
Abstract
Purpose:
To determine the effects of laparoscopic adjustable gastric banding (LAGB) on albuminuria in patients with obesity, type 2 diabetes mellitus (T2DM) and established diabetic nephropathy.
Methods:
A retrospective analysis of clinical records from a tertiary diabetes service identified obese patients with T2DM who had micro- or macroalbuminuria prior to LAGB surgery. Clinical data from follow-up appointments including albuminuria were analysed.
Results:
A total of 23 T2DM patients were included in the final study. Of 7 patients with macroalbuminuria at baseline, 2 reverted to normoalbuminuria, 2 reverted to microalbuminuria and 3 remained with macroalbuminuria on their final recording in the 36-month period of follow-up. Of 16 patients with microalbuminuria, 9 reverted to normoalbuminuria, while 6 remained with microalbuminuria.
Conclusion:
This study demonstrates significant improvements in albuminuria in patients with established diabetic nephropathy following LAGB. These results suggest the potential for LAGB to improve or reverse renal damage in patients with T2DM.
Keywords
Introduction
Obesity is associated with an increased mean arterial pressure, glomerular filtration rate (GFR) and albumin excretion rate, and therefore, a generally increased workload for the kidneys.1–3 This association exists regardless of whether a patient is suffering from co-morbidities such as diabetes mellitus.
There is a higher prevalence of obesity among patients with type 2 diabetes mellitus (T2DM) than in the general population, and the prevalence of T2DM increases with weight. 4 Indeed, excess body weight is the most significant modifiable risk factor that contributes to the development of T2DM, with approximately 80% of diabetes cases being preventable via the avoidance of an overweight or obese status. 5
Diabetic nephropathy is a leading cause of end-stage renal disease (ESRD) worldwide, and about one-third of patients with T2DM have micro- or macroalbuminuria. 6 Furthermore, micro- and macroalbuminuria are associated with morbidity and mortality in patients with T2DM, 7 with both micro- and macroalbuminuria associated with an increased renal and cardiovascular risk. 8 As albuminuria level rises, so does the degree of functional disability experienced by diabetic patients, independent of chronic co-morbidities (heart disease, chronic lung disease, stroke and arthritis), systolic blood pressure (SBP), glycaemic control, renal function, total cholesterol and chronic inflammation. 9
Bariatric surgery is an important treatment option for reducing weight among severely obese patients, due to its proven effects on long-term weight management in comparison to non-surgical treatment methods. 10 It has also been shown to significantly improve outcomes in those with chronic renal impairment, with the potential to assist patients who have developed ESRD to progress to a state that improves their candidacy for transplantation. 11
All forms of bariatric surgery have been shown to, at differing degrees, be associated with the remission of diabetes, with glycaemia returning to below the diabetic range without the aid of pharmacological agents or additional surgical therapy.12–18 The effects of bariatric surgery on renal function are not well defined. Two studies have shown that gastric bypass may lead to improvement in albuminuria levels,3,19 and two other studies have shown improvements with biliopancreatic diversion (BPD).12,20
In Australia, the majority of bariatric surgery is laparoscopic gastric banding (LAGB). To our knowledge, the literature is yet to provide an indication as to the benefits of LAGB for diabetic patients with micro- or macroalbuminuria. The aim of our study was therefore to determine whether T2DM patients undergoing LAGB with established diabetic nephropathy had an improvement in their albuminuria levels.
Methods
We conducted a retrospective study through a search of the electronic health records of the clinics at the Baker IDI Heart and Diabetes Institute for patients with T2DM who had undergone gastric banding surgery. Results of laboratory investigations and clinical examinations from our patient records, over the period from 2002 to 2012, were analysed. These included albumin–creatinine ratio (ACR) and HbA1c levels, weight, body mass index (BMI), SBP and diastolic blood pressure (DBP). Other information recorded included gender, age, date of LAGB and whether the patient was on an angiotensin converting enzyme-inhibitor (ACEI), an angiotensin receptor blocker (ARB) or any other antihypertensive medication.
