive vascular diseases, coronary disease, diabetes and stroke,8,9 and therefore, studying the cause of the MetS may provide clues for prevention and treatment for some occlusive vascular diseases. Although the underlying cause of the MetS is still unclear, both genetic and environmental factors may be associated with the etiopathogenesis of the MetS,10,11 with the latter playing a predominant role in the development of MetS, such as factors related to rapid nutritional transition, rural-to-urban migration, and adoption of a sedentary lifestyle. 12
With rapid economic development and urbanization over the past two decades, the lifestyle and diet in China have changed substantially, which in turn has increased the prevalence of cardiovascular diseases (CVD). 7 Several studies have reported a high prevalence of individual components of MetS such as obesity and hypertension in adults across urban areas of China;13,14 however, the epidemiology of MetS in that population has not been fully explored. In addition, racial and ethnic differences are known to influence the prevalence and risk of MetS, and more recent definitions of MetS have tended to be ethnic-specific. 15 In this study, we assessed the prevalence of MetS and associated risk profiles in a sample of urban Chinese adults selected according to the criteria set by the National Cholesterol Education Program/Adult Treatment Panel (NCEP/ATP III) modified by the American Heart Association/National Heart, Lung and Blood Institute (AHA/NHLBI) in September 2005. 15
Methods
Sample design
The subjects were selected from the sample used in the Control Hypertension and Other Risk Factors to Prevent Stroke with Nutrition Education in Urban Area of Northeast China (CHPSNE) study, which was randomly selected from 14 cities with over 20 million residents from Liaoning province in Northeast China. These 14 cities were stratified into three socio-economic zones: low, medium and high. In April 2009, three cities (Shenyang, Anshan and Jinzhou) were randomly selected from these three zones. The number of urban districts in Shenyang, Anshan and Jinzhou were 5, 3 and 3, respectively. From each of the selected 3 cities, 3 communities were randomly selected from each urban district in the city, yielding a total of 33 communities in the study sample. From each selected community, 500 households were randomly selected, and from each household, only 1 participant (≥5 years of residency) was randomly selected without replacement. The sampling procedure of the CHPSNE study is shown in Figure 1. This study was approved by the ethics committee of China Medical University and all subjects provided written informed consent. Subjects were excluded from the survey if they were unwilling to complete all required questions.
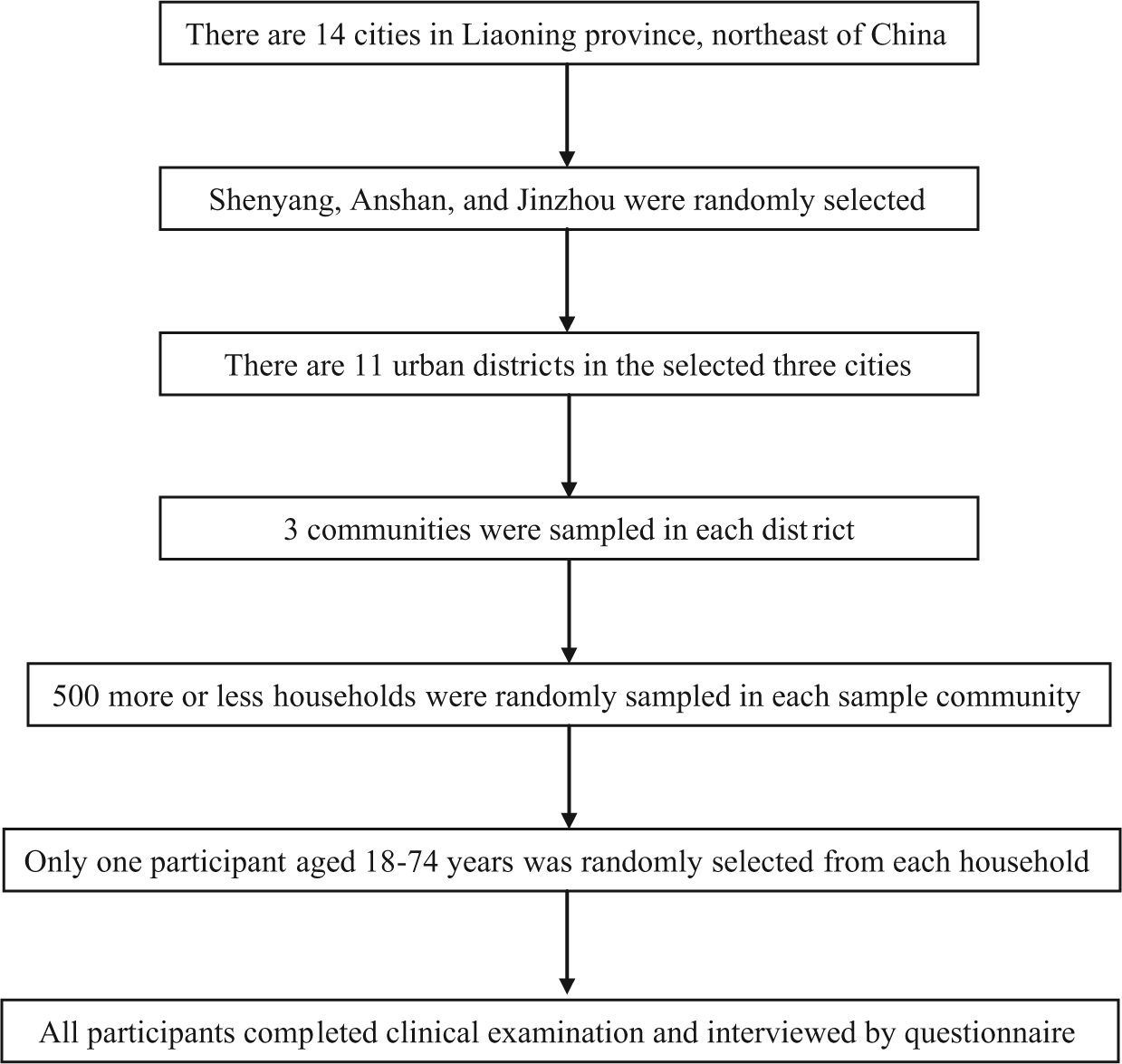
Sampling procedure of the CHPSNE study (Control Hypertension and Other Risk Factors to Prevent Stroke with Nutrition Education in Urban Area of Northeast China).