Patients were included in the study if they had T2DM, had undergone LAGB and had raised ACR prior to surgery. A minimum of one follow-up ACR was a requirement for inclusion. The most recent data within the 18 months prior to surgery were used as a baseline for each of the outlined patient characteristics. The last result within each 12-month period over the following 36 months was then recorded as the follow-up data. The final data for the entire 36-month period were also recorded, as not all patients had a result recorded in every 12-month period.
Determination of normo-, micro- and macroalbuminuria was based on spot urine ACR measurements. Normoalbuminuria was defined as an ACR less than 2.5 mg/mmol for men, and less than 3.5 mg/mmol for women; microalbuminuria was defined as an ACR between 2.5 and 25 mg/mmol for men, and 3.5 and 35 mg/mmol for women and macroalbuminuria was defined as an ACR greater than 25 mg/mmol for men, and greater than 35 mg/mmol for women.
Patient ACR levels were measured using a DCA 2000® + Analyzer. This device used an immunoturbidimetric agglutination complex for the determination of albumin (range of 5–300 mg/L), and Benedict/Behre chemistry for the determination of creatinine (range of 1.3–44.2 mmol/L), in order to calculate an ACR level of the patient’s urine sample.
HbA1c levels were measured by an Afinion™ AS100 Analyzer, which used a boronate affinity assay. BMI was calculated as weight (kg)/height (m2). Blood pressure (BP) was measured in a sitting position using a standard sphygmomanometer of appropriate cuff size.
Patients were categorized as improved or not improved, according to their micro- or macroalbuminuria classification at their final recording within the 36-month period. Patients who improved included those who went from macroalbuminuria to normoalbuminuria or to microalbuminuria, or microalbuminuria to normoalbuminuria. Patients who did not improve included those who remained with macroalbuminuria, remained with microalbuminuria or went from microalbuminuria to macroalbuminuria.
The results are presented as mean ± standard deviation (SD), median (25th–75th percentile) or as n (%). Statistical significance was determined using the Mann–Whitney U test, Wilcoxon Signed-Rank test, McNemar test or Fisher Exact test. The level of significance was set at p < 0.05. Microsoft Excel was used for all calculations.
Results
There were 139 diabetes mellitus patients who had attended the Baker IDI Diabetes Clinic and underwent bariatric surgery. Of these patients, 50 had normoalbuminuria prior to surgery and were excluded. Other exclusions were 8 who did not have T2DM; 7 who had LAGB prior to diagnosis with T2DM, 31 who did not have the date of their surgery recorded, 16 who did not have their ACR measured within the 18 months prior to surgery, 2 who underwent alternative bariatric surgery shortly following LAGB, 1 who did not have any further ACR recordings following surgery and 1 who had pre-existing glomerulonephritis. In this report, 23 T2DM patients were included, and all of these patients underwent LAGB between November 2004 and January 2011, with a mean follow-up period of 30 months.
There were 12 men (52%) and 11 women (48%) included in our study (Table 1), and at baseline prior to LAGB, 16 had microalbuminuria and 7 macroalbuminuria. As many of the urine albumin concentrations for the patients in the macroalbuminuria group were above the upper limit of the measurable range (>300 mg/L), it was not possible to calculate the median ACR for these patients. The median ACR for the patients with microalbuminuria was 7.88 mg/mmol (quartiles: 5.61–12.30).
Baseline characteristics of patients.