A total of 17,954 subjects were randomly selected from 33 communities and were invited to participate. A total of 15,477 persons (8156 men and 7321 women) completed the survey and examination. The overall response rate was 86.2%. The age of the subjects was 18–74 years, with an average age of 44.9 ± 13.5 years.
Anthropometric measurements
The anthropometric measurements of height, weight and waist circumference (WC) were measured using a standardized protocol. 16 Height was measured, to the nearest 0.5 cm, without shoes, with the participant’s back square against the wall tape, eyes looking straight ahead with a right-angle triangle resting on the scalp and against the wall. Weight was measured with a lever balance to the nearest 100 g, without shoes, in light undergarments. WC was defined as the midpoint between the lower rib and upper margin of the iliac crest, measured to the nearest 0.5 cm by a nurse using a tape with an insertion buckle at one end. Body mass index (BMI) was calculated as weight (in kilograms) divided by height (in metres) squared (kg/m2).
Blood pressure measurement
Three blood pressure (BP) measurements were obtained from each participant by trained and certified observers according to a common protocol adapted from procedures recommended by the American Heart Association. 17 BP was measured three times with the participant in the sitting position after 5 min of rest, and the time interval between three measurements of BP was 2 min. In addition, participants were advised to avoid alcohol, cigarette smoking, coffee/tea and exercise for at least 30 min before their BP was measured. A standardized mercuric-column sphygmomanometer was used, and one of four cuff sizes (paediatric, regular adult, large or thigh) was chosen based on the circumference of the participant’s arm.
Laboratory analysis
A venous blood sample was collected from each participant after a 12-h fast to assess serum levels of total cholesterol (TC), triglycerides (TG), high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C) and fasting blood glucose (FBG). All biochemical analyses were performed in the institutional laboratory that met the standards of the National Reference laboratory. TG, HDL and serum glucose were assayed using enzymatic methods, dextran-magnesium precipitation and hexokinase/glucose-6-phosphate dehydrogenase, respectively. 18
Diagnostic criteria for MetS
According to the NCEP/ATP III definition, modified subsequently by the AHA/NHLBI to use region/ethnicity-specific WC thresholds and reduce the fasting glucose threshold, the diagnosis of MetS was made when three or more of the following risk factors were present: a WC > 90 cm in men and >80 cm in women, fasting glucose ≥100 mg/dL, systolic BP ≥130 mmHg or diastolic BP ≥85 mmHg, fasting TG ≥150 mg/dL and HDL-C < 40 mg/dL in men and <50 mg/dL in women. 15
Information on demographics (i.e. age, sex and residential area), socio-economic status (i.e. education level achieved, occupation and annual household income) and other information was collected using a standardized questionnaire that has been used for other studies in China. 13 For example, we calculated the age of subjects by using their birthday, got the information of education level by using the question ‘Which is your highest academic degree (1, no school; 2, primary school; 3, junior high school; 4, senior high school; 5, college or higher)’, selected the information of family income per year by the question ‘How much do your family earn last year?’. Cooked wheaten foods were defined as foods made from wheat such as wheat bread, biscuit, steamed bread, noodles and others. Organization cadre was defined as the governmental and institutional employees who usually have a relatively higher education level and more regular work schedule than the general population.
Statistical methods
Continuous variables are presented as the mean ± standard deviation (SD) and categorical variables as the percentage in each subgroup. Comparisons of continuous variables between groups were performed by analysis of t-test. The chi-square test was used to test for the difference in groups for a categorical variable. Multivariable logistic regression was used to calculate the adjusted odds ratios (aORs) with 95% confidence intervals (95% CIs) for MetS adjusted for the following covariables: age, race or ethnicity, education level, occupation, household income, family hypertension history, smoking status, drinking status, physical activity, diet status, and study district (defined as a dummy variable), which were preliminarily found to be significant from univariable logistic regression analysis. These covariables were selected from a set of recommended variables in the literature. All data analyses were conducted using SAS software Version 9.1 (SAS Institute Inc., Cary, NC). All statistical tests were 2-tailed, and significance was declared when the p value <0.05.
Results
Of the 15,477 subjects, 4237 had MetS. The overall prevalence of MetS was 27.4%, with 27.9% in men and 26.8% in women (χ2 = 2.21, p = 0.14). However, in analysis stratified by age, among the subjects aged <55 years, the prevalence of MetS was higher in men than in women; however, among the subjects aged 55–64 years and 65–74 years, the reverse was true (Figure 2). There was also a drop in the prevalence in the oldest age group (65–74 years), especially for men.
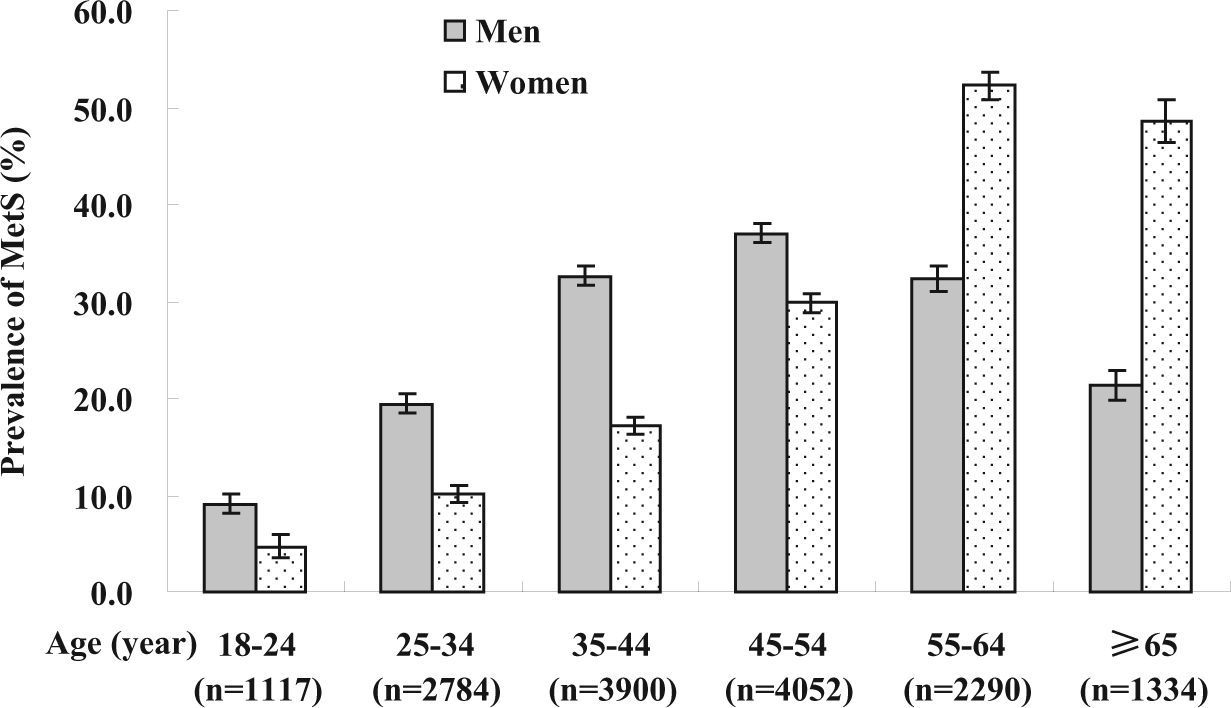
Prevalence of MetS by sex according to age group.
Table 1 shows the prevalence of the individual risk factors included in MetS, overall and stratified by sex. The characteristics of the participants in this study stratified by sex are shown in Table 2. A significant difference was found between the two sex groups in education level, occupation, family income, family history of hypertension, smoking, drinking, diet control and like drinking sugary drinks (all p < 0.05). Heterogeneity of associations with MetS by sex, as evidenced by significant interaction p-values, was noted with age, race/ethnicity, education level, family income, family history of hypertension, alcohol consumption, physical activity, low-calorie, low-fat diet, and drinking sugar-sweetened beverages (all p < 0.01); no interaction by sex was evident with occupation, cigarette smoking, and type of the staple food (all p > 0.05).
Prevalence (%) of individual atherosclerosis-related risk factors of MetS in the general population based on the NCEP/ATP III modified by the AHA/NHLBI criteria by sex in an urban population in Northeast China.