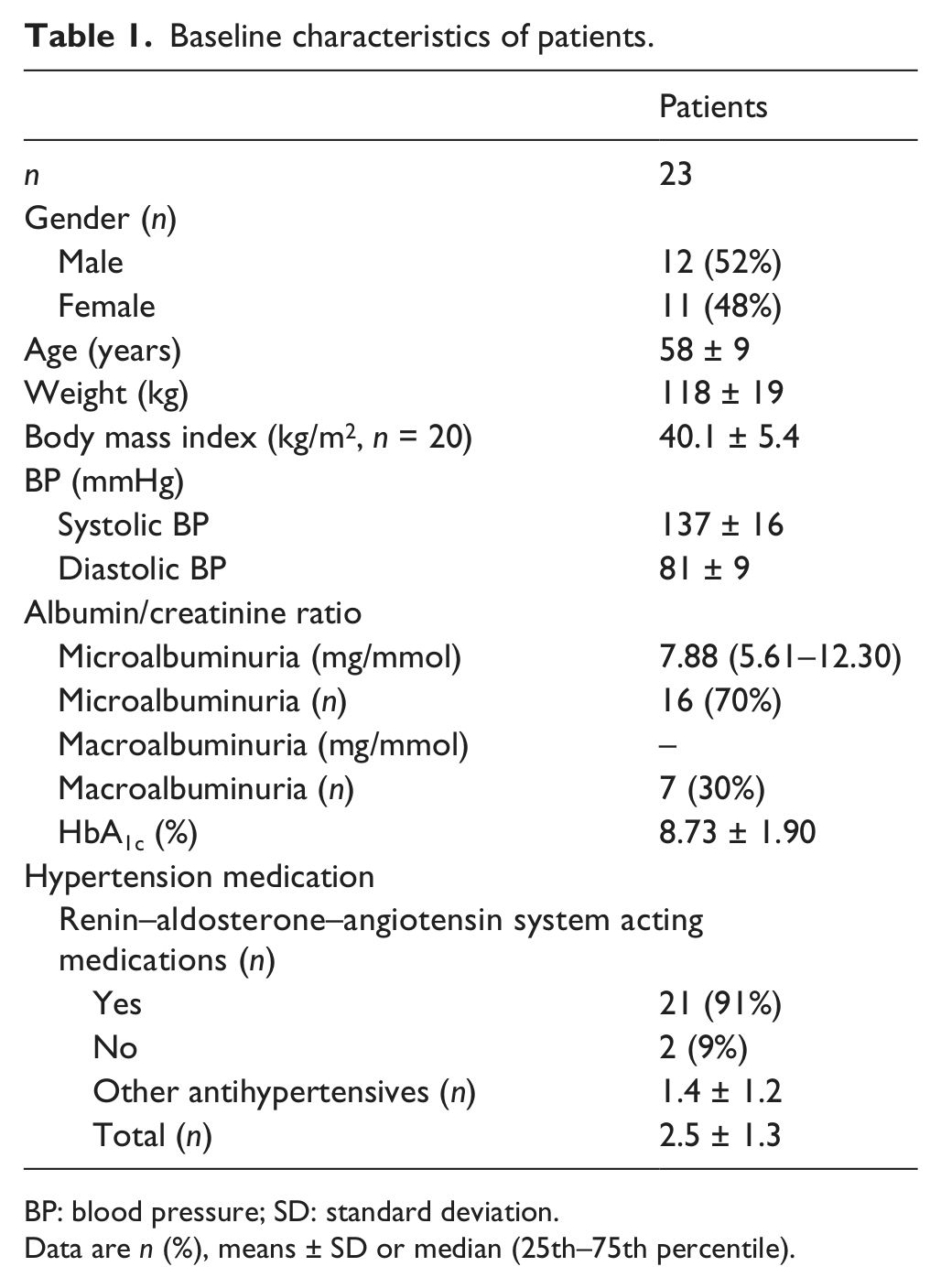
BP: blood pressure; SD: standard deviation.
Data are n (%), means ± SD or median (25th–75th percentile).
The characteristics of patients prior to surgery, as well as their final recording within the 36-month period, are shown in Table 2. The most notable changes include the improvement in weight, BMI, microalbuminuria level, HbA1c and DBP. There was no improvement in SBP.
Results pre- and post-LAGB surgery.
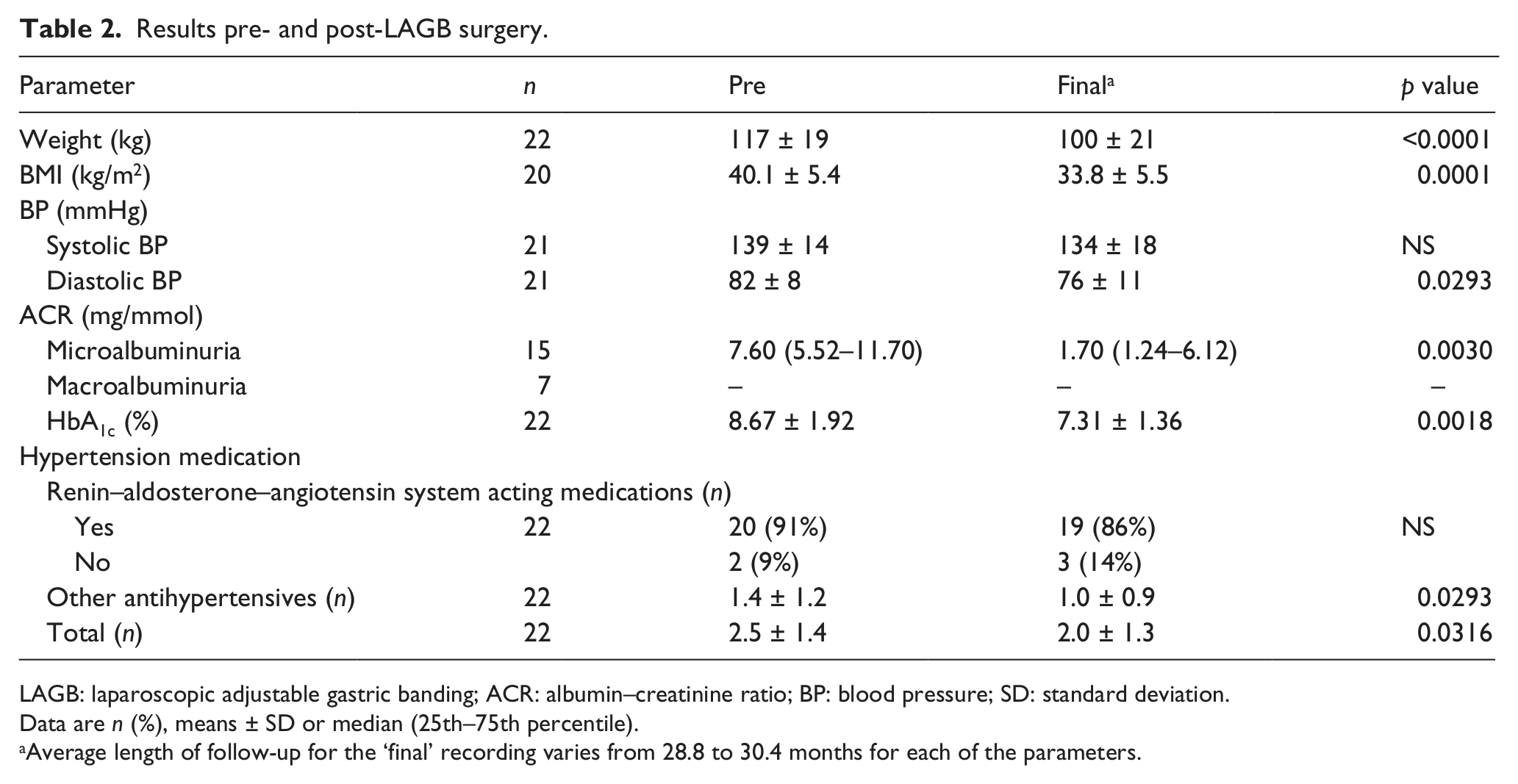
LAGB: laparoscopic adjustable gastric banding; ACR: albumin–creatinine ratio; BP: blood pressure; SD: standard deviation.
Data are n (%), means ± SD or median (25th–75th percentile).
Average length of follow-up for the ‘final’ recording varies from 28.8 to 30.4 months for each of the parameters.
Of the 7 patients with macroalbuminuria, 2 reverted to normoalbuminuria, 2 reverted to microalbuminuria and 3 remained with macroalbuminuria by their final recording in the 36-month period of follow-up. Of the 16 patients with microalbuminuria, 9 reverted to normoalbuminuria, while 6 remained with microalbuminuria. There was 1 patient who progressed from microalbuminuria to macroalbuminuria.