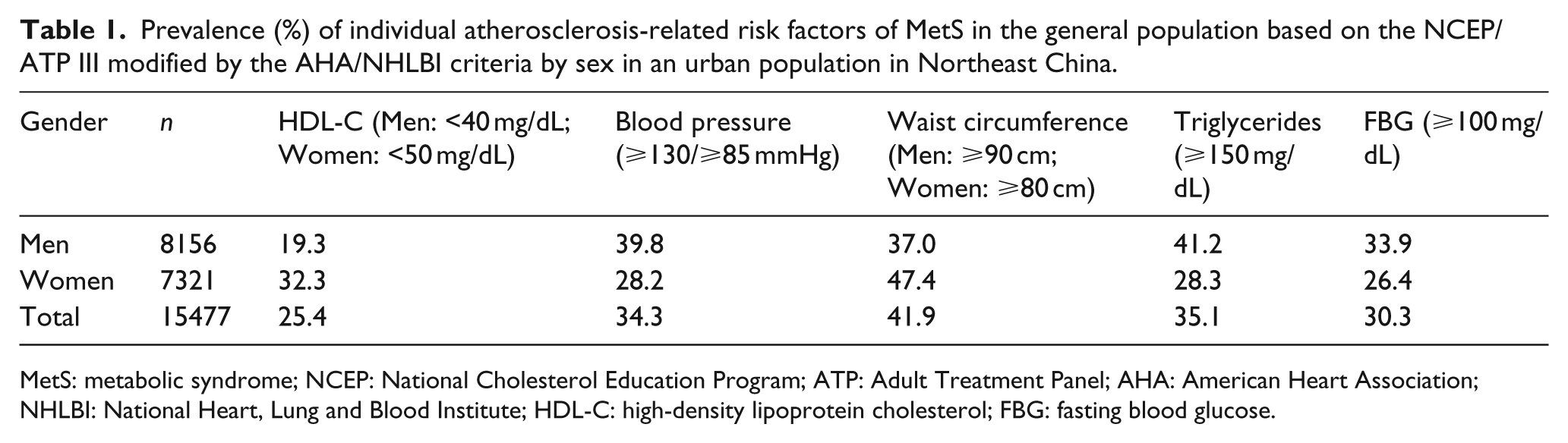
MetS: metabolic syndrome; NCEP: National Cholesterol Education Program; ATP: Adult Treatment Panel; AHA: American Heart Association; NHLBI: National Heart, Lung and Blood Institute; HDL-C: high-density lipoprotein cholesterol; FBG: fasting blood glucose.
Distributions of demographics and lifestyle factors by gender.
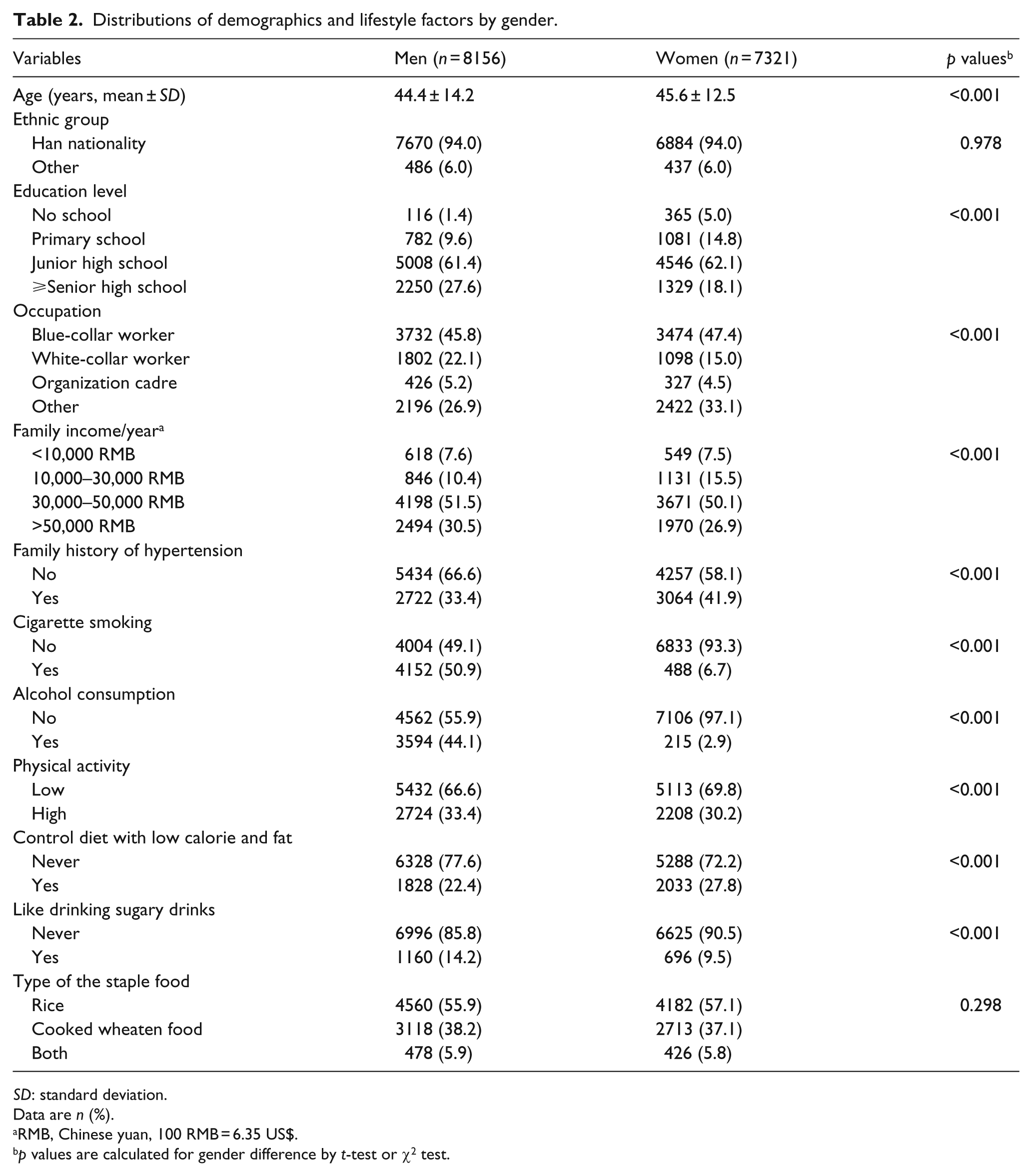
SD: standard deviation.