There were no significant differences in the majority of baseline characteristics between patients with improved albuminuria classification and patients who did not improve (Table 3). However, those that improved were younger, with an average age of 54 ± 8 years, compared with 64 ± 6 years (p < 0.01); they were on fewer antihypertensive medications, with an average of 1.8 ± 1.3 compared to 3.3 ± 0.8 (p < 0.01) and they had a lower mean SBP of 130 ± 15 mmHg compared to 146 ± 12 mmHg (p < 0.05). There was no significant association found between change in the number of antihypertensive medications used and change in albuminuria classification.
Differences in baseline characteristics between patients according to albuminuria classification at 36 months post-LAGB.
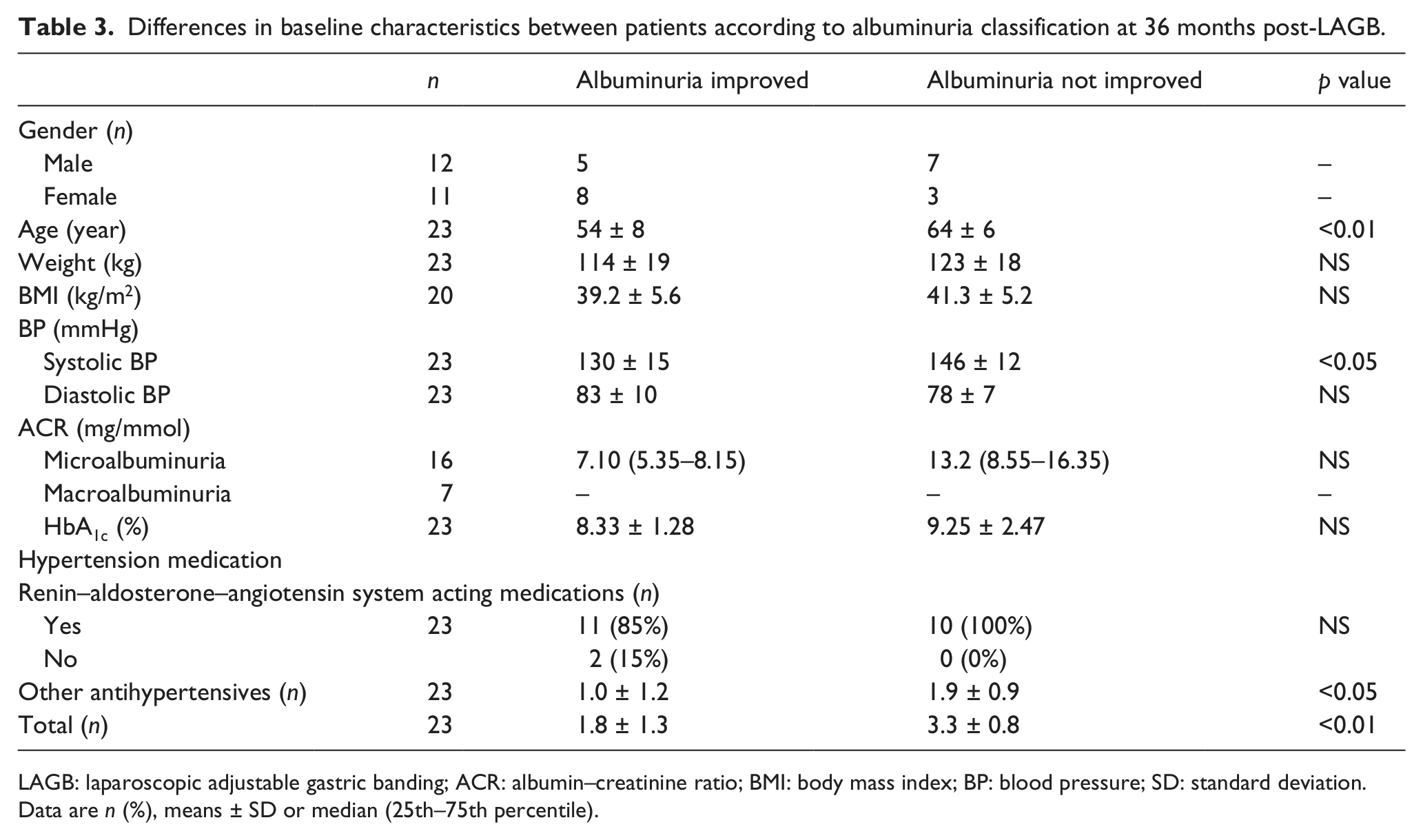
LAGB: laparoscopic adjustable gastric banding; ACR: albumin–creatinine ratio; BMI: body mass index; BP: blood pressure; SD: standard deviation.