Data are n (%).
RMB, Chinese yuan, 100 RMB = 6.35 US$.
p values are calculated for gender difference by t-test or χ2 test.
When analyses were stratified by sex, risk factors associated with MetS were different among men (Table 3) and women (Table 4). Among men, the adjusted OR (aOR) for the prevalence of MetS was first increased with increased age but then decreased, and the subjects with a higher education level and a higher family income were associated with a higher risk of developing MetS (Table 3). However, among women, the prevalence of MetS consistently increased with age, and after adjusting for all other factors, a higher level of education and a higher family income were associated with a lower MetS prevalence (Table 4). Among men, increased physical activity was associated with a decreased MetS prevalence (aOR = 0.88, 95% CI: 0.79–0.99), but an increased prevalence of MetS among women (aOR = 1.14, 95% CI: 1.00–1.29). White-collar men appeared to have a higher risk for developing MetS than blue-collar men, but white-collar women and women who had worked in an organization cadre have a lower risk of developing MetS. In addition, MetS was associated with smoking, drinking and drinking sugar-sweetened beverages in men but not in women.
Factors associated with the prevalence of MetS from multivariable logistic regression models in men (N = 8156).
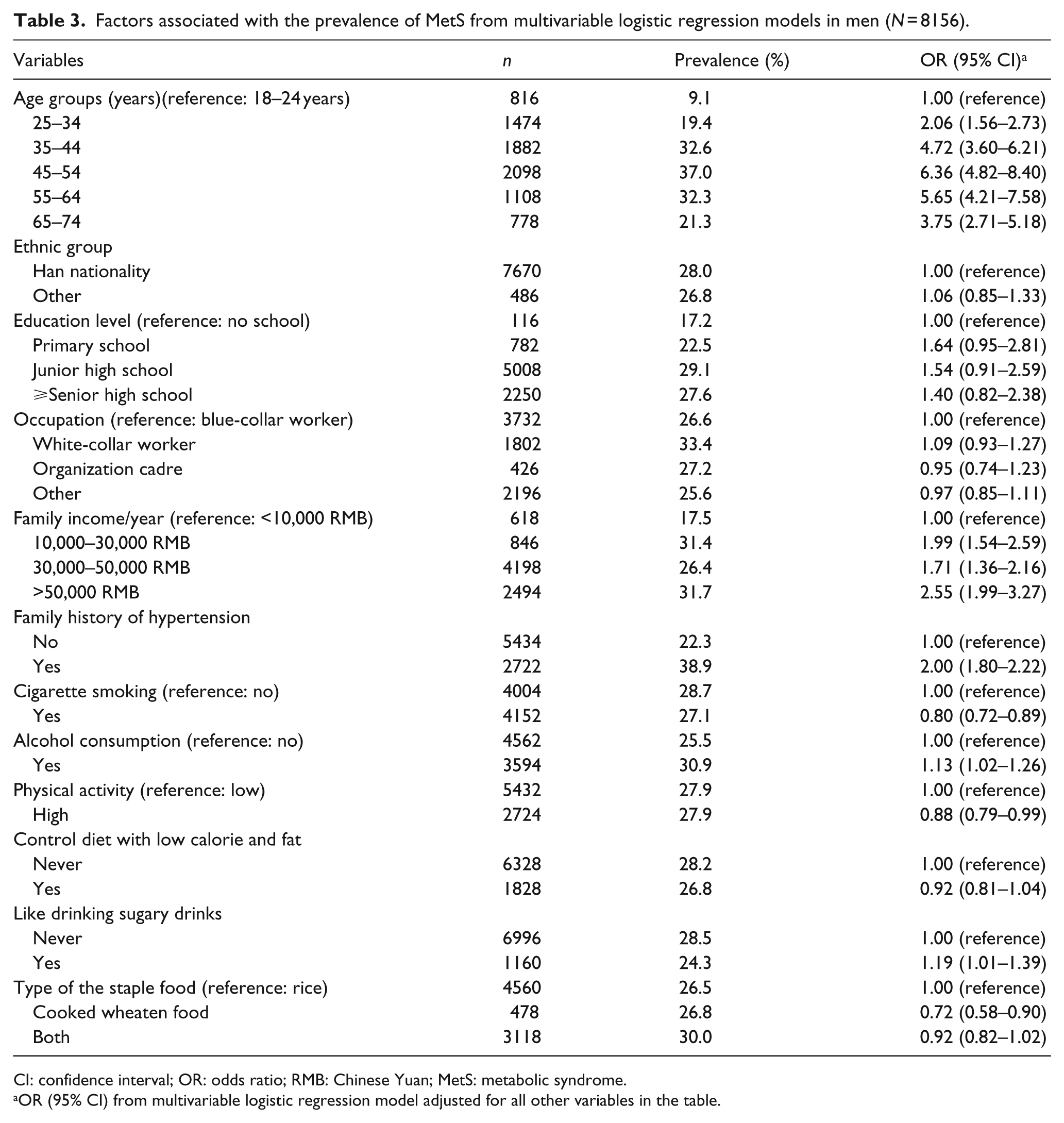
CI: confidence interval; OR: odds ratio; RMB: Chinese Yuan; MetS: metabolic syndrome.