Data are n (%), means ± SD or median (25th–75th percentile).
Patients with an improved albuminuria classification had significantly lower body weight at 12 months than those from the unimproved group (96 ± 14 kg compared to 113 ± 14 kg, p < 0.05), as well as a lower SBP (127 ± 8 mmHg compared to 143 ± 13 mmHg, p < 0.02). The group that did not improve had more use of antihypertensive medications at 12 months (average of 1.3 ± 1.1 medications compared to 3.0 ± 0.8, p < 0.01). By the final recording, weight loss and SBP were no longer found to be significantly different between the two groups. However, use of antihypertensive medications continued to be significantly different (average of 1.3 ± 1.0 medications compared to 2.8 ± 1.0, p < 0.01). The final recordings of DBP were significantly lower among the group that did not improve (70 ± 9 mmHg compared to 81 ± 10 mmHg, p < 0.02). All other characteristics at the final recording did not differ significantly between the groups.
Although single ACR measurements were used to diagnose normo-, micro-, and macroalbuminuria, previous ACR measurements confirmed that six of the seven patients who we classified as macroalbuminuric had established macroalbuminuria based on multiple urine ACR measurements; one macroalbuminuric patient had a previous recording in the microalbuminuria range. Of the 16 patients who we classified as microalbuminuric, all but 3 had established microalbuminuria based on multiple urine ACR measurements.
Discussion
Our study shows that more than 50% of the T2DM patients with diabetic nephropathy undergoing LAGB experienced a substantial improvement in albuminuria levels. This includes the potential for complete reversion from macroalbuminuria to normoalbuminuria.
Our results are similar to that of studies of Roux-en-Y Gastric Bypass (RYGB),3,19 and BPD,12,20 and their associations with renal function. All five studies have shown an improvement in albuminuria levels, from 100% reversion of microalbuminuria after 10 years of follow-up in patients who have undergone BPD, 12 to a decrease from 22.2% to 6.2% of patients having microalbuminuria after 12 months of follow-up following RYGB. 19 However, to our knowledge, our study is the first to demonstrate an improvement in macroalbuminuria, in particular, reversion from macroalbuminuria to normoalbuminuria, in T2DM patients following bariatric surgery. It is also, to our knowledge, the first study to demonstrate an improvement in both macroalbuminuria and microalbuminuria following LAGB.
The mechanisms behind the improvement in albuminuria levels following bariatric surgery are unclear. It is an area that requires further investigation, as has previously been alluded to in the literature. 21 There is known to be a link between obesity and albuminuria associated with renal vasodilatation and hyperfiltration,1,22 and it is also recognized that diabetes causes damage and loss of podocytes – glomerular epithelial cells implicated in the regulation of the glomerular filtration barrier – leading to albuminuria. 23 Other key mechanisms involved in mediating albuminuria have been proposed to include the involvement of inflammatory cytokines, renal lipotoxicity and haemodynamic factors. 21 Obesity results in an elevation in circulating proinflammatory cytokines such as interleukin-6 (IL-6) and C-reactive protein (CRP), 24 which have been shown to contribute to renal interstitial fibrosis via upregulation of transforming growth factor (TGF)-β1. 25 However, it is difficult to determine the exact mechanisms contributing to the decrease in albuminuria in our patients who have undergone LAGB.
It has previously been shown that there is a significant relationship between degree of proteinuria and risk for progression to ESRD. 26 Patients with higher levels of baseline proteinuria are more likely to progress to ESRD, and similarly, early reduction in proteinuria is associated with decreased risk of progression to ESRD. 26 Age appears to be associated with the reversibility of albuminuria in patients undergoing bariatric surgery. A previous study 27 found that patients who lost the least amount of body weight following RYGB were older on average and displayed a non-significant reversion from microalbuminuria to normoalbuminuria, unlike those who were younger and lost more weight. This is evident in our study, where we found a significant difference in the age of those who improved and those who did not. It may suggest that albuminuria is more likely to reverse in younger patients, although numbers here are small. This may be due to less permanent structural renal injury in younger patients.