OR (95% CI) from multivariable logistic regression model adjusted for all other variables in the table.
Factors associated with the prevalence of MetS from multivariable logistic regression models in women (N = 7321).
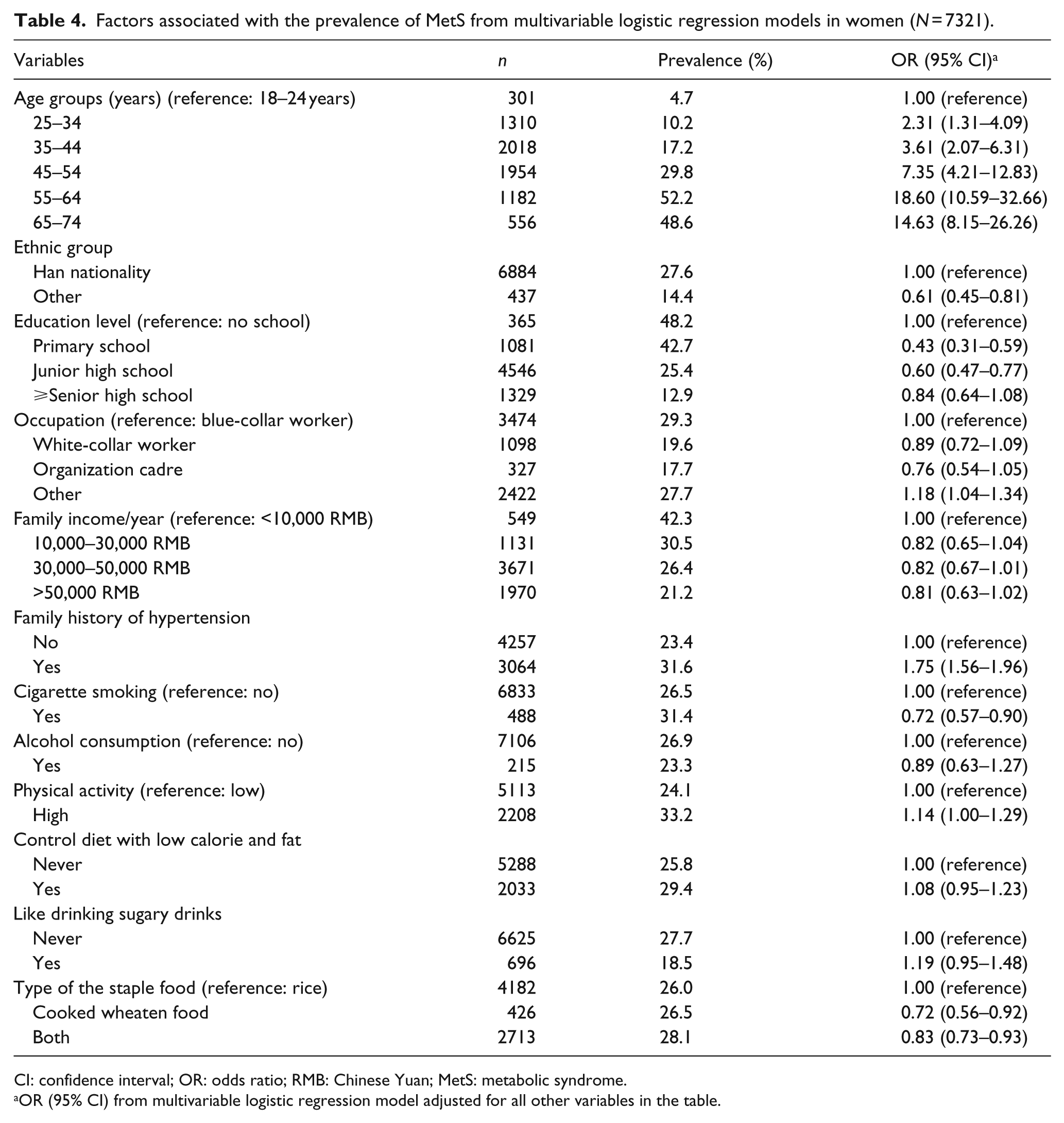
CI: confidence interval; OR: odds ratio; RMB: Chinese Yuan; MetS: metabolic syndrome.
OR (95% CI) from multivariable logistic regression model adjusted for all other variables in the table.
Discussion
The results of this study provide up-to-date information on the current prevalence of MetS, and the individual risk factors defining the condition, among the urban adult population in Northeast China. This study was conducted on a large representative sample of the adults in urban areas of China using standard protocols and instruments. Strict training processes for data collectors and vigorous quality assurance programmes were used to ensure the quality of the data collection. Additional strengths of the study include the high response rate, the use of three BP measurements, and detailed information on the history of hypertension, history of diabetes, and pharmaceutical treatment. For all these reasons, these data likely constitute the most accurate and precise estimates of the prevalence of MetS, as well as data on the risk factors defining the condition, that are available for the general urban Chinese population living in Northeast China.
Overall, the results of this study reported a MetS prevalence of 27.4% in urban adults aged 18–74 years in Northeast China, which is higher than many developing and developed countries. For example, the prevalence of MetS in the Philippines among adults aged ≥20 years was estimated to be 18.6% (17.5% in men and 19.7% in women) in 2003. 19 A recent study conducted in 23 provinces of Iran showed that the prevalence of MetS was only 2.5% in Iranian adolescents. 20 Using International Diabetes Foundation (IDF) criteria, Hajat and Shather 21 reported that MetS was present in 29.0% of Middle East population. In the United States, the National Health and Nutrition Examination Survey (NHANES) 1999–2000 reported that the prevalence of MetS in adults aged ≥20 years was 31.9% (30.6% in men and 33.2% in women). 22
The prevalence of MetS reported in the present study was higher than that reported in other studies conducted in China. For example, a community-based study on 653 subjects in Hong Kong with a mean age of 55.1 years (SD = 10.4 years) reported that the overall prevalence of MetS was estimated to be 28.8% (30.8% in men and 27.0% in women). 23 The Dongfeng-Tongji Cohort (DFTJ cohort) study, conducted in Wuhan, China in 2008, reported that the overall prevalence of MetS in urban adults aged ≥50 years was 33.2% (27.4% in men and 37.8% in women). 24 Recently, a large-scale population-based cross-sectional study conducted in Zhejiang Province, China, in 2010 reported that the prevalence of MetS among 8169 men aged 19–97 years was 15.2%. 25 A recent community-based study conducted in 2012 in 1724 adults aged 18–75 years in Southern China reported that the prevalence of MetS was 22.2%. 26 Compared with the results of the above studies, the findings in the present study indicate that MetS has become a major public health problem in urban areas of Northeast China, and call for an urgent need for the prevention and treatment of MetS in these areas. MetS is considered a risk factor as important as smoking for the development of occlusive vascular diseases and atherosclerotic diseases. 8 Therefore, the diagnosis and treatment of MetS are extremely important for occlusive vascular diseases and atherosclerotic diseases because its prevalence is increasing worldwide.
Previous studies reported that the prevalence of MetS was found to be higher in women than in men.19,22,24,27 Our study showed that the prevalence of MetS in men (27.9%) was not statistically different than in women (26.8%), which was consistent with the finding of the MetS prevalence in the two sexes from a study in Indians (17.6% in men vs 16.8% in women). 28 However, the analysis stratified by age showed that the prevalence of MetS in men aged <55 years was higher than in women in the same age group, but the reverse was true for those aged ≥55 years. Other studies also have similarly shown a higher prevalence of MetS among women than men and an increase in the strength of this sex-related correlation with increased age. 19
The possible mechanism underlying the sex difference in prevalence of MetS is still uncertain. Some potential explanations have been proposed. First, evidence has shown associations between MetS and selected environmentally hazardous materials, with difference noted in the associations by sex. For example, previous studies reported that serum perfluoroalky chemicals (PFCs), a class of human-made organic chemicals, were associated with glucose homeostasis and indicators of MetS, 29 and several studies have reported the sex-specific toxicity after exposed to PFCs.30,31 Experimental studies showed that the biological half-life of PFCs in male rats is 70 times longer than in female rats, and the difference is mainly attributed to a difference in renal clearance [CL(R)]. 32 These studies reported that sex hormones may play an important role in the sex difference of PFCs CL(R). For example, castration of male rats resulted in a 14-fold increase in the CL(R) of PFCs, which is comparable to that in female rats. However, testosterone treatment reduced the elevated PFCs CL(R) in castrated males. Second, hormonal factors, postmenopausal weight gain and a different risk profile might account for the difference in prevalence of MetS between women and men. For example, we have noticed a large percentage of male smokers (50.9%) in this study, but only 6.7% of females reported smoking. In Asia, especially in China, according to conventional rules of etiquette, smoking in women is subject to harsh social stigmatization. So, compared with Western developed countries, the proportion of current women smokers in cities of China is lower. In developed countries, especially in the English-speaking countries, almost 25% of women are smokers. Results from the European Community Respiratory Health Survey (ECRHS) showed that the proportion of maternal smoking was over 40% in Denmark, Iceland and the English-speaking countries, even the proportion of maternal smoking in pregnancy reached 27% in Ireland. 33 Differences in the proportion of smoking by sex could partly explain the different prevalence of MetS observed in these Chinese populations. Especially concerning is the increase in the number of younger and female smokers in recent years. Therefore, we should correctly recognize the association between cigarette smoking and health consequences, and emphasize the education for health, which will be useful to the prevention of MetS diseases in humans.