A significant finding from our study relates to the weight loss among patients at 12 months following LAGB. Patients who lost a greater amount of weight within the first 12 months had a greater chance of improving their albuminuria classification. This may allude to the impact of weight loss on kidney function potentially via effects on inflammation. The degree of weight loss in our study group was around 17 kg and was substantially smaller than in other studies.2,3,12,19,20 This may relate to the fact that other studies have focused on other forms of bariatric surgery, such as RYGB,2,3,19 BPD12,20 and vertical banded gastroplasty (VBG), 1 which have been shown to be more successful in increasing weight loss. 13 This may be significant in terms of the amount of improvement in albuminuria for our patients, as a lesser degree of weight loss may lead to a lesser degree of albuminuria improvement.
We found that patients who improved their albuminuria classification were more likely to be on fewer antihypertensive medications prior to LAGB. This may be explained by the higher SBP exhibited among the patients at baseline who did not improve in our study. It is probable that this relates to the increased age of those who did not improve compared with those who did. A higher baseline SBP would indicate that more aggressive BP control is required, and therefore, a greater number of antihypertensive medications are needed.
Some recent literature has indicated that dipeptidyl peptidase-4 (DPP-4) inhibitors may contribute to a reduction in albuminuria.28,29 In our cohort, there were only 5 patients commenced on a DPP-4 inhibitor during the study period, and of these, only 2 showed improvement in albuminuria. We therefore concluded that therapy with DPP-4 inhibitors did not play a significant role in albuminuria outcomes in this study.
It is well recognized in the literature that patients with diabetic nephropathy demonstrate progression of renal dysfunction to the point of ESRD. Up to 20% of patients with overt nephropathy will progress to ESRD, regardless of the presence of intervention, within 20 years of onset. 30 More relevant to our study, it has been found that 5.4% of patients with microalbuminuria progress to overt nephropathy each year. 31 Yet in our study, only one out of 16 microalbuminuric patients (6.3%) progressed to macroalbuminuria in 3 years. Although short-term, our results are quite promising, as they highlight a substantial improvement in the progression of renal dysfunction.
It should be noted that the regression of microalbuminuria in diabetes is common, and despite the statistical significance in this study, may be a chance finding.32,33 Regression from macroalbuminuria to normoalbuminuria or microalbuminuria, however, is a rare occurrence, and in this study, found in 60% of patients with macroalbuminuria.
A clear limitation of our study is the lack of a control group as with many other similar studies.3,12,19,20 The small size of our study group also acts as a limitation. This was largely due to insufficient recordings of surgery dates and ACR measurements prior to surgery. However, similar studies3,12,19,20 had comparable limitations with relatively small sample sizes. Large randomized clinical trials are needed to more definitively assess the effects of bariatric surgery and weight loss on renal function.
As was the case with a number of other similar studies,3,12,19,20 another limitation of our study was the use of a single ACR measurement to diagnose normo-, micro- and macroalbuminuria. It is worth noting that the majority of patients from our study had established nephropathy prior to surgery; however, it is possible that some of the patients may have been misclassified.
Conclusion
This small study in patients with T2DM undergoing laparoscopic adjustable gastric banding surgery demonstrates significant improvements in albuminuria in patients with established diabetic nephropathy. This may have significant implications for patients with severe obesity and albuminuria and requires further investigation in larger clinical trials. While there is still a need to further explore the exact mechanisms behind this improvement, these results demonstrate a significant potential for LAGB to improve renal function in patients with T2DM, therefore contributing to improved long-term health outcomes.
Footnotes
Acknowledgements
Dylan T Stephenson would like to thank the Baker IDI Diabetes and Heart Institute for providing him with the opportunity to take on this research.
Declaration of conflicting interests
The authors declare that there is no conflict of interest.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.