The association between smoking and MetS was found negative for men and women from this study, especially for women. As shown in Table 4, in women, the prevalence of MetS was significantly higher in smokers than in non-smokers (31.4% vs 26.5%; χ2 = 5.49, p = 0.019); however, when adjusted for age and other covariables, the aOR for MetS was 0.72 (95% CI: 0.57–0.90) for female smokers. A possible explanation is that the smoking effect may be modified by age in light of the fact that female smokers were older than non-smokers (53.4 ± 11.6 vs 45.0 ± 12.4 years). It is well known that the prevalence of MetS increases with age. For example, when the models were adjusted only for other variables but not including age, smoking remained as a risk factor for MetS (aOR = 1.24, 95% CI: 1.01–1.52) among women. A similar pattern was also observed with sugar-sweetened drink consumption. When adjusted for age and other variables, the aOR for MetS was 1.19 for women with higher sugar-sweetened drink consumption, whereas the prevalence of MetS was only 18.5% in the group with high consumption of sugar-sweetened drinks versus 27.7% in never category. This may also be the age effect, because the average age of women in the group with highest consumption (37.1 ± 10.6 years) was lower than that of never consumers (46.5 ± 12.4 years). When the age variable was deleted from the models, the aORs changed to 0.72 (95% CI: 0.59–0.89). Also, this same phenomenon has been found in the association between smoking and CVD reported in other studies.34,35 For example, one of our previous studies has reported that the prevalence of hypertension was 31.0% in female smokers versus 24.2% in non-smokers, whereas the OR for hypertension was lower than 1 for female smokers when adjusted for age. 34 Despite the observation that smoking was associated with lower risk of MetS in the present study, it may still be associated with future greater risk of adverse clinical events.
Gender, as opposed to sex, is a social construct and includes cultural norms, roles, and behaviours shaped by relations among women and men. 36 Gender, inherently social, varies continuously over multiple dimensions over the life course. Gender describes patterns of behaviour, place, and role, determining where people spend time and their activities, thereby shaping exposure distributions. Our multivariable logistic regression analysis revealed a difference in the association of risk factors with MetS prevalence between men and women. As shown in Tables 3 and 4, as educational level increases, the prevalence of MetS significantly increased among men but decreased among women. A similar pattern was also observed with family income. White-collar men had a higher prevalence of MetS than blue-collar men (aOR = 1.09), whereas white-collar women had a lower prevalence of MetS than blue-collar women (aOR = 0.89). A possible explanation is that white-collar workers usually have a relatively higher level of education and a much higher income than the blue-collar workers. Therefore, on the basis of these results, it may be possible that men with higher education and incomes may suffer from other potential MetS-aggravating factors such as they may spend more time sitting in front of their computers and, accordingly, may not get enough exercise and/or may suffer from mental health problems due to work-related stress and anxiety. As the reasons for MetS and high education, high-income and white-collar career associations in men are still unclear, future studies are needed to give more explicit explanations.
Our results showed little or even reverse association between increasing physical exercise and low-calorie diet with the risk of MetS among women. However, this finding should be interpreted with care, because there might be large bias in the definition and classification of physical exercise and low-calorie diet. For example, patients with chronic diseases may pay more attention to avoid exposure to risk factors and seek some behaviour intervention such as physical exercise and low-calorie diet. Also, physical exercise and low-calorie diet may be the responses (‘effect’) to development of MetS rather than the cause among Chinese women. The reasons for these associations are unclear, and need to be explored further.
Our study has several limitations. First, the study used a cross-sectional design, which cannot infer causal relationships between MetS and socio-demographic lifestyle characteristics. Second, because exposure information was primarily obtained through a questionnaire, recall bias, where the respondent might be affected not just by the correct answer but by the respondent’s memory, cannot be ruled out. Third, due to the nature of the survey questions (yes or no), misclassification on behavioural risk factors (occupation, family income, smoking, drinking and exercising) was possible. Finally, as noted by previous studies, a significant association has been found between MetS and confounding factors such as marriage age, reproductive history (higher parity and earlier age at menarche), menopause, family structure, and mental and emotional stress; 37 however, these confounding factors are not available in the present study. Furthermore, the lack of clinical outcomes (CVD events) is also an important limitation in this study.
In conclusion, this study showed a high prevalence of MetS and multiple risk factors associated with MetS. Therefore, both the general public and health professionals need to be better informed about the new guidelines. In addition, due to the gender-based variability by state and society, designing effective localized health interventions requires clarity about these distinct sources of difference (sex), with an aim of improving population health. Furthermore, careful consideration of sex effects and exploration of nascent methods for quantitative analyses stratified by sex may help to elucidate sources of difference.
Footnotes
Acknowledgements
We are very grateful for the participants from Northeast China. We would also like to thank the anonymous reviewers for their very helpful comments.
Declaration of conflicting interests
The authors report no conflicts of interest. The authors are alone responsible for the content and writing of the paper.
Funding
This research was supported by grants from the Liaoning Province Education Department Foundation (L2010672), and the Liaoning Province Science and Technology Foundation (2013225049